
Abstract
Objective
This study aims to analyze the risk factors for early postoperative brain injury in patients undergoing cardiovascular surgery and explore the predictive value of transcranial color Doppler (TCCD) and regional cerebral oxygen saturation (rSO2) for detecting early postoperative brain injury in cardiovascular surgery patients.
Methods
A total of 55 patients undergoing cardiovascular surgery with cardiopulmonary bypass in Changzhou No.2 The People’s Hospital of Nanjing Medical University were included in this study. Neuron-specific enolase (NSE) concentration was measured 24 h after operation. Patients were divided into brain injury (NSE ≥ 16.3 ng/mL) and normal (0 < NSE < 16.3 ng/mL) groups according to the measured NSE concentration. The clinical outcomes between the two groups were compared, including decreased rSO2 and cerebral blood flow (as measured by TCCD) levels. The risk factors of early postoperative brain injury were analyzed by multivariate logistic regression analysis, and the significant variables were analyzed by receiver operating characteristic (ROC) analysis.
Results
A total of 50 patients were included in this study, with 20 patients in the brain injury group and 30 patients in the normal group. Cardiopulmonary bypass time (min) (107 ± 29 vs. 90 ± 28, P = 0.047) and aortic occlusion time (min) (111 (IQR 81–127) vs. 87 (IQR 72–116), P = 0.010) were significantly longer in the brain injury group than in the normal group. Patients in the brain injury group had greater decreased rSO2 (%) (27.0 ± 7.3 vs. 17.5 ± 6.1, P < 0.001) and cerebral blood flow (%) (44.9 (IQR 37.8–69.2) vs. 29.1 (IQR 12.0–48.2), P = 0.004) levels. Multivariate logistic regression analysis suggested that decreased rSO2 and cerebral blood flow levels, aortic occlusion time, and history of atrial fibrillation were independent risk factors for early postoperative brain injury (P < 0.05). ROC analysis reported that the best cutoff values for predicting early postoperative brain injury were 21.4% and 37.4% for decreased rSO2 and cerebral blood flow levels, respectively (P < 0.05).
Conclusion
The decreased rSO2 and cerebral blood flow levels, aorta occlusion time, and history of atrial fibrillation were independent risk factors for early postoperative brain injury. TCCD and rSO2 could effectively monitor brain metabolism and cerebral blood flow and predict early postoperative brain injury.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
1 Introduction
Cardiopulmonary bypass (CPB) has been widely used in cardiovascular surgery since 1953, but CPB may also cause subsequent organ damage (e.g., brain damage) [1]. Injury to the central nervous system after cardiovascular surgery can reduce the quality of life of patients and lead to death [2], and the incidence of central nervous system complications after cardiovascular surgery could be as high as 5% [3]. Therefore, the use of perioperative brain monitoring equipment is conducive to the early detection of brain injury to reduce the incidence of brain injury and improve the prognosis of patients. The regional cerebral oxygen saturation (rSO2) reflects the oxygen supply and demand of brain tissues. Although rSO2 has been widely used to monitor brain oxygen metabolism during cardiovascular surgery [4,5,6,7], the intraoperative prediction of early postoperative brain injury has not been reported thus far. In addition, there is a lack of methods to effectively monitor the cerebral blood flow, which corresponds to cerebral perfusion during surgery. The transcranial color Doppler (TCCD) combines color Doppler, two-dimensional grayscale images, and spectral Doppler to display the blood vessels and determine the blood flow spectrum. Herein, this study aimed to use TCCD to monitor the changes in cerebral blood flow during cardiovascular surgery. Additionally, this study evaluated the risk factors of early brain injury after cardiovascular surgery and investigated the predictive value of TCCD and rSO2 for detecting early postoperative brain injury.
2 Materials and methods
2.1 Patients and study design
This study was approved by the Ethics Committee of The Affiliated Changzhou No. 2 People’s Hospital of Nanjing Medical University ([2022]KY216-01) and registered with the Chinese Clinical Trials Registry (ChiCTR2300072145). A total of 55 patients undergoing cardiovascular surgery with cardiopulmonary bypass at our hospital between October 2022 and August 2023 were selected as subjects for this study.
Inclusion criteria included the following: (1) patients undergoing cardiovascular surgery with cardiopulmonary bypass; (2) over 18 years old; (3) signed informed consent.
