
Abstract
Purpose
Although evidence is building on the positive effects of physical activity for prostate cancer survivors, less is known about the possible independent effects of sedentary behavior on quality of life and psychological well-being in this population. We determined the extent to which objectively measured moderate-to-vigorous physical activity (MVPA) and sedentary behavior were independently associated with quality of life, anxiety, and depressive symptoms in prostate cancer survivors.
Methods
An exploratory cross-sectional analysis was undertaken on baseline data from a multicenter, cluster randomized controlled trial on the efficacy of a clinician referral and 12-week exercise program for men who had completed active treatment for prostate cancer. Multiple regression analyses were performed using data from 98 prostate cancer survivors who wore hip-mounted accelerometers (time spent sedentary defined as <100 counts per minute [CPM]; MVPA defined as >1,951 CPM) and completed self-report instruments on their quality of life, anxiety, and depressive symptoms. Results were compared with minimal clinically important differences for the quality of life scales.
Results
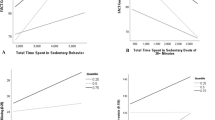
Independent of sedentary behavior, increases in MVPA of between 15 and 33 min/day were associated with clinically important (but not statistically significant) improvements in three quality of life scales (insomnia, diarrhea, and financial difficulties). Independent of MVPA, decreases in sedentary behavior of 119 and 107 min/day were associated with clinically important (but not statistically significant) improvements in physical functioning and role functioning, respectively.
Conclusion
Within our exploratory study, modest increases in MVPA and more substantive decreases in sedentary behavior were independently associated with clinically important improvements in several quality of life scales. Further research, including prospective studies, is required to understand sedentary behavior across larger and more representative samples (in terms of their physical, psychological, and social functioning and their engagement in physical activity) of prostate cancer survivors.
Trial registration
Australia and New Zealand Clinical Trials Register (ANZCTR): ACTRN12610000609055
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Prostate cancer is the second most common cancer in men worldwide and has a high survival rate [1]. Having been diagnosed with prostate cancer, however, is associated with poorer mental health (e.g., increased anxiety, depressive symptoms, and psychological distress) [2, 3], functional limitations (e.g., urinary, bowel, and sexual dysfunction) [4], low levels of moderate-to-vigorous physical activity (MVPA) [5, 6], and reduced quality of life [2, 4]. Engaging in physical activity can ameliorate many of the adverse effects of prostate cancer and its treatments, with systematic review findings strongest for the positive effect of physical activity on aerobic endurance, muscular endurance, and quality of life in this population [7, 8]. Conversely, evidence is emerging that sedentary behavior poses a health risk that is independent of insufficient physical activity [9–11]. Sedentary behavior is defined as “any waking behavior characterized by an energy expenditure ≤1.5 METs [metabolic equivalents] while in a sitting or reclining posture” [12]. From research with adults, there is strong evidence that sedentary behavior is associated with all-cause mortality, fatal and non-fatal cardiovascular disease, type 2 diabetes, and metabolic syndrome independent of physical activity [13]. Comparisons between men with and without history of prostate cancer, however, have yielded inconsistent findings with respect to time spent sedentary [14, 15], and few studies have focused on the association between sedentary behavior and health outcomes (particularly mental health outcomes) in prostate cancer survivors [5, 16]. Greater understanding of the independent effects of physical activity and sedentary behavior on the quality of life and psychological well-being of prostate cancer survivors is warranted and would assist in the design of targeted interventions to improve the lives of prostate cancer survivors.
The ENGAGE (efficacy of a referral and physical activity program for survivors of prostate cancer) study was a multicenter, cluster randomized controlled trial to determine the efficacy of a clinician referral and 12-week exercise program to increase physical activity among men who had completed active treatment for prostate cancer [17, 18]. Compared to men in the control condition, those in the intervention significantly increased their vigorous physical activity levels and experienced increased cognitive functioning and reduced depressive symptoms [18]. This trial is one of only a few studies involving prostate cancer survivors that included measures of quality of life and psychological well-being, as well as objective measures of physical activity and sedentary behavior. Given the potential utility inherent in understanding these relationships for the development and refinement of interventions to improve health outcomes, we conducted a secondary analysis of the ENGAGE study baseline data. The aim of this exploratory cross-sectional analysis was to determine the extent to which MVPA and sedentary behavior were independently associated with quality of life, anxiety, and depressive symptoms in prostate cancer survivors prior to commencement of the exercise program. We also assessed whether the associations found could be clinically important.
