
Abstract
Background
Atrial fibrillation (AF) is the most prevalent cardiac condition linked to increased mortality due to complications such as stroke. Oral anticoagulant (OAC) is the mainstay in preventing cerebrovascular accidents in patients with AF. Recent evidence identified gaps in physician’s knowledge in diagnosing and managing patients with AF. This study aims to assess Syrian physicians’ knowledge, attitude, and practices regarding the use of anticoagulant therapy in non-valvular AF (NVAF) patients. A cross-sectional study was conducted using a validated web-based questionnaire, which included 56 items separated into four sections that collected information about demographics, knowledge, attitude, and practices. Chi-square and Kruskal Wallis were performed to analyze the statistical relationships between the knowledge, attitude, practice, and demographic variables.
Results
A total of 497 participants completed the survey, of which 62.6% were between the ages of 25 and 35. The average participant scores for knowledge, attitude, and practices were (48.18 ± 21.57), (81.54 ± 9.26), and (62.83 ± 12.42), respectively. Participants who demonstrated good understanding, a positive attitude, and good practices were 22.3%, 87.3%, and 25.4%, respectively. The fear of bleeding was identified as the most significant barrier to initiating anticoagulant medication in AF patients (55.5%). Doctors who attended training had a better knowledge score than those who did not (mean ± S.D. = 57.24 ± 20.7). Participants who stated that over 70% of their AF patients use aspirin received the highest attitude score (mean ± S.D = 86.98 ± 21.17). PhD participants reported higher practice scores than those with other educational backgrounds (mean ± S.D = 73.96 ± 11.3).
Conclusion
This research showed that primary care physicians in Syria had optimistic views regarding OAC therapy, suggesting that training interventions targeting physicians may lead to improvement in the treatment of patients with NVAF in Syria.
Similar content being viewed by others


Introduction
Atrial fibrillation (AF) is the most prevalent persistent arrhythmia, with more than 33 million globally diagnosed. Various severe cardiovascular and cerebrovascular complications, such as myocardial infarction, heart failure, stroke, and premature death, are linked to atrial fibrillation [1]. Globally, the incidence and prevalence rates of AF are increasing as the life expectancy for more people is rising. The prevalence of atrial fibrillation has tripled during the last 50 years. The number of patients diagnosed with AF in Asia by 2050 is expected to be at least 72 million, with 3 million people expected to suffer from strokes secondary to AF [2].
Numerous recognized cardiovascular risk factors, such as hypertension, valvular heart disease, and diabetes mellitus, have been identified as independent predictors of atrial fibrillation. Other risk factors include obesity, excessive alcohol consumption, male sex, and left ventricular hypertrophy. Thus, screening patients with these risk factors may be advantageous to diagnose AF before complications occur [3].
Although paroxysmal AF is linked with a slightly lower risk of stroke and systemic embolism in comparison to permanent AF, it is still accompanied by a high possibility of stroke incidence [4]. Paroxysmal AF and atrial arrhythmia, or atrial high-rate events (AHRE), may be identified via comprehensive screening utilizing equipment like pacemakers, implanted cardiac monitors, patches, or smartphones [5].
Atrial fibrillation patients have a high risk of morbidity and mortality due to ischemic stroke; as a result, stroke prevention in the case of non-valvular AF (NVAF) is a top concern for doctors, patients, and their families, as well as for society. Several approaches have been developed to prevent strokes [6]. The CHA2DS2-VASC score is the gold standard for stroke prediction in AF patients since the European Society of Cardiology (ESC) guidelines recommended in 2012 to use this score for stroke risk stratification [7].
Oral anticoagulation (OAC) therapy primarily prevents thromboembolic events and stroke in patients with NAVF [8]. In patients with AF, stroke risk reduction is prioritized when considering anticoagulant medications, and higher bleeding risk in favor of reducing stroke risk is usually accepted. However, patient preferences should be considered when deciding the type of OAC treatment [9].
Antiplatelet and vitamin K antagonists were the only options to prevent stroke in AF until 2009. However, vitamin K antagonists’ use limitations have been established, such as a narrow therapeutic index, serious interactions with food and other medications, and the need for monitoring. New OACs (NOAC) are easier to administer than warfarin since they are given at a constant dosage without frequent monitoring [10,11,12]. However, recent studies have shown that in patients with cardiovascular disease, the nonadherence rate to treatment may approach 50% after 12 months. Since NOACs’ anticoagulant action lasts only 12–24 h after each dose, poor adherence would put NOAC therapy at risk [13]
A recent study encompassing six European countries found that physicians needed to be more confident in handling anticoagulant medication in patients with complex AF and identified significant gaps in physicians’ Knowledge and abilities in all aspects of AF treatment [14]. Another study showed that the main factors for underusing vitamin K antagonists among patients were the lack of knowledge and comprehension [15]. In contrast, the significant concerns among physicians were uncertainty and the need for personalized decision-making. Providing decision-making tools and improving primary care-hospital cooperation might help atrial fibrillation patients adopt this crucial therapy option. Increasing physician knowledge will aid general practitioners in treating AF with anticoagulation in primary care facilities. If these obstacles are addressed and a shared care plan is developed, AF may be better managed within primary care [16].
