
Abstract
In this study of early functional changes in Parkinson’s disease (PD), we aimed to provide a comprehensive assessment of the development of changes in both cortical and subcortical neurophysiological brain activity, including their association with clinical measures of disease severity. Repeated resting-state MEG recordings and clinical assessments were obtained in the context of a unique longitudinal cohort study over a seven-year period using a multiple longitudinal design. We used linear mixed-models to analyze the relationship between neurophysiological (spectral power and functional connectivity) and clinical data. At baseline, early-stage (drug-naïve) PD patients demonstrated spectral slowing compared to healthy controls in both subcortical and cortical brain regions, most outspoken in the latter. Over time, spectral slowing progressed in strong association with clinical measures of disease progression (cognitive and motor). Global functional connectivity was not different between groups at baseline and hardly changed over time. Therefore, investigation of associations with clinical measures of disease progression were not deemed useful. An analysis of individual connections demonstrated differences between groups at baseline (higher frontal theta, lower parieto-occipital alpha2 band functional connectivity) and over time in PD patients (increase in frontal delta and theta band functional connectivity). Our results suggest that spectral measures are promising candidates in the search for non-invasive markers of both early-stage PD and of the ongoing disease process.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Parkinson’s disease is a progressive neurodegenerative disease characterized by classical motor symptoms as well as a wide range of non-motor symptoms, among which cognitive decline (Chaudhuri et al. 2006). The pathological hallmark of Parkinson’s disease is the deposition of alpha synuclein in the brain, which initially mainly affects the brainstem, including the neurons of the nigrostriatal dopamine system, and extends to widespread cortical brain regions in more advanced disease stages (Braak et al. 2003). This pathology affects the brain function, although its mechanism is as yet unknown.
Magnetoencephalography (MEG) can be used to measure brain activity with high temporal and good spatial resolution (Baillet 2017; Litvak et al. 2021). Changes in neurophysiological measures of cortical brain activity such as spectral slowing and loss of interactions between brain regions, i.e. functional connectivity, are well-established phenomena in Parkinson’s disease (Bosboom et al. 2006, 2009b; Caviness et al. 2007, 2016; Hassan et al. 2017; Stoffers et al. 2007). These changes correlate with clinical measures of disease progression (Geraedts et al. 2018; Olde Dubbelink et al. 2013a, 2013b; Yassine et al. 2022) and can have predictive value for cognitive deterioration, such as the conversion to Parkinson’s disease dementia (Arnaldi et al. 2017; Klassen et al. 2011; Olde Dubbelink et al. 2014b). Hence, neurophysiological patterns hold promise as biomarkers of the degenerative process in Parkinson’s disease, for instance for prognosis or the assessment of treatment effects of future disease-modifying therapies.
Already at the earliest Parkinson’s disease stages, slowing of oscillatory brain activity and functional connectome changes have been demonstrated (De Micco et al. 2021; Stoffers et al. 2007). As nigrostriatal changes lie at the heart of early-stage Parkinson’s disease (i.e. motor) symptoms, one would expect functional changes in subcortical brain regions as well. Previous neurophysiological studies have focused on cortical brain regions, with the exception of local field potentials recorded from the subthalamic nucleus in deep brain stimulation-treated patients. In recent years, increasing evidence suggests the feasibility to project MEG-signals onto other subcortical brain regions (Boon et al. 2017; Hillebrand and Barnes 2005; Hillebrand et al. 2012, 2016a, 2005; Pizzo et al. 2019), which allows for a reliable measurement of functional properties of these subcortical brain areas.
Previous longitudinal studies in Parkinson’s disease using EEG or MEG had a follow-up duration of approximately four years (Caviness et al. 2015; Olde Dubbelink et al. 2013a, 2013b; Yassine et al. 2022) or were performed in moderately advanced Parkinson’s disease patients (average disease duration of 8.5 years at baseline in that study) (Caviness et al. 2015). Hence, the full picture of the neurophysiological changes that occur throughout the course of Parkinson’s disease is currently lacking. Ideally, one would follow a cohort of Parkinson’s disease patients from disease onset up to a disease duration of 15–20 years. In our study we have met this aim by using a so-called ‘multiple longitudinal design’ in which we included patients with different baseline disease durations (ranging from early-stage, drug-naive patients to patients with a disease duration of 13 years) in combination with a seven year follow-up duration. We recently demonstrated the feasibility of combining data recorded longitudinally on two different MEG systems in healthy controls, by analyzing the MEG data in source-space and excluding the gamma band (Boon et al. 2021). In this study, the spectral power and functional connectivity results remained stable over time. This allowed us to combine the MEG data recorded in a Parkinson’s disease cohort over a period of seven years using two different recording systems (CTF at baseline and follow-up 1; Elekta Vectorview at follow-up 2).
In the present study, we assessed MEG-based measures of spectral power and functional connectivity (the corrected amplitude envelope correlation (AEC-c)) at three time points in a cohort that initially included 61 Parkinson’s disease patients and 16 healthy controls. We hypothesized to find neurophysiological changes in subcortical brain regions in de novo Parkinson’s disease, and expected these to be more prominent than the changes in cortical brain regions. In addition, we expected longitudinal neurophysiological changes in subcortical brain regions to be associated most strongly with Parkinson’s disease-related motor impairments and neurophysiological changes in (mainly posterior) cortical brain regions to be associated most strongly with cognitive decline (Boon et al. 2017; Olde Dubbelink et al. 2014b; Scheijbeler et al. 2022).
Materials and Methods
Participants
At baseline, 70 non-demented patients with idiopathic Parkinson’s disease (disease duration 0–13 years, including 18 early-stage drug-naïve (de novo) patients) and 21 healthy controls (age-matched to the de novo patients) were consecutively approached and included in this multiple longitudinal study at Amsterdam UMC from April 2003 to March 2006 (Boon et al. 2017; Olde Dubbelink et al. 2014a, 2014b, 2013a, 2013b; Stoffers et al. 2007). The inclusion and exclusion criteria have previously been described in (Stoffers et al. 2007). Patients underwent motor and cognitive assessments, as well as MEG and MRI recordings at three time points (BL and two follow-up visits scheduled approximately 4 and 7 years later). Only data of the BL study visit were used in case of the healthy controls (HCs), part of the follow-up data has previously been used (Boon et al. 2021). Figure 1 shows the number of participants at each time point, as well as the number of participants included in the final analysis (and the reason for exclusion). 61 patients (including 17 de novo patients) and 16 HCs were analyzed at baseline (BL), 39 patients at follow-up 1 (FU1), and 35 patients at follow-up 2 (FU2).

Flowchart of patient inclusion. PD Parkinson’s disease, MEG magnetoencephalography
All participants gave written informed consent to the research protocol, which was approved by the medical ethical committee of Amsterdam UMC, location VU University Medical Center (Amsterdam, The Netherlands). Ethics review conformed to the Helsinki declaration. All recordings/assessments were carried out in accordance with relevant guidelines and regulations. Reporting of this study meets the STROBE guidelines (Vandenbroucke et al. 2007).
