
Abstract
Purpose
We investigated the effect of different surgical procedures and radioactive iodine treatment (RAIT) on in vitro fertilization/intracytoplasmic sperm injection (IVF/ICSI) outcomes and evaluated whether possible risk factors, including age, thyroid-stimulating hormone (TSH) levels, and thyroid antibody positivity, were associated with adverse IVF/ICSI outcomes.
Methods
This retrospective study included 76 women with infertility who had received thyroid cancer (TC) treatment among 137,698 infertile women who underwent IVF/ICSI cycles at the Peking University Third Hospital between 2010 and 2019. Clinical pregnancy and live birth rates were assessed.
Results
We found that the clinical pregnancy and live birth rates in women who underwent partial thyroidectomy were 7- and 6-fold higher, respectively, than those in women who underwent total thyroidectomy. We observed no significant differences in the clinical pregnancy and live birth rates between the RAIT and non-RAIT groups, even after adjusting for age, TSH levels, surgical treatment, and thyroid antibody positivity. Multivariate logistic regression analysis showed that age and TSH levels were not associated with decreased clinical pregnancy and live birth rates. Women with thyroid antibody positivity had significantly lower clinical pregnancy and live birth rates than women without thyroid antibody positivity.
Conclusion
Our study showed lower clinical pregnancy and live birth rates in women who underwent total thyroidectomy than in women who underwent partial thyroidectomy. Thyroid antibody positivity is an important risk factor for adverse IVF/ICSI outcomes in women who have received TC treatment.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Several studies have demonstrated a significant association between reproductive factors and the risk of thyroid cancer (TC), and a higher prevalence of TC has been observed in women with infertility than in those without infertility [1,2,3]. For women with TC complicated by infertility, a careful balance between TC and assisted reproductive treatment is required. However, few studies have evaluated the impact of different TC treatments on in vitro fertilization/intracytoplasmic sperm injection (IVF/ICSI) outcomes.
Sufficient thyroid hormone secretion and a normal thyroid gland regulatory capacity are essential for follicular growth, pregnancy maintenance, and fetal development [4]. Both hyperthyroidism and hypothyroidism during pregnancy may be associated with adverse pregnancy outcomes [5]. Partial or total thyroidectomy combined with thyroid hormone suppression remains the standard treatment for patients with TC. A total or partial reduction in thyroid function after thyroidectomy and prolonged thyroid hormone-suppression therapy to reduce tumor recurrence may affect reproductive function and increase the risk of adverse pregnancy outcomes. The degree of thyroid function deficiency and thyroid hormone replacement dose differ between patients following total and partial thyroidectomy. Whether different surgical procedures trigger different pregnancy outcomes in women with TC remains unknown.
Except for thyroid function, an increasing number of recent studies began to focus on the impact of thyroid autoimmunity on the IVF/ICSI outcomes. Thyroglobulin, serving as a template and thyroid peroxidase, functioning as a key enzyme in thyroid hormone biosynthesis, constitutes the major thyroid autoantigens involved in the pathophysiology of thyroid autoimmunity [6]. Thyroid antibodies, mainly thyroid peroxidase antibody (TPOAb) and thyroglobulin antibody (TGAb), are important serum markers for diagnosing Hashimoto’s thyroiditis. The association between thyroid antibodies and IVF/ICSI outcomes has been demonstrated in some studies; however, the results are still controversial [7]. There are a few studies analyzing the effect of thyroid antibodies on IVF/ICSI outcomes in patients with TC although several studies have reported an increased risk of TC in patients positive for thyroid antibodies [8,9,10].
Radioactive iodine treatment (RAIT) after thyroidectomy is frequently used as an adjuvant therapy for the ablation of thyroid remnants. Although the 2017 American Thyroid Association guidelines recommend that pregnancy should be deferred for 6 months after RAIT, the results of studies that explored the correlation between RAIT and pregnancy outcomes are still controversial [5, 11,12,13]. Studies have reported that RAIT affects ovarian function and is associated with oligomenorrhea and early-onset menopause [14, 15]. However, the effect of RAIT on follicular development and IVF/ICSI outcomes remains unknown.
This study aimed to investigate the effect of different types of surgical procedures and RAIT on IVF/ICSI outcomes in women with TC and analyze whether possible risk factors, including age, thyroid-stimulating hormone (TSH) levels, and thyroid antibody positivity, were associated with adverse IVF/ICSI outcomes.
