
Abstract
Purpose
Catheter ablation for atrial fibrillation (AF) has become a widely accepted procedure in most of the large cardiac centers throughout the world. However, little is known regarding the knowledge, attitude, and behavior (KAB) of AF patients undergoing radiofrequency catheter ablation (RFCA). Our purpose is to investigate the status and influencing factors of KAB in these patients.
Methods
We conducted a KAB survey utilizing specifically designed questionnaires among hospitalized AF patients undergoing RFCA from July 2008 to April 2009.
Results
A total of 116 AF participants were enrolled and 113 were effective sample, the response rate was 97%. Only 47% of the participants answered questions regarding knowledge about AF correctly. Knowledge deficits were greater in male patients, poorly educated and first-time RFCA patients. With regard to attitude, 45% of participants considered daily pulse examination to be unnecessary. Higher knowledge scores, persistent AF and AF recurrence were positive predictors of attitude. Despite adherence to take medication was high, more than half of the participants demonstrated poor monitor behavior. Knowledge, attitude, and the number of previous attempts at RFCA were factors affecting the self-management behavior.
Conclusions
AF patients undergoing RFCA have knowledge deficits in general and there is a lack of consistency among their KAB. In order to establish a better attitude and self-management behavior, AF patients undergoing RFCA need comprehensive education by the KAB questionnaire according to the KAB theory.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
1 Introduction
Atrial fibrillation (AF) is the most common cardiac arrhythmia in clinical settings. The estimated prevalence of AF is 0.4-1.0% in the general population and increases with age [1]. A population-based study in China revealed that 0.77% of Chinese are currently afflicted by AF. This suggests that there are over 10 million adults with AF in China [2]. AF is likely to become more prevalent due to increasing cardiovascular risk factors, and the rising age of the population. Although AF itself is not directly life threatening, its complications (such as stroke and cardiac dysfunction) significantly increase morbidity and mortality, thereby making AF a serious medical and social problem [3, 4].
Knowledge, attitude, and behavior (KAB), also found in literature as knowledge-attitude-practice (KAP), is an important theoretical model of health education, which asserts that behavior change is affected by knowledge and attitude [5]. From social learning theory, the health belief model, and the model of responsible environmental behavior, we learn that attitude is significantly important in behavior adoption. One implication is that educators should work to instill positive attitude into people in order to change their choice of action. People are likely to take action if they believe what they are going to do bear a significant value. These motivations can be further reinforced by successful experience, as well as the positive feedbacks that come along, in similar situation [5]. Evidence suggests that compliance is improved if patients know what they have been prescribed, what it will do to their bodies, what will happen if they fail to take medications according to doctor’s instruction, any factors which may alter drug efficacy, and any possible side effects [6]. Patients’ belief regarding their health care is an important factor that influences their decision to accept, decline, or comply with anticoagulant therapy, particularly warfarin [7]. Previous studies have demonstrated that the majority of AF patients possess very little knowledge about their disease and anticoagulation therapy [8, 9]. Munschauer et al. pointed out that appropriate education can improve awareness of AF and promote their self-monitoring behavior, thereby effectively preventing stroke [10]. However, these studies concerning health education of AF patients were all confined to drug therapy.
To the best of our knowledge, no such study has examined the KAB of AF patients undergoing radiofrequency catheter ablation (RFCA), specifically healthy behavior, such as periodic self-monitoring, adherence to medication regimen, and periodic follow-up. The aim of this study is to investigate the status and influencing factors of KAB in patients with AF who would undergo RFCA, providing a foundation to develop effective education approaches to increase patient’s knowledge, so as to form a correct attitude and self-management behavior after they undergo RFCA.
2 Methods
2.1 Patient eligibility
From July 2008 to April 2009, 116 consecutive patients with AF, who would undergo RFCA, were recruited into the study. All participants had at least two ECG-documented episodes of AF, and had been diagnosed with AF for 6 months. Participants should have been taking warfarin for at least 3 months before hospitalization.
Exclusion criteria for patients included the following: (a) malignant tumor or other diseases at the terminal stage, (b) the occurrence of myocardial infarction or thromboembolic events within 3 months, (c) physical or mental limitations in completing the questionnaire, (d) thyroid dysfunction, or (e) unwillingness to sign informed consent.