Methods
Study population
The ENGAGE study recruitment and sample details have been described previously [17, 18]. Inclusion criteria were men diagnosed with stage I, II, or III prostate cancer who had (a) completed active treatment for prostate cancer within the previous 3–12 months (patients on hormone treatment were eligible to participate), and (b) the ability to complete surveys in the English language. Patients were excluded if they had any musculoskeletal, cardiovascular, or neurological disorders that could limit them from exercising. Eligible patients were recruited through the outpatient clinics of three large public health services and four private clinics located in metropolitan Melbourne, Australia. The patients’ treating clinicians provided medical clearance for all participants prior to their involvement in the exercise program. Of the 741 patients screened for this study, 443 met the eligibility criteria, and 147 were contactable and agreed to participate. Of these 147 participants, 98 provided complete accelerometer, quality of life, anxiety, and depressive symptoms data (34 chose not to wear accelerometers, 13 provided invalid accelerometer data, and 2 had incomplete quality of life, anxiety, and depressive symptoms data).
Ethics approval to conduct this study was obtained from the human research ethics committees of the health services and host university involved in this study. Informed consent was obtained from all individual participants included in the study.
Measurements
Baseline data on demographics, clinical characteristics, quality of life, anxiety, depressive symptoms, physical activity, and time spent sedentary were collected. Demographics and clinical characteristics obtained through self-report questionnaires included: age, height, weight, relationship status, highest level of education, and treatment regime. Self-reported heights and weights were used to calculate body mass index (BMI) (kg/m2) scores. Clinical characteristics obtained from medical records included: stage of disease, weeks since active treatment, and health service type (public/private).
Quality of life was measured using the European Organization for Research and Treatment of Cancer core quality of life questionnaire (EORTC QLQ-C30(V3)) [19] and the prostate tumor-specific module (EORTC QLQ-PR25) [20]. The EORTC QLQ-C30(V3) has a global health status scale, five functional scales (physical, role, cognitive, emotional, and social), and nine symptom scales (fatigue, nausea and vomiting, pain, dyspnea, insomnia, appetite loss, constipation, diarrhea, and financial difficulties). The EORTC QLQ-PR25 has two functional scales (sexual activity and sexual functioning) and four symptom scales (urinary symptoms, bowel symptoms, hormonal treatment-related symptoms, and incontinence aid). Both measures have convergent and discriminant validity, as well as adequate internal consistency reliability [19, 20]. Minimal clinically important differences for the scales (each of which ranges from 0 to 100) have been estimated to be approximately 5–10 points [21–23]. This estimation strongly overlaps with guidelines for small-sized, clinically relevant differences (ranging from 3 to 7 points for diarrhea to 6–19 points for role functioning) produced from a method combining a systematic review, a meta-analysis, and expert opinions [24].
Anxiety was measured with the Memorial Anxiety Scale for Prostate Cancer (MAX-PC) [25]. The MAX-PC has three subscales (prostate cancer anxiety, prostate-specific antigen anxiety, and fear of recurrence) and a total anxiety scale. The MAX-PC has concurrent validity with established anxiety measures (e.g., the anxiety subscale of the Hospital Anxiety and Depression Scale [26]), discriminant validity, internal consistency, and test–retest reliability [25, 27].
Depressive symptoms were measured using the Centre for Epidemiological Studies Depression Inventory (CES-D) [28]. The scale has strong concurrent validity with both clinical and self-report criteria, and sound construct validity [28].
Physical activity and time spent sedentary were measured using hip-mounted ActiGraph GT1 M (Pensacola, FL) units. The accelerometer is a valid and reliable tool for measuring physical activity and sedentary time among adults [29–31]. Each participant was shown how to wear the accelerometer on a nylon belt over the right hip (physical activity estimates do not vary by right or left hip placement [32]) and was also provided with written instructions on the use of the accelerometer. Participants were asked to start wearing the accelerometer when they got out of bed the next morning and asked to wear it for seven consecutive days during waking hours. On completion of the seven days, participants were asked to return the accelerometer in a reply-paid envelope. Data from the ActiGraph units were processed using ActiLife software (V6.7.1) and managed using a customized Microsoft Excel macro. Time spent sedentary was defined as <100 counts per minute [CPM], and MVPA was defined as >1,951 CPM [30]. To be included in the analysis, participants were required to have worn the accelerometer for at least 10 h each day (60 min or more of consecutive zero counts, without “tolerance,” was considered non-wear of the device) for at least four of the seven days (based on Healy et al. [31]). Average daily minutes in MVPA and time spent sedentary were calculated for each participant based on the number of valid days of data provided. Due to differences in daily accelerometer wear time between participants, sedentary behavior was standardized to a 12-hour wear time using the formula:
This standardized sedentary behavior variable was used in the analyses.
Current guidelines suggest that prostate cancer survivors engage in at least 150 min/week of moderate-intensity physical activity or 75 min/week of vigorous-intensity physical activity or an equivalent combination of moderate and vigorous physical activity, which may include weight-bearing exercises [33].