Exclusion criteria were as follows: (1) abnormal preoperative NSE concentration; (2) preoperative examination reported carotid artery stenosis; (3) reported stroke or transient ischemic attack within six months before surgery; (4) missing temporal window; (5) under 18 years old; (6) emergency operation; (7) patient rejection; and/or (8) unforeseen accidents during the perioperative period.
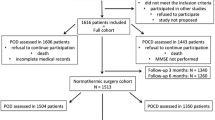
The neuron-specific enolase (NSE) concentration reflects the degree of brain injury [8]. After excluding samples with serum Hb > (0.6 g/L) 24 h after surgery, the patients were divided according to the measured NSE concentration into the brain injury (≥ 16.3 ng/mL) and normal (0–16.3 ng/mL) groups. The flow chart of the study is displayed in Fig. 1.

Flowchart of patient selection
2.2 Anesthesia
Anesthesia monitoring, electrocardiogram, pulse oxygen saturation, and non-invasive arterial blood pressure were performed/measured after the patient entered the operating room. A radial artery puncture revealed the invasive arterial pressure. A three-lumen tube was placed into the right internal jugular vein, and the central venous pressure was measured. Intravenous anesthesia (midazolam at 0.1 mg/kg, propofol at 2 mg/kg, sufentanil at 1 µg/kg, and rocuronium at 1 mg/kg) was administered after 3 min of pure oxygen mask ventilation at 6 L/min with a tidal volume of 6–8 mL/kg and frequency of 16 times/min. The position of the tracheal tube was set based on the carbon dioxide waveform after expiratory breath. During the operation, norepinephrine, ephedrine, atropine, nitroglycerin, and dopamine were used to regulate blood pressure to the optimum. Transesophageal ultrasound was used to monitor the patient’s heart condition throughout the operation. A cardiopulmonary bypass was performed by the same person.
2.3 TCCD measurement
A cardiac ultrasound instrument (Mindray, MT3, China) and a probe (P4-2s) with a probe frequency of 2.5 MHz were used to measure the bilateral middle cerebral artery flow. The probe was applied to the preauricular region of the temporal bone, and the optimal contralateral cranial window was scanned in B-scan mode to detect the midbrain. Color mode was then activated, and the colored image was superimposed on the B-scan image to display the middle cerebral artery. The spectrum was then generated with the angle between the direction of the ultrasound and the blood adjusted to less than 20°. The optimal spectrum was obtained, and the mean cerebral blood flow velocity (Vmin), diameter R of the middle cerebral artery, and blood flow velocity time integral (VTI) were measured accordingly. The cerebral blood flow per unit of time was calculated according to the formula: Q = π(R/2)^2×VTI
The definitions of the relevant parameters are as follows:
Baseline cerebral blood flow value of each patient: The mean left and right cerebral blood flow were measured 5 min before anesthesia induction.
Minimum cerebral blood flow value of each patient: The left and right cerebral blood flow values were recorded every 10 min from the beginning to the end of the cardiopulmonary bypass. The average values of the left and right sides were calculated, and the lowest value was selected.
Decreased cerebral blood flow value: (Basic value of cerebral blood flow–minimum value of cerebral blood flow)/basic value of cerebral blood flow ×100%.
2.4 rSO2 measurements
Intraoperative rSO2 was monitored by near-infrared spectroscopy (Covidien, 5100 C, USA). The level of rSO2 was continuously measured after the patient entered the operating room by attaching the electrodes to the left and right frontal parts of the patient.
The definitions of the relevant parameters are as follows:
Baseline rSO2 value of each patient: Average rSO2 readings on the left and right sides of the patient at the time of air inhalation measured 5 min before anesthesia induction.
Minimum rSO2 value of each patient: The average rSO2 value of the left and right sides was recorded every 10 min during cardiopulmonary bypass, and the lowest value was taken.
Decreased rSO2 value: (rSO2 base value–rSO2 lowest value)/rSO2 base value ×100%.
2.5 Observational indices
The following indices were recorded and compared between the two groups: (1) general patient information such as age, sex, body mass index (BMI), history of hypertension, diabetes, cerebral infarction, and atrial fibrillation; (2) left ventricular ejection fraction (LVEF), preoperative platelet count, preoperative erythrocyte specific volume (HCT), operation time, cardiopulmonary bypass time, aortic occlusion time, postoperative hospital stay, NSE concentration, and other clinical indices; (3) decreased cerebral blood flow and rSO2 levels.