This cross-sectional study aimed to assess Syrian physicians’ knowledge, attitude, and practice regarding the use of anticoagulant therapy in NVAF patients. The findings will contribute to the present knowledge and will be helpful for decision-makers and policymakers in guiding AF treatment.
Methods
Study setting and design
This online cross-sectional study was performed between 21 December 2022 and 3 February 2023. Each respondent was informed of the study objectives and the research team identification. Additionally, the right to withdraw from the study at any time and the total confidentiality of the personal information was assured, and the fact that only fully reported data would be analyzed. This study included cardiologists, other internists, consultants, and resident doctors within the general internal medicine department or its sub-specialties. Physicians who were unwilling to participate and practitioners from different specialties were excluded from this survey. The questionnaire was based on a previous study conducted in China [17].
The questionnaire was translated into Arabic to ensure complete comprehension of the items. The link for the Google form with the questionnaire was sent to respondents through social media platforms, such as WhatsApp, Facebook, and Telegram. Another source for collecting data was face-to-face interviews between data collectors and physicians within governmental and private hospitals. The minimal sample size was estimated by applying a single proportion of the population formula [n = [(Zα/2)2. P (1−P)]/d2]. With a 95% confidence level (Zα/2 = 1.96), and a 5% margin of error, the KAP level was assumed at 50% to ensure the largest sample size. The required sample size was 385. However, we enrolled 498 participants in this study.
Measures
A modified and validated KAP questionnaire model developed by Ye et al. was used as a measurement tool 15. The questionnaire of this study included 56 items divided into four sections. The first part represented the demographic information of the study population and their previous experience in dealing with AF patients. The second, third, and fourth sections assessed knowledge, attitude, and practice toward anticoagulant therapy in patients with NVAF, respectively. Knowledge, attitude, and practice were rated as either poor (below 39.0%), average (40.0–69.0%), or good (above 70.0%), where these cut-off points were predetermined based on the prior study.
Practitioners’ demographics and their previous experience in dealing with AF patients
Overall, this domain contained 19 questions. We obtained the main properties of the study’s respondents by asking them 13 questions about their sociodemographics, including age, gender, academic specialty, number of years of work experience, and professional title. The participant’s monthly income was defined as poor, moderate, good and excellent if it was < 30%, between 30 and 50%, between 50 and 80% and > 80% of the area median income, respectively. In this part, participants were also asked six questions about their previous experience in dealing with AF patients, including the total number and age of the AF patients they have managed in the past year, the main obstacles of starting anticoagulant therapy in their AF patients, and whether their AF patients were treated with aspirin or warfarin.
Knowledge regarding anticoagulant therapy in patients with NVAF and the sources of information
Fourteen questions were included in this segment. We questioned the participants on issues such as AF diagnosis, the scores used to predict stroke risk and bleeding threat in AF patients, laboratory tests used to monitor AF patients treated with warfarin, the target range of International normalized ratio (INR) in AF patients managed with warfarin under 75 years old and above it, and about NOAC use. In the context of knowledge, participants were asked about their source of information concerning AF and the sources they prefer to use to gather knowledge about AF. Each knowledge item question scored one point for a correct answer and zero for an incorrect answer. The total knowledge score was computed by the addition of all score items.
Attitude toward anticoagulant therapy in patients with NVAF
This section included 13 questions to measure participants’ attitudes toward anticoagulant therapy in NVAF patients. Participants were investigated about their degree of agreement with the necessity of using the stroke score tool to calculate the risk of stroke in AF patients before anticoagulant therapy, the necessity of using the bleeding score tool to evaluate the risk of bleeding in AF patients before anticoagulant treatment, the need of understanding the risk of stroke and bleeding in AF patients, and the necessity to tell AF patients about medication and food that affect warfarin's anticoagulant effects. A 5-point Likert scale (1 = strongly disagree, 5 = strongly agree) was used to examine participants’ attitudes toward anticoagulant therapy in NVAF patients.