Participants Characteristics
Disease duration was calculated on the basis of the patients’ estimation of the onset of the classical Parkinson’s disease motor symptoms. Educational level was determined on the basis of the International Standard Classification of Education (ISCED).(UNESCO 1997) Unified Parkinson’s Disease Rating Scale motor ratings (UPDRS-III) (Fahn S 1987) were obtained in the ‘ON’ medication state by a trained physician (with the exception of 17 de novo Parkinson’s disease patients at baseline who were not on dopaminergic medication yet). For each patient, the Hoehn and Yahr stage was determined (Hoehn and Yahr 1967). The total dose of dopamine replacement therapy was converted to a so-called levodopa equivalent daily dose (LEDD) as described previously (Olde Dubbelink et al. 2013a). Levodopa was always used in combination with a peripheral decarboxylase inhibitor. Two patients were using rivastigmine at the time of FU1 and one patient at the time of FU2. Global cognitive function was assessed using the Cambridge Cognitive Examination (CAMCOG) scale (Roth et al. 1986). Conversion to PD dementia was assessed using the clinical criteria recommended by the Movement Disorders Society Task Force (Dubois et al. 2007).
Data Acquisition
During all recordings, patients were on their usual dose of dopaminergic medication (note that the 17 de novo cases did not use dopaminergic medication at BL). BL and FU1 MEG data were acquired using a 151-channel whole-head MEG system (CTF systems Inc., Vancouver, Canada) in an eyes-closed resting-state condition for five minutes while participants were seated inside a magnetically shielded room. Sample rates of 312.5 (BL) and 625 Hz (FU1) were used during recordings. At the beginning and end of each recording the head position relative to the coordinate system of the helmet was assessed by leading small currents through three head position indicator (HPI) coils attached to the left and right pre-auricular points and the nasion. For more details on the recordings, see previous publications from our group (Boon et al. 2021; Olde Dubbelink et al. 2013a).
FU2 MEG data were recorded using a 306-channel Vectorview system (Elekta Neuromag, Oy, Helsinki, Finland) in an eyes-closed resting-state condition for five minutes in a supine position, with a sample rate of 1250 Hz. The head position relative to the MEG sensors was recorded continuously using the signals of four HPI coils. The coil positions were digitized before each recording, as well as the outline of the patient’s scalp (~ 500 points), using a 3D digitizer (Fastrak, Polhemus, Colchester, VT, USA).
Structural T1-weighted MR imaging was performed at all three time points (BL; 1.0 T, Impact, Siemens, Erlangen, Germany; FU1 and FU2; 3.0 T, GE Signa HDxt, Milwaukee, WI, USA). In preparation for the MR imaging at BL and FU1, vitamin E capsules were placed at the same anatomical landmarks where the three HPI coils had been placed during MEG-registration.
Data Preprocessing
Standard implementations of the analysis pipeline were used for both MEG systems as described below. FU1 MEG data were downsampled to 312.5 Hz to obtain the same sample rate as at BL. MEG channels that were malfunctioning, for example due to excessive noise, were identified based on visual inspection and not included in the further analysis (all by the same observer KTEOD; mean number of excluded channels: BL/FU1 2.4, range 2–7; FU2 6.7, range 2–11). BL and FU1 data were split into epochs (13.11 s, 4096 samples) and epochs containing artefacts were discarded (BL mean 2.5, range 0–11; FU1 mean 2.8, range 0–12). In addition, the temporal extension of Signal Space Separation (tSSS) in MaxFilter software (Elekta Neuromag Oy, version 2.2.15) was applied to FU2 data to remove artefacts (Taulu and Hari 2009; Taulu and Simola 2006), using a sliding window of 10 s and a subspace correlation-limit of 0.9.
Participants’ MEG data were co-registered to their structural MRIs using in-house software, in case of BL/FU1 through identification of the same anatomical landmarks (left and right pre-auricular points and nasion; estimated co-registration error < 6 mm) in both modalities, and in case of FU2 through a surface-matching procedure, with an estimated resulting accuracy of 4 mm (Whalen et al. 2008). For all three time points, the automated anatomical labelling (AAL) atlas was used to label the voxels in 78 cortical and 12 subcortical regions of interest (ROIs) in the subjects’ co-registered MRI using SPM (Gong et al. 2009; Tzourio-Mazoyer et al. 2002). In order to reconstruct a single time-series of neuronal activity for a ROI (Hillebrand et al. 2012) we used each ROI’s centroid as representative for that ROI (Hillebrand et al. 2016b). A scalar beamformer was used to reconstruct beamformer weights for each centroid using broadband data (0.5–48 Hz) (Hillebrand and Barnes 2005; Hillebrand et al. 2005) (Synthetic Aperture Magnetometry (SAM)) (Vrba and Robinson 2002) for BL and FU1, and Elekta’s beamformer implementation, a scalar beamformer comparable to SAM (version 2.2.15; Elekta Neuromag Oy) for FU2). Mean length of broadband data was 231 s (range 157 – 432 s) for BL, 252 s (range 130 – 328 s) for FU1, and 313 s (range 296 – 495 s) for FU2. Broadband data were projected through the normalized (Cheyne et al. 2007) beamformer weights for each centroid of the 90 ROIs. For further details on the projection of MEG data to source-space, see our previous publication on the healthy controls of this cohort (Boon et al. 2021). Subsequently, FU2 time-series were downsampled (4x, in order to obtain the same sample rate as at BL) and split into epochs of 4096 samples (13.11 s) as well.
Ten artefact and drowsiness-free epochs were selected per subject at each time point by visual analysis (KTEOD/LIB). For frequency band specific analyses, epochs were filtered in five canonical frequency bands (delta (0.5–4 Hz), theta (4–8 Hz), alpha1 (8–10 Hz), alpha2 (10–13 Hz, as the distinction between alpha1 and alpha2 oscillations may have functional significance (Klimesch et al. 2005)), and beta (13–30 Hz). We excluded the gamma band, as we previously demonstrated in healthy subjects that gamma power values were not stable between the two different MEG systems, possibly due to a difference in the handling of artefacts (Boon et al. 2021).
Data Analysis
Spectral and functional connectivity analyses were performed using in-house software (BrainWave, version 0.9.152.12.26; CJS, available from http://home.kpn.nl/stam7883/brainwave.html). We created group-averaged power spectra (0.5–30 Hz) for each time point separately, normalized the spectra using the area under the curve (Fig. 2A), and determined the peak frequency within the 4–13 Hz frequency range (spectral resolution of 0.076 Hz). Furthermore, for each ROI, we estimated frequency band specific relative power (relative to the total spectral power between 0.5 and 30 Hz) and functional connectivity with the rest of the brain.