2.6 Statistical analysis
IBM SPSS Statistics 23 (IBM Corporation, Armonk, NY, USA) was used for data processing, and the graphs were plotted using GraphPad Prism 8 (GraphPad Software, La Jolla, CA, USA). The Shapiro-Wilk test was used to test data normality, and the continuous variables were expressed as the mean and standard deviation (normal distribution) or the median and interquartile range (non-normal distribution). Differences were compared using the student’s t-test and Mann-Whitney U rank-sum tests. Categorical variables were expressed as numbers and percentages, and the differences were compared using a chi-square test. A multiple linear regression model was constructed to evaluate the relationship between perioperative data and NSE concentration. A logistic regression (step forward, enter when P < 0.05, exit when P > 0.1) model was constructed to determine the risk factors for early brain injury after cardiac surgery. The best predictive values for continuous variables were calculated based on recipient operating characteristic (ROC) curves, and both the Hosmer and Lemeshow statistics were used to assess the model fit. P-value < 0.05 was considered statistically significant.
3 Results
A total of 55 patients were enrolled in the study, of which five were removed (two perioperative deaths, two missing temporal window, and one missing data), and 50 patients were included in the final analysis. A total of 20 patients had abnormal NSE (brain injury group), and a total of 30 patients had normal NSE (normal group).
3.1 Comparison of baseline and perioperative data between the two groups
No statistically significant difference existed in basic features between the two groups (Table 1). For perioperative characteristics, CPB time (min) in the brain injury group was longer than that in the normal group (107 ± 29 vs. 90 ± 28, P = 0.047), and aortic occlusion time was significantly different between the two groups (P = 0.010), which was 111 (IQR 81–127) min in the brain injury and 87 (IQR 72–116) min in the normal group, respectively. In addition, the brain injury group reported lower rSO2 (%) (27.0 ± 7.3 vs. 17.5 ± 6.1, P < 0.001) and cerebral blood flow (%) (44.9 (IQR 37.8–69.2) vs. 29.1 (IQR 12.0–48.2), P = 0.004) values and larger concentrations of NSE (36.7 (IQR 30.2–49.3) vs. 10.6 (IQR 3.8–12.4), P < 0.001) than the control group (Table 2).
3.2 Correlation of cerebral blood flow, rSO2, and NSE concentration
The variance inflation factor (VIF) of all continuous variables was less than five, indicating that there was no interaction between the continuous variables. Baseline data and perioperative characteristics were included in the variables to construct a linear regression model for NSE concentration. Results indicated that the decreased rSO2 levels strongly correlated with the concentration of NSE (β = 0.583, P < 0.001). In addition, NSE concentrations were higher in patients with a history of cerebral infarction (β = 0.279, P = 0.020) (Table 3).
To determine the variables related to abnormal NSE concentration, the decreased rSO2 effect was excluded from the variables, and the remaining variables were included in another multiple linear regression analysis. Results revealed that the regression equation of this model was significant (F = 5.746, P < 0.001) (Table 4). NSE concentration was lower in patients without a history of cerebral infarction than in patients with a history of cerebral infarction before surgery (β = 0.289, P = 0.027). Lower cerebral blood flow led to higher NSE concentrations (β = 0.354, P = 0.005). Similarly, aortic occlusion time (β = 0.332, P = 0.011) effectively predicted NSE concentration. Taken together, these variables accounted for approximately 40.4% of the differences in NSE concentrations between the two groups.
3.3 Analysis of multivariate logistic regression results
In the regression model that included the decreased rSO2 level (Table 5), decreased rSO2 decline was an independent risk factor for postoperative brain injury, with an odds ratio value (OR) of 1.246. The regression model that did not include the decreased rSO2 level (Table 6), the decreased cerebral blood flow (OR = 1.047, P = 0.013), the duration of aortic occlusion (OR = 1.044, P = 0.010), and the history of atrial fibrillation (R = 5.257, P = 0.044) were independent risk factors for postoperative brain injury. The Hosmer-Lemeshow test revealed that the model was well-fitting (P > 0.05).
3.4 Analysis of the best predictive values in the ROC curve
The area under the ROC curve, corresponding to the correlation between decreased rSO2 and brain injury, was 0.863 (95% CI: 0.758–0.967, P < 0.001). The area under the ROC curve, corresponding to the correlation between decreased cerebral blood flow and brain injury, was 0.739 (95% CI: 0.603–0.875, P = 0.004) (Fig. 2). The best intercept values for predicting brain injury were 21.4% (sensitivity: 80%; specificity: 85%) and 37.4% (sensitivity: 67%; specificity: 80%) for decreased rSO2 and cerebral blood flow levels (Table 7).
