
Abstract
Cell shrinkage is one of the earliest events during apoptosis. Cell shrinkage also occurs upon hypertonic stress, and previous work has shown that hypertonicity-induced cation channels (HICCs) underlie a highly efficient mechanism of recovery from cell shrinkage, called the regulatory volume increase (RVI), in many cell types. Here, the effects of HICC activation on staurosporine-induced apoptotic volume decrease (AVD) and apoptosis were studied in HeLa cells by means of electronic cell sizing and whole-cell patch-clamp recording. It was found that hypertonic stress reduces staurosporine-induced AVD and cell death (associated with caspase-3/7 activation and DNA fragmentation), and that this effect was actually due to activation of the HICC. On the other hand, staurosporine was found to significantly reduce osmotic HICC activation. It is concluded that AVD and RVI reflect two fundamentally distinct functional modes in terms of the activity and role of the HICC, in a shrunken cell. Our results also demonstrate, for the first time, the ability of the HICC to rescue cells from the process of programmed cell death.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
It has become increasingly evident in recent years that the mechanisms of cell volume regulation are employed in a variety of physiological processes, in addition to just the maintenance of cell homeostasis. Among these processes are the coordination of transport across the apical and basolateral membranes in epithelia, the locomotion of cells, the regulation of metabolic processes in the liver and, most notably, the control of cell proliferation and apoptosis [1–3].
Since the rates of ion transport through channels are some 4–5 orders of magnitude higher than those achieved by transporters (carriers and pumps), any modulation of ion channel activity may serve as a rapid and efficient mechanism of osmolyte transport and cell volume regulation. Accordingly, hypertonicity-induced cation channels (HICCs) were found to be the main mediators of the “regulatory volume increase (RVI)” of a shrunken cell, whenever a system was analysed in a quantitative fashion [3–5]. Despite the low selectivity of HICCs for Na+ over K+, activation of these channels leads to an actual net uptake of cations, which is mainly due to the membrane voltage, which is negative intracellularly. Anions and osmotically obliged water follow, allowing the cell to complete the process of RVI [3–5].
Persistent isotonic shrinkage of a given cell, as opposed to hypertonicity-induced shrinkage, is one of the hallmarks of apoptosis. In many instances, this “apoptotic volume decrease (AVD)” employs the activation of K+ channels, which serve as the main routes of K+ exit [6–9]. Cl− channels also should open, with this parallel transport strongly depending, however, on whether or not the electro-chemical driving forces actually favour conductive Cl− export [1, 2, 10–12].
The question is thus raised of how hypertonic stress might interfere with AVD. Would osmotic shrinkage facilitate the process? Or would the activation of HICCs or RVI oppose the induction of apoptosis?
Materials and methods
Cell culture
Human cervix HeLa cells were grown as monolayers in minimum essential medium supplemented with 10% fetal bovine serum, 100 μg/ml streptomycin and 40 IU/ml penicillin, under 95% air/5% CO2 at 37°C. For the experiments, cells were mechanically detached from the plastic substrate of the culture flasks with a jet of culture medium and then kept in suspension for 15–120 min.
Determination of cell volume
Changes of HeLa cell volume were quantified by means of electronic cell sizing on a Coulter-type analyzer (CDA-500; Sysmex, Kobe, Japan), as previously described [13]. The experimental solution contained (in mM): NaCl, 95; KCl, 4.5; MgCl2, 1; CaCl2, 1; NaHCO3, 10; HEPES, 5. Osmolality was adjusted to values from 300 to 600 mosmol/kg-H2O by adding mannitol under osmometric control (OM802; Vogel, Giessen, Germany). Measurements were performed at room temperature.
Patch-clamp experiments
Membrane currents were recorded in the fast whole-cell mode of the patch-clamp technique using 2 MΩ borosilicate pipettes. Currents were recorded with an Axopatch 200B amplifier (Molecular Devices, Union City, CA), filtered at 5 kHz with a four-pole Bessel filter and digitized at 20 kHz. pClamp 9.02 software (Molecular Devices) was used for control of the pulse protocol, as well as for data acquisition and analysis. Series resistance was <5 MΩ and was compensated (by 70–80%) to minimize voltage errors. In the experiments, voltage ramps from −80 to +20 mV and of 1 s duration were applied every 10 s; holding voltage was −30 mV.
