
Abstract
Purpose
The debate between off-pump coronary artery bypass grafting (OPCAB) and on-pump coronary artery bypass grafting (ONCAB) in diabetic patients remains. This meta-analysis aimed to investigate outcomes after OPCAB versus ONCAB for patients with diabetes.
Methods
Literature research was conducted up to December 2023 using Ovid Medline, EMBASE, and the Cochrane Library. Eligible studies were observational studies with a propensity-score analysis of OPCAB versus ONCAB. The primary outcomes were early mortality and mid-term survival. The secondary outcomes were cerebrovascular accidents, reoperation for bleeding, incomplete revascularization, myocardial infarction, low cardiac output, and renal replacement therapy.
Results
Our research identified seven observational studies with a propensity-score analysis enrolling 13,085 patients. There was no significant difference between OPCAB and ONCAB for early mortality, mid-term survival, myocardial infarction, low cardiac output, and renal replacement therapy. OPCAB was associated with a lower risk of cerebrovascular accidents (OR 0.43; 95% CI, 0.24–0.76, P = 0.004) and reoperation for bleeding (OR 0.60; 95% CI, 0.41–0.88, P = 0.009). However, OPCAB was associated with a higher risk of incomplete revascularization (OR 2.07; 95% CI, 1.60–2.68, P < 0.00001).
Conclusion
Among patients with diabetes, no difference in early mortality and mid-term survival was observed. However, OPCAB was associated with a lower incidence of morbidity, including cerebrovascular accidents and reoperation for bleeding.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
By 2030, the number of people with type 2 diabetes worldwide is expected to reach 7079 per 100,000 [1]. The increasing prevalence of type 2 diabetes is a global health concern. The atherosclerotic cardiovascular disease is the primary cause of death for individuals with diabetes [2]. About 25 to 40% of patients undergoing myocardial revascularization have diabetes [3]. They are a high-risk group for coronary artery bypass surgery (CABG) and percutaneous coronary intervention (PCI), who are more likely to suffer from complex coronary heart disease and have a higher incidence of postoperative adverse events than non-diabetic patients [4].
In patients with multi-vessel coronary artery disease and diabetes, CABG had a mortality benefit over PCI [5]. However, the debate between OPCAB and ONCAB has lasted over three decades [6]. OPCAB can avoid the use of cardiopulmonary bypass and reduce aortic manipulations, but the quality of coronary revascularization has been questioned. Previous studies showed that OPCAB has benefits in high-risk patients, including elderly patients and patients with low ejection fraction, but which type of CABG has a better prognosis in diabetic patients remains unclear. Many randomized controlled trials compared OPCAB and ONCAB in unselected patients. Still, few randomized controlled trials (RCT) have been conducted in patients with diabetes. Although two studies [7, 8] from the ROOBY trial reported early and mid-term results after OPCAB and ONCAB in diabetic patients, they were both post hoc analyses, and patients’ allocation conversion may influence the outcomes. Some observational studies comparing the two surgical techniques in diabetic patients have unbalanced preoperative baseline data, which reflected patient selection biases. When results from these non-randomized studies are included in meta-analyses, they should always be evaluated cautiously. A propensity-score analysis, including matching and covariate adjustment, is a powerful tool to strengthen causal inferences drawn from observational studies [9].
To determine whether OPCAB improves outcomes in diabetic patients compared with ONCAB, we performed a meta-analysis of observational studies using propensity-score analysis.
Methods
Search Strategy
This systematic review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 and AMSTAR (Assessing the methodological quality of systematic reviews) Guidelines [10, 11]. The study was preregistered at the International Prospective Register of Systematic Reviews (PROSPERO). We systematically searched the major databases through December 17, 2023, including Ovid MEDLINE, EMBASE, and the Cochrane Library, using keywords and Medical Subject Headings (MeSH). The search strategy included the following terms: “off-pump,” “Coronary Artery Bypass,” “CABG,” “coronary artery bypass graft,” and “Diabetes Mellitus”). (details about the complete search strategy are available in Supplemental Table 1).
Inclusion and Exclusion Criteria
The studies were screened by two authors independently, and any discrepancies regarding a study’s eligibility were resolved by discussion and consensus. The inclusion criteria were as follows: (1) studies comparing OPCAB versus ONCAB in diabetic patients; (2) studies using propensity-score analysis; (3) studies published with full available text in English. The exclusion criteria were as follows: (1) concomitant surgical interventions other than CABG; (2) reviews, letters, editorials, conference abstracts, and case reports.