Power spectral analysis. A Whole-group normalized power spectra at three time points, including the healthy controls (HC) at baseline (BL). Spectral power between 0.5 and 30 Hz was averaged over all brain regions. B Violin plots summarizing the baseline comparison between three groups; de novo PD patients, more advanced treated PD patients and HCs. A significance level of 0.05/6 (Bonferroni correction) was applied. C Violin plots summarizing the longitudinal analysis. Statistical testing was performed using linear mixed-models. A significance level of 0.05/6 (Bonferroni correction) was applied. n.s. non-significant, HC healthy control, FU1 follow-up 1, FU2 follow-up 2
We estimated functional connectivity using the AEC-c, an implementation of the AEC (Brookes et al. 2012; Bruns et al. 2000) corrected for volume conduction/field spread, using a symmetric orthogonalisation procedure (Brookes et al. 2012; Hipp et al. 2012) applied to each epoch: To adjust for any negative correlations, 1 was added to the raw AEC values and subsequently divided by 2, leading to values between 0 and 1, and with 0.5 indicating absence of functional connectivity. The AEC-c was calculated for all possible pairs of ROIs, leading to a 90*90 adjacency matrix. AEC-c values were subsequently averaged per ROI. This resulted in a single AEC-c value per ROI (per frequency band), reflecting the mean functional connectivity of that region with the rest of the brain.
Next, both relative power values and functional connectivity values were averaged for i) all cortical brain regions (regions 1–78; ii) all subcortical brain regions (regions 79–90, see Supplementary Table 1 for definitions and order of the regions). Results of 10 epochs were averaged per patient.
Statistical Analysis
Patient Characteristics
The baseline composition of the study cohort was statistically tested as follows: Age, disease duration, UPDRS-III score, LEDD total dose, and CAMCOG were tested using independent sample t-tests. Sex and HY score were tested using Chi-square tests and ISCED using Fisher’s exact test. The cohorts studied at BL, FU1 and FU2 showed differences due to drop-out of patients. Hence, our analysis can be considered as a missing data analysis. The group composition over time was therefore not statistically tested.
Spectral Power and Functional Connectivity: Baseline Comparison
First, we analyzed spectral power and functional connectivity averaged over (i) all cortical brain regions and (ii) all subcortical brain regions, separately for HCs, de novo patients and treated (more advanced) patients. Next, we performed linear mixed-models separately for the cortical and subcortical brain regions, with a grouping variable (HCs, de novo and more advanced treated PD patients; represented by dummy variables) and the covariates age, gender and ISCED (dichotomized at 3).
In order to explore whether neurophysiological characteristics of subcortical brain regions differed more from HCs than those of cortical brain regions, we created linear mixed-models with the neurophysiological measure as dependent variable, the grouping variable (control or de novo PD patient), location variable (cortical or subcortical), the interaction between the group and location variables, as well as the covariates age, gender and ISCED (dichotomized).
As an additional analysis, we explored whether functional connectivity between individual brain regions (connections) was significantly different between healthy controls and the two PD groups. Therefore, we applied permutation tests (N = 50,000; p < 0.05) on all 90*90 individual, with an FDR correction for the number of connections.
Spectral Power and Functional Connectivity: Longitudinal Changes
We used linear mixed-models to evaluate the longitudinal changes in spectral power and functional connectivity in Parkinson’s disease patients. Linear mixed-models can account for the dependency of the observations within the patient and the fact that not all patients had undergone a (complete) study visit at all three time points. In the linear mixed-models the time variable (BL, FU1, FU2) was treated as a categorical variable and represented by dummy variables. Age at baseline, disease duration at baseline, gender, ISCED (dichotomized), and LEDD were included in the model as covariates. MEG-machine was not included as covariate here, as it was redundant because of the inclusion of the time variable. Relative spectral power (per frequency band; delta to beta band), peak frequency, and functional connectivity (per frequency band; functional connectivity of one brain region with the rest of the brain) were each averaged over cortical and subcortical brain regions separately and were used as dependent variables.
Next, we explored whether the strength of the functional connections significantly changed over time (BL to FU1) for the PD group. Again, we applied permutation tests (N = 50,000; p < 0.05) on all individual connections, with an FDR correction for the number of connections.
Relationship Between Spectral Power Measures and Clinical Measures of Disease Progression
We analyzed the relationship between the longitudinal courses of the spectral measures and global measures of cognitive (CAMCOG) and motor (UPDRS-III) function using linear mixed-models. CAMCOG and UPDRS-III were treated as dependent variables, spectral measures (delta to beta relative power and peak frequency) as independent variables. Age at baseline, disease duration at baseline, gender, ISCED (dichotomized; only included in case of analyses involving CAMCOG), recording system (CTF versus Elekta), and LEDD were included in the model as covariates. Neurophysiological measures of i) cortical brain regions and ii) subcortical brain regions were used as independent variables in separate analyses. Due to collinearity of the neurophysiological measures, it was not possible to combine them in a single linear mixed-model.
Statistical analyses were performed using the IBM SPSS Statistics 26 software package (IBM Corporation, New York, USA). A significance level of 0.05/6 was applied in the baseline comparisons and the analyses on longitudinal changes, as we applied Bonferroni correction for the number of comparisons (comparisons between three groups (HC’s, early and more advanced PD patients) or three time points and two groups of brain regions (subcortical and cortical)), separately for each frequency band). In the other analyses, a significance level of 0.05 was applied. In the linear mixed-models, a random intercept was used. Supplementary Fig. 1 gives an overview of the statistical tests performed in this study.
Results
Patient Characteristics
Participant characteristics and details on statistics are summarized in Table 1. The HCs were age-matched to the de novo PD patients, the more advanced (treated) patients were significantly older. All 17 de novo patients were included in the longitudinal analysis, of which 9 completed all three study visits. Twenty-two patients had a ‘complete’ dataset and were analyzed at three time points. HCs had significantly better CAMCOG scores than both Parkinson’s disease groups (Table 1A). At FU1, three patients fulfilled the criteria for Parkinson’s disease dementia and at FU2 six patients fulfilled these criteria. The composition of the cohorts studied at BL, FU1 and FU2 are demonstrated in Table 1B.
Spectral Power
Figure 2A shows a global normalized power spectrum, group-averaged per time point, in which de novo and treated Parkinson’s disease patients were combined. At BL, the peak frequency was significantly lower in the Parkinson’s disease group than in the HC group (Fig. 2B). The peak frequency also significantly decreased further over time in the Parkinson’s disease group (Fig. 2C).