3.5 Comparison of postoperative hospital stay between the two groups
Patients in the brain injury group reported a longer hospital stay than patients in the normal group, but the difference was not statistically significant (P = 0.064) (Fig. 3).

The area under the ROC curve for the ability of decreased rSO2 and cerebral blood flow levels to predict early brain injury

Comparison of postoperative hospital stay between the brain injury and normal groups

Cerebral blood flow spectrum during cardiopulmonary bypass
4 Discussion
The non-pulsating blood flow caused by the cardiopulmonary bypass device damages multiple organs in the body, especially the brain. Non-physiological blood flow alters blood supply to the brain tissues, and damage to the transmission of arterial pulsation to the “pulse brain” tissue will alter the brain structure and function [9, 10]. Brain injury after cardiovascular surgery will increase the degree of pain in patients and reduce their quality of life [2]. Therefore, it is crucial to implement intraoperative brain monitoring and timely intervention to reduce the incidence of postoperative brain injury. In this study, TCCD was used to monitor the changes in cerebral blood flow during cardiac surgery, and rSO2 was used to monitor the changes in cerebral oxygen metabolism. Taken together, TCCD and rSO2 could effectively predict early postoperative brain injury, and this study also identified the risk factors of early brain injury after cardiovascular surgery.
NSE is considered a specific neuro-biochemical marker of neuronal injury [11]. The level of serum NSE was significantly increased after brain injury and was significantly correlated with the severity of brain injury after ischemia [12]. In this study, the patients were divided into the early postoperative brain injury and normal groups according to the measured NSE concentration 24 h post-surgery. We observed significant differences in CPB time, decreased rSO2 level, decreased cerebral blood flow level, aortic occlusion time, and NSE concentration between the two groups. Further analysis indicated that decreased rSO2 level was strongly correlated with NSE concentration. In the model without decreased rSO2, decreased cerebral blood flow level, aortic occlusion time, and cerebral infarction history were correlated with NSE. Therefore, decreased rSO2 was considered the most important factor affecting NSE concentration. Patients with a history of cerebral infarction were more likely to be affected by ischemia, and the degree and time of low cerebral blood flow that could be tolerated were also reduced. Hence, patients with a history of cerebral infarction in this trial were more likely to develop postoperative NSE abnormalities.
The parameter rSO2 has good stability and is not affected by arterial pulse. Additionally, relatively stable rSO2 values could be observed in patients with hemodynamic instability or even cardiac arrest [13]. In this study, decreased rSO2 level was identified as an independent risk factor for postoperative brain injury with high diagnostic value. If decreased rSO2 level was more than 21.4%, postoperative brain injury was more likely to occur. Similarly, Klinkova et al. observed that 19% of 200 patients with a 20% or greater decrease in rSO2 during CPB had a higher risk of neurological complications [14]. It was also reported that maintaining intraoperative rSO2 levels above 80% of the baseline value during cardiac surgery could reduce the incidence of cognitive impairment seven days post-surgery [15]. In a coronary artery bypass grafting study, patients with rSO2 levels maintained above 75% of baseline value spent significantly less time in the intensive care unit and hospital stay after surgery than patients in the no-intervention group [16]. These studies demonstrated that monitoring rSO2 is important to improve cardiac surgery. However, rSO2 levels may be affected inevitably. rSO2 monitoring is affected by the position of its electrodes. Usually, the electrodes are selected to be placed on the forehead. Although global cerebral oxygen sufficiency can be evaluated, it may not be possible to detect changes in areas far from the monitored site. Another factor is its signal may be disturbed by external information, such as skull thickness, skin pigment, etc., and we may eliminate some of the effects by maintaining the same position during the operation. Moreover, rSO2 monitoring is also susceptible to hemoglobin concentration, especially during cardiac surgery, when blood is diluted to a certain extent, such that decreased hemoglobin levels can also lead to decreased rSO2 levels [17]. Therefore, it is inadequate to evaluate cerebral blood flow with only rSO2 levels during surgery. Likewise, this study further evaluated TCCD to measure cerebral hemodynamics, obtain cerebral blood flow, observe vascular misalignment, and determine the presence of plaque [18]. Our findings revealed that, in the absence of decreased rSO2 levels, decreased cerebral blood flow (measured by TCCD) was identified as an independent risk factor for early postoperative brain injury, and the decrease of more than 37.4% could predict early postoperative brain injury. Six patients in the brain injury group had no significant decrease in rSO2, while the decrease in cerebral blood flow measured by TCCD was much greater than 37.4%. Hence, TCCD could be used to supplement rSO2 monitoring for more accurate and comprehensive results. According to Catena et al. [19], during aortic arch surgery, TCCD could monitor cerebral blood flow, optimize the rate of anterograde and retrograde cerebral perfusion, and avoid hyper-perfusion or hypo-perfusion during cardiac arrest. Additionally, during cardiopulmonary bypass, the cerebral blood flow spectrum was altered with a jagged waveform, which was consistent with our observation (Fig. 4). This change is related to the use of non-pulsating pumps during cardiopulmonary bypass. In addition, TCCD can also detect the occurrence of embolic events [20]. However, its limitations can lead to difficulties. TCCD operation is dependent on the operator’s proficiency. Therefore, it is not easy for any one person to obtain it, provided that it is systematically trained.