Statistical analysis
Statistical analyses were performed using Stata (Version 13) software. Independent t tests and Chi-squared tests were used to determine whether there were differences between men with and without complete data in terms of their demographic and clinical characteristics. Subsequent analyses were performed on the data from the men with complete data.
The sexual functioning and incontinence aid scales were omitted from the analysis due to a high amount of non-responses (62.2 and 70.4 %, respectively). Responding to these items was conditional on participants being sexually active in the last 4 weeks and wearing incontinence aids, respectively. For the remaining variables, a negligible amount of data were missing (<0.01 %). The result from Little’s [34] test (χ 2(390) = 399.21, p = .36) suggests that data were missing completely at random.
Using multiple regression analyses, MVPA and standardized sedentary behavior (as continuous variables) were simultaneously regressed against each of the quality of life, anxiety, and depressive symptoms scales and subscales. Adjusted multiple regression analyses were also performed with demographic variables (age, BMI, relationship status, and highest level of education), clinical variables (number of comorbidities, weeks since active treatment, stage of disease, treatment regime, and health service type), and clinician (to assess the effect of clustering) screened as potential covariates or factors. Variables that were related (p ≤ .10) to any of the quality of life, anxiety, and depressive symptoms scales and subscales in bivariate analyses were included in the initial adjusted regression models. Using backward elimination, covariates and factors were then removed from these models (one by one, in an iterative process) when p ≥ .05. Because these analyses focused on estimation, rather than prediction, attention is paid to the unstandardized beta coefficients and their confidence intervals (rather than effect sizes for the proportions of variance explained). The unstandardized beta coefficients represent the changes in quality of life, anxiety, and depressive symptom scores per 1 min/day increase in MVPA or standardized sedentary behavior after adjusting for the other covariates and factors included in each model.
Exact p values are reported together with unstandardized beta coefficients and their confidence intervals. Although adjusting the α value to protect against inflation of experiment-wise error when multiple tests are performed is generally advisable [35, 36], making such an adjustment in this study could result in Type II errors, which may discourage researchers from further investigations in this area. Given that our prime focus was on hypothesis generation, rather than hypothesis validation, we did not adjust for multiple comparisons. Accordingly, α was set at 0.05. Sample size calculations for the ENGAGE study were based on the primary outcomes for the main trial [17, 18], rather than the exploratory secondary analyses reported here. Modest recruitment and the constraints of fixed-term funding meant that the target of recruiting 220 participants [17] was not achieved.
Given that the study was exploratory, we also assessed whether the associations could be clinically important, irrespective of their statistical significance. A minimal clinical important difference can be defined as “the smallest difference in score in the domain of interest which patients perceive as beneficial and which would mandate, in the absence of troublesome side effects and excessive cost, a change in the patient’s management” [37]. The results from the multiple regression analyses were compared with minimal clinically important differences for the quality of life scales using two methods. First, the changes in MVPA and, separately, in sedentary behavior needed to obtain minimal clinically important differences were calculated. Minimal clinically important differences in quality of life scales were defined as the lower limits of the ranges for small-sized, clinically relevant differences provided in published guidelines [24]. A small-sized difference is one that is subtle, but clinically relevant. For each scale, the changes in MVPA per day, and (separately) in sedentary behavior per day, needed to obtain clinically important differences were calculated by dividing the small-sized clinically important difference by the adjusted unstandardized beta coefficients. Second, the changes in quality of life scores from performing recommended levels of MVPA were determined. Prostate cancer survivors are recommended to undertake at least 150 min/week of moderate physical activity or 75 min/week vigorous physical activity or an equivalent combination of moderate and vigorous physical activity [33, 38, 39]. For the purpose of this analysis, this guideline was translated into a daily recommendation of 21 min (150 min/7 days) of MVPA. For each scale, the effect of performing recommended levels of MVPA was calculated by multiplying the daily recommendation for MVPA (21 min/day) and the adjusted unstandardized coefficient. Using published guidelines, the resulting change in quality of life score was interpreted as being trivial (no difference or unlikely to have clinical relevance), small (subtle, but nevertheless clinically relevant), medium (likely to be clinically relevant), or large (unequivocal clinical relevance) [24]. The analysis did not include the anxiety or depressive symptoms scales, because, as far as we are aware, clinically important differences for these scales have yet to be established.