Looking at spectral power, the baseline analysis (Fig. 2B) demonstrates significantly higher relative theta band power in both Parkinson’s disease groups compared with healthy controls, both for cortical and subcortical brain regions. Relative alpha2 power and peak frequency were significantly lower in the Parkinson’s disease groups, both for cortical and subcortical brain regions. In addition, only for the cortical brain regions, alpha1 band power was significantly higher (all Parkinson’s disease patients) and beta band power significantly lower (treated patients). There were no significant differences between the de novo patients and the treated patients. In addition, using linear mixed-models, we found that de novo PD patients deviated from controls stronger for cortical than for subcortical brain regions for alpha1 and beta band power (p = 0.028 and 0.008, respectively).
Over time, the pattern of slowing further developed as we found increases in relative delta and theta power, and decreases in relative alpha2 and beta power. The magnitude of these changes was comparable between cortical and subcortical brain regions (Fig. 2C; see Supplementary Table 2 for statistics).
Functional Connectivity
There were no significant baseline group differences in the whole-brain functional connectivity analysis (Supplementary Fig. 2A). We also observed no significant longitudinal changes in whole-brain functional connectivity, except for a significant increase in subcortical beta band functional connectivity between FU1 and FU2 (Supplementary Fig. 2B). Because of the scarcity of results in the whole-brain analyses, functional connectivity was not used as input for the associations with clinical measures of disease severity.
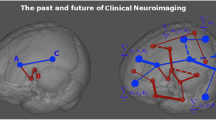
In the connection-specific analysis (Fig. 3) we found significantly higher theta band functional connectivity for the more advanced PD patients compared with HCs, mainly for the frontal connections. In addition, there was significantly lower alpha2 band functional connectivity of parieto-occipital connections for the PD group (both early and more advanced patients) compared with HCs.

Functional connectivity: Connection-specific analysis. Distribution of significant differences in functional connectivity between two individual brain regions. Differences are displayed on a standard brain viewed from (left to right) left lateral, top, and frontal (Xia et al. 2013). Red represents a significant increase in functional connectivity, blue a decrease. In the top two panels we compared two groups at baseline, in the lowest panel we compared two time points in the PD group. PD, Parkinson’s disease; HC, healthy control; BL, baseline; FU1, follow-up 1
In the longitudinal analysis of the PD group, between BL and FU1, we found significant increases in delta and theta band functional connectivity for frontal connections.
Relationship Between Neurophysiological Parameters and Clinical Measures of Disease Progression
We analyzed the longitudinal relationship between the spectral measures (delta to beta band relative power, peak frequency) and scores on the CAMCOG and UPDRS-III, separately for cortical and subcortical brain regions.
Both for cortical and subcortical brain regions, higher relative delta power was significantly associated with worse performance on CAMCOG. In addition, lower relative alpha1, alpha2, and beta power, as well as lower peak frequency, all in cortical and subcortical areas, were associated with worse performance on CAMCOG (Table 2). Conversely, higher (cortical) relative delta power and (cortical and subcortical) theta power were associated with higher scores on the UPDRS-III. In addition, lower relative (cortical) alpha2, lower relative (cortical and subcortical) beta power, and lower peak frequency (cortical and subcortical) were associated with worse motor performance (i.e. higher scores on UPDRS-III).
Next, for the spectral measures that demonstrated a significant association with a clinical measure, we displayed the cortical topographic distribution of (only) the significant associations as a post-hoc analysis. We restricted these figures to the cortical brain regions for visualization purposes, but we did calculate the individual associations of the subcortical brain regions (Supplementary Table 3). Figure 4 illustrates the longitudinal relations of relative beta band power and peak frequency with clinical measures of disease severity. The relationship between lower beta band power and worse cognitive performance was strongest for frontal cortical brain regions, whereas the relationship between lower beta band power and worse motor function was strongest (most negative) for the temporal-occipital brain regions. Interestingly, the relationship was weakest for the sensorimotor regions. For peak frequency, the strongest associations with clinical measures of disease severity were found for the temporal, parietal and occipital brain regions, both for the relationship with cognitive and motor performance. The remaining topographic distributions (delta-alpha2) can be found in Supplementary Fig. 3. Higher delta power in parieto-temporal regions was most strongly associated with cognitive and motor impairment (in the latter case also the occipital brain regions), higher frontal theta power with motor dysfunction, lower frontal alpha1 and alpha2 power with cognitive dysfunction, and lower parieto-temporal-occipital alpha2 power with motor impairment.

Topographic distribution of clinical associations. Distribution of longitudinal associations between relative beta band power and CAMCOG, relative beta band power and UPDRS-III, peak frequency and CAMCOG, peak frequency and UPDRS-III. Associations only concern cortical brain regions and are expressed as the estimated regression coefficient and displayed as a color-coded map on a parcellated template brain viewed from, in clockwise order, the left, top, right, right-midline and left-midline. Red represents a positive association, blue a negative association. Importantly, higher CAMCOG scores correspond to better cognitive functioning, whereas higher UPDRS-III scores correspond to worse motor functioning. Therefore, lower relative beta band power and lower peak frequency are associated with worse clinical (both cognitive and motor) functioning. All individual associations were statistically significant, except for a number of associations concerning the beta band (threshold around an estimated regression coefficient of -20). As we treated this analysis as a post-hoc analysis, we did not correct for multiple comparisons. The distribution of the remaining frequency bands that had significant associations with clinical measures of disease progression can be found in Supplementary Fig. 3
In Supplementary Table 3 we show the associations of individual subcortical brain regions with clinical measures of disease severity. The most outspoken pattern was the fact that activity in the hippocampus had the weakest association with CAMCOG and UPDRS-III for the frequency bands between delta and alpha2, but the strongest association with CAMCOG and UPDRS-III in the beta band. The results on peak frequency did not show a clear pattern.
Discussion
In this longitudinal MEG study, we used a multiple longitudinal design to be able to analyze the changes in brain activity in Parkinson’s disease patients from disease onset up to a disease duration of 15–20 years. In the earliest Parkinson’s disease stages, we found activity changes in both cortical and subcortical brain regions, but, surprisingly, the changes in subcortical regions were less prominent than the changes in the cortical regions. Furthermore, in our longitudinal analyses we observed a progressive spectral slowing of brain activity throughout the course of the disease. This spectral slowing was strongly associated with clinical measures of disease progression (cognition and motor function), most outspoken for the cortical brain regions. We did not observe whole-brain functional connectivity changes in the baseline analysis and whole-brain functional connectivity hardly changed over time. However, in the connection-specific analysis we did observe significant changes at baseline (increased theta, decreased alpha2 functional connectivity), as well as over time in PD patients (increase in frontal delta and theta band functional connectivity).