In cardiovascular surgery, it is often necessary to block the aorta to facilitate the operation. However, the results of this study suggested that the duration of aortic occlusion over 86 min may indicate early postoperative brain injury. Long-term aortic occlusion may not only affect cerebral perfusion but also damage the vascular endothelium and induce coagulation disorders. In addition, a history of atrial fibrillation was a risk factor for early postoperative brain injury. Atrial fibrillation causes cerebral blood flow and fluctuations in blood perfusion to the brain. Studies have found that atrial fibrillation can damage the blood-brain barrier, causing patients to be more susceptible to cognitive impairments later in life [21]. In this study, the duration of hospital stay in the brain injury group was longer than that in the normal group, but there was no statistical difference. However, in some studies, longer hospital stays after surgery were associated with lower rSO2 levels [4, 22], which could be due to other clinical factors.
There were some limitations in this study, particularly the inclusion of more than one type of cardiovascular surgery, which might have affected the results. Likewise, further research is required to investigate specific interventions to reduce early postoperative brain injury.
In conclusion, the combined multi-modal monitoring of rSO2 and TCCD holds great significance for brain protection during cardiovascular surgery and can be used to predict early postoperative brain injury.
Data availability
No datasets were generated or analysed during the current study.
References
GIBBON JH Jr. Application of a mechanical heart and lung apparatus to cardiac surgery. Minn Med. 1954;37(3):171–85.
Cropsey C, Kennedy J, Han J, Pandharipande P. Cognitive dysfunction, Delirium, and stroke in cardiac surgery patients. Semin Cardiothorac Vasc Anesth. 2015;19(4):309–17.
Arrowsmith JE, Grocott HP, Reves JG, Newman MF. Central nervous system complications of cardiac surgery. Br J Anaesth. 2000;84(3):378–93.
Apostolidou I, Morrissette G, Sarwar MF, Konia MR, Kshettry VR, Wahr JA, Lobbestael AA, Nussmeier NA. Cerebral oximetry during cardiac surgery: the association between cerebral oxygen saturation and perioperative patient variables. J Cardiothorac Vasc Anesth. 2012;26(6):1015–21.
Yu Y, Lyu Y, Jin L, Xu L, Wang H, Hu Y, Ren Y, Guo K. Prognostic factors for permanent neurological dysfunction after total aortic arch replacement with regional cerebral oxygen saturation monitoring. Brain Behav. 2019;9(7):e01309.
Rogers CA, Stoica S, Ellis L, Stokes EA, Wordsworth S, Dabner L, Clayton G, Downes R, Nicholson E, Bennett S, Angelini GD, Reeves BC, Murphy GJ. Randomized trial of near-infrared spectroscopy for personalized optimization of cerebral tissue oxygenation during cardiac surgery. Br J Anaesth. 2017;119(3):384–93.
Zhang Y, Duan B, Wang L, Ye Z, Pan Y, Guo Q, Wang E. Association between the variability of cerebral oxygen saturation during cardiopulmonary bypass and delayed postoperative neurocognitive recovery in cardiac valve surgical patients: a pilot study. Int J Clin Pract. 2021;75(1):e13651.
Persson L, Hårdemark HG, Gustafsson J, Rundström G, Mendel-Hartvig I, Esscher T, Påhlman S. S-100 protein and neuron-specific enolase in cerebrospinal fluid and serum: markers of cell damage in human central nervous system. Stroke. 1987 Sep-Oct;18(5):911-8. https://doi.org/10.1161/01.str.18.5.911. PMID: 3629651.
Wagshul ME, Eide PK, Madsen JR. The pulsating brain: a review of experimental and clinical studies of intracranial pulsatility. Fluids Barriers CNS. 2011;8(1):5.