Data Extraction and Quality Assessment
All data were extracted independently and crosschecked by two review authors. Any disagreements between the two authors were discussed until they reached a consensus. Disagreements were resolved by discussion with a third author when necessary. The following variables were included: study demographics (the lead author, publication year, observation period, study location, number of centers, design, and sample size); patient demographics; comorbidities (age, sex, hypertension, myocardial infarction history, ejection fraction, renal dysfunction); and outcomes. In case of discrepancies, they were resolved by consultation. The quality of the included papers was assessed using the Newcastle–Ottawa Scale [12].
Outcomes
The primary outcomes were early mortality and mid-term survival. Early mortality was defined as any cause of death within 30 days after surgery or before discharge. Mid-term was defined as a follow-up of at least more than 1 year. Secondary outcomes included the following: (1) cerebrovascular accident; (2) bleeding complications; (3) incomplete revascularization; (4) myocardial infarction; (5) renal replacement therapy; (6) low cardiac output.
Statistical Analysis
All statistical analysis was conducted using RevMan 5.3 software or R software. Random-effects models with inverse variance and Mantel–Haenszel were chosen, and odds ratios (OR) and hazard ratios (HR) with 95% confidence intervals (CIs) and P values (considered statistically significant when P < 0.05) were calculated and used to represent the results following analysis. The heterogeneity was evaluated by the chi[2] test and calculated by I2 statistic. Clinical outcomes were presented through the graphic presentation in Forest plots. Publication bias was also assessed through funnel plots. Subgroup analysis of the primary outcomes was performed according to the propensity score method (propensity score matching and propensity score covariate adjustment) adopted by the included studies.
Results
Study Characteristics
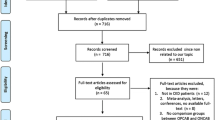
A total of 1119 records were identified through an initial search, and 7 trials [13,14,15,16,17,18,19] published between 2004 and 2023 were finally included (Fig. 1). Among the included studies, four used propensity-score matching, and three used propensity-score covariate adjustment. Overall, 6212 patients were treated with OPCAB, whereas 6873 were treated with ONCAB.

PRISMA flow diagram
The main characteristics of the included trials are shown in Table 1, and the baseline characteristics of the patients are summarized in Table 2. The mean age of the OPCAB participants varied from 59.9 to 70.0 years, whereas the mean age of the ONCAB participants ranged from 60.4 to 69.0 years. The percentage of female participants, hypertension, myocardial infarction history, renal disease, and the mean number of grafts are also shown in Table 2. The risk of bias assessment is shown in Supplemental Table 2.
Primary Outcomes
Except for one study without a definite follow-up period, six studies were included to compare the early mortality of patients with OPCAB versus ONCAB. There was no statistically significant difference in early mortality for OPCAB versus ONCAB (OR 0.68; 95% CI, 0.39–1.18, P = 0.17, I2 = 57%) among studies analyzed in propensity score matching (OR 0.84; 95% CI, 0.46–1.52, P = 0.56, I2 = 61%) and propensity score covariate adjustment (OR 0.27; 95% CI, 0.05–1.46, P = 0.13, I2 = 56%) (Fig. 2A).

Forest plot for early mortality (A) and mid-term survival (B)
Data from four studies with a more than 1-year follow-up also showed no difference in mid-term survival for OPCAB versus ONCAB (HR 0.99; 95% CI, 0.79–1.24, P = 0.94, I2 = 71%) (Fig. 2B).
Secondary Outcomes
Compared with the ONCAB group, OPCAB was associated with a lower risk of cerebrovascular accidents (OR 0.43; 95% CI, 0.24–0.76, P = 0.004, I2 = 0%) (Fig. 3A) and reoperation for bleeding (OR 0.60; 95% CI, 0.41–0.88, P = 0.009, I2 = 0%) (Fig. 3B). Pooled data from two propensity score matching showed OPCAB was associated with a higher risk of incomplete revascularization (OR 2.07; 95% CI, 1.60–2.68, P < 0.00001) (Fig. 3C).