Practice toward anticoagulant therapy in patients with NVAF
We included 18 questions in this domain to evaluate practitioners’ experience dealing with non-valvular atrial fibrillation patients. This part showed different scenarios, and participants were asked to choose the appropriate management in each scenario. This part discussed issues such as the use of stroke risk score tools to assess stroke risk in AF patients, the use of bleeding risk score tools to assess bleeding risk in AF patients, informing the patient of the food and drugs that interact with warfarin, informing the patient of the increased risk of stroke related to AF. Respondents were also questioned about their previous attendance of training lectures about atrial fibrillation and anticoagulation therapy and their future desire to attend conferences on this topic. A 4-point scale (1 = never, 4 = always) was performed to measure participants' practice toward anticoagulant therapy in NVAF patients.
Pilot study
To confirm the validity and clarity of the survey, we administered it to 50 members of the public selected at random before accreditation. After performing pilot research and ensuring the questionnaire had strong internal consistency (Cronbach’s alpha was between 0.712 and 0.861), we distributed it.
Ethical considerations
The Syrian Ethical Society for Scientific Research provided ethical approval and Aleppo University provided ethical clearance. Participants were given a link to access an online Google survey, and on the first page of the survey, they were asked if they agreed to complete the questionnaire. Before completing the questionnaire, participants were sent to the linked page containing important research information. The questionnaire took five to twelve minutes to complete, and the responses were saved in a secure online database.
Statistical analysis
We used IBM Statistical Package for the Social Sciences (SPSS) Statistics ver.28 and Microsoft Excel ver.365 for the performance of statistical analysis, considering p-values equal to or below 0.05 as significant values. For continuous data (scores) that were not normally distributed according to the Shapiro–Wilk test, the Kruskal–Wallis was performed to determine the difference between the scores and basic variables. However, the chi-square test was used to reveal the difference between the categorical variables. In addition, we carried out binary logistic regression to define the actual probabilities of each subgroup having adequate levels of knowledge, attitude, and practices of anticoagulant therapy in patients with NVAF.
Results
Participant demographics
The respondents’ demographic data are summarized in Table 1. A total of 511 doctors were invited to participate in this study; however, 14 declined, reducing the final sample size to 497. Almost two-thirds of the participants (62.6%) were male, whereas most respondents (93.7%) were aged between 25 and 35. Less than half of the participants (47.5%) reported moderate monthly income, while 83.5% were residents’ doctors. 87.1% of the study sample reported less than five years of working experience. Nearly a third of respondents (34.0%) indicated they had attended training courses in their specialty. Just 11.3% of participants stated they had 20–49 AF patients in the past year; 20.5% stated 40–69% of their patients take aspirin. Lastly, 10.4% of participants revealed that 20–39% of their AF patients take warfarin.
Participant’s knowledge assessment
Most participants knew how to diagnose AF, and 74.6% knew the tool that could be used to predict stroke risk in AF patients. Most respondents (81.7%) indicated the correct risk factors included in the CHADS2 score, while 21.3% did not. Approximately, 36.4% and 75.9% of respondents did not recognize the risk factors “Hypertension, Abnormal renal/liver function, Stroke, Bleeding history or predisposition, Labile INR, Elderly, Drugs/alcohol concomitantly” (HAS-BLED) score included and how long coagulation function should be monitored in AF patients with long-term warfarin therapy at a stable period, respectively. The target range of INR in AF patients with warfarin under 75 years old and the target range of INR in AF patients over 75 years old were identified among 42.9% and 45.7% of respondents, respectively. Most respondents (90.5%) and (94.2%) replied correctly about the factor that is susceptible to the anticoagulation effect of warfarin and the antagonist that antagonizes warfarin’s anticoagulation, respectively (Table 2).
Most participants (85.7%) reported that electrocardiogram (ECG) made the diagnoses of AF, while 13.7% were done by Holter. 23.5% and 33% of respondents did not know the tool used to predict stroke risk in AF patients and can be used to predict bleeding risk in AF patients, respectively. Hypertension and diabetes were identified by 71% and 55.5% of respondents as risk factors in the CHADS2 score and CHADS2-VASc score, respectively. Only 3% of the participants used the Outcomes Registry for Better Informed Treatment of Atrial Fibrillation (ORBIT) score to predict bleeding risk in AF patients. Most of the respondents (83.5%) addressed INR as an indicator that should be monitored in AF patients with warfarin; however, 19.9% of respondents expressed that every seven days, the period coagulation function should be monitored in AF patients with long-term warfarin therapy at a stable period. A portion (42.9%) of participants thought the target range of INR in AF patients taking warfarin under 75 years of age was 2.0–3.0. Nearly two-thirds of respondents, 62.8%, identified food as a factor that is susceptible to the anticoagulation effect of warfarin (Table 3).