Bateman GA. Pulse wave encephalopathy: a spectrum hypothesis incorporating Alzheimer’s disease, vascular dementia and normal pressure hydrocephalus. Med Hypotheses. 2004;62(2):182–7.
Wunderlich MT, Ebert AD, Kratz T, Goertler M, Jost S, Herrmann M. Early neurobehavioral outcome after stroke is related to release of neurobiochemical markers of brain damage. Stroke. 1999;30(6):1190–5.
Woertgen C, Rothoerl RD, Brawanski A. Neuron-specific enolase serum levels after controlled cortical impact injury in the rat. J Neurotrauma. 2001;18(5):569–73.
Sanfilippo F, Serena G, Corredor C, Benedetto U, Maybauer MO, Al-Subaie N, Madden B, Oddo M, Cecconi M. Cerebral oximetry and return of spontaneous circulation after cardiac arrest: a systematic review and meta-analysis. Resuscitation. 2015;94:67–72.
Kamenskaya O, Klinkova A, Loginova I, Lomivorotov VV, Shmyrev V, Chernyavskiy A. Brain oxygen supply in older adults during coronary artery bypass grafting. J Cardiothorac Vasc Anesth. 2020;34(12):3275–81.
Colak Z, Borojevic M, Bogovic A, Ivancan V, Biocina B, Majeric-Kogler V. Influence of intraoperative cerebral oximetry monitoring on neurocognitive function after coronary artery bypass surgery: a randomized, prospective study. Eur J Cardiothorac Surg. 2015;47(3):447–54.
Murkin JM, Adams SJ, Novick RJ, Quantz M, Bainbridge D, Iglesias I, Cleland A, Schaefer B, Irwin B, Fox S. Monitoring brain oxygen saturation during coronary bypass surgery: a randomized, prospective study. Anesth Analg. 2007;104(1):51–8.
Kishi K, Kawaguchi M, Yoshitani K, Nagahata T, Furuya H. Influence of patient variables and sensor location on regional cerebral oxygen saturation measured by INVOS 4100 near-infrared spectrophotometers. J Neurosurg Anesthesiol. 2003;15(4):302–6.
Dupont G, Burnol L, Jospe R, Raphael T, Auboyer C, Molliex S, Gergelé L, Morel J. Transcranial color duplex Ultrasound: A Reliable Tool for cerebral hemodynamic Assessment in Brain injuries. J Neurosurg Anesthesiol. 2016;28(2):159–63.
Catena E, Tasca G, Fracasso G, Toscano A, Bonacina M, Narang T, Galanti A, Triggiani M, Lorenzi G, Gamba A. Usefulness of transcranial color Doppler ultrasonography in aortic arch surgery. J Cardio vasc Med (Hagerstown). 2013;14(8):597–602.
Rasulo FA, Bertuetti R. Transcranial Doppler and Optic nerve Sonography. J Cardiothorac Vasc Anesth. 2019;33:S38–52.
Galenko O, Jacobs V, Knight S, Bride D, Cutler MJ, Muhlestein JB, Carlquist JL, Anderson JL, Knowlton KU. Jared Bunch T. Circulating Levels of Biomarkers of Cerebral Injury in patients with Atrial Fibrillation. Am J Cardiol. 2019;124(11):1697–700.
Fischer GW, Lin HM, Krol M, Galati MF, Di Luozzo G, Griepp RB, Reich DL. Noninvasive cerebral oxygenation may predict outcome in patients undergoing aortic arch surgery. J Thorac Cardiovasc Surg. 2011;141(3):815–21.
Acknowledgements
The current work received exclusive support from departmental resources.
Funding
The current work received exclusive support from departmental resources. (Grant numbers: ZD202318;CMCC202214)
Author information
Authors and Affiliations
Contributions
Conception and design: ZQW; Data collection and analysis: YL, LZ, LXW; Writing—original draft preparation: YL; Writing—review and editing: ZQW. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Ethics Committee of The Affiliated Changzhou No. 2 People’s Hospital of Nanjing Medical University ([2022]KY216-01) and registered with the Chinese Clinical Trials Registry (ChiCTR2300072145).
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Liu, Y., Zhao, L., Wang, X. et al. Predictive value of TCCD and regional cerebral oxygen saturation for detecting early postoperative brain injury. J Clin Monit Comput (2024). https://doi.org/10.1007/s10877-024-01165-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s10877-024-01165-y