The general pattern of spectral slowing involved both cortical and subcortical brain regions. Although we expected early functional changes in subcortical brain regions to be more outspoken than cortical changes, the subcortical changes were weaker than the cortical changes in case of alpha1 and beta power. Nonetheless, spectral power values were highly correlated between cortical and subcortical brain regions (Pearson’s r ranging between 0.913 and 0.965 for different frequency bands, p < 0.001). Besides a physiological explanation for this high correlation, as cortical and subcortical activity are structurally connected, field spread may have played a role, which is not corrected for in case of spectral analyses. Clearly, we do not know whether small subcortical changes may have preceded cortical changes at the premotor disease stage. Also, perhaps some of the subcortical changes were too local to be picked up by our MEG system, as the spatial resolution deeper in the brain is not as good as at the cortical level (Hillebrand and Barnes 2002). In addition, local (subcortical) pathological changes may have more distant (cortical) effects via ascending neurotransmitter systems. Spectral slowing at the cortical level is hypothesized to be a consequence of dopaminergic, noradrenergic, serotonergic and cholinergic dysfunction (Bosboom et al. 2009a; Détári et al. 1999; Rea et al. 2021) and could also be an effect of local Lewy body and tau pathology in thalamocortical circuits (Freunberger et al. 2011; Steriade et al. 1990). There are no previous EEG/MEG studies in early-stage Parkinson’s disease to compare our results with, but fMRI studies have shown functional changes (loss of functional connectivity) within the basal ganglia circuit in early-stage Parkinson’s disease (Rolinski et al. 2015; Szewczyk-Krolikowski et al. 2014) that were paralleled by whole-brain changes in activity (Pan et al. 2017).
We found strong longitudinal associations between spectral measures (spectral slowing) and clinical measures of disease severity. Based on the regression coefficients, we conclude that subcortical spectral measures were associated equally strongly with cognitive performance (CAMCOG) as cortical spectral measures (Table 2). However, unexpectedly, subcortical spectral measures were less strongly associated with motor function (UPDRS-III) than with cognitive performance (CAMCOG). Also, of the individual subcortical brain regions, relative beta band power of the hippocampus was most strongly associated with CAMCOG and UPDRS-III. Moreover, relative beta band power in the sensorimotor cortex was only poorly associated with UPDRS-III scores, compared to the rest of the cortex. The finding that both subcortical (except the hippocampus) spectral measures and beta band power in the sensorimotor cortex were associated poorly with UPDRS-III scores may originate from compensatory mechanisms secondary to motor impairment, as was previously hypothesized (Hirschmann et al. 2013; Pollok et al. 2013). Alternatively, the lack of strong associations may result from treatment with dopaminergic medication. The amount of dopaminergic medication (LEDD) is associated with lower relative beta power in the motor cortex (Pearson’s r left motor cortex, -0.213 p = 0.015, right motor cortex, -0.240 p = 0.005), but this could be both a disease effect or a treatment effect. Supplementary Fig. 4 demonstrates that sensorimotor beta power remains largely intact against a background of generalized slowing of cortical brain activity, especially between BL and FU1, despite worsening motor scores over time. For further considerations regarding the complex interplay between motor function and beta band power/functional connectivity we refer the reader to our review on this topic (Boon et al. 2019).
When considering the region-specific post-hoc analyses of the other frequency bands, we found that cognitive decline and motor dysfunction were related to spectral slowing, sometimes in the same brain regions (see for example peak frequency in Fig. 4), sometimes in different brain regions (see alpha2 in Supplementary Fig. 3). As hypothesized, lower peak frequency in posterior cortical brain regions correlated strongest with global cognitive decline (Fig. 4). This may reflect ‘posterior cortical dysfunction’, a clinical profile that may indicate a higher risk of developing PD dementia (Kehagia et al. 2013).
A correlation of oscillatory slowing with motor dysfunction has only been reported incidentally (Morita et al. 2009) and has not been found in other studies (Geraedts et al. 2018; Olde Dubbelink et al. 2013a). Possibly, our long follow-up duration allowed us to find the correlations between spectral slowing and motor dysfunction. Motor and cognitive impairment may be associated with spectral slowing via a general underlying mechanism. When we added UPDRS-III performance as a covariate in the linear mixed-model for the association between CAMCOG and peak frequency, the association remained present (standardized effect size 2.32, p = 0.001), but not the other way around (standardized effect size -1.50, p = 0.128). We therefore conclude that, although motor and cognitive impairment are both related to the same underlying disease process, their pathophysiology does not fully overlap.
We chose not to include functional connectivity in our analyses of longitudinal associations with clinical measures of disease severity. At the whole-brain baseline analysis, we did not observe significant group differences in functional connectivity and over time, only subcortical beta band functional connectivity significantly changed. This was unexpected, as a previous analysis in the same cohort showed longitudinal decreases in alpha1 and alpha2 functional connectivity, although only between baseline and FU1 and with another measure of functional connectivity (Olde Dubbelink et al. 2013b). In addition, a recent high-density EEG study with a longitudinal design demonstrated a progressive loss of functional connectivity in correlation with global cognitive decline and lateralization of motor symptoms (Yassine et al. 2022). The differences between the present and previous study may partly be explained by the fact that AEC-c is an amplitude-based measure that is fundamentally different from the phase-based measures (phase lag index, phase locking value) that were used in other longitudinal studies on PD patients (Olde Dubbelink et al. 2013b; Yassine et al. 2022).
When we additionally performed a connection-specific analysis, we did observe local differences in functional connectivity. We found higher theta band functional connectivity of frontal connections and lower alpha2 band functional connectivity of parieto-occipital connections in PD patients compared with HCs. The loss of alpha2-band functional connectivity in PD patients is in line with previous studies in PD (Olde Dubbelink et al. 2013b; Yassine et al. 2022), although in these studies the changes were present throughout the brain. The parieto-occipital changes in alpha2 functional connectivity match the observations in Alzheimer’s disease (AD), in which the same (amplitude-based) functional connectivity measure was used (Schoonhoven et al. 2022). In addition, in this latter study, higher delta (AEC-d) and theta band (phase lag index) functional connectivity was seen in AD patients, which may reflect a general tendency to find higher functional connectivity values for slower frequencies in neurodegenerative diseases. In our connection-specific analysis, we found higher frontal theta band functional connectivity in PD patients, both at baseline and during follow-up.
The results of the connection-specific analysis indicate that potentially important findings can be missed in a whole-brain analysis in which subtle differences may be ‘averaged out’. Furthermore, the addition of a third time point and a different MEG system may have confounded the analysis. The only significant whole-brain change we observed was an increase in beta band functional connectivity between FU1 and FU2. Since an increase in beta band functional connectivity was also present in our healthy control group, this may be related to the change from one MEG system to the other (Boon et al. 2021).
Our results confirm that neurophysiological patterns are good candidates in the search for biomarkers of the degenerative process in Parkinson’s disease. Although we did not study the risk of conversion to Parkinson’s disease dementia, a previous analysis in this study cohort demonstrated that lower beta band power, especially in the posterior brain regions, was a strong predictor for conversion (Olde Dubbelink et al. 2014b). Our result in Fig. 4 was therefore somewhat surprising, as we found that beta band power of frontal cortical brain regions correlated strongest with global cognitive decline. The identification of a subgroup of Parkinson’s disease patients at high risk for dementia may be important for patients and caregivers in the context of advanced care planning, and also for future studies aimed at disease-modifying therapies to slow down cognitive decline. In the latter case, a neurophysiological biomarker may also serve as an objective read-out parameter of treatment success.