2.2 Questionnaire introduction and data acquisition
There was no existed questionnaire that assessed KAB related to patients with AF undergoing RFCA. Following the previous relative literature[1, 8, 9, 11–13], a structured questionnaire was accordingly designed specifically for patients with AF undergoing RFCA based on face to face interview results of 30 patients with AF undergoing RFCA and the advice by experts and panel discussions. These allowed us to check if the questions were well understood and all pertinent to our project. Minor corrections were made accordingly, so that the questionnaire was in a definitive form.
There were four parts to the questionnaire. The first part included some biographical information of participants such as age, gender, marital status, occupation, educational level, AF classification, initial ablation/redo ablation, and previous attempts at RFCA and AF history.
The second part was a disease knowledge scale which had 25 items in total and included five aspects (Appendix A): (1) knowledge about AF, (2) knowledge about warfarin, (3) knowledge about a healthy lifestyle, (4) knowledge about RFCA, and (5) knowledge about self-monitoring. All subjects need to respond “Yes,” “No,” or “Unknown” to each question. A correct answer was scored 1; an incorrect answer or an answer of “Unknown”was scored 0. For example, one of the questions was “Does it necessary to monitor INR when taking warfarin? The answering options were: Yes/No/Unknown”. Scores of each item were summed up, and the total score ranged from 0 to 25. Score percentage = mean score/maximum possible score ×100%. Higher scores indicated more knowledge about AF.
The third part was the attitude scale also included five content domains as follows (Appendix B): (1) perceived severity of AF (item1-3), (2) perceived susceptibility (item 4-6), (3) perceived benefits (item 7-10), (4) perceived barriers (item 11-14), and (5) motivation to maintain health (item 15-17). For each item, participants rated their self-care attitude on a five-point Likert scale from “I do not agree at all” to “I completely agree”. If the question was non-invert, the answer of “I do not agree at all” was scored 1 and “I completely agree” was scored 5. If the question was invert, the opposite was true. The total score ranging from 17 to 85 was calculated by summing up the scores of each item. A higher score indicated a more positive attitude.
The last part is the behavior scale which had 13 items covering information on self-management behavior (Appendix C). It included adherence to medication regimen (item 1-4), international normalized ratio (INR) monitoring, periodic follow-up, daily pulse self-examination, and a healthy lifestyle (item 8-13). For each item, participants rated their self-management behavior on a four-point Likert scale ranging from 1 (“never”) to 4 (“always”). The total score ranging from 13 to 52 was calculated by summing up the scores of each item. Higher scores indicated a better self-management behavior. The content domain’s score was calculated by putting together the scores for each item in one dimension.
This questionnaire was previously tested in a pre-survey including 276 patients with AF undergoing RFCA from the First Affiliated Hospital of Nanjing Medical University in China. This pilot test was performed to determine the reliability and validity of the questionnaire. In our study, Cronbach’s alpha coefficient was used to assess the internal consistency of questionnaire’s reliability. Content validity and construct validity were used to assess the validity of the questionnaire. A good questionnaire should have a Cronbach’s α coefficient more than 0.8. Cronbach’s α of KAB questionnaire in AF patients were 0.885, 0.825, and 0.862, respectively, all of which are more than 0.8, showing that the KAB questionnaire has a good internal consistency reliability. The KAB questionnaire was modified and evaluated by experts group including six cardiology experts, two cardiology nursing specialist, and one expert in nursing education. Content validity was expressed by content validity index (CVI). Generally, CVI should reach more than 0.75. The CVI of the KAP questionnaires were 0.946, 0.921, and 0.949, respectively. It proved that the item of the KAP questionnaires appropriate coverage of the health-related knowledge, attitude, and behavior in AF patients. We assessed construct validity by exploratory factor analysis. A principal component analysis using a varimax rotated solution produced five, five, and three factors with Eigenvalues greater than 1.0 of the three questionnaires, respectively. Inspection of the items loading on each factor suggested that they were best described as “AF”, “warfarin”, “healthy lifestyle”, “RFCA”, and “self-monitoring” of knowledge questionnaire, “severity of AF”, “susceptibility”, “benefits”, “barriers”, and “motivation to maintain health” of attitude questionnaire, “adherence to medication regimen”, “monitoring”, and “healthy lifestyle” of behavior questionnaire. Communalities of each item were greater than 0.4, it means that every subject could explain more than 40% variance. These results showed that the questionnaire had good construct validity. To conclude, all above demonstrated that this questionnaire had a good reliability and validity for the assessment of AF patients’ KAB who were undergoing RFCA.
