
Abstract
Off-pump coronary artery bypass surgery (OPCAB) has been hypothesised to be beneficial in the high-risk patient population undergoing re-operative coronary artery bypass graft surgery (CABG). In addition, this technique has been demonstrated to provide subtle benefits in end-organ function including heart, lungs and kidney. The aims of this study were to assess whether OPCAB is associated with a lower incidence of major adverse cardiovascular and cerebrovascular events (MACCE) and other adverse outcomes in re-operative coronary surgery. Twelve studies, incorporating 3471 patients were identified by systematic literature review. These were meta-analysed using random-effects modelling. Primary endpoints were MACCE and other adverse outcomes including myocardial infarction, stroke, renal dysfunction, low cardiac output state, respiratory failure and atrial fibrillation. A significantly lower incidence of myocardial infarction, stroke, renal dysfunction, low cardiac output state, respiratory failure and atrial fibrillation was observed with OPCAB (OR 0.58; 95% CI (confidence interval) [0.39-0.87]; OR 0.37; 95% CI [0.17-0.79]; OR 0.39; 95% CI [0.24-0.63]; OR 0.14; 95% CI [0.04-0.56]; OR 0.36; 95% CI [0.24-0.54]; OR 0.41; 95% CI [0.22-0.77] respectively). Sub-group analysis using sample size, matching score and quality score was consistent with and reflected these significant findings. Off-pump coronary artery bypass grafting reduces peri-operative and short-term major adverse outcomes in patients undergoing re-operative surgery. Consequently we conclude that OPCAB provides superior organ protection and a safer outcome profile in re-operative CABG.
Similar content being viewed by others


Introduction
The outcome profile of off-pump coronary artery bypass surgery (OPCAB) has received much attention and analysis. Whilst recent randomised trials have popularly failed to demonstrate the beneficial effects of OPCAB in comparison to on-pump coronary artery surgery (ONCAB) with regards to mortality and major adverse cardiovascular and cerebrovascular events (MACCE), subtle benefits in end-organ function have been observed [1, 2]. However, the scepticism surrounding the external validity of these trials, regarding selective patient enrolment and individual surgeon’s OPCAB experience still remains [3], and has heralded the need for closer analysis of registry data, providing a closer ‘real-life’ representation of the population [4, 5].
Off-pump coronary artery bypass surgery has been demonstrated to reduce early mortality in re-operative coronary artery bypass surgery (CABG) [6]. The aim of this study is to address the question of whether OPCAB is associated with a lower incidence of MACCE and other adverse outcomes in re-operative coronary surgery.
Review
Materials and methods
Search
A literature search was performed using PubMed, EMBASE and Google Scholar up to May 2013 using the MESH headings “coronary artery bypass, off-pump” and “reoperation”. Studies in English comparing outcomes in re-operative patients undergoing OPCAB versus ONCAB were included (Table 1).
Outcomes of interest
Primary outcomes of interest in the OPCAB and ONCAB groups were peri-operative and short-term (30-day) MACCE and other adverse outcomes including myocardial infarction, stroke, renal dysfunction, low cardiac output state, respiratory failure and atrial fibrillation.
Analysis
Meta-analysis was performed in line with recommendations from PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) and MOOSE (Meta-Analysis of Observational Studies in Epidemiology) [7, 8]. A random-effects model was used to analyse the data and the odds ratio (OR) was used as the summary statistic for binary data. Studies reporting zero events for both OPCAB and ONCAB groups were excluded from the meta-analysis.
Quantitative assessment of data validity and heterogeneity was performed using subgroup analysis for: (1) Studies with a large sample size (≥50) in each cohort, (2) Studies with a high degree of matching between OPCAB and ONCAB groups (matching score ≥ 8), and (3) Studies with a quality score ≥ 8.