Materials and methods
Study population
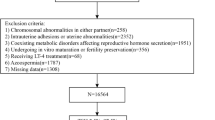
A total of 137,698 women with infertility underwent IVF/ICSI treatment at the Reproductive Center of the Peking University Third Hospital between January 2010 and August 2019. Excluding patients >45 years old or complicated with other cancers, this study included 76 women with both infertility and a history of thyroidectomy for TC who underwent their first IVF/ICSI cycle after the surgery (Fig. 1). All the women had a histological diagnosis of papillary thyroid carcinoma. After excluding 2 patients with no oocyte retrieved, 6 patients with no embryo obtained, 1 patient canceling cycle, and 3 patients with missing data, 64 women with successful embryo transfer were included in our analysis, who were divided into two groups based on a history of partial and total thyroidectomy (n=38 and 26 women, respectively); 11 of the 26 women who underwent total thyroidectomy received RAIT.

Flow chart of study cohort selection. IVF/ICSI, in vitro fertilization/intracytoplasmic sperm injection
IVF treatment
All women included in the study underwent a standardized ovarian stimulation regimen and oocyte retrieval and fertilization followed by planned fresh or frozen embryo transfer. We treated 7, 12, 4, 33, and 8 women with ultra-long, long-term, short-term, antagonist, and mini-stimulation protocols, respectively. Recombinant human chorionic gonadotropin (HCG) was administered to trigger oocyte maturation when the mean diameter of at least two follicles reached 18 mm. Oocyte retrieval was performed 34 to 36 h after HCG administration. Insemination was performed 4 to 6 h after oocyte retrieval through either conventional IVF or ICSI, depending on the sperm quality. High-quality day 3 embryos or blastocysts were transferred to the women 3 or 5 days after oocyte retrieval. Some women underwent frozen embryo transfers because of a high risk of ovarian hyperstimulation syndrome, high progesterone levels, or personal reasons.
Laboratory testing for thyroid function
Serum TSH, free thyroxine (FT4), thyroid peroxidase antibody (TPOAb), and thyroglobulin antibody (TGAb) levels were measured using a fully automated chemiluminescence immunoassay analyzer (ADVIA Centaur XP, Siemens Healthcare Diagnostics, Munich, Germany) before ovarian stimulation was performed. The TSH and FT4 reference values were 0.55–4.78 μIU/mL and 0.89–1.80 ng/dL, respectively. Based on the reference range provided by the manufacturer, TPOAb was defined as clinically positive at >60IU/mL, and TGAb was defined as clinically positive at >60IU/mL. In our study, patients positive for at least one of the thyroid antibodies were defined as thyroid antibody positivity. Of 64 patients in the TC group, 27 patients showed thyroid antibody positivity including 15 patients with co-positive for TPOAb and TGAb, 8 patients with isolated positive for TGAb, and 4 patients with isolated positive for TPOAb.
Study outcomes
The IVF/ICSI outcomes in women who underwent the first IVF cycle and achieved embryo transfer were analyzed. Clinical pregnancy was defined as at least 1 gestational sac in the uterus identified on ultrasonography 35 days after embryo transfer. Live birth was defined as the delivery of at least one newborn that exhibits any sign of life, irrespective of gestation duration.
Statistical analysis
Continuous and categorical variables are expressed as mean (standard deviation) and numbers (percentages), respectively. Student’s t-test and the chi-square test were used to compare differences in continuous and categorical variables, respectively, between the total and partial thyroidectomy groups. When continuous variables did not follow a Gaussian distribution, they were presented as median (interquartile range), and comparisons between groups were performed using the Mann–Whitney U test. To adjust for the relevant factors, multivariate logistic regression analysis was performed to calculate the odds ratios (ORs) with 95% confidence intervals (CIs). Results with a 2-tailed P-value <0.05 were considered significant. All statistical analyses were performed using SPSS version 24.0 (IBM corp., Armonk, NY).