Forest plot for cerebrovascular accidents (A), reoperation for bleeding (B), and incomplete revascularization (C)
There was no statistically significant difference in myocardial infarction (OR 0.70; 95% CI, 0.42–1.15, P = 0.16, I2 = 7%) (Fig. 4A); low cardiac output for OPCAB versus ONCAB (OR 0.68; 95% CI, 0.43–1.07, P = 0.09, I2 = 0%) (Fig. 4B); and renal replacement therapy (OR 0.75; 95% CI, 0.37–1.53, P = 0.44, I2 = 68%) (Fig. 4C).

Forest plot for myocardial infarction (A), low cardiac output (B), and renal replacement therapy (C)
Publication Bias
Only seven studies were included, so assessing them for publication bias seemed meaningless. Nevertheless, funnel plots were performed to show that studies presented a symmetric distribution, which indicated no obvious publication bias existed (Supplemental Fig. 1 and Fig. 2).
Discussion
In this meta-analysis of observational studies with a propensity-score analysis, we explored outcomes after OPCAB or ONCAB for patients with diabetes mellitus. The main findings can be summarized as follows: (1) there was no significant difference in early mortality and mid-term survival. (2) OPCAB was associated with a lower risk of cerebrovascular accident and reoperation for bleeding but with a higher risk of incomplete revascularization.
A previous meta-analysis reported that OPCAB was associated with superior early mortality in high-risk groups, including octogenarians, patients with left ventricular dysfunction, and patients with chronic kidney disease [20,21,22]. However, our result showed that OPCAB and ONCAB had similar early mortality in patients with diabetes. Of note, one study [14] did not mention follow-up time for death and was thus not included in the analysis. Sensitivity analysis was performed by including the data in the study and reanalyzing it, and the difference still did not reach statistical significance (P = 0.07).
Our study revealed that there was no difference in mid-term survival for OPCAB versus ONCAB. A previous meta-analysis, including 7 RCTs with more than 4 years of follow-up, showed that compared with OPCAB in unselected patients, ONCAB appeared to offer superior long-term survival [23]. However, the evidence was deemed unsuitable due to using OR instead of HR, between-study heterogeneity, and fixed-effect model instead of random-effect model [24, 25]. Our study used HR and a random-effect model to overcome these disadvantages. Taggart et al. [26] found that off-pump and on-pump techniques achieved comparable long-term outcomes. However, OPCAB performed by low-volume off-pump surgeons was associated with a lower number of grafts and increased cardiovascular death. Completeness of revascularization and graft patency are the two factors contributing to the outcomes of CABG [23, 27]. Our result showed that OPCAB was associated with a higher risk of incomplete revascularization. In a more extended follow-up period, it may lead to lower survival [28]. With the development of heart positioning devices and the enrichment of surgeons’ experience, complete revascularization can be achieved in OPCAB [29].
OPCAB achieves better in postoperative morbidities, including cerebrovascular accident and reoperation for bleeding. Several previous studies demonstrated that compared with ONCAB, the incidence of stroke after OPCAB was lower [29, 30]. OPCAB eliminates the need for aortic cannulation and cross-clamping [31]. Lorusso et al. [30] showed a strong association between aortic manipulation and neurological outcomes after CABG surgery. The retrospective, multicenter, international study included 25,388 patients and suggested that the majority of the published research on the relationship between postoperative stroke and aortic manipulation was likely to be underpowered due to the low incidence of stroke and limited sample size. Considering that diabetic patients have a higher incidence of stroke after myocardial reperfusion therapy [32], OPCAB may provide additional benefits for this particular population.
Our study showed that OPCAB reduced the risk of reoperation for bleeding after surgery. Reduction of platelet counts and platelet dysfunction was a cause of bleeding after cardiopulmonary bypass [33, 34]. In addition, OPCAB does not require the establishment of extracorporeal circulation, and fewer incisions and sutures mean a reduced risk of bleeding [35]. Previous studies in other high-risk patients also reported higher blood transfusion rates in the ONCAB group [21, 22].
A recent study showed that the elevation of postoperative cardiac biomarkers (creatine kinase-MB and troponin I) after ONCAB was significantly higher than after OPCAB. However, they were quite lower than the threshold values defining postoperative myocardial infarction [36], which might explain the lack of differences in myocardial infarction in this analysis. Our study showed no difference in low cardiac output syndrome for OPCAB versus ONCAB. In contrast to our findings, previous meta-analyses suggested that OPCAB was associated with a lower incidence of low cardiac output in both the general and the re-operative population [37, 38]. More research is needed to confirm the result.