Each participant was interviewed by the investigator in a standardized manner on the second day of hospitalization. If the participant was illiterate, the investigator would explain the questions and helped the participant to complete the questionnaire. If the participant wanted to fill it by their own, they could finish it according to the directions on the questionnaire. If the data was not filled out completely, we would re-back or call him/her for supplement.
2.3 Statistical analysis
Data were double-entered into Epidata 3.1 and analyzed by SPSS15.0. Frequencies, percentages, means, and standard deviations were used to describe the demographic and clinical characteristics of the sample, knowledge level, attitude, and self-management behaviors. After checking that there was no multicollinearity between the variables, multiple regression analysis was performed using backward elimination to determine what variables were significant in predicting the KAB of AF patients undergoing RFCA. Multicollinearity was assessed by correlation coefficients between variables and the variance inflation factor. The backward elimination technique began by calculation of F-statistics for a model, including all independent variables. The variables were deleted from the model one by one until all the variables remaining in the model produced F-statistics significant at P < 0.05. At each step, the variable showing the smallest contribution to the model was deleted. All statistical tests were two-tailed, and P < 0.05 was considered to indicate a statistically significant difference.
3 Results
In total, questionnaires were delivered to 116 patients, and 113 were effective samples. The response rate was 97%. The three noneffective questionnaires were ruled out due to the language or reading barriers during the interview of the patients.
3.1 Characteristics of participants
Of the participants, 113 (age 56.2 ± 10.3 years) were included in the final analysis. The participants’ characteristics are shown in Table 1.
3.2 Knowledge and its influencing factors on AF patients
The percentage of participants reporting correct responses related to AF healthcare knowledge was low (Table 2). There were knowledge deficits regarding potential hazards of AF, purpose of therapy for AF, purpose of monitoring INR, vitamin K-contained products, dietary-drug interactions, complications of AF ablation, the treatment efficacy of RFCA, and sings/symptoms need to report to doctor. Of the participants, only 47% were able to report correct knowledge related to AF. Table 3 shows the domains’ scores of participants who reported correct responses to items related to AF healthcare knowledge. The total score for healthcare knowledge about AF was 11.79 ± 5.58 (range 0-24).
The relationship between knowledge and ten characteristic factors of the 113 AF participants was explored with multiple linear regression. In regression analysis, the dependent variable was the total score of knowledge, and the independent variables were the ten characteristics of participants, such as age, gender, marital status, occupation, educational level, AF classification, initial ablation/redo ablation, previous attempts at RFCA and AF history. The result suggests that female patients (B = 2.025, P = 0.028), those with higher education (B = 2.118, P < 0.001), and more RFCA attempts (B = 3.870, P < 0.001) were predictors of greater AF knowledge.
3.3 Attitude and its influencing factors in AF patients
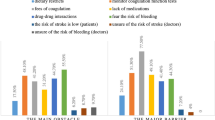
Table 4 presents the domains’ scores of participants’ healthy attitude related to AF. Approximately half of the participants (45%) answered that it was unnecessary to take periodic follow-up and pulse monitoring. Of the participants, 27% reported that if there is no embolic complication, it is unnecessary to take anticoagulant drugs. Eighteen percent stated that taking medication on schedule is troublesome; it is convenient to take medication only when feeling uncomfortable. The mean score of attitude of the 113 participants was 71.23 ± 6.64 with a range of 56-83.
In linear regression analysis, the dependent variable was the total score of the attitude, and the independent variables were the ten characteristics of participants and the knowledge score. The result suggested that higher knowledge scores (B = 0.417, P < 0.001), persistent AF (B = 2.513, P = 0.028) and AF recurrence (B = 2.866, P = 0.024) were positive predictors of AF attitude.
3.4 Self-management behavior and its influencing factors in AF patients
Table 5 demonstrates the number and percentage of participants reporting performance of self-management behavior. More than half of the participants showed poor monitor behavior (never or seldom). Of the patients, 58% were not able to have INR monitored on the requested dates, 50% patients were not able to attend regular follow-up on the requested dates, and 64% patients admitted not checking their pulse daily. However, the percentage of adherence to prescribed medication was higher than any other area of compliance. The mean score of taking medications as prescribed domain was 13.30 ± 2.34 (range 8-16), INR monitoring domain was 2.20 ± 1.15 (range 1-4), keeping follow-up domain was 2.38 ± 1.07 (range 1-4), daily pulse self-examination domain only was 1.96 ± 1.05 (range 1-4), and healthy lifestyle domain was 18.78 ± 2.78 (range 10-24). The mean score of behavior in this study was 38.63 ± 5.78 with a range of 21-50.