Results
The baseline characteristics of the women who underwent total and partial thyroidectomy are shown in Table 1. There were no differences in age, body mass index, duration and types of infertility, causes of infertility, basal hormone levels, antral follicle count, FT4 levels, and thyroid antibody positivity rates between the two groups. However, we observed a significant difference in TSH levels between the two groups. TSH levels were significantly lower in women who underwent total thyroidectomy than in women who underwent partial thyroidectomy (median [interquartile range]: 0.3 [0.1–0.9] vs. 0.7 [0.2–1.4], P=0.04). Table 2 compares the controlled ovarian stimulation (COS) protocols and IVF and embryo transfer data between women who underwent total and partial thyroidectomy. There were no differences in the COS protocols, gonadotropin dose, number of COS days, HCG trigger day hormone levels, and number of good-quality embryos between the two groups. The number of retrieved oocytes was significantly lower in women who underwent total thyroidectomy than in women who underwent partial thyroidectomy (median [interquartile range]: 7.0 [6.0–11.3] vs. 10.5 [6.0–17.3], P=0.047).
A total of 22 women achieved clinical pregnancy, with no significant differences between the total and partial thyroidectomy groups (23.1% vs. 44.7%, P=0.076; Table 3). One patient in the partial thyroidectomy group had an early pregnancy abortion. No significant differences were observed in the live birth rates (23.1% vs. 42.1%, P=0.115; Table 3) between the total and partial thyroidectomy groups. However, after adjusting for age, TSH levels, RAIT, thyroid antibody positivity and protocols of COS, women who underwent partial thyroidectomy had 7- and 6-fold higher clinical pregnancy and live birth rates, respectively, than those who underwent total thyroidectomy (OR, 7.70 and 6.40; 95% CI, 1.22–48.77 and 1.02–40.34; P=0.030 and 0.048, respectively; Table 5).
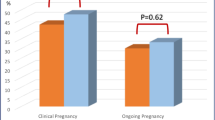
No significant difference was observed in clinical pregnancy and live birth rates between the RAIT and non-RAIT groups (27.3% vs. 37.7% and 27.3% vs. 35.8%, P=0.732 and 0.735, respectively; Table 4) even after adjusting for age, TSH levels, surgical treatment, thyroid antibody positivity and protocols of COS (OR, 1.66 and 1.96; 95% CI, 0.18–15.61 and 0.20–18.91; P=0.660 and 0.559, respectively; Table 5).
Multivariate logistic regression analysis was performed to evaluate several factors associated with the IVF/ICSI outcomes in women who received TC treatment. The age and TSH levels showed no association with the clinical pregnancy and live birth rates (Table 5). Thyroid antibody positivity was an important risk factor for IVF/ICSI outcomes. Compared with women without thyroid antibody positivity, those with thyroid antibody positivity had significantly lower clinical pregnancy (OR, 0.22; 95% CI, 0.05–0.95; P=0.042).
Discussion
To the best of our knowledge, our study is the first to demonstrate the differences in IVF/ICSI outcomes between women who underwent total and partial thyroidectomy. After adjusting for age, TSH levels, thyroid antibody positivity, RAIT and protocols of COS, we found that clinical pregnancy and live birth rates were significantly lower in women who underwent total thyroidectomy than in those who underwent partial thyroidectomy. The mechanism triggering this difference remains unknown; however, hypothalamus-pituitary-thyroid (H-P-T) axis deficiency and hypocalcemia may be involved. Sufficient thyroid hormone availability is an essential regulator in fetal growth and development. Fetal demand for thyroid hormone during early pregnancy solely depends on the supply transferred from maternal thyroid hormone because the fetal thyroid gland is non-functional until the 18th week of pregnancy. Thus, the demand for thyroid hormone availability is significantly increased during early pregnancy. Human chorionic gonadotropin (HCG), produced specifically and rapidly in early pregnancy, stimulates the thyroid gland via binding to the TSH receptor, thereby triggering an elevation in serum FT4 levels and a subsequent feedback suppression in TSH concentration. The HCG-mediated thyroid response is an important way safeguarding the adequate thyroid hormone [16, 17]. Total ablation of thyroid gland in patients with total thyroidectomy leads to the damage in the H-P-T axis and the deficiency in the secretion of thyroid hormone and the feedback suppression of TSH, which may induce an imbalance in thyroid hormone availability. Aside from the H-P-T axis damage, hypocalcemia and vitamin D deficiency may also be associated with adverse IVF/ICSI outcomes. Filippo et al. reported a nearly 3-fold higher hypocalcemia risk in patients who underwent total thyroidectomy than in patients who underwent lobectomy [18]. Vitamin D plays a pivotal role in regulating calcium metabolism, and a recent study showed a significant association between postoperative hypocalcemia and low preoperative vitamin D levels in patients after total thyroidectomy [19]. Many studies have reported on the correlation between vitamin D deficiency and decreased clinical pregnancy and live birth rates after IVF/ICSI [20, 21]. Lower calcium and vitamin D levels in women with total thyroidectomy may be an important risk factor associated with IVF/ICSI outcomes, and appropriate calcium and vitamin D supplement doses may be considered before commencing IVF/ICSI treatment in women with TC.