Quality assessment
The studies were assessed in two ways: (1) using a matching criteria score, and (2) using a quality assessment score based on a modified Newcastle-Ottawa scale (Table 2) [9]. The matching score was calculated for each study by attributing one point for each pre-operative characteristic for which no statistically significant difference between the OPCAB and ONCAB groups was observed (Table 3). The maximum matching score was 37 and the median score was 8. Studies with a score equal to or greater than 8 points were considered as highly-matched studies and were subgroup analysed. The modified Newcastle-Ottawa quality score was calculated for each study using the subgroup criteria of ‘selection’, ‘comparability’ and ‘outcome assessment’, and attributing stars to each study for these criteria (Table 4). The maximum quality assessment score was 15 and the median score was 8. Studies achieving a score equal to or greater than 8 points were considered as high-quality and were subgroup analysed.
Results
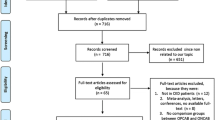
Twelve studies were identified by systematic search to fulfil the inclusion criteria (Figure 1) [10–21]. These studies included 3,471 patients, 1,286 of whom underwent OPCAB and 2,185 underwent ONCAB. All studies used standard cardiopulmonary bypass (CPB) circuits without the use of minimised systems. There were several variations in myocardial arrest and cardioplegia strategy within the ONCAB group. Of the 12 studies, five used cold blood cardioplegia [12, 14–16, 21], one used cold crystalloid [10], 2 used a combination of cold blood and cold crystalloid [11, 20] and one study used a combination of cold blood, warm blood and hypothermic ventricular fibrillation [19]. The majority of studies (5/9) administered a combination of antegrade and retrograde cardioplegia [11, 14, 16, 17, 21]. Two studies used only an antegrade approach [19, 20] and the remainder did not specify their technique.

Search strategy.
Primary outcomes
Myocardial infarction
The incidence of acute myocardial infarction was 3.03% in the OPCAB group and 4.94% in the ONCAB group, as reported by all studies. This reduction with OPCAB was statistically significant using a random effects model (OR 0.58; 95% CI (confidence interval) 0.39-0.87) (Figure 2). No significant heterogeneity was found between the studies.

Myocardial infarction for OPCAB and ONCAB groups.
Stroke
The incidence of stroke was 0.47% in the OPCAB group and 2.38% in the ONCAB group, as reported by all studies. This reduction with OPCAB was statistically significant using the random effects model (OR 0.37; 95% CI 0.17-0.79) (Figure 3), without significant heterogeneity between the studies.

Stroke for OPCAB and ONCAB groups.
Renal failure
The incidence of acute renal failure with or without the need for renal replacement therapy was 1.56% in the OPCAB group and 5.22% in the ONCAB group, as reported by ten studies [11, 13–21]. This reduction with OPCAB was statistically significant using the random effects model (OR 0.39; 95% CI 0.24-0.63) (Figure 4), without significant heterogeneity between the studies.

Renal failure for OPCAB and ONCAB groups.
Low cardiac output state
The incidence of the use of peri- or post-operative intra-aortic balloon pump (IABP) secondary to a low cardiac output state was 0.31% in the OPCAB group and 3.62% in the ONCAB group, as reported by five studies [11, 14, 19–21]. This reduction with OPCAB was statistically significant using the random effects model (OR 0.14; 95% CI 0.04-0.56) (Figure 5), without significant heterogeneity between the studies.

Low cardiac output state for OPCAB and ONCAB groups.
Respiratory failure
The incidence of acute respiratory failure or acute respiratory distress syndrome (ARDS) was 3.03% in the OPCAB group and 4.81% in the ONCAB group, as reported by six studies [11, 13, 14, 16, 19, 20]. This reduction with OPCAB was statistically significant using the random effects model (OR 0.36; 95% CI 0.24-0.54) (Figure 6), without significant heterogeneity between the studies.

Respiratory failure for OPCAB and ONCAB groups.
A trial fibrillation
The incidence of post-operative atrial fibrillation was 5.05% in the OPCAB group and 13.8% in the ONCAB group, as reported by seven studies [10, 12, 14, 16, 17, 20, 21]. This reduction with OPCAB was statistically significant using the random effects model (OR 0.41; 95% CI 0.22-0.77) (Figure 7), without significant heterogeneity between the studies.