In backward elimination of linear regression analysis, the dependent variable was the total score of the behavior, and the independent variables were the knowledge, attitude score, and the ten characteristics of the participants. The result demonstrates that knowledge (B = 0.539, P < 0.001) and attitude (B = 0.175, P = 0.024) were positive predictors of AF self-management behavior, while the number of previous attempts at RF catheter ablation was a negative predictor of AF self-management behavior (B = -3.007, P < 0.001).
4 Discussion
In the past decade, RFCA for AF evolved rapidly and has now become a commonly performed procedure in many major hospitals throughout the world. Close attention to anticoagulation therapy of patients before, during, and after RFCA is critical to avoid the occurrence of thromboembolic event, which is recognized as one of the most serious complications of AF itself and AF ablation procedures. Antiarrhythmic drugs are commonly employed to treat all patients in the first 1-3 months after RFCA [11]. Therefore, it is important to ensure drug therapy is effective and safe after an ablation, and it is meaningful to enhance self-management behavior in patients with AF.
KAB theory believes that healthcare knowledge is the basis of establishing a better attitude and behavior, and positive attitude is the propulsion to form a good self-management behavior. Our study evaluated KAB, and identified factors related to KAB among AF patients who underwent RFCA. Numerous implications for health education practices are evident from the results of this study.
4.1 Delivering appropriate knowledge to male and poorly educated patients
The results of this study show that the percentage of participants who were able to report correct AF knowledge was low. This is not unique and is very similar to the previous researches [8, 9]. McCabe et al. found there were knowledge deficits related to AF symptoms, purpose of medication, risks for stroke, warning signs of stroke, and complications of warfarin in their research [8]. These deficits will raise the risk of bleeding and/or predisposition to thromboembolism.
Our study also revealed that gender, level of education, and the number of previous RFCA attempts are positive predictors of AF knowledge, and the difference is statistically significant. Female AF patients seem to have a greater interest in the consequences of their diseases and pay more attention to their health status, which made them more responsive to education campaigns. With higher education levels, the knowledge score of AF patients is significantly higher, which may relate to the ability to self-learning, acquiring, and understanding knowledge. This interpretation was supported by our findings and the previous studies [8, 12]. Healthcare providers ought to strengthen measures aimed at improving knowledge about AF in male patients and poorly educated patients. A trend toward higher scores was found in those patients having more RFCA attempts. This may be attributed to having more educational opportunities during a previous hospitalization.
However, formal education provided during hospitalization did not appear to be retained at 2 weeks after discharge in the previous study [8]. Health education is not once and for all. Even in female patients and those with higher education level and more RFCA attempts who may possess much more knowledge, healthcare providers should still intensify efforts to disseminate healthcare knowledge to them. Education throughout all populations in order to supplement and reinforce AF knowledge. So from this study, we hope healthcare providers should continue their healthcare education to all the AF patients both before and after hospitalization.
4.2 Raising more awareness among with paroxysmal AF patients and initial ablation AF patients
AF education and research should not only be stressed in terms of increasing patients’ knowledge, but also on their attitude. In China, AF education and research had paid more attention to increasing in patients’ knowledge, but few focused on patients’ beliefs and attitudes.
Patients’ beliefs about their healthcare are important factors that influence their decision to accept, decline, or comply with anticoagulant therapy, particularly warfarin [14]. But our study found that 27% of the participants believed that it was unnecessary to take anticoagulant drugs if there was no embolic complication. So, healthcare education givers should raise more attention towards AF patients’ attitude. The other finding from our study was that knowledge was a positive predictor of AF attitude. AF patients with more knowledge possessed more positive attitudes. This is consistent with the KAB theory. In this study, analysis demonstrated that the attitude scores in persistent AF patients and recurrent AF participants were significantly higher than those in paroxysmal and initial ablation patients. This may be because patients with persistent AF or AF recurrence knew the difficulties of the treatment and this made them pay more attention to their health status. The previous study revealed that after a brief educational intervention with an information booklet, there was a non-significant trend towards an increase in awareness of the severity and consequences of AF [9]. Because of this, educational intervention should be emphasized to focus on the patients’ attitude produced by the KAB questionnaire according to the KAB theory.