RAIT is widely used for postsurgical TC treatment. Recently, an increasing number of studies have focused on the effect of RAIT on reproductive function and fertility in women of childbearing age. Ceccarelli et al. suggested that RAIT might contribute to follicular atresia and menopause induction [14]. A recent meta-analysis that included 22 studies demonstrated that RAIT negatively influenced the menstrual cycle in the first year after treatment but was not associated with diminished long-term fertility [22]. Several studies have reported a correlation between RAIT and pregnancy outcomes; however, the results are controversial. Wu et al. and Anderson et al. reported that RAIT did not affect the birth rate, while another cohort study found that RAIT was significantly associated with a lower successful delivery rate [11,12,13]. Recently, Kim et al. conducted a large-scale, nationwide cohort study that evaluated whether the interval between conception and RAIT was associated with an increased risk of adverse pregnancy outcomes. The study found that conception that occurred less than 6 months after RAIT was associated with higher congenital malformation and miscarriage risks; however, the association was not observed in the 6–11 month interval group [23]. There are no studies that have reported an appropriate interval between RAIT and IVF/ICSI treatment. In our study, all women underwent IVF/ICSI treatment more than 6 months after RAIT, and we identified no significant correlation between RAIT and lower clinical pregnancy and live birth rates. Thus, based on our findings, IVF/ICSI treatment may be ideal for women who have previously undergone RAIT when IVF/ICSI treatment is performed more than 6 months after RAIT.
Our multivariate logistic regression analysis showed that the presence of thyroid antibody positivity was significantly associated with decreased clinical pregnancy rates in women with TC treatment. Some studies have reported that patients with thyroid antibody positivity were more likely to develop TC. For example, Qin et al. reported a higher prevalence of elevated TGAb and TPOAb in patients with TC than in those with benign thyroid nodules [8]. Another prospective study recruited 2100 patients with thyroid nodules and reported a significantly increased OR of raised TGAb levels in the presence of TC, further conferring TGAb with a role in predicting the TC risk [24]. Kratky et al. and Wong et al. reported a significant association between thyroid antibodies including TPOAb and TGAb and the risk of TC based on the patients after fine needle aspiration biopsy of thyroid nodule and identified thyroid antibody positivity as a risk factor of malignancy [9, 10]. Although no studies have evaluated the impact of thyroid antibodies on IVF/ICSI outcomes in infertile women with TC, several studies have demonstrated an association between the presence of thyroid antibodies and IVF/ICSI outcomes in women with infertility. Karacan et al. analyzed the ICSI outcomes in 253 women undergoing ICSI-embryo transfer cycles and found that the presence of thyroid antibodies did not affect the ICSI outcome in euthyroid and antiphospholipid antibody-negative women [25]. In a meta-analysis that included 12 studies, Busnelli et al. provided a comprehensive analysis of the association between thyroid antibody positivity and IVF/ICSI outcomes [7]. They concluded that the presence of thyroid antibodies had a detrimental effect on pregnancy outcomes, with an increased miscarriage risk and a decreased live birth frequency. Our study is the first to provide evidence that thyroid antibody positivity is an independent risk factor for adverse IVF/ICSI outcomes in women with TC treatment. However, the mechanism through which thyroid antibodies affect pregnancy outcomes remains unclear. Our previous study demonstrated that treatment with levothyroxine did not reduce the miscarriage rates or increase the clinical pregnancy and live birth rates of women undergoing IVF-ET who had normal thyroid function and tested positive for thyroid autoantibodies [26]. Dysfunctions in immunological regulation may be involved in the mechanism and should be explored further [27].