Results
Participant demographic and clinical characteristics are provided in Table 1. Briefly, the men had a mean age of 65.6 years (SD = 8.5), were overweight (BMI: M = 28.0, SD = 3.7), and had last undergone active treatment, on average, 25.3 weeks prior (SD = 10.0). Compared to men who did not have complete data (n = 49), those with complete data (n = 98) were, on average, 5 years older (p < . 01) and had undergone different treatment regimes (i.e., more likely to have been treated with both surgery and radiotherapy and less likely to have undergone surgery only; p = .04) (see Table 1). There were no statistically significant differences for BMI, relationship status, highest level of education, number of comorbidities, weeks since active treatment, stage of disease, and health service type. Participants wore the accelerometers, on average, 14 h/day (SD = 1.4) for between 4 and 8 days (M = 6.5, SD = 0.9). They spent, on average, 38 min/day (SD = 22) engaged in MVPA and 10 h/day (SD = 1.5) in sedentary behavior (standardized for accelerometer wear time to 9 h/day, SD = 0.8).
In general, unstandardized beta coefficients for associations between MVPA and quality of life, anxiety, and depressive symptoms scales and subscales were larger than those between sedentary behavior and these variables (Table 2). None of the analyses returned statistically significant results, however.
Interpretation of the unstandardized beta coefficients with reference to guidelines for minimal clinically important differences in quality of life scores revealed that an increase in MVPA of less than 1 hour per day was associated with clinically important (but not statistically significant) differences in several symptom scales (fatigue, insomnia, diarrhea, and financial difficulties; Table 3). Undertaking recommended levels of MVPA (i.e., 21 min/day, equivalent to 150 min/week) was only related (but not to a statistically significant level) to reductions in insomnia and financial difficulties to a clinically important extent.
Discussion
Within our small study population of prostate cancer survivors, achievable increases in MVPA and reductions in sedentary behavior were associated with clinically important improvements in several aspects of quality of life. These findings support evidence from randomized controlled trials (synthesized in a recent systematic review [40]) showing a positive relationship between physical activity and quality of life in prostate cancer survivors. Our work extends current knowledge through (1) demonstrating the potential independent benefits of increasing MVPA and reducing sedentary behavior for improving quality of life, (2) providing evidence of such relationships when activity levels are objectively measured, and (3) interpreting these effects with reference to minimal clinically important differences.
The magnitudes of the adjusted unstandardized beta weights for the associations between both MVPA and sedentary behavior and both physical functioning and fatigue suggest that clinically important changes on these quality of life scales may be achievable for many men with prostate cancer. Although increasing MVPA by 52–78 min/day or reducing sedentary behavior by 119–132 min/day may be beyond many men with prostate cancer, the independence of these effects suggests that more modest increases in MVPA combined with lower reductions in sedentary behavior are likely to produce clinically important changes. These findings are consistent with those of a systematic review on the effect of exercise on the quality of life of adult post-treatment cancer survivors [41]. In this review, the observed mean difference in EORTC QLQ-C30 physical functioning and fatigue scores from baseline to up to 12 weeks were 6.23 points (95 % CI 1.74, 10.72) and −22.45 (95 % CI −50.66, 5.77), respectively. Although this evidence from randomized controlled trials may suggest that engaging in physical activity enhances physical functioning to a modest extent [41], our data are open to reverse causation. That is, it may also be the case that people who have higher levels of physical functioning participate in higher levels of physical activity.
Several quality of life scales were associated with MVPA to a similar or greater extent than physical functioning and fatigue (social functioning, pain, dyspnea, insomnia, diarrhea, and financial difficulties). Systematic review evidence on adult post-treatment cancer survivors suggests that exercise may improve social functioning and sleep disturbance, but may have no effect on pain [41]. For breast and colon cancer patients undergoing adjuvant chemotherapy, however, a recent study has shown that physical activity can reduce nausea and vomiting, and pain [42]. Furthermore, some associations may be more plausibly explained as reverse causations; diarrhea, for example, may be more likely to decrease someone’s involvement in physical activity than an increase in physical activity would be to decrease diarrhea. More work is needed to identify the circumstances in which physical activity can be effective in reducing cancer-related symptoms. Physical activity may be more effective at times when patients are experiencing higher levels of symptoms.
The findings support advice within physical activity guidelines that exceeding the recommended physical activity levels is likely to provide additional benefits [38, 39]. The interpretations of several of the adjusted unstandardized beta coefficients are that clinically important improvements in several quality of life scales could be achieved through engaging in additional MVPA and reducing sedentary behavior. As prostate cancer emerges at a time of life when many men are retired and may have time to undertake more frequent physical activity, promoting programs that increase activity levels and reduce sedentary behavior may be effective in this population.
The adjusted unstandardized beta coefficients for the associations between sedentary behavior and quality of life illustrate the potential importance of reducing sedentary behavior. Reducing sedentary behavior (e.g., through standing more and sitting less) by less than 2 h/day was associated with clinically important improvements in several quality of life scales (physical functioning, role functioning, dyspnea). As such, reducing sedentary behavior meaningfully compliments the effects achievable through increasing MVPA. Our findings are consistent with those of a systematic review in which emerging evidence was presented of higher levels of sedentary behavior being associated with both lower quality of life [43] and greater risk of depression [44] in adults (not cancer survivors). Research with cancer populations is mixed, with some evidence for an association between sedentary behavior and quality of life [45–48], and other studies showing no effects [16, 49].