4.3 Encouraging more compliance of the patients with multiple RF attempts
There is a general consensus that all AF patients who underwent RFCA should be followed up at a minimum of 3 months following the procedure. It is appropriate to prescribe oral anticoagulant before and to re-initiate it after the procedure [13]. Healthcare providers should encourage patients to monitor their pulse for irregularity, and this may serve as an initial screening tool for asymptomatic AF episodes [11].
Doctors and nurses should pay close attention to self-management behaviors in AF patients who undergo RFCA. Unfortunately, our study suggests that AF patients have poor adherence to monitoring behaviors such as periodic INR test, out-patient follow up, and daily pulse examination. These findings are similar to the previous research [15]. Self-management strategies should especially target patients with multiple RF attempts, who were more likely to demonstrate low compliance behavior. One potential reason for low compliance might be their disappointment with the ‘failure’ of previous RFCA procedures, as people say, you persuade by reason and motivate through emotion. This was further supported by the study of Schneider and Cheslock [5]. They believe that emotions have a cognitive component, and they can be the predictors of behavior. In our study, these highly selected patients had lower behavior scores, but their knowledge scores were higher. It suggested that there was lack of consistency among knowledge, attitude and behavior in these patients. Nolte et al. found that statements of patients on stroke do not necessarily translate the knowledge into adequate behavior [12]. This is why more compliance should be encouraged in this subgroup of patients.
The other finding from our study was that knowledge and attitude were positive predictors of AF self-management behavior, which was consistent with the KAB theory. However, methods of how to ensure consistency among such patients’ KAB are yet to be explored.
5 Study limitations
The sample size of the patient population was relatively small and the data was collected from only one academic hospital of one geographical location. KAB might vary under different circumstances. This should be taken into consideration when interpreting our results. Moreover, self-management behavior was evaluated only by self-reporting. When interviewing, poor behavior to treatment regimens might tend to be underestimated and good behavior might tend to be overestimated. Further studies are necessary to address these limitations.
6 Conclusions
This study is the first to address the gap in our understanding of the KAB of AF patients undergoing RFCA. In addition, it has demonstrated that AF patients have knowledge deficits and there is a lack of consistency among their KAB. In order to establish a better attitude and self-management behavior, AF patients undergoing RFCA need comprehensive education by the KAB questionnaire they have finished according to the KAB theory. Moreover, further study is required to assess the effect by the KAB model healthcare education.
References
European Heart Rhythm Association; Heart Rhythm Society, Fuster, V., Rydén, L. E., Cannom, D. S., Crijns, H. J., et al. (2006). ACC/AHA/ESC 2006 guidelines for the management of patients with atrial fibrillation—executive summary: a report of the American College of Cardiology/American Heart Association task force on practice guidelines and the European Society of Cardiology committee for practice guidelines (writing committee to revise the 2001 guidelines for the management of patients with atrial fibrillation). Journal of the American College of Cardiology, 48, 854–906.
Zhou, Z. Q., Hu, D. Y., Chen, J., Zhang, R. H., Li, K. B., & Zhao, X. L. (2004). An epidemiological survey of atrial fibrillation in China. Zhonghua Nei Ke Za Zhi, 43, 491–494.
Chugh, S. S., Blackshear, J. L., Shen, W. K., Hammill, S. C., & Gersh, B. J. (2001). Epidemiology and natural history of atrial fibrillation: clinical implications. Journal of the American College of Cardiology, 37, 371–378.
Le Heuzey, J. Y., Paziaud, O., Piot, O., Said, M. A., Copie, X., Lavergne, T., et al. (2004). Cost of care distribution in atrial fibrillation patients: the COCAF study. American Heart Journal, 147, 121–126.
Schneider, B., & Cheslock, N. (2003). Measuring results: gaining insight on behavior change strategies and evaluation methods for environmental education, museum, health, and social marketing programs. San Francisco, CA: CoEvolution Institute.
Miller, N. H. (1997). Compliance with treatment regimens in chronic asymptomatic diseases. The American Journal of Medicine, 102, 43–49.
Protheroe, J., Fahey, T., Montgomery, A. A., & Peters, T. J. (2000). The impact of patients’ preferences on the treatment of atrial fibrillation: observational study of patient-based decision analysis. BMJ, 320, 1380–1384.