Participant attitude assessment
A total of 18.3% of the participants strongly agreed the type of AF would affect the doctor's initiation of anticoagulant therapy and choice of oral anticoagulants. In comparison, 12.9% and 11.1% didn’t agree if it is necessary to use the stroke score tool to assess the risk of stroke in AF patients before anticoagulant therapy and if it is essential to use the bleeding score tool to measure the risk of bleeding in AF patients before anticoagulant treatment. Of the respondents, only 26.6% disagreed and were not more concerned about the risk of bleeding in AF patients than the risk of stroke in AF patients.
Reducing the risk of stroke and bleeding caused by AF is critical for AF patients, according to more than half of the respondents (56.7%). Of the participants, 6.2%, 2.0%, and 4.0% reported their disagreement that it is safe to maintain the INR between 2.0 and 3.0 for warfarin anticoagulation therapy in NVAF patients; that it is necessary to tell AF patients about medication and food that affect warfarin's anticoagulant effects, and they fully understand the views of AF patients on reducing the risk of stroke and bleeding caused by warfarin therapy, respectively. Finally, 53.7% and 63.8% of respondents addressed strongly they hope to have more Knowledge to discuss the advantages and disadvantages of stroke, bleeding risk, and anticoagulation, and they think doctors can improve the standard anticoagulant treatment rate in AF patients after training in atrial fibrillation, respectively (Table 4).
Participant’s practices assessment
Only 38% of participants have never made a differential diagnosis according to the duration of the onset of atrial fibrillation. On the other hand, 22.5% and 20.9% indicated they sometimes made differential diagnoses between valvular AF and non-valvular AF in AF patients when they dealt with AF and used stroke risk score tools to assess stroke risk in AF patients, respectively. Moreover, 32.4% of respondents stated they often use bleeding risk score tools to evaluate bleeding risk in AF patients. Additionally, 36.4% of respondents reported they sometimes would give warfarin for anticoagulant treatment to a 75-year-old male NVAF patient with hypertension and no history of diabetes and cardiovascular disease.
A proportion of 32.8% stated they would not provide the AF patient who had gastrointestinal bleeding three months ago and has stopped bleeding for 1-week oral anticoagulant therapy, whereas 38.8% expressed they would never give warfarin to the AF patient whose nose bleeds once and gum occasionally bleeds when brushing his teeth. Furthermore, 32.6% of participants expressed that the AF patient with coronary stent implantation for one month should often give antiplatelet and warfarin therapy (Table 5).
Participant’s knowledge, attitude, and practice scores
Less than half of the participants (42.5%) reported poor knowledge grade. Most respondents (87.3%) reported a good attitude, whereas 68.6% indicated a fair practice grade. The mean score and standard deviation for knowledge, attitude, and practice were (48.18 ± 21.57), (81.54 ± 9.26), and (62.83 ± 12.42), respectively (Table 6).
Barriers and obstacles to starting OAC
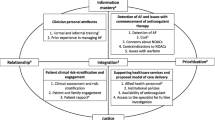
The main obstacle to starting anticoagulant treatment in AF patients identified by participants was the fear of the risk of bleeding (55.5%) participants; however, monitoring coagulation function tests, drug-drug interactions, and fees of coagulation were identified by 48.1%, 44.7%, and 41.2%, respectively of respondents. Regarding the significant barrier affecting AF patients' compliance, fees of coagulation were reported by 77.5% of respondents. However, monitoring coagulation function tests, lack of medications, and fear of the risk of bleeding were indicated by 51.3%, 49.1%, and 44.3%, respectively (Fig. 1).

The main obstacles for starting OAC therapy and barriers affecting patients’ compliance
Demographic factors and participant’s knowledge
From the total participants, 25.6% of males showed poor knowledge, whereas 14.9% of females showed fair knowledge. A good understanding was identified among 17.9% of those who live in the city, 11.5% of those with moderate monthly income, and 16.3% of singles. 35.4% of residents, 38.6% of participants with less than five years of practice, and 34.2% of those who didn’t attend training reported poor knowledge. 11.3% of Participants with 1–9 AF patients in the past year indicated fair awareness. Good awareness was noticed among 6.8% of respondents who stated their AF patients aged 60–69 years, while 11.9% of participants who addressed 40–69% of their AF patients taking aspirin showed fair knowledge (Table 7). Doctors who attended training had a better knowledge score than those who did not (mean ± S.D. = 57.24 ± 20.7).
Demographic factors and participant’s attitude
A good attitude was identified among 55.3% of males and 81.4% among those aged 20–35. 36.2% of participants had a good monthly income and 71.4% of singles reported good attitudes. A fair attitude was noticed among 11.3% of residents and 12.1% of those with less than 5 years of practice. 27.0% of participants with 1–9 AF patients in the past year indicated good attitude. Furthermore, a good attitude was noticed among 25.6% of respondents who stated their AF patients aged between 60 and 69 years, while 19.9% of participants who addressed 40–69% of their AF patients taking aspirin showed a good attitude. (Table 8). Participants who stated that over 70% of their AF patients use aspirin received the highest attitude score (mean ± S.D = 86.98 ± 21.17).