Limitations of this study include ceiling and floor effects (many data points at the upper and lower limits, respectively, of response scales) for several of the quality of life, anxiety, and depressive symptoms scales (which attenuated the magnitudes of correlations observed), the participants’ high levels of functioning, the small sample size, potential confounding, and the inability of the accelerometers to detect posture. Men in this study had reasonably high quality of life scores, and negligible levels of anxiety and depressive symptoms, thus producing ceiling and floor effects. The men were highly functioning, with the EORTC QLQ-C30(V3) scores, for example, being consistently higher than, but within one standard deviation of, norms for prostate cancer survivors aged 60–69 years [50]. The men were also more physically active than other samples of prostate cancer survivors reported in the literature [5]. Our exclusion of men with musculoskeletal, cardiovascular, or neurological disorders that could limit them from exercising from this study may have been partially responsible for producing this sample of highly functioning men and the limited variation in much of our data. The sample size in this study was small, meaning that the null findings could have been due to low statistical power and that the reported findings may be unstable and will require replication with larger samples. Even so, the use of an objective measure for assessing physical activity is a major strength of this study, because measurement error (which can reduce statistical power [51]) is substantially less with accelerometers compared to physical activity logs and questionnaires [52]. Although the study was undertaken with data from a cluster randomized controlled trial, the study reported here is cross-sectional, meaning that the results are subject to residual confounding as with any observational study. Finally, the hip-worn ActiGraph accelerometer was unable to detect posture, which means that if a participant was standing still and accumulating <100 CPM, this activity would be incorrectly classified as sedentary time resulting in an over-estimation of activity of this intensity [31].
This study is novel in its focus, as it provided a snapshot of physical activity and time spent sedentary in prostate cancer survivors using an objective measure, and their associations with quality of life, anxiety, and depressive symptoms. The findings suggest it may be possible to achieve clinically important improvements in quality of life through increasing MVPA and reducing sedentary behavior. Further research is needed to examine these relationships more closely using objective measures of sitting, such as the thigh-worn activPAL inclinometer [53]. In addition, researchers have an opportunity to build on the work showing, for example, that patterns of sedentary behavior, such as the frequency of interruptions to sustained bouts of sitting, influence health outcomes irrespective of the total volume of sedentary behavior [54]. Future research, including prospective studies, would ideally involve larger and more representative samples of prostate cancer survivors, in terms of their physical, psychological, and social functioning and their engagement in objectively assessed physical activity.
References
Ferlay J, Soerjomataram I, Dikshit R, Eser S, Mathers C, Rebelo M, Parkin DM, Forman D, Bray F (2015) Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer 136:E359–E386. doi:10.1002/ijc.29210
Couper JW, Love AW, Duchesne GM, Bloch S, Macvean M, Dunai JV, Scealy M, Costello A, Kissane DW (2010) Predictors of psychosocial distress 12 months after diagnosis with early and advanced prostate cancer. Med J Aust 193:S58–S61
Watts S, Leydon G, Birch B, Prescott P, Lai L, Eardley S, Lewith G (2014) Depression and anxiety in prostate cancer: a systematic review and meta-analysis of prevalence rates. BMJ Open 4:e003901–e003901. doi:10.1136/bmjopen-2013-003901
Kyrdalen AE, Dahl AA, Hernes E, Småstuen MC, Fosså SD (2013) A national study of adverse effects and global quality of life among candidates for curative treatment for prostate cancer. BJU Int 111:221–232. doi:10.1111/j.1464-410X.2012.11198.x