Atrial fibrillation for OPCAB and ONCAB groups.
Subgroup analysis
Sample size
Seven studies had a large sample size (≥50) in each cohort and were in this subgroup analysis [10, 11, 13, 14, 16, 17, 19].
Myocardial infarction was again significantly lower in the OPCAB compared to the ONCAB group (2.99% vs. 4.28%; OR 0.63; 95% CI 0.41-0.99). Incidence of stroke was again significantly lower with OPCAB (0.36% vs. 2.56% ONCAB; OR 0.28; 95% CI 0.11-0.69). Similarly, the incidence of renal failure was again significantly lower with OPCAB (1.36% vs. 5.51% ONCAB; OR 0.35; 95% CI 0.20-0.60). Four studies [11, 14, 16, 19] reported a significantly reduced incidence of low cardiac output states with OPCAB (0.27% vs. 3.78% ONCAB; OR 0.11; 95% CI 0.01-0.87). Five studies [11, 13, 14, 16, 19] reported a significantly reduced incidence of respiratory failure/ARDS with OPCAB (3.45% vs. 5.73% ONCAB; OR 0.35; 95% CI 0.23-0.52). Four studies [10, 14, 16, 17] reported a reduced incidence of atrial fibrillation with OPCAB (4.35% vs. 12.24% ONCAB; OR 0.51; 95% CI 0.17-1.51).
Matching score and quality score
Eight studies were attributed a matching score of 8 or greater and were included in this subgroup analysis [11, 13–15, 17, 19–21]. Nine studies were attributed a quality score of 8 or greater and were included in this analysis [11, 13–15, 17–21]. All studies with high matching score were also found to have high quality score and therefore subgroup analysis for matching and quality scores are considered together.
Myocardial infarction was again significantly lower in the OPCAB compared to the ONCAB group (2.51% vs. 4.9%; OR 0.54; 95% CI 0.33-0.89). Incidence of stroke was again significantly lower with OPCAB (0.6% vs. 2.64% ONCAB; OR 0.36; 95% CI 0.16-0.82). Similarly, the incidence of renal failure was again significantly lower with OPCAB (2.15% vs. 5.95% ONCAB; OR 0.40; 95% CI 0.24-0.68). Five studies [11, 14, 19–21] reported a significantly reduced incidence of low cardiac output states with OPCAB (0.48% vs. 4.35% ONCAB; OR 0.14; 95% CI 0.04-0.56). Five studies [11, 13, 14, 19, 20] reported a significantly reduced incidence of respiratory failure/ARDS with OPCAB (1.67% vs. 3.86% ONCAB; OR 0.33; 95% CI 0.18-0.59). Four studies [14, 17, 20, 21] reported a significantly reduced incidence of atrial fibrillation with OPCAB (7.85% vs. 22.6% ONCAB; OR 0.33; 95% CI 0.16-0.70).
Comment
This meta-analysis demonstrates that OPCAB reduces the incidence of major adverse events in the peri-operative and short-term follow-up period. Significant reductions were observed in the rates of myocardial infarction, stroke, renal failure, low cardiac output state, respiratory failure and atrial fibrillation. These observed beneficial effects of OPCAB remained consistent in the subgroup analysis of large sample size, high matching score and high quality score studies.
Re-operative coronary artery surgery poses a great risk to an already high-risk, older patient cohort with potentially higher co-morbidity and end-organ disease. The challenging technical aspects of the operation itself; including sternal re-entry, epicardial adhesions, patent or diseased in-situ grafts, more advanced coronary and aortic disease burden and the sufficiency of myocardial protection are all the challenging technical aspects contributing to the high-risk nature of the operation. These complexities of re-operative coronary surgery have inevitably not permitted the inclusion of these patients in randomised trials.
A very clear spectrum of difficulty is observed in different patients undergoing re-operative coronary artery surgery, providing a spectrum of challenges. Baseline co-morbidities, ventricular function and the quality of target coronary vessels are some of the factors affecting the decision to undertake OPCAB, the risk of conversion to ONCAB, the degree of target vessel revascularisation, the effect on target organ preservation and ultimately the outcome profile [6].