A strength of the current analysis is the multiple longitudinal design with a long follow-up duration of seven years, which allowed us to longitudinally cover 15–20 years of the disease course. In addition, the inclusion of a third time point (second follow-up) adds robustness to previously published results on spectral power at the first two time points (Olde Dubbelink et al. 2013a), as it confirms that the observed trends in spectral slowing are progressive over time. In addition, this is the first MEG study exploring the presence of subcortical neurophysiological changes in the earliest clinical motor stages of Parkinson’s disease, as well as the further development of these changes over time. Three potential limitations of our study deserve consideration. First, our baseline cohort decreased from 61 patients at BL to 39 patients at FU1. This is explained by the fact that data of 19 patients could not be used (low quality data, no MRI-scan; see also Fig. 1). 23 patients were lost to follow-up 2, possibly due to high disease burden. Given that this group was clinically more severely affected, the dropout of these subjects can only have led to an underestimation of true disease effects. In addition, our linear mixed models account for missing data, so that reliable longitudinal associations could still be established. Second, several subjects could not be included in the follow-up visits because they had poor-quality data or because they were lost to follow-up (see Fig. 1 for an overview). The majority of missing data was due to poor-quality MEG or MRI data, which is a random phenomenon. We do not have an overview of the reasons why patients were lost to follow-up, but there may have been a selective dropout of patients with a high (subjective) disease burden. However, this could only have led to an underestimation of the true effects.
Third, although there is increasing evidence that projecting MEG to subcortical sources is feasible, MEG is most sensitive to cortical sources (Hillebrand and Barnes 2002). The sensitivity for subcortical sources can be further improved using new analysis techniques such as ‘blind source separation’ (López-Madrona et al. 2022; Pizzo et al. 2019), methods that increase the contrast between cortical and subcortical sources (Quraan et al. 2011), or in-mouth sensors (Tierney et al. 2021).
In conclusion, already at the earliest disease stages of Parkinson’s disease, there are neurophysiological changes in Parkinson’s disease patients both at the subcortical and cortical level, most outspoken for the latter. In our analysis using a multiple longitudinal design, spanning 15–20 years of disease duration, we found strong longitudinal associations between spectral slowing of brain activity and clinical measures of disease severity, especially cognition. Functional connectivity changes were present, but only localized and not at the whole-brain level. Our results indicate that spectral power is a promising candidate in the search for a non-invasive marker to monitor the ongoing disease process in Parkinson’s disease.
References
Arnaldi D, De Carli F, Famà F, Brugnolo A, Girtler N, Picco A, Pardini M, Accardo J, Proietti L, Massa F, Bauckneht M, Morbelli S, Sambuceti G, Nobili F (2017) Prediction of cognitive worsening in de novo Parkinson’s disease: clinical use of biomarkers. Mov Disord 32(12):1738–1747
Baillet S (2017) Magnetoencephalography for brain electrophysiology and imaging. Nat Neurosci 20(3):327–339
Boon LI, Hillebrand A, Dubbelink KTO, Stam CJ, Berendse HW (2017) Changes in resting-state directed connectivity in cortico-subcortical networks correlate with cognitive function in Parkinson’s disease. Clin Neurophysiol 128(7):1319–1326
Boon LI, Geraedts VJ, Hillebrand A, Tannemaat MR, Contarino MF, Stam CJ, Berendse HW (2019) A systematic review of MEG-based studies in Parkinson’s disease: the motor system and beyond. Hum Brain Mapp 40(9):2827–2848
Boon LI, Tewarie P, Berendse HW, Stam CJ, Hillebrand A (2021) Longitudinal consistency of source-space spectral power and functional connectivity using different magnetoencephalography recording systems. Sci Rep 11(1):16336
Bosboom JL, Stoffers D, Stam CJ, van Dijk BW, Verbunt J, Berendse HW, Wolters EC (2006) Resting state oscillatory brain dynamics in Parkinson’s disease: an MEG study. Clin Neurophysiol 117(11):2521–2531
Bosboom JL, Stoffers D, Stam CJ, Berendse HW, Wolters EC (2009a) Cholinergic modulation of MEG resting-state oscillatory activity in Parkinson’s disease related dementia. Clin Neurophysiol 120(5):910–915
Bosboom JL, Stoffers D, Wolters EC, Stam CJ, Berendse HW (2009) MEG resting state functional connectivity in Parkinson’s disease related dementia. J Neural Transm 116(2):193–202
Braak H, Del Tredici K, Rüb U, De Vos RA, Steur ENJ, Braak E (2003) Staging of brain pathology related to sporadic Parkinson’s disease. Neurobiol Aging 24(2):197–211
Briels CT, Schoonhoven DN, Stam CJ, de Waal H, Scheltens P, Gouw AA (2020) Reproducibility of EEG functional connectivity in Alzheimer’s disease. Alzheimers Res Ther 12(1):68
Brookes MJ, Woolrich MW, Barnes GR (2012) Measuring functional connectivity in MEG: a multivariate approach insensitive to linear source leakage. Neuroimage 63(2):910–920
Bruns A, Eckhorn R, Jokeit H, Ebner A (2000) Amplitude envelope correlation detects coupling among incoherent brain signals. NeuroReport 11(7):1509–1514
Caviness JN, Hentz JG, Evidente VG, Driver-Dunckley E, Samanta J, Mahant P, Connor DJ, Sabbagh MN, Shill HA, Adler CH (2007) Both early and late cognitive dysfunction affects the electroencephalogram in Parkinson’s disease. Parkinsonism Relat Disord 13(6):348–354
Caviness JN, Hentz JG, Belden CM, Shill HA, Driver-Dunckley ED, Sabbagh MN, Powell JJ, Adler CH (2015) Longitudinal EEG changes correlate with cognitive measure deterioration in Parkinson’s disease. J Parkinsons Dis 5(1):117–124
Caviness JN, Utianski RL, Hentz JG, Beach TG, Dugger BN, Shill HA, Driver-Dunckley ED, Sabbagh MN, Mehta S, Adler CH (2016) Differential spectral quantitative electroencephalography patterns between control and Parkinson’s disease cohorts. Eur J Neurol 23(2):387–392
Chaudhuri KR, Healy DG, Schapira AH (2006) Non-motor symptoms of Parkinson’s disease: diagnosis and management. Lancet Neurol 5(3):235–245
Cheyne D, Bostan AC, Gaetz W, Pang EW (2007) Event-related beamforming: a robust method for presurgical functional mapping using MEG. Clin Neurophysiol 118(8):1691–1704
Colclough GL, Woolrich MW, Tewarie PK, Brookes MJ, Quinn AJ, Smith SM (2016) How reliable are MEG resting-state connectivity metrics? Neuroimage 138:284–293
De Micco R, Agosta F, Basaia S, Siciliano M, Cividini C, Tedeschi G, Filippi M, Tessitore A (2021) Functional connectomics and disease progression in drug-Naïve Parkinson’s disease patients. Mov Disord 36(7):1603–1616
Demuru M, Gouw AA, Hillebrand A, Stam CJ, van Dijk BW, Scheltens P, Tijms BM, Konijnenberg E, Ten Kate M, den Braber A, Smit DJA, Boomsma DI, Visser PJ (2017) Functional and effective whole brain connectivity using magnetoencephalography to identify monozygotic twin pairs. Sci Rep 7(1):9685
Détári L, Rasmusson DD, Semba K (1999) The role of basal forebrain neurons in tonic and phasic activation of the cerebral cortex. Prog Neurobiol 58(3):249–277
Dubois B, Burn D, Goetz C, Aarsland D, Brown RG, Broe GA, Dickson D, Duyckaerts C, Cummings J, Gauthier S, Korczyn A, Lees A, Levy R, Litvan I, Mizuno Y, McKeith IG, Olanow CW, Poewe W, Sampaio C, Tolosa E, Emre M (2007) Diagnostic procedures for Parkinson’s disease dementia: recommendations from the movement disorder society task force. Mov Disord 22(16):2314–2324
Fahn S, E.R., Committee Members of the UPDRS Develeopment., 1987. The unified Parkinson's disease rating scale. Recent developments in Parkinson's disease. . 2nd ed. Florham Park, NY: Macmillan Healthcare Information: p.153–163.