Demographic factors and participant’s practices
Only 4.6% of males showed poor practice, whereas 28.8% of females showed fair practice. Good practice was identified among 20.5% of those who live in the city, 11.1% of those with moderate monthly income, and 18.3% of singles. 61.8% of residents, 63.0% of participants with less than five years of practice, and 47.9% of those who didn’t attend training reported fair practice. 7.5% of Participants with 1–9 AF patients in the past year indicated good practice. Fair practice was noticed among 17.5% of respondents who stated their AF patients aged between 60 and 69 years, while only 3.6% of participants who addressed 40–69% of their AF patients taking aspirin showed good practice (Table 9). PhD participants reported higher practice scores than those with other educational backgrounds (mean ± S.D = 73.96 ± 11.3).
Factors associated with knowledge score
In the binary logistic regression analysis, out of fourteen variables, only six predictors were statistically significant for predicting adequate knowledge of primary care physicians (PCPs) in anticoagulant therapy for NVAF patients (p-value < 0.05). Females were less expected to have good Knowledge than males (OR = 0.525). Respondents aged 36–50 years were less likely to have good Knowledge than those aged between 20 and 35 (OR = 0.038). Participants attending training had higher odds of understanding 2.369 times than those who didn’t (Table 10).
Factors associated with attitude score
The Attitude of PCPs in anticoagulant therapy for NVAF patients was statistically correlated to two variables in the binary logistic regression analysis (p-value < 0.05). Participants with good practice grades were 5.872 times more likely to have a good attitude than those with bad\fair practice grades (Table 11).
Factors associated with practice score
We identified a statistically significant correlation between an adequate level of practice and four variables in the binary logistic regression (p-value < 0.05). Physicians were more likely to have good practice than residents (OR = 5.679). Participants who scored good knowledge grades had higher odds of having good practice than those with bad\fair knowledge grades (OR = 4.143) (Table 12).
Discussion
The risk of developing atrial fibrillation (AF) rises with age; it is the most common kind of cardiac arrhythmia affecting people over 60 [18]. According to the Global Burden of Disease Study findings conducted in 2010, more than one-third of all patients suffering from AF are above 80 [19].
The current study was aimed at evaluating Syrian physicians’ knowledge, attitude, and practice regarding the use of anticoagulant therapy in NVAF patients and how their demographic characteristics may significantly impact it. Overall, the study findings indicate that Syrian physicians showed suboptimal knowledge and understanding regarding the diagnosis of AF and screening of bleeding risk, where 35% had a fair knowledge score. Furthermore, the results suggested that younger participants and those attending training exhibited better knowledge. Additionally, higher knowledge scores correlated with better practice, while better practice scores were linked to better attitudes.
According to the study, a much lower percentage of Syrians diagnosed with AF sought medical care in community clinics than the expected number of Syrians who had AF. According to the survey results, 20.5% of physicians recommend aspirin to between 40 and 69% of their patients. This finding is particularly striking compared to the findings of a study in China, where 41.6% of primary care physicians employed aspirin as an OAC therapy for more than 70% of their NVAF patients. In addition, between 20 and 39% of those diagnosed with AF had reevaluation by 10.4% of the study's participants to initiate warfarin treatment. According to the findings of the Chinese research, however, just 0.4% of primary care physicians administered warfarin as an OAC medication to more than 70% of their patients who had NVAF [17]. This knowledge gap was further demonstrated in a recent study among physicians [20].
Elderly adults with AF need antithrombotic therapy to reduce the chance of a stroke Patients in the community diagnosed with NVAF should discuss with their PCPs the possibility of taking the anticoagulant warfarin [21]. The findings of this study show that PCPs have an insufficient grasp of the anticoagulant therapy options available for patients with NVAF. Despite this, most responders (87.3%) reported having a positive mindset. Our findings are corroborated by the results of another study, which found that 89.8% of PCPs there got excellent ratings in the survey’s component that measured attitude [17]. Moreover, an Iraqi study conveyed positive attitudes toward the use of OAC for NVAF patients, despite lacking in knowledge, further verifying the current study findings [22].
This study identified that not all PCPs knew how to identify AF, and some do not frequently utilize evaluation techniques to evaluate the relevant risks faced by patients with NVAF in their clinical practice. It was observed that patients with NVAF needed a greater understanding of such methods for calculating the risk of stroke and bleeding. Based on this observation, we concluded that the treatment of OAC therapy in patients with NVAF was not optimal.