The conduct of OPCAB, whilst in itself very challenging, prompting scepticism regarding surgeon experience and expertise, does provide very clear protection for the heart, the brain and other organs. Firstly, avoiding manipulation of the aorta and previous bypass grafts in OPCAB reduces the risk of coronary and cerebral embolisation. Secondly, providing sufficient myocardial protection in the setting of extensive coronary disease is challenging and often requires a retrograde approach. Utilisation of intra-coronary shunts in OPCAB reduce the ischaemic time and consequent myocardial stunning. Thirdly, the avoidance of extra-corporeal membrane circulation eliminates the systemic inflammatory response observed with CPB, protecting predominantly the lungs and the kidneys as well as all other organs. Finally, the elimination of the CPB-induced coagulopathy may decrease the need for transfusion and potentially reduce re-exploration for bleeding [6]. However, it is crucial to consider that, given the spectrum of difficulty observed with re-operative coronary surgery and the factors affecting the decision to undertake OPCAB, appropriate patient selection is of paramount importance, whereby OPCAB is not necessarily the most appropriate technique for all patients.
In a recent analysis of the Society of Thoracic Surgeons Adult Cardiac Surgery Database by Ghanta et al. [22], outcomes of 72,431 patients undergoing isolated reoperative coronary artery bypass grafting were observed over the period 2000 to 2009. Risk-adjusted rates of stroke decreased from 1.9% in 2000 to 1.6% in 2009 (relative risk reduction -16.5%, p < 0.001); of renal failure decreased from 5.5% to 4.9% (-15.4%, p < 0.004); of prolonged ventilation increased from 11.6% to 15.3% (31.4%, p = 0.532); and of atrial fibrillation increased from 19.0% to 19.9% (4.8%, p = 0.532); amongst other outcome measures of morbidity observed. The OPCAB outcome measures of our study compare favourably with those of Ghanta and colleagues, the largest report to date analysing isolated reoperative CABG.
OPCAB has been demonstrated to reduce early mortality in re-operative CABG [6]. The aim of this study was to explore beyond these effects on mortality and attempt to ascertain whether OPCAB can reduce MACCE and other adverse outcomes in re-operative CABG by means of providing more superior organ protection. All of the studied outcome measures were demonstrated to be significantly reduced with OPCAB, emphasising the superior organ protection provided by the technique.
Limitations
The issue of surgeon experience and expertise with OPCAB surgery has been a source of much debate and criticism [2]. This challenging technique has a very pronounced learning curve and requires time and experience in order for the outcomes to be comparable. The same concept applies for re-operative surgery. Whilst not under the same degree of scepticism, owing to the lack of randomised trials, re-operation itself is an even bigger challenge, requiring particular experience and is more time consuming. In order to improve the validity and reliability of the results of this study, surgeon experience in both OPCAB and re-operative CABG will need to be accounted and adjusted for.
A further limitation of this study is the short follow-up period of analysis. We have demonstrated significant reduction in 30-day adverse outcomes using OPCAB, however in order to allow generalisation of these results regarding the outcome profile of OPCAB in re-operative CABG, mid- and long-term analysis of adverse outcomes are required.
A further limitation of this study which is required to be taken into account is that OPCAB is not necessarily the most appropriate technique for all patients undergoing re-operative CABG. This technique can only be demonstrated to be superior in the setting of suitable coronary target vessels, a low risk of conversion to ONCAB and minimal requirement for manipulation of the heart, allowing for target vessel revascularisation.
Conclusions
Off-pump coronary artery bypass grafting reduces peri-operative and short-term major adverse outcomes in patients undergoing re-operative coronary artery surgery. These outcomes include myocardial infarction, stroke, renal failure, low cardiac output state, respiratory failure and new-onset atrial fibrillation. Consequently we conclude that OPCAB provides superior organ protection and a safer outcome profile in re-operative CABG.