McCabe, P. J., Schad, S., Hampton, A., & Holland, D. E. (2008). Knowledge and self-management behaviors of patients with recently detected atrial fibrillation. Heart & Lung, 37, 79–90.
Lane, D. A., Ponsford, J., Shelley, A., Sirpal, A., & Lip, G. Y. (2006). Patient knowledge and perceptions of atrial fibrillation and anticoagulant therapy: effects of an educational intervention programme. The West Birmingham atrial fibrillation project. International Journal of Cardiology, 110, 354–358.
Munschauer, F. E., 3rd, Sohocki, D., Smith Carrow, S., & Priore, R. L. (2004). A community education program on atrial fibrillation: implications of pulse self-examination on awareness and behavior. Journal of Stroke and Cerebrovascular Diseases, 13, 208–213.
European Heart Rhythm Association (EHRA); European Cardiac Arrhythmia Scoiety (ECAS); American College of Cardiology (ACC); American Heart Association (AHA); Society of Thoracic Surgeons (STS), Calkins, H., et al. (2007). HRS/EHRA/ECAS expert consensus statement on catheter and surgical ablation of atrial fibrillation: recommendations for personnel, policy, procedures and follow-up: a report of the Heart Rhythm Society (HRS) task force on catheter and surgical ablation of atrial fibrillation. Heart Rhythm, 4, 816–861.
Nolte, C. H., Rossnagel, K., Jungehuelsing, G. J., Müller-Nordhorn, J., Roll, S., Reich, A., et al. (2005). Gender differences in knowledge of stroke in patients with atrial fibrillation. Preventive Medicine, 41, 226–231.
Scholten, M. F., Thornton, A. S., Mekel, J. M., Koudstaal, P. J., & Jordaens, L. J. (2005). Anticoagulation in atrial fibrillation and flutter. Europace, 7, 492–499.
Protheroe, J., Fahey, T., Montgomery, A. A., & Peters, T. J. (2000). The impact of patients’ preferences on the treatment of atrial fibrillation: observational study of patient based decision analysis. BMJ, 320, 1380–1384.
Hu, D., & Sun, Y. (2008). Epidemiology, risk factors for stroke, and management of atrial fibrillation in China. Journal of the American College of Cardiology, 52, 865–868.
Acknowledgments
The authors gratefully acknowledge Haishan Wang, Fengxiang Zhang, Jing Wang, Weizu Ju, Yuan Tao, Qin Wang, Minqiong Cheng, Yan Zhou, Saijun Yang, Yin Wang, Hongyan Jia, Ting Gong, Chunxiang Li, Tianzhen Shi, Wei Yan, Qian Hu, and Qian Tang for their contribution to this study as data collectors. The authors also gratefully acknowledge Yanhui Sheng, Jiangang Zhou, Qijun Shan, Chun Chen, Rong Yang, and Xiujuan Zhou for their contribution to this study as questionnaire designers. Finally, we express our sincere gratitude to the patients who participated in this study.
Ethics
The study complies with the Declaration of Helsinki that the research protocol is approved by the ethics committee of the First Affiliated Hospital of Nanjing Medical University, and that the informed consent of the patients has been obtained.
Conflict of interest
None declared.
Funding
This work was supported by the Jiangsu Provincial Natural Science grant in China (grant number BK2005218).
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Author information
Authors and Affiliations
Corresponding author
Additional information
Wenhua Xu and Guozhen Sun contributed equally to this work.
Appendices
Appendix A. Knowledge survey of patients with AF undergoing RFCA
Directions: This questionnaire was to investigate the status of knowledge, attitude and behavior (KAB) in patients with atrial fibrillation (AF) who undergo radiofrequency catheter ablation (RFCA). The result is essential for guiding future research and providing a foundation for interventions to promote effective self-management on AF patients. As each person’s ideas and practices vary, there is no right and wrong answers. Please fill the questionnaire according to your real feeling and situation. Thank you for participating in this survey.