Anticoagulant treatment with warfarin has several drawbacks including the impact of variability, which is connected to clinical and hereditary variables and drug-drug and drug-food interactions [23]. However, drug-drug interactions were found in 41.2% of the cases despite these limits, which are critical for patient education. This occurs less often than in research from China when 65.58% of PCPs gave incorrect answers to questions about the variables, genes, medicines, and nutrition that were likely to interact with warfarin [17].
Stroke and bleeding risk must be assessed before starting OAC therapy for NVAF. PCPs caring for patients with NVAF should weigh the risks of bleeding against the potential benefits of avoiding strokes when making treatment decisions. The best possible therapy choice may then be made. Even though the CHADS2-VASc score and the HAS-BLED score are crucial tools in generating such clinical judgments, most participants lacked an in-depth understanding of both measures. Therefore, we promote continued education among community-based PCPs, especially in using simple scoring systems to enhance clinical decision-making. In a recent study, PCPs admitted they utilized the HASBLED score and the CHA2DS2-VASc score to determine the patient’s risk of bleeding and stroke, which also affected their decision to start anticoagulants which agrees with the findings of the current study [24].
Our findings indicate that 68.6% of respondents reported being at an appropriate level of practice for their roles, and 87.3% said they had a positive attitude. Thus, most likely, a lack of education was to blame for the underuse of OAC in NVAF patients. The average score for practicality was 83.33, with chief medical officers and those with 20 + years of experience scoring higher than those with less experience.
The results of the current study highlight the impact of training on knowledge level, where it reveals that respondents who received training had better knowledge scores compared to those without. This is consistent with previous studies where education and training were proven essential for ensuring optimal AF therapy [20]. Furthermore, research has demonstrated the importance of the role of training in enhancing PCP, knowledge in AF management [16].
The current findings revealed that the main obstacle to initiating anticoagulant treatment in AF was the fear of bleeding risk while the major barrier to OAC compliance was found to be coagulation fees followed by monitoring coagulation function tests, which complies with previous reported evidence [22, 25].
Community hospital PCPs in urban and rural regions scored best in Knowledge, followed by their urban counterparts, and finally by their rural counterparts in the country's geographic center. Previous research conducted in China [17] demonstrates similar results. Central urban areas have more medical resources when comparing center urban regions to urban–rural intersections and rural areas [26]. On the other hand, in a previous study, PCPs working in rural regions had a higher practice score in comparison to those working in urban centers. This contradiction may be explained by the small number of PCPs in the mentioned study hindering the generalization of this finding [22].
As a result, many people with NVAF are encouraged by this aspect to seek care at the best facilities. Suburban residents have a low health literacy [27], which leaves primary care physicians in urban and rural regions with fewer patients suffering from NVAF. This might be why PCPs in the central urban and rural areas have lower average test results. However, there needs to be appropriate research conducted to explain these findings. Our study’s sample size may be increased to evaluate these elements better.
The current study and previous reports identifying physician prescribing patterns helps enforce the importance of clinical decision-making and physician knowledge in appropriate anticoagulant prescribing [28].
Limitations
This is the first cross-sectional observational research of KAPs for PCPs on OAC treatment in patients with NVAF in Syria. We included a suitable sample size to decrease bias and analysis errors. However, as our study design is cross-sectional, the limitations consisted of difficulty in making causal inferences, the determined analysis relationships might be difficult to interpret, and susceptibility to nonresponse and recall biases. Furthermore, the significant reliance on mainly social media platforms for data collection may have introduced selection bias since it excludes those who could not be reached through those platforms.
Conclusion
OAC treatment effectively prevented embolization in patients with NVAF due to the understanding and actions of PCPs. This study showed that PCPs in Syria who participated had optimistic views and attitudes, despite suboptimal knowledge. The results indicated that participants attending training demonstrated better knowledge suggesting that training interventions aimed at PCPs play a crucial role in improving the treatment of patients with NVAF. Furthermore, higher knowledge scores correlated with better practice, while better practice scores were linked to better attitudes.
Availability of data and material
The datasets used and analyzed during the current study are available from the corresponding author upon reasonable request.