Abbreviations
- ARDS:
-
Acute respiratory distress syndrome
- CABG:
-
Coronary artery bypass graft
- CI:
-
Confidence interval
- CPB:
-
Cardiopulmonary bypass
- IABP:
-
Intra-aortic balloon pump
- MACCE:
-
Major adverse cardiovascular and cerebrovascular events
- MOOSE:
-
Meta-analysis of observational studies in epidemiology
- ONCAB:
-
On-pump coronary artery bypass
- OPCAB:
-
Off-pump coronary artery bypass
- OR:
-
Odds ratio
- PRISMA:
-
Preferred reporting items for systematic reviews and meta-analyses.
References
Lamy A, Devereaux PJ, Prabhakaran D, Taggart DP, Hu S, Paolasso E, Straka Z, Piegas LS, Akar AR, Jain AR, Noiseux N, Padmanabhan C, Bahamondes JC, Novick RJ, Vaijyanath P, Reddy S, Tao L, Olavegogeascoechea PA, Airan B, Sulling TA, Whitlock RP, Ou Y, Ng J, Chrolavicius S, Yusuf S, CORONARY Investigators: Off-pump or on-pump coronary-artery bypass grafting at 30 days. N Engl J Med. 2012, 366: 1489-1497.
Lamy A, Devereaux PJ, Prabhakaran D, Taggart DP, Hu S, Paolasso E, Straka Z, Piegas LS, Akar AR, Jain AR, Noiseux N, Padmanabhan C, Bahamondes JC, Novick RJ, Vaijyanath P, Reddy S, Tao L, Olavegogeascoechea PA, Airan B, Sulling TA, Whitlock RP, Ou Y, Ng J, Chrolavicius S, Yusuf S, CORONARY Investigators: Effects of off-pump and on-pump coronary-artery bypass grafting at 1 year. N Engl J Med. 2013, 368: 1179-1188.
Shroyer AL, Grover FL, Hattler B, Collins JF, McDonald GO, Kozora E, Lucke JC, Baltz JH, Novizky D, Affairs Randomized On/Off Bypass (ROOBY) Study Group: Veterans’ On-pump versus off-pump coronary-artery bypass surgery. N Engl J Med. 2009, 361: 1827-1837.
Emmert MY, Salzberg SP, Seifert B, Rodriguez H, Plass A, Hoerstrup SP, Grunenfelder J, Falk V: Is off-pump superior to conventional coronary artery bypass grafting in diabetic patients with multivessel disease?. Eur J Cardiothorac Surg. 2011, 40: 233-239.
Puskas JD, Kilgo PD, Lattouf OM, Thourani VH, Cooper WA, Vassiliades TA, Chen EP, Vega JD, Guyton RA: Off-pump coronary bypass provides reduced mortality and morbidity and equivalent 10-year survival. Ann Thorac Surg. 2008, 86: 1139-1146. discussion 1146
Sepehripour AH, Saso S, Harling L, Punjabi P, Ashrafian H, Athanasiou T: Does off-pump coronary revascularisation reduce mortality in re-operative coronary artery surgery? A meta-analysis of observational studies. Perfusion. 2013, 28: 340-349.
Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group: Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ. 2009, 339: b2535-
Stroup DF, Berlin JA, Morton SC, Olkin I, Williamson GD, Rennie D, Moher D, Becker BJ, Sipe TA, Thacker SB: Meta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA. 2000, 283: 2008-2012.
Taggart DP, D’Amico R, Altman DG: Effect of arterial revascularization on survival: a systematic review of studies comparing bilateral and single internal mammary arteries. Lancet. 2001, 358: 870-875.
Alamanni F, Pompilio G, Polvani G, Agrifoglio M, Zanobini M, Parolari A, Cannata A, Biglioli P: Off-pump redo coronary artery bypass grafting: technical aspects and early results. Heart Surg Forum. 2002, 5 (Suppl 4): S432-444.
Bergsland J, Hasnain S, Lajos TZ, Salerno TA: Elimination of cardiopulmonary bypass: a prime goal in reoperative coronary artery bypass surgery. Eur J Cardiothorac Surg. 1998, 14: 59-62. discussion 62–63
Czerny M, Zimpfer D, Kilo J, Gottardi R, Dunkler D, Wolner E, Grimm M: Coronary reoperations: recurrence of angina and clinical outcome with and without cardiopulmonary bypass. Ann Thorac Surg. 2003, 75: 847-852.