Lynch BM, Dunstan DW, Winkler E, Healy GN, Eakin E, Owen N (2011) Objectively assessed physical activity, sedentary time and waist circumference among prostate cancer survivors: findings from the National Health and Nutrition Examination Survey (2003–2006). Eur J Cancer Care 20:514–519. doi:10.1111/j.1365-2354.2010.01205.x
Chipperfield K, Fletcher J, Millar J, Brooker J, Smith R, Frydenberg M, Oh T, Burney S (2013) Factors associated with adherence to physical activity guidelines in patients with prostate cancer. Psychooncology 22:2478–2486. doi:10.1002/pon.3310
Baumann FT, Zopf EM, Bloch W (2012) Clinical exercise interventions in prostate cancer patients: a systematic review of randomized controlled trials. Support Care Cancer 20:221–233. doi:10.1007/s00520-011-1271-0
Keogh J, MacLeod R (2012) Body composition, physical fitness, functional performance, quality of life, and fatigue benefits of exercise for prostate cancer patients: a systematic review. J Pain Symptom Manage 43:96–110. doi:10.1016/j.jpainsymman.2011.03.006
Salmon J, Bauman A, Crawford D, Timperio A, Owen N (2000) The association between television viewing and overweight among Australian adults participating in varying levels of leisure-time physical activity. Int J Obes 24:600–606. doi:10.1038/sj.ijo.0801203
Gennuso KP, Gangnon RE, Matthews CE, Thraen-Borowski KM, Colbert LH (2013) Sedentary behavior, physical activity, and markers of health in older adults. Med Sci Sports Exerc 45:1493–1500. doi:10.1249/MSS.0b013e318288a1e5
Owen N, Healy GN, Matthews CE, Dunstan DW (2010) Too much sitting: the population health science of sedentary behavior. Exerc Sport Sci Rev 38:105–113. doi:10.1097/JES.0b013e3181e373a2
Sedentary Behaviour Research Network (2012) Standardized use of the terms “sedentary” and “sedentary behaviours”. Appl Physiol Nutr Metab 37:540–542. doi:10.1139/h2012-024
de Rezende LFM, Lopes MR, Rey-López JP, Matsudo VKR, Luiz OC (2014) Sedentary behavior and health outcomes: an overview of systematic reviews. PLoS One 9(8):e105620. doi:10.1371/journal.pone.0105620
Rogers LQ, Courneya KS, Gururaja RP, Markwell SJ, Imeokparia R (2008) Lifestyle behaviors, obesity, and perceived health among men with and without a diagnosis of prostate cancer: a population-based, cross-sectional study. BMC Public Health 8:23–31. doi:10.1186/1471-2458-8-23
Kim RB, Phillips A, Herrick K, Helou M, Rafie C, Anscher MS, Mikkelsen RB, Ning Y (2013) Physical activity and sedentary behavior of cancer survivors and non-cancer individuals: results from a national survey. PLoS One 8(3):e57598. doi:10.1371/journal.pone.0057598
Phillips SM, Stampfer MJ, Chan JM, Giovannucci EL, Kenfield SA (2015) Physical activity, sedentary behavior, and health-related quality of life in prostate cancer survivors in the health professionals follow-up study. J Cancer Surviv 9:500–511. doi:10.1007/s11764-015-0426-2
Livingston PM, Salmon J, Courneya KS, Gaskin CJ, Craike M, Botti M, Broadbent S, Kent B (2011) Efficacy of a referral and physical activity program for survivors of prostate cancer [ENGAGE]: rationale and design for a cluster randomised controlled trial. BMC Cancer 11:237. doi:10.1186/1471-2407-11-237
Livingston PM, Craike M, Salmon J, Courneya KS, Gaskin CJ, Fraser SF, Mohebbi M, Broadbent S, Botti M, Kent B, the ENGAGE Uro-Oncology Clinicians’ Group (2015) Effects of a clinician referral and exercise program for men who have completed active treatment for prostate cancer: a multicentre cluster randomized controlled trial [ENGAGE]. Cancer 121:2646–2654. doi:10.1002/cncr.29385
Aaronson NK, Ahmedzai S, Bergman B, Bullinger M, Cull A, Duez NJ, Filiberti A, Flechtner H, Fleishman SB, de Haes JCJM, Kaasa S, Klee M, Osoba D, Razavi D, Rofe PB, Schraub S, Sneeuw K, Sullivan M, Takeda F (1993) The European Organization for Research and Treatment of Cancer QLQ-C30: a quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst 85:365–376. doi:10.1093/jnci/85.5.36510.1093/jnci/85.5.365
van Andel G, Bottomley A, Fosså SD, Efficace F, Coens C, Guerif S, Kynaston H, Gontero P, Thalmann G, Akdas A, D’Haese S, Aaronson N (2008) An international field study of the EORTC QLQPR25: a questionnaire for assessing the healthrelated quality of life of patients with prostate cancer. Eur J Cancer Care 44:2418–2424. doi:10.1016/j.ejca.2008.07.030