This study had several strengths. To date, this study investigates the largest number of infertile patients with TC who underwent IVF/ICSI treatment. Second, to the best of our knowledge, this is the first study to evaluate the association between TC treatment and IVF/ICSI outcomes. The major limitation is the retrospective design of this study, which may cause information bias. The thyroid hormone and TSH levels during the period of pregnancy were not obtained. Further prospective studies with a larger sample size are required to confirm these findings. In conclusion, this study evaluated the effects of different types of surgical procedures and RAIT on IVF/ICSI outcomes and analyzed the possible risk factors associated with adverse IVF/ICSI outcomes in women with TC treatment. Our study showed that clinical pregnancy and live birth rates were lower in women who underwent total thyroidectomy than in women who underwent partial thyroidectomy. Our study suggests that clinicians should carefully consider an optimal surgical procedure for women of childbearing age with TC. However, we found that RAIT did not affect IVF/ICSI outcomes if the IVF/ICSI treatment occurred more than 6 months after RAIT. Furthermore, our study showed that thyroid antibody positivity was an independent risk factor for adverse IVF/ICSI outcomes.
Data Availability
The datasets used or analyzed during the current study are available from the corresponding author on reasonable request.
References
Zamora-Ros R, Rinaldi S, Biessy C, Tjønneland A, Halkjaer J, Fournier A, et al. Reproductive and menstrual factors and risk of differentiated thyroid carcinoma: the EPIC study. Int J Cancer. 2015;136:1218–27.
Ding DC, Chen W, Wang JH, Lin SZ, Sung FC. Thyroid cancer risk in women with infertility and association with fertility medications in Taiwan. Cancer. 2019;125:1701–8.
Shin S, Sawada N, Saito E, Yamaji T, Iwasaki M, Shimazu T, et al. Menstrual and reproductive factors in the risk of thyroid cancer in Japanese women: the Japan Public Health Center-Based Prospective Study. Eur J Cancer Prev. 2018;27:361–9.
Krassas GE, Poppe K, Glinoer D. Thyroid function and human reproductive health. Endocr Rev. 2010;31:702–55.
Alexander EK, Pearce EN, Brent GA, Brown RS, Chen H, Dosiou C, et al. Guidelines of the American Thyroid Association for the diagnosis and management of thyroid disease during pregnancy and the postpartum. Thyroid. 2017;27:315–89.
Carvalho DP, Dupuy C. Thyroid hormone biosynthesis and release. Mol Cell Endocrinol. 2017;458:6–15.
Busnelli A, Paffoni A, Fedele L, Somigliana E. The impact of thyroid autoimmunity on IVF/ICSI outcome: a systematic review and meta-analysis. Hum Reprod Update. 2016;22:793–4.
Qin J, Yu Z, Guan H, Shi L, Liu Y, Zhao N, et al. High thyroglobulin antibody levels increase the risk of differentiated thyroid carcinoma. Dis Markers. 2015;2015:648670.
Krátký J, Ježková J, Kosák M, Vítková H, Bartáková J, Mráz M, et al. Positive antithyroid antibodies and nonsuppressed TSH are associated with thyroid cancer: a retrospective cross-sectional study. Int J Endocrinol. 2018;2018:9793850.
Wong SL, Grodski S, Yeung MJ, Serpell JW. Anti-thyroid antibodies as a predictor of thyroid cancer. ANZ J Surg. 2015;85:849–53.
Wu JX, Young S, Ro K, Li N, Leung AM, Chiu HK, et al. Reproductive outcomes and nononcologic complications after radioactive iodine ablation for well-differentiated thyroid cancer. Thyroid. 2015;25:133–8.
Anderson C, Engel SM, Weaver MA, Zevallos JP, Nichols HB. Birth rates after radioactive iodine treatment for differentiated thyroid cancer. Int J Cancer. 2017;141:2291–5.
Ko KY, Yen RF, Lin CL, Cheng MF, Huang WS, Kao CH. Pregnancy outcome after I-131 therapy for patients with thyroid cancer: a nationwide population-based cohort study. Medicine (Baltimore). 2016;95:e2685.
Ceccarelli C, Bencivelli W, Morciano D, Pinchera A, Pacini F. 131I therapy for differentiated thyroid cancer leads to an earlier onset of menopause: results of a retrospective study. J Clin Endocrinol Metab. 2001;86:3512–5.
Sawka AM, Lakra DC, Lea J, Alshehri B, Tsang RW, Brierley JD, et al. A systematic review examining the effects of therapeutic radioactive iodine on ovarian function and future pregnancy in female thyroid cancer survivors. Clin Endocrinol. 2008;69:479–90.