Abbreviations
- AF:
-
Atrial fibrillation
- OAC:
-
Oral anticoagulant
- NVAF:
-
Non-valvular Atrial fibrillation
- KAP:
-
Knowledge, attitude, and practices
- AHRE:
-
Atrial high-rate events
- ESC:
-
European Society of Cardiology
- NOAC:
-
New oral anticoagulants
- INR:
-
International normalized ratio
- SPSS:
-
Statistical package for the social sciences
- CHADS2-VASc:
-
Congestive heart failure, hypertension, age ≥ 75 (doubled), diabetes, stroke (doubled), vascular disease score
- HAS-BLED:
-
Hypertension, abnormal renal/liver function, stroke, bleeding history or predisposition, labile INR, elderly, drugs/alcohol concomitantly
- ECG:
-
Electrocardiogram
- PCP:
-
Primary care physicians
- ORBIT:
-
Outcomes registry for better informed treatment of atrial fibrillation
References
Wijesurendra RS, Casadei B (2019) Mechanisms of atrial fibrillation. Heart 105(24):1860–1867. https://doi.org/10.1136/heartjnl-2018-314267
Kornej J, Börschel CS, Benjamin EJ, Schnabel RB (2020) Epidemiology of atrial fibrillation in the 21st century: novel methods and new insights. Circ Res 127(1):4–20. https://doi.org/10.1161/CIRCRESAHA.120.316340
Lau DH, Nattel S, Kalman JM, Sanders P (2017) Modifiable risk factors and atrial fibrillation. Circulation 136(6):583–596. https://doi.org/10.1161/CIRCULATIONAHA.116.023163
Morillo CA, Banerjee A, Perel P, Wood D, Jouven X (2017) Atrial fibrillation: the current epidemic. J Geriatr Cardiol 14(3):195–203. https://doi.org/10.11909/j.issn.1671-5411.2017.03.011
Jones NR, Taylor CJ, Hobbs FDR, Bowman L, Casadei B (2020) Screening for atrial fibrillation: a call for evidence. Eur Heart J 41(10):1075–1085. https://doi.org/10.1093/eurheartj/ehz834
Alkhouli M, Noseworthy PA, Rihal CS, Holmes DRJ (2018) Stroke prevention in nonvalvular atrial fibrillation: a stakeholder perspective. J Am Coll Cardiol 71(24):2790–2801. https://doi.org/10.1016/j.jacc.2018.04.013
Jagadish PS, Kabra R (2019) Stroke risk in atrial fibrillation: beyond the CHA(2)DS(2)-VASc score. Curr Cardiol Rep 21(9):95. https://doi.org/10.1007/s11886-019-1189-6
Raparelli V, Proietti M, Cangemi R, Lip GYH, Lane DA, Basili S (2017) Adherence to oral anticoagulant therapy in patients with atrial fibrillation. Focus on non-vitamin K antagonist oral anticoagulants. Thromb Haemost 117(2):209–218. https://doi.org/10.1160/TH16-10-0757
Wilke T, Bauer S, Mueller S, Kohlmann T, Bauersachs R (2017) Patient preferences for oral anticoagulation therapy in atrial fibrillation: a systematic literature review. Patient 10(1):17–37. https://doi.org/10.1007/s40271-016-0185-9
Xu Z-Q, Xu Z-H, Zhang N (2023) Comprehensive systematic review and meta-analysis on anticoagulants and aspirin for stroke prevention in non-valvular atrial fibrillation patients. Eur Rev Med Pharmacol Sci 27(22):11002–11012. https://doi.org/10.26355/eurrev_202311_34469
Çakmak T, Çakmak E, Balgetir F, Yaşar E, Karakuş Y (2023) Do novel oral anticoagulant drugs used in patients with nonvalvular atrial fibrillation act only as anticoagulants? Eur Rev Med Pharmacol Sci 27(7):2946–2952. https://doi.org/10.26355/eurrev_202304_31926
Mtwesi V, Amit G (2019) Stroke prevention in atrial fibrillation: the role of oral anticoagulation. Med Clin North Am 103(5):847–862. https://doi.org/10.1016/j.mcna.2019.05.006
Desteghe L, Kluts K, Vijgen J, Koopman P, Dilling-Boer D, Schurmans J, Dendale P, Heidbuchel H (2017) The health buddies app as a novel tool to improve adherence and knowledge in atrial fibrillation patients: a pilot study. JMIR Mhealth Uhealth 5(7):e98. https://doi.org/10.2196/mhealth.7420
Heidbuchel H, Dagres N, Antz M, Kuck K-H, Lazure P, Murray S, Carrera C, Hindricks G, Vahanian A (2018) Major knowledge gaps and system barriers to guideline implementation among European physicians treating patients with atrial fibrillation: a European Society of Cardiology international educational needs assessment. Europace 20(12):1919–1928. https://doi.org/10.1093/europace/euy039
Mas Dalmau G, Sant Arderiu E, Enfedaque Montes MB, Solà I, Pequeño Saco S, Alonso Coello P (2017) Patients’ and physicians’ perceptions and attitudes about oral anticoagulation and atrial fibrillation: a qualitative systematic review. BMC Fam Pract 18(1):3. https://doi.org/10.1186/s12875-016-0574-0