Maringwa J, Quinten C, King M, Ringash J, Osoba D, Coens C, Martinelli F, Reeve BB, Gotay C, Greimel E, Flechtner H, Cleeland CS, Schmucker-Von Koch J, Weis J, Van Den Bent MJ, Stupp R, Taphoorn MJ, Bottomley A, Project obotEP, Group BC (2011) Minimal clinically meaningful differences for the EORTC QLQ-C30 and EORTC QLQ-BN20 scales in brain cancer patients. Ann Oncol 22:2107–2112. doi:10.1093/annonc/mdq726
Osoba D, Rodrigues G, Myles J, Zee B, Pater J (1998) Interpreting the significance of changes in health-related quality-of-life scores. J Clin Oncol 16:139–144
King MT (1996) The interpretation of scores from the EORTC quality of life questionnaire QLQ-C30. Qual Life Res 5:555–567. doi:10.1007/BF00439229
Cocks K, King MT, Velikova G, Martyn St-James M, Fayers PM, Brown JM (2011) Evidence-based guidelines for determination of sample size and interpretation of the European Organisation for the Research and Treatment of Cancer Quality of Life Questionnaire Core 30. J Clin Oncol 29:89–96. doi:10.1200/jco.2010.28.0107
Roth AJ, Rosenfeld B, Kornblith AB, Gibson C, Scher HI, Curley-Smart T, Holland JC, Breitbart W (2003) The memorial anxiety scale for prostate cancer. Cancer 97:2910–2918. doi:10.1002/cncr.11386
Zigmond AS, Snaith RP (1983) The hospital anxiety and depression scale. Acta Psychiatr Scand 67:361–370. doi:10.1111/j.1600-0447.1983.tb09716.x
Roth AJ, Nelson CJ, Rosenfeld B, Warshowski A, O’Shea N, Scher H, Holland JC, Slovin S, Curley-Smart T, Reynolds T, Breitbart W (2006) Assessing anxiety in men with prostate cancer: further data on the reliability and validity of the Memorial Anxiety Scale for Prostate Cancer (MAX–PC). Psychosomatics 47:340–347. doi:10.1176/appi.psy.47.4.340
Radloff LS (1977) The CES-D scale: a self-Report depression scale for research in the general population. Appl Psychol Meas 1:385–401. doi:10.1177/014662167700100306
Sirard JR, Melanson EL, Li L, Freedson PS (2000) Field evaluation of the Computer Science and Applications, Inc. physical activity monitor. Med Sci Sports Exerc 32:695–700
Freedson PS, Sirard J, Debold E, Pate R, Dowda M, Trost S, Sallis J (1998) Calibration of the Computer Science and Applications, Inc. (CSA) accelerometer. Med Sci Sports Exerc 30:777–781
Healy GN, Clark BK, Winkler EAH, Gardiner PA, Brown WJ, Matthews CE (2011) Measurement of adults’ sedentary time in population-based studies. Am J Prev Med 41:216–227. doi:10.1016/j.amepre.2011.05.005
Aadland E, Ylvisåker E (2015) Reliability of the Actigraph GT3X+ accelerometer in adults under free-living conditions. PLoS One 10(8):e0134606. doi:10.1371/journal.pone.0134606
Skolarus TA, Wolf AMD, Erb NL, Brooks DD, Rivers BM, Underwood W, Salner AL, Zelefsky MJ, Aragon-Ching JB, Slovin SF, Wittmann DA, Hoyt MA, Sinibaldi VJ, Chodak G, Pratt-Chapman ML, Cowens-Alvarado RL (2014) American Cancer Society prostate cancer survivorship care guidelines. CA Cancer J Clin 64:225–249. doi:10.3322/caac.21234
Little RJA (1988) A test of missing completely at random for multivariate data with missing values. J Am Statist Assoc 83:1198–1202. doi:10.2307/2290157
Cohen J (1990) Things I have learned (so far). Am Psychol 45:1304–1312. doi:10.1037/0003-066X.45.12.1304
Gaskin CJ, Happell B (2014) Power, effects, confidence, and significance: an investigation of statistical practices in nursing research. Int J Nurs Stud 51:795–806. doi:10.1016/j.ijnurstu.2013.09.014
Jaeschke R, Singer J, Guyatt GH (1989) Measurement of health status: ascertaining the minimal clinically important difference. Control Clin Trials 10:407–415. doi:10.1016/0197-2456(89)90005-6
Rock CL, Doyle C, Demark-Wahnefried W, Meyerhardt J, Courneya KS, Schwartz AL, Bandera EV, Hamilton KK, Grant B, McCullough M, Byers T, Gansler T (2012) Nutrition and physical activity guidelines for cancer survivors. CA Cancer J Clin 62:242–274. doi:10.3322/caac.21142
US Department of Health and Human Services (2008) 2008 Physical activity guidelines for Americans. US Department of Health and Human Services, Washington, DC
Bourke L, Smith D, Steed L, Hooper R, Carter A, Catto J, Albertsen PC, Tombal B, Payne HA, Rosario DJ (2016) Exercise for men with prostate cancer: a systematic review and meta-analysis. Eur Urol 69:693–703. doi:10.1016/j.eururo.2015.10.047