-
01
Do you know what types of problems AF can cause (or what were potential hazards of AF)? (Yes/No)
-
02
Do you know what the symptoms of AF are? (Yes/No)
-
03
Do you know therapeutic strategies of AF? (Yes/No)
-
04
Do you know the purpose of therapy for AF? (Yes/No)
-
05
Should warfarin/aspirin/other anti-platelet medication be taken by patients with AF? (Yes/No/Unknown)
-
06
Do you know the benefits of taking warfarin/aspirin/other anti-platelet medication? (Yes/No)
-
07
Do you know if there are any side effects of taking warfarin/aspirin/other anti-platelet medication? (Yes/No)
-
08
Do you know the purpose of monitoring INR? (Yes/No)
-
09
Do you know what the target of INR controlling is? (Yes/No)
-
10
Does it necessary to monitor INR when taking warfarin? (Yes/No/Unknown)
-
11
Are you able to name some Vitamin K-contained products? (Yes/No)
-
12
Do you know what kind of food can affect INR level? (Yes/No)
-
13
Do you know what kind of medication can affect INR level? (Yes/No)
-
14
Do you know any signs/symptoms caused by excessive anticoagulation? (Yes/No)
-
15
Do you know the impact of emotion on AF? (Yes/No)
-
16
Do you know the impact of smoking on AF? (Yes/No)
-
17
Do you know the impact of alcohol or caffeinated beverages on AF? (Yes/No)
-
18
Can the treatment efficacy of RFCA reach 100%? (Yes/No/Unknown)
-
19
Do you know the complications of RFCA? (Yes/No)
-
20
Should warfarin be taken within 3 months after RFCA? (Yes/No/Unknown)
-
21
Should medication for AF be taken within 3 months after RFCA? (Yes/No/Unknown)
-
22
Should periodic ECG monitoring be carried out after RFCA? (Yes/No/Unknown)
-
23
Do you know if you have any kind of signs/symptoms, then you need to consult a doctor or nurse? (Yes/No)
-
24
Do you know the normal pulse rate? (Yes/No)
-
25
Should self-examination of pulse be taken every day within 3 months after RFCA? (Yes/No/Unknown)
AF atrial fibrillation, INR international normalized ratio, RFCA radiofrequency catheter ablation
Appendix B. Attitude survey of patients with AF undergoing RFCA
-
01
I think AF is a serious disease.
-
02
I think AF will have serious complications if not treated.
-
03
I think AF will affect quality of life if not treated.
-
04
I am afraid that I might have the complications of AF someday.
-
05
I think AF episode could occur any time.
-
06
I am very easy to have AF episode.
-
07
Preventive medication saves more money than treatment of complications of AF.
-
08
Improving life style helps to cure disease.
-
09
Good compliance can reduce uncomfortable symptoms caused by AF.
-
10
AF can be improved and cured by proper treatment.
-
*11
If there is no embolic complication, it is unnecessary to take anticoagulant drugs.
-
*12
Taking medication on schedule is troublesome, it is convenient to take medication only when feeling uncomfortable.
-
*13
It is not necessary to receive any treatment after RFCA.
-
*14
It is a waste of time for periodic follow-up.
-
15
Discussing with doctors about AF helps a lot for my health condition.
-
16
The guidance of the medical staff is more reliable than the information provided by newspaper, television or other media.
-
17
I should take periodic follow-up and pulse monitoring in order to detect asymptomatic AF episodes and the health problems in early stage.
*11-14 were invert items, AF atrial fibrillation, RFCA radiofrequency catheter ablation
Appendix C. Behavior survey of patients with AF undergoing RFCA
-
01
Are you willing to take medication as many times per day as suggested by your doctor?
-
02
Are you willing to take medication according to the dosage suggested by your doctor?
-
03
Are you willing to take medication at the right time requested by your doctor?
-
04
Are you willing to take medication according to the treatment schedule suggested by your doctor?
-
05
Will you be able to have INR monitored on the requested dates?
-
06
Will you be able to attend regular follow-up on the requested dates?
-
07
I check pulse daily.
-
08
I quit or restrict smoking.
-
09
I restrict alcohol intake.
-
10
I have a reasonable diet according to my AF condition.
-
11
I take an adequate rest according to my AF condition.
-
12
I do appropriate exercise according to my AF condition.
-
13
I maintain a positive and stable emotion every day.
AF atrial fibrillation; INR international normalized ratio
Rights and permissions
Open Access This is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License (https://creativecommons.org/licenses/by-nc/2.0), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
About this article
Cite this article
Xu, W., Sun, G., Lin, Z. et al. Knowledge, attitude, and behavior in patients with atrial fibrillation undergoing radiofrequency catheter ablation. J Interv Card Electrophysiol 28, 199–207 (2010). https://doi.org/10.1007/s10840-010-9496-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10840-010-9496-2