Our study did not show a significant difference in renal replacement therapy for OPCAB versus ONCAB. Similarly, a previous meta-analysis found no difference in renal failure between the two techniques in diabetic patients [39]. This meta-analysis included three more studies [17, 40, 41] than ours, and two [17, 41] had worse preoperative renal function in the OPCAB group. Our study only included studies using propensity-score matching or covariate adjustment, which could effectively reduce confounding bias. Of note, previous studies showed that in patients with preoperative moderate or severe renal failure, OPCAB technology has a protective effect on early postoperative outcomes, including the need for dialysis [42, 43]. Still, the protective effect was not observed in patients with mildly reduced renal function [43]. Thus, preoperative renal function may influence the protective effect of OPCAB, which needs more randomized controlled trials to verify.
This meta-analysis included seven observational studies that used the propensity-score analysis. Compared with a single small sample study, the meta-analysis had better statistical power. The current study suggested that in diabetic patients who need to undergo CABG, the patient’s perioperative risks and long-term outcomes should be comprehensively evaluated when choosing a surgical plan. The doctor’s OPCAB experience and the cost of treatment should also be considered.
Limitation
Firstly, surgeon experience is vital for OPCAB. Since the number of surgeries performed by the surgeon was not provided in the included studies, subgroup analysis cannot be performed. Secondly, when comparing the mid-term mortality of OPCAB and ONCAB, data were from four studies due to the limited number of studies reporting long-term follow-up results. Despite the small number of studies, the results are still well-powered, considering that all included studies used a propensity-score analysis and the heterogeneity was low. We look forward to more studies with long-term follow-ups being published in the future. In addition, the subgroup analysis based on statistical design was not performed for mid-term survival because of the inclusion of only one propensity-score covariate adjustment study. Finally, due to the lack of grouping of preoperative renal function, subgroup analysis could not be performed to clarify whether preoperative renal function is related to the protective effect of OPCAB in diabetic patients.
Conclusion
OPCAB provides significant benefits in terms of early postoperative complications, including cerebrovascular events and reoperation for bleeding. Although OPCAB and ONCAB were comparable in terms of early mortality and mid-term survival, ONCAB was associated with a lower risk for incomplete revascularization. Our findings can provide a scientific rationale for planning the appropriate operative strategy for future CABG cases with diabetes.
Data Availability
Data are available from the corresponding author upon reasonable request.
Code Availability
Not applicable.
References
Khan M, Hashim MJ, King JK, Govender RD, Mustafa H, Al KJ. Epidemiology of type 2 diabetes-global burden of disease and forecasted trends. J Epidemiol Glob Health. 2020;10(1):107–11.
American Diabetes Association. 10. Cardiovascular disease and risk management: standards of medical care in diabetes-2021. Diabetes Care. 2021;44(Suppl 1):S125–S150.
Taggart DP, Audisio K, Gerry S, et al. Single versus multiple arterial grafting in diabetic patients at 10 years: the arterial revascularization trial. Eur Heart J. 2022;43(44):4644–52.
Milojevic M, Serruys PW, Sabik JR, et al. Bypass surgery or stenting for left main coronary artery disease in patients with diabetes. J Am Coll Cardiol. 2019;73(13):1616–28.
Head SJ, Milojevic M, Daemen J, et al. Mortality after coronary artery bypass grafting versus percutaneous coronary intervention with stenting for coronary artery disease: a pooled analysis of individual patient data. The Lancet (British edition). 2018;391(10124):939–48.
Gaudino M, Angelini GD, Antoniades C, et al. Off-pump coronary artery bypass grafting: 30 years of debate. J Am Heart Assoc. 2018;7(16):e009934.
Shroyer ALWP, Hattler BM, Wagner THP, et al. Comparing off-pump and on-pump clinical outcomes and costs for diabetic cardiac surgery patients. Ann Thorac Surg. 2014;98(1):38–45.
Shroyer A, Quin JA, Wagner TH, et al. Off-pump versus on-pump impact: diabetic patient 5-year coronary artery bypass clinical outcomes. Ann Thorac Surg. 2019;107(1):92–8.