Ooi PC, Ramayah G, Omar SR, Rajadorai V, Nadarajah T, Ting CH, Teng CL (2021) Knowledge, attitude, and practice regarding atrial fibrillation among primary care physicians: the potential role of postgraduate training. Malays Fam Phys 16(1):39–49. https://doi.org/10.51866/oa0002
Ye S, Wang T, Liu A, Yu Y, Pan Z, Gu J (2020) A study of knowledge, attitudes, and practices of primary care physicians toward anticoagulant therapy in patients with non-valvular atrial fibrillation in Shanghai. China BMC Fam Pract 21(1):165. https://doi.org/10.1186/s12875-020-01236-4
Wang X, Zhang C (2022) Chinese expert consensus on the diagnosis and treatment of chronic heart failure in elderly patients (2021). Aging Med (Milton) 5(2):78–93. https://doi.org/10.1002/agm2.12215
Feigin VL, Forouzanfar MH, Krishnamurthi R, Mensah GA, Connor M, Bennett DA, Moran AE, Sacco RL, Anderson L, Truelsen T, O’Donnell M, Venketasubramanian N, Barker-Collo S, Lawes CMM, Wang W, Shinohara Y, Witt E, Ezzati M, Naghavi M, Murray C (2014) Global and regional burden of stroke during 1990–2010: findings from the Global Burden of Disease Study 2010. Lancet 383(9913):245–254. https://doi.org/10.1016/s0140-6736(13)61953-4
Li C, Meng Y, Meng X, Song Y (2023) Knowledge, attitude and practice toward oral anticoagulants among patients with atrial fibrillation. Front Cardiovasc Med. https://doi.org/10.3389/fcvm.2023.1301442
Ali A, Bailey C, Abdelhafiz AH (2012) Stroke prevention with oral anticoagulation in older people with atrial fibrillation—a pragmatic approach. Aging Dis 3(4):339–351
Alassi A, Al-Qerem W, Hameed AJL (2021) Iraqi primary care physician’s knowledge, attitudes, and practices (KAP) toward anticoagulant therapy in nonvalvular atrial fibrillation patients: a cross-sectional study. Pharmacologyonline 3:1385–1397
Carballo F, Albillos A, Llamas P, Orive A, Redondo-Cerezo E, Rodríguez de Santiago E, Crespo J (2022) Consensus document of the Spanish Society of Digestives Diseases and the Spanish Society of Thrombosis and Haemostasis on massive nonvariceal gastrointestinal bleeding and direct-acting oral anticoagulants. Revis Espanola de Enfermedades Dig 114(7):375–389. https://doi.org/10.17235/reed.2022.8920/2022
Chaterji S, Lian LG, Lee TY, Chua L, Wee SY-M, Yap SL, Tan NC (2021) Factors influencing primary care physicians’ prescribing behavior of anticoagulant therapy for the management of patients with non-valvular atrial fibrillation in Singapore: a qualitative research study. BMC Fam Pract 22(1):101. https://doi.org/10.1186/s12875-021-01453-5
Alshammari DA (2018) Assessment of family physician’s knowledge, attitude and barriers to the use of oral anticoagulation therapy among atrial fibrillation patients in Riyadh City. J Med Sci Clin Res 6(7):348–357. https://doi.org/10.18535/jmscr/v6i7.59
Loftus J, Allen EM, Call KT, Everson-Rose SA (2018) Rural-urban differences in access to preventive health care among publicly insured Minnesotans. J Rural Health 34(Suppl 1):s48–s55. https://doi.org/10.1111/jrh.12235
Chen X, Orom H, Hay JL, Waters EA, Schofield E, Li Y, Kiviniemi MT (2019) Differences in rural and urban health information access and use. J Rural Health 35(3):405–417. https://doi.org/10.1111/jrh.12335
Almalki AS, Al Recheq HA, Bajnaid E, Boraii S, Abdelaziz DH, El Hadidi S (2023) Prescribing patterns of thromboprophylaxis post-bariatric surgeries: no additional benefits of extended prophylaxis. Futur J Pharm Sci 9(1):18. https://doi.org/10.1186/s43094-023-00468-2
Acknowledgements
None.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Author information
Authors and Affiliations
Contributions
SS, YA, HB, and HA contributed to the conception and design of the study. MNN, NJ, AI, and BD collected, distributed, and organized the data sets. EM and SM analyzed the study data. BS and WH prepared the first draft of the manuscript. The final manuscript was revised by NOES and EAW. All the authors approved the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The Syrian Ethical Society for Scientific Research provided ethical approval. Ref. No.: HN/47-15 and consent was received from participants prior to study inclusion.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Swed, S., Bohsas, H., Alibrahim, H. et al. Assessing physicians’ knowledge, attitude, and practice on anticoagulant therapy in non-valvular atrial fibrillation: Syrian insights. Futur J Pharm Sci 10, 36 (2024). https://doi.org/10.1186/s43094-024-00595-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43094-024-00595-4