Hershman JM. Physiological and pathological aspects of the effect of human chorionic gonadotropin on the thyroid. Best Pract Res Clin Endocrinol Metab. 2004;18:249–65.
Korevaar TIM, Medici M, Visser TJ, Peeters RP. Thyroid disease in pregnancy: new insights in diagnosis and clinical management. Nat Rev Endocrinol. 2017;13:610–22.
Di Filippo L, Giugliano G, Tagliabue M, Gandini S, Sileo F, Allora A, et al. Total thyroidectomy versus lobectomy: surgical approach to T1-T2 papillary thyroid cancer. Acta Otorhinolaryngol Ital. 2020;40:254–61.
Bove A, Dei Rocini C, Di Renzo RM, Farrukh M, Palone G, Chiarini S, et al. Vitamin D deficiency as a predictive factor of transient hypocalcemia after total thyroidectomy. Int J Endocrinol. 2020;2020:8875257.
Zhao J, Huang X, Xu B, Yan Y, Zhang Q, Li Y. Whether vitamin D was associated with clinical outcome after IVF/ICSI: a systematic review and meta-analysis. Reprod Biol Endocrinol. 2018;16:13.
Lv SS, Wang JY, Wang XQ, Wang Y, Xu Y. Serum vitamin D status and in vitro fertilization outcomes: a systematic review and meta-analysis. Arch Gynecol Obstet. 2016;293:1339–45.
Piek MW, Postma EL, van Leeuwaarde R, de Boer JP, Bos AME, Lok C, et al. The effect of radioactive iodine therapy on ovarian function and fertility in female thyroid cancer patients: a systematic review and meta-analysis. Thyroid. 2021. https://doi.org/10.1089/thy.2020.0356.
Kim HO, Lee K, Lee SM, Seo GH. Association between pregnancy outcomes and radioactive iodine treatment after thyroidectomy among women with thyroid cancer. JAMA Intern Med. 2020. https://doi.org/10.1001/jamainternmed.2019.4644.
Azizi G, Keller JM, Lewis M, Piper K, Puett D, Rivenbark KM, et al. Association of Hashimoto’s thyroiditis with thyroid cancer. Endocr Relat Cancer. 2014;21:845–52.
Karacan M, Alwaeely F, Cebi Z, Berberoglugil M, Batukan M, Ulug M, et al. Effect of antithyroid antibodies on ICSI outcome in antiphospholipid antibody-negative euthyroid women. Reprod BioMed Online. 2013;27:376–80.
Wang H, Gao H, Chi H, Zeng L, Xiao W, Wang Y, et al. Effect of levothyroxine on miscarriage among women with normal thyroid function and thyroid autoimmunity undergoing in vitro fertilization and embryo transfer: a randomized clinical trial. JAMA. 2017;318:2190–8.
Min Y, Wang X, Chen H, Yin G. The exploration of Hashimoto’s thyroiditis related miscarriage for better treatment modalities. Int J Med Sci. 2020;17:2402–15.
Code availability
Not applicable.
Funding
This work was supported by the National Key R&D Program of China (Grant no. 2019YFC1005106) and National Natural Science Foundation of China (Grant no. 81871212).
Author information
Authors and Affiliations
Contributions
Ning Huang, Hongbin Chi, and Jie Qiao developed the conception and design of the study. Ning Huang participated in patient follow-up and wrote the initial draft of the paper. Ning Huang, Lin Zeng, and Jie Yan contributed to the data analysis. All authors contributed to the research discussion and manuscript revision. All authors listed have made a substantial, direct, and intellectual contribution to the work and approved it for publication.
Corresponding authors
Ethics declarations
Ethics approval
The study was approved by the Peking University Third Hospital Medical Science Research Ethics Committee (Approval Number: M2020567).
Consent to participate
Approval for a waiver for written consent was obtained from the Peking University Third Hospital Medical Science Research Ethics Committee due to the retrospective nature of this study.
Consent for publication
This manuscript has not been published or presented elsewhere and is not under consideration by another journal. All study participants provided informed consent and approved it for publication.
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Huang, N., Zeng, L., Yan, J. et al. Impact of thyroid cancer treatment on assisted reproductive technology outcomes in women with infertility. J Assist Reprod Genet 38, 2121–2128 (2021). https://doi.org/10.1007/s10815-021-02204-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10815-021-02204-2