Freunberger R, Werkle-Bergner M, Griesmayr B, Lindenberger U, Klimesch W (2011) Brain oscillatory correlates of working memory constraints. Brain Res 1375:93–102
Geraedts VJ, Marinus J, Gouw AA, Mosch A, Stam CJ, van Hilten JJ, Contarino MF, Tannemaat MR (2018) Quantitative EEG reflects non-dopaminergic disease severity in Parkinson’s disease. Clin Neurophysiol 129(8):1748–1755
Gong G, He Y, Concha L, Lebel C, Gross DW, Evans AC, Beaulieu C (2009) Mapping anatomical connectivity patterns of human cerebral cortex using in vivo diffusion tensor imaging tractography. Cereb Cortex 19(3):524–536
Hassan M, Chaton L, Benquet P, Delval A, Leroy C, Plomhause L, Moonen AJ, Duits AA, Leentjens AF, van Kranen-Mastenbroek V, Defebvre L, Derambure P, Wendling F, Dujardin K (2017) Functional connectivity disruptions correlate with cognitive phenotypes in Parkinson’s disease. Neuroimage Clin 14:591–601
Hillebrand A, Barnes GR (2002) A quantitative assessment of the sensitivity of whole-head MEG to activity in the adult human cortex. Neuroimage 16(3 Pt 1):638–650
Hillebrand A, Barnes GR (2005) Beamformer analysis of MEG data. Int Rev Neurobiol 68:149–171
Hillebrand A, Singh KD, Holliday IE, Furlong PL, Barnes GR (2005) A new approach to neuroimaging with magnetoencephalography. Hum Brain Mapp 25(2):199–211
Hillebrand A, Barnes GR, Bosboom JL, Berendse HW, Stam CJ (2012) Frequency-dependent functional connectivity within resting-state networks: an atlas-based MEG beamformer solution. Neuroimage 59(4):3909–3921
Hillebrand A, Nissen I, Ris-Hilgersom I, Sijsma N, Ronner H, van Dijk B, Stam C (2016a) Detecting epileptiform activity from deeper brain regions in spatially filtered MEG data. Clin Neurophysiol 127(8):2766–2769
Hillebrand A, Tewarie P, Van Dellen E, Yu M, Carbo EW, Douw L, Gouw AA, Van Straaten EC, Stam CJ (2016b) Direction of information flow in large-scale resting-state networks is frequency-dependent. Proc Natl Acad Sci USA 113(14):3867–3872
Hipp JF, Hawellek DJ, Corbetta M, Siegel M, Engel AK (2012) Large-scale cortical correlation structure of spontaneous oscillatory activity. Nat Neurosci 15(6):884–890
Hirschmann J, Ozkurt TE, Butz M, Homburger M, Elben S, Hartmann CJ, Vesper J, Wojtecki L, Schnitzler A (2013) Differential modulation of STN-cortical and cortico-muscular coherence by movement and levodopa in Parkinson’s disease. Neuroimage 68:203–213
Hoehn MM, Yahr MD (1967) Parkinsonism. onset, progression, and mortality. Neurology 17(5):427–427
Kehagia AA, Barker RA, Robbins TW (2013) Cognitive impairment in Parkinson’s disease: the dual syndrome hypothesis. Neurodegener Dis 11(2):79–92
Klassen BT, Hentz JG, Shill HA, Driver-Dunckley E, Evidente VG, Sabbagh MN, Adler CH, Caviness JN (2011) Quantitative EEG as a predictive biomarker for Parkinson disease dementia. Neurology 77(2):118–124
Klimesch W, Schack B, Sauseng P (2005) The functional significance of theta and upper alpha oscillations. Exp Psychol 52(2):99–108
Litvak V, Florin E, Tamás G, Groppa S, Muthuraman M (2021) EEG and MEG primers for tracking DBS network effects. Neuroimage 224:117447
López-Madrona VJ, Medina Villalon S, Badier JM, Trébuchon A, Jayabal V, Bartolomei F, Carron R, Barborica A, Vulliémoz S, Alario FX, Bénar CG (2022) Magnetoencephalography can reveal deep brain network activities linked to memory processes. Hum Brain Mapp
Morita A, Kamei S, Serizawa K, Mizutani T (2009) The relationship between slowing EEGs and the progression of Parkinson’s disease. J Clin Neurophysiol 26(6):426–429
Olde Dubbelink KT, Stoffers D, Deijen JB, Twisk JW, Stam CJ, Berendse HW (2013a) Cognitive decline in Parkinson’s disease is associated with slowing of resting-state brain activity: a longitudinal study. Neurobiol Aging 34(2):408–418
Olde Dubbelink KT, Stoffers D, Deijen JB, Twisk JW, Stam CJ, Hillebrand A, Berendse HW (2013b) Resting-state functional connectivity as a marker of disease progression in Parkinson’s disease: a longitudinal MEG study. Neuroimage Clin 2:612–619
Olde Dubbelink KT, Hillebrand A, Stoffers D, Deijen JB, Twisk JW, Stam CJ, Berendse HW (2014a) Disrupted brain network topology in Parkinson’s disease: a longitudinal magnetoencephalography study. Brain 137(Pt 1):197–207
Olde Dubbelink KT, Hillebrand A, Twisk JW, Deijen JB, Stoffers D, Schmand BA, Stam CJ, Berendse HW (2014b) Predicting dementia in Parkinson disease by combining neurophysiologic and cognitive markers. Neurology 82(3):263–270
Pan P, Zhang Y, Liu Y, Zhang H, Guan D, Xu Y (2017) Abnormalities of regional brain function in Parkinson’s disease: a meta-analysis of resting state functional magnetic resonance imaging studies. Sci Rep 7(1):40469
Pizzo F, Roehri N, Medina Villalon S, Trébuchon A, Chen S, Lagarde S, Carron R, Gavaret M, Giusiano B, McGonigal A, Bartolomei F, Badier JM, Bénar CG (2019) Deep brain activities can be detected with magnetoencephalography. Nat Commun 10(1):971
Pollok B, Kamp D, Butz M, Wojtecki L, Timmermann L, Sudmeyer M, Krause V, Schnitzler A (2013) Increased SMA-M1 coherence in Parkinson’s disease—pathophysiology or compensation? Exp Neurol 247:178–181