McMurry TL, Hu Y, Blackstone EH, Kozower BD. Propensity scores: methods, considerations, and applications in the Journal of Thoracic and Cardiovascular Surgery. J Thorac Cardiovasc Surg. 2015;150(1):14–9.
Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017:j4008.
Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Int J Surg. 2021;88:105906.
Wells G, Shea B, O’Connell D, Peterson J, Welch V, Losos M. The NewcastleOttawa scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. Available at: https://www.ohri.ca/programs/clinical_epidemiology/oxford.asp. Accessed 11 Sept 2021.
Srinivasan AK, Grayson AD, Fabri BM. On-pump versus off-pump coronary artery bypass grafting in diabetic patients: a propensity score analysis. Ann Thorac Surg. 2004;78(5):1604–9.
Emmert MY, Salzberg SP, Seifert B, et al. Is off-pump superior to conventional coronary artery bypass grafting in diabetic patients with multivessel disease? Eur J Cardiothorac Surg. 2011;40(1):233–9.
Renner A, Zittermann A, Aboud A, et al. Coronary revascularization in diabetic patients: off-pump versus on-pump surgery. Ann Thorac Surg. 2013;96(2):528–34.
Benedetto U, Caputo M, Vohra H, et al. Off-pump versus on-pump coronary artery bypass surgery in patients with actively treated diabetes and multivessel coronary disease. J Thorac Cardiovasc Surg. 2016;152(5):1321–30.
Singh A, Schaff HV, Mori BM, et al. On-pump versus off-pump coronary artery bypass graft surgery among patients with type 2 diabetes in the bypass angioplasty revascularization investigation 2 diabetes trial. Eur J Cardiothorac Surg. 2016;49(2):406–16.
Huang K, Wu I, Chou N, et al. Late outcomes of off-pump versus on-pump coronary bypass in patients with diabetes: a nationwide study from Taiwan. J Thorac Cardiovasc Surg. 2019;157(3):960–9.
Song Y, Wang C, Tang C, et al. Off-pump vs. on-pump bypass surgery grafting in diabetic patients with three-vessel disease: a propensity score matching study. Front Cardiovasc Med. 2023;10:1249881.
Khan H, Uzzaman M, Benedetto U, Butt S, Raja SG. On- or off-pump coronary artery bypass grafting for octogenarians: a meta-analysis of comparative studies involving 27,623 patients. Int J Surg. 2017;47:42–51.
Guan Z, Guan X, Gu K, et al. Short-term outcomes of on- vs off-pump coronary artery bypass grafting in patients with left ventricular dysfunction: a systematic review and meta-analysis. J Cardiothorac Surg. 2020;15(1):84.
Wang Y, Zhu S, Gao P, Zhou J, Zhang Q. Off-pump versus on-pump coronary surgery in patients with chronic kidney disease: a meta-analysis. Clin Exp Nephrol. 2018;22(1):99–109.
Smart NA, Dieberg G, King N. Long-term outcomes of on- versus off-pump coronary artery bypass grafting. J Am Coll Cardiol. 2018;71(9):983–91.
Ma G, Fan Y, Shao W, Qi LW. Meta-analysis for the prognosis of on-pump versus off-pump coronary artery bypass grafting. J Am Coll Cardiol. 2018;72(3):344–5.
Shah R. Long-term survival with on-pump coronary artery bypass grafting. J Am Coll Cardiol. 2018;72(3):344.
Taggart DP, Gaudino MF, Gerry S, et al. Ten-year outcomes after off-pump versus on-pump coronary artery bypass grafting: insights from the arterial revascularization trial. J Thorac Cardiovasc Surg. 2021;162(2):591–9.
Yang L, Lin S, Zhang H, et al. Long-term graft patency after off-pump and on-pump coronary artery bypass: a coronary trial cohort. Ann Thorac Surg. 2020;110(6):2055–61.
Thakur U, Nerlekar N, Muthalaly RG, et al. Off- vs. on-pump coronary artery bypass grafting long-term survival is driven by incompleteness of revascularisation. Heart Lung Circ. 2020;29(1):149–55.
Wang C, Jiang Y, Song Y, et al. Off-pump or on-pump coronary artery bypass at 30 days: a propensity matched analysis. Front Cardiovasc Med. 2022;9:965648.
Lorusso R, Moscarelli M, Di Franco A, et al. Association between coronary artery bypass surgical techniques and postoperative stroke. J Am Heart Assoc. 2019;8(24):e013650.