Mishra SI, Scherer RW, Geigle PM, Berlanstein DR, Topaloglu O, Gotay CC, Snyder C (2012) Exercise interventions on health-related quality of life for cancer survivors. Cochrane Database Syst Rev. doi:10.1002/14651858.CD007566.pub2
van Waart H, Stuiver MM, van Harten WH, Geleijn E, Kieffer JM, Buffart LM, de Maaker-Berkhof M, Boven E, Schrama J, Geenen MM, Meerum Terwogt JM, van Bochove A, Lustig V, van den Heiligenberg SM, Smorenburg CH, Hellendoorn-van Vreeswijk JAJH, Sonke GS, Aaronson NK (2015) Effect of low-intensity physical activity and moderate- to high-intensity physical exercise during adjuvant chemotherapy on physical fitness, fatigue, and chemotherapy completion rates: results of the PACES randomized clinical trial. J Clin Oncol 33:1918–1927. doi:10.1200/JCO.2014.59.1081
Rhodes RE, Mark RS, Temmel CP (2012) Adult sedentary behavior: a systematic review. Am J Prev Med 42:e3–e28. doi:10.1016/j.amepre.2011.10.020
Teychenne M, Ball K, Salmon J (2010) Sedentary behavior and depression among adults: a review. Int J Behav Med 17:246–254. doi:10.1007/s12529-010-9075-z
Lowe SS, Danielson B, Beaumont C, Watanabe SM, Baracos VE, Courneya KS (2014) Associations between objectively measured physical activity and quality of life in cancer patients with brain metastases. J Pain Symptom Manage 48:322–332. doi:10.1016/j.jpainsymman.2013.10.012
Phillips SM, Awick EA, Conroy DE, Pellegrini CA, Mailey EL, McAuley E (2015) Objectively measured physical activity and sedentary behavior and quality of life indicators in survivors of breast cancer. Cancer 121:4044–4052. doi:10.1002/cncr.29620
George SM, Alfano CM, Groves J, Karabulut Z, Haman KL, Murphy BA, Matthews CE (2014) Objectively measured sedentary time is related to quality of life among cancer survivors. PLoS One 9(2):e87937–e87937. doi:10.1371/journal.pone.0087937
Lynch BM, Cerin E, Owen N, Hawkes AL, Aitken JF (2011) Television viewing time of colorectal cancer survivors is associated prospectively with quality of life. Cancer Causes Control 22:1111–1120. doi:10.1007/s10552-011-9786-8
George SM, Alfano CM, Smith AW, Irwin ML, McTiernan A, Bernstein L, Baumgartner KB, Ballard-Barbash R (2013) Sedentary behavior, health-related quality of life and fatigue among breast cancer survivors. J Phys Act Health 10:350–358
Scott NW, Fayers PM, Aaronson NK, Bottomley A, de Graeff A, Groenvold M, Gundy C, Koller M, Petersen MA, Sprangers MAG (2008) EORTC QLQ-C30: Reference values. EORTC Headquarters, Brussels
Sutcliffe JP (1958) Error of measurement and the sensitivity of a test of significance. Psychometrika 23:9–17. doi:10.1007/BF02288974
Ferrari P, Friedenreich C, Matthews CE (2007) The role of measurement error in estimating levels of physical activity. Am J Epidemiol 166:832–840. doi:10.1093/aje/kwm148
Grant PM, Ryan CG, Tigbe WW, Granat MH (2006) The validation of a novel activity monitor in the measurement of posture and motion during everyday activities. Br J Sports Med 40:992–997. doi:10.1136/bjsm.2006.030262
Healy GN, Dunstan DW, Salmon J, Cerin E, Shaw JE, Zimmet PZ, Owen N (2008) Breaks in sedentary time: beneficial associations with metabolic risk. Diabetes Care 31:661–666. doi:10.2337/dc07-2046
Acknowledgments
This study was funded by the Australian Research Council (LP100200176) and the Prostate Cancer Foundation of Australia, with in-kind support from YMCA Victoria, Eastern Health, Epworth Healthcare, North Eastern Metropolitan Integrated Cancer Service, and Peter MacCallum Cancer Centre. Kerry S. Courneya is supported by the Canada Research Chairs Program. Jo Salmon is supported by a Principal Research Fellowship from the National Health & Medical Research Council (APP1026216).
Author information
Authors and Affiliations
Corresponding author
Additional information
This work was conducted when Dr Craike was employed at Deakin University. She is now employed at Victoria University.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Gaskin, C.J., Craike, M., Mohebbi, M. et al. Associations of objectively measured moderate-to-vigorous physical activity and sedentary behavior with quality of life and psychological well-being in prostate cancer survivors. Cancer Causes Control 27, 1093–1103 (2016). https://doi.org/10.1007/s10552-016-0787-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10552-016-0787-5