D’Ancona G, Karamanoukian H, Ricci M, Salerno T, Lajos T, Bergsland J: Reoperative coronary artery bypass grafting with and without cardiopulmonary bypass: determinants of perioperative morbidity and mortality. Heart Surg Forum. 2001, 4: 152-158. dicussion 158–159
Dewey TM, Magee MJ, Acuff T, Prince S, Herbert M, Edgerton JR, Mack MJ: Beating heart surgery reduces mortality in the reoperative bypass patient. Heart Surg Forum. 2002, 5 (Suppl 4): S301-316.
Gerli C, Mantovani L, Franco A, De Luca M, Bergonzi PC, Boroli F, Romano A, Landoni G, Zangrillo A: Redo coronary artery bypass grafting on the beating heart and transfusion needs. Minerva Anestesiol. 2006, 72: 985-993.
Mishra YK, Collison SP, Malhotra R, Kohli V, Mehta Y, Trehan N: Ten-year experience with single-vessel and multivessel reoperative off-pump coronary artery bypass grafting. J Thorac Cardiovasc Surg. 2008, 135: 527-532.
Morris CD, Puskas JD, Pusca SV, Lattouf OM, Cooper WA, Vassiliades TA, Chen EP, Thourani VH, Kilgo PD, Guyton RA: Outcomes after off-pump reoperative coronary artery bypass grafting. Innovations (Phila). 2007, 2: 29-32.
Schutz A, Mair H, Wildhirt SM, Gillrath G, Lamm P, Kilger E, Reichart B: Re-OPCAB vs. Re-CABG for myocardial revascularization. Thorac Cardiovasc Surg. 2001, 49: 144-148.
Teodori G, Iaco AL, Di Mauro M, Cini R, Di Giammarco G, Vitolla G, Calafiore AM: Reoperative coronary surgery with and without cardiopulmonary bypass. J Card Surg. 2000, 15: 303-308.
Tugtekin SM, Alexiou K, Kappert U, Esche E, Joskowiak D, Knaut M, Matschke K: Coronary reoperation with and without cardiopulmonary bypass. Clin Res Cardiol. 2006, 95: 93-98.
Vohra HA, Bahrami T, Farid S, Mafi A, Dreyfus G, Amrani M, Gaer JA: Propensity score analysis of early and late outcome after redo off-pump and on-pump coronary artery bypass grafting. Eur J Cardiothorac Surg. 2008, 33: 209-214.
Ghanta RK, Kaneko T, Gammie JS, Sheng S, Aranki SF: Evolving trends of reoperative coronary artery bypass grafting: an analysis of the Society of Thoracic Surgeons Adult Cardiac Surgery Database. J Thorac Cardiovasc Surg. 2013, 145: 364-372.
Acknowledgements
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
AS - made substantial contributions to conception and design, acquisition of data, analysis and interpretation of data; involved in drafting the manuscript and revising it critically for important intellectual content; given final approval of the version to be published; and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. LH - made substantial contributions to conception and design, acquisition of data, analysis and interpretation of data; involved in drafting the manuscript and revising it critically for important intellectual content; given final approval of the version to be published; and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. HA - made substantial contributions to conception and design; involved in drafting the manuscript and revising it critically for important intellectual content; and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. RC - made substantial contributions to conception and design; involved in drafting the manuscript and revising it critically for important intellectual content; and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. TA - made substantial contributions to conception and design; involved in drafting the manuscript and revising it critically for important intellectual content; given final approval of the version to be published; and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. All authors read and approved the final manuscript.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Sepehripour, A.H., Harling, L., Ashrafian, H. et al. Does off-pump coronary revascularization confer superior organ protection in re-operative coronary artery surgery? A meta-analysis of observational studies. J Cardiothorac Surg 9, 115 (2014). https://doi.org/10.1186/1749-8090-9-115
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1749-8090-9-115