Kowalewski MM, Pawliszak WM, Malvindi PGM, et al. Off-pump coronary artery bypass grafting improves short-term outcomes in high-risk patients compared with on-pump coronary artery bypass grafting: meta-analysis. J Thorac Cardiovasc Surg. 2016;151(1):60–77.
Gaba P, Sabik JF, Murphy SA, et al. Percutaneous coronary intervention versus coronary artery bypass grafting in patients with left main disease with and without diabetes: findings from a pooled analysis of 4 randomized clinical trials. Circulation. 2024;149(17):1328–38.
Ascione R, Williams S, Lloyd CT, Sundaramoorthi T, Pitsis AA, Angelini GD. Reduced postoperative blood loss and transfusion requirement after beating-heart coronary operations: a prospective randomized study. J Thorac Cardiovasc Surg. 2001;121(4):689–96.
Ballotta A, Saleh HZ, El Baghdady HW, et al. Comparison of early platelet activation in patients undergoing on-pump versus off-pump coronary artery bypass surgery. J Thorac Cardiovasc Surg. 2007;134(1):132–8.
Wang C, Jiang Y, Song Y, et al. Off-pump or on-pump coronary artery bypass at 30 days: a propensity matched analysis. Front Cardiovasc Med. 2022;9.
Matsuhashi K, Takami Y, Maekawa A, et al. Comparison between off-pump and on-pump beating heart coronary artery bypass grafting. Thorac Cardiovasc Surg. Published online February 9, 2024. https://doi.org/10.1055/a-2239-1810.
Sepehripour AH, Harling L, Ashrafian H, Casula R, Athanasiou T. Does off-pump coronary revascularization confer superior organ protection in re-operative coronary artery surgery? A meta-analysis of observational studies. J Cardiothorac Surg. 2014;9(1):115.
Zhang P, Wang L, Zhai K, et al. Off-pump versus on-pump redo coronary artery bypass grafting: a systematic review and meta-analysis. Perfusion. 2021;36(7):724–36.
Wang Y, Shi X, Du R, Chen Y, Zhang Q. Off-pump versus on-pump coronary artery bypass grafting in patients with diabetes: a meta-analysis. Acta Diabetol. 2017;54(3):283–92.
Abraham R, Karamanoukian HL, Jajkowski MR, et al. Does avoidance of cardiopulmonary bypass decrease the incidence of stroke in diabetics undergoing coronary surgery? Heart Surg Forum. 2001;4(2):135.
Magee MJ, Dewey TM, Acuff T, et al. Influence of diabetes on mortality and morbidity: off-pump coronary artery bypass grafting versus coronary artery bypass grafting with cardiopulmonary bypass. Ann Thorac Surg. 2001;72(3):776–81.
Rocha RV, Yanagawa B, Hussain MA, et al. Off-pump versus on-pump coronary artery bypass grafting in moderate renal failure. J Thorac Cardiovasc Surg. 2020;159(4):1297–304.
Ueki C, Miyata H, Motomura N, et al. Off-pump technique reduces surgical mortality after elective coronary artery bypass grafting in patients with preoperative renal failure. J Thorac Cardiovasc Surg. 2018;156(3):976–83.
Funding
This work was supported by the National Key R&D Project of China (2023YFC2706200); the National Key Research and Development Program of Guangzhou (Grant number: 202103000014); and the National Natural Science Foundation of China (Grant number: 82370271;82070297).
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. QR, YH, and ZW conceived and drafted the study. QR, GL, and CT analyzed and interpreted the data. QR, YH, and QL drafted the manuscript. KL and JP processed and beautified the pictures and tables. ZW critically revised the manuscript. All authors have approved the final draft of the manuscript.
Corresponding author
Ethics declarations
Ethics Approval
Not applicable.
Consent to Participate
Not applicable.
Competing Interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.


Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

{kind=link}
{kind=link}
Cite this article
Ren, Q., Li, G., Chu, T. et al. Off-pump Versus On-pump Coronary Artery Bypass Grafting in Diabetic patients: A Meta-analysis of Observational Studies with a Propensity-Score Analysis. Cardiovasc Drugs Ther (2024). https://doi.org/10.1007/s10557-024-07603-y
Accepted:
Published:
DOI: https://doi.org/10.1007/s10557-024-07603-y