Quraan MA, Moses SN, Hung Y, Mills T, Taylor MJ (2011) Detection and localization of hippocampal activity using beamformers with MEG: a detailed investigation using simulations and empirical data. Hum Brain Mapp 32(5):812–827
Rea RC, Berlot R, Martin SL, Craig CE, Holmes PS, Wright DJ, Bon J, Pirtošek Z, Ray NJ (2021) Quantitative EEG and cholinergic basal forebrain atrophy in Parkinson’s disease and mild cognitive impairment. Neurobiol Aging 106:37–44
Rolinski M, Griffanti L, Szewczyk-Krolikowski K, Menke RAL, Wilcock GK, Filippini N, Zamboni G, Hu MTM, Mackay CE (2015) Aberrant functional connectivity within the basal ganglia of patients with Parkinson’s disease. NeuroImage 8:126–132
Roth M, Tym E, Mountjoy CQ, Huppert FA, Hendrie H, Verma S, Goddard R (1986) CAMDEX. A standardised instrument for the diagnosis of mental disorder in the elderly with special reference to the early detection of dementia. Br J Psychiatry 149:698–709
Scheijbeler EP, Schoonhoven DN, Engels MMA, Scheltens P, Stam CJ, Gouw AA, Hillebrand A (2022) Generating diagnostic profiles of cognitive decline and dementia using magnetoencephalography. Neurobiol Aging 111:82–94
Schoonhoven DN, Briels CT, Hillebrand A, Scheltens P, Stam CJ, Gouw AA (2022) Sensitive and reproducible MEG resting-state metrics of functional connectivity in Alzheimer’s disease. Alzheimers Res Ther 14(1):38
Steriade M, Gloor P, Llinas RR, Da Silva FL, Mesulam M-M (1990) Basic mechanisms of cerebral rhythmic activities. Electroencephalogr Clin Neurophysiol 76(6):481–508
Stoffers D, Bosboom JL, Deijen JB, Wolters EC, Berendse HW, Stam CJ (2007) Slowing of oscillatory brain activity is a stable characteristic of Parkinson’s disease without dementia. Brain 130(Pt 7):1847–1860
Szewczyk-Krolikowski K, Menke RA, Rolinski M, Duff E, Salimi-Khorshidi G, Filippini N, Zamboni G, Hu MT, Mackay CE (2014) Functional connectivity in the basal ganglia network differentiates PD patients from controls. Neurology 83(3):208–214
Taulu S, Hari R (2009) Removal of magnetoencephalographic artifacts with temporal signal-space separation: demonstration with single-trial auditory-evoked responses. Hum Brain Mapp 30(5):1524–1534
Taulu S, Simola J (2006) Spatiotemporal signal space separation method for rejecting nearby interference in MEG measurements. Phys Med Biol 51(7):1759–1768
Tierney TM, Levy A, Barry DN, Meyer SS, Shigihara Y, Everatt M, Mellor S, Lopez JD, Bestmann S, Holmes N, Roberts G, Hill RM, Boto E, Leggett J, Shah V, Brookes MJ, Bowtell R, Maguire EA, Barnes GR (2021) Mouth magnetoencephalography: A unique perspective on the human hippocampus. Neuroimage 225:117443
Tzourio-Mazoyer N, Landeau B, Papathanassiou D, Crivello F, Etard O, Delcroix N, Mazoyer B, Joliot M (2002) Automated anatomical labeling of activations in SPM using a macroscopic anatomical parcellation of the MNI MRI single-subject brain. Neuroimage 15(1):273–289
UNESCO (1997) International standard classification of education (ISCED). http://www.uis.unesco.org/Education/Pages/international-standardclassification-of-education.aspx
Vandenbroucke JP, von Elm E, Altman DG, Gøtzsche PC, Mulrow CD, Pocock SJ, Poole C, Schlesselman JJ, Egger M (2007) Strengthening the reporting of observational studies in epidemiology (STROBE): explanation and elaboration. PLoS Med 4(10):e297
Vrba J, Robinson S (2002) SQUID sensor array configurations for magnetoencephalography applications. Supercond Sci Technol 15(9):R51
Whalen C, Maclin EL, Fabiani M, Gratton G (2008) Validation of a method for coregistering scalp recording locations with 3D structural MR images. Hum Brain Mapp 29(11):1288–1301
Xia M, Wang J, He Y (2013) BrainNet Viewer: a network visualization tool for human brain connectomics. PLoS ONE 8(7):e68910
Yassine S, Gschwandtner U, Auffret M, Achard S, Verin M, Fuhr P, Hassan M (2022) Functional Brain Dysconnectivity in Parkinson’s Disease: A 5-Year Longitudinal Study. Mov Disord 37(7):1444–1453
Acknowledgements
We thank Kim T.E. Olde Dubbelink (KTEOD) for identifying the study subjects and obtaining MEG data, as well as for her help in preprocessing and epoch selection for all three time points.
Funding
This project was supported by Stichting Parkinson NL.
Author information
Authors and Affiliations
Contributions
Conceptualization: LIB, AH, MMS, CJS, HWB Data curation: LIB, AH, HWB Collection of the data: AH, CJS, HWB Analysis: LIB, AH, JT, CJS, HWB Writing original draft: LIB All authors reviewed the manuscript
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Handling Editor: Seppo Ahlfors
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Boon, L.I., Hillebrand, A., Schoonheim, M.M. et al. Cortical and Subcortical Changes in MEG Activity Reflect Parkinson’s Progression over a Period of 7 Years. Brain Topogr 36, 566–580 (2023). https://doi.org/10.1007/s10548-023-00965-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10548-023-00965-w