The bath solution (pH 7.5) contained (in mM): NaCl, 94; Na-gluconate, 6; MgCl2, 1; CaCl2, 2; TEA-Cl, 2; HEPES, 10; d-glucose, 10. Osmolality was adjusted to 310 (isotonic) and 400 mosmol/kg-H2O (hypertonic) by the addition of mannitol.
The pipette solution (pH 7.3, 300 mosmol/kg-H2O) contained (in mmol/l): NaCl, 26; Na-gluconate, 69; MgCl2, 1; TEA-Cl, 2; Na2-ATP, 2; Na2-GTP, 0.5; HEPES, 10; EGTA, 1. With these ion gradients, the equilibrium potentials for Na+ and Cl− (as the only permeant ions) are set at 0 and −30 mV, respectively [13]. Experiments were performed at room temperature.
Monitoring apoptotic cell death
Cell viability and caspase-3/7 activity were determined by use of a calorimetric MTT assay (Cell Counting Kit-8; Dojindo, Kumamoto, Japan) and a fluorometric probe (Apo-ONE Homogeneous Caspase-3/7 Assay; Promega, Madison, WI), respectively.
Fragmentation of DNA was determined by means of a photometric enzyme immunoassay (Cell Death Detection ELISAPLUS, Roche Applied Science, Diagnostics, Mannheim, Germany) with HeLa cells plated on 96-well plates. Following exposure to the various experimental conditions, cells were lysed and centrifuged at 200g. The cytoplasmic (DNA containing) fraction was then transferred to streptavidin-coated microtiter plates that had been incubated with a biotinylated monoclonal anti-histone antibody. Finally, the amount of the fragmented DNA on bound nucleosomes was determined with a peroxidase-conjugated monoclonal anti-DNA antibody and the substrate ABTS [2,2′-azino-di-(3-ethylbenzthiazoline sulfonate)], which was quantified photometrically at 405 nm. In all measurements, cells were incubated for 6 h at 37°C.
Testing for necrosis and late apoptosis
Necrosis and late apoptosis of cells were quantified fluorometrically on the basis of a propidium iodide staining of nuclei (excitation/emission at 530 nm/620 nm) performed with reference to an overall staining of cells by Hoechst 33342 (excitation/emission at 350 nm/460 nm).
Chemicals
All reagents were purchased from Sigma–Aldrich (Tokyo, Japan).
Statistical analysis
Data are presented as mean values ± SEM with n denoting the number of observations. Student’s t tests for paired and unpaired data were used as appropriate and P < 0.05 was considered significant.
Results and discussion
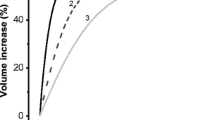
As was determined by means of electronic cell sizing, increasing osmolality from 300 mosmol/kg-H2O to 330, 400, 500 and 600 mosmol/kg-H2O led to an initial shrinkage of HeLa cells to 96.6 ± 0.4, 82.6 ± 1.9, 72.5 ± 0.2 and 66.2 ± 0.6% of the control level, respectively (n = 10; Fig. 1a). When plotted as a function of 1/osmolality (which is equivalent to a ‘Boyle-van’t Hoff graph’ [3, 14]), these data could readily be fitted by a straight line; its intercept with the y-axis yields the osmotically active versus inactive space of the cells, with the latter amounting to 30.6% of total cell volume (Fig. 1a, Insert). This osmometric behaviour of HeLa cells was then followed by an active volume recovery to 101.7 ± 0.4, 92.6 ± 0.5, 89.7 ± 0.8 and 88.4 ± 0.9%, in 120 min of hypertonic stress (Fig. 1a, b). The process of “regulatory volume increase (RVI)” occurred at essentially constant rates that equalled 0.4 ± 0.2, 0.9 ± 0.2, 1.6 ± 0.2 and 1.8 ± 0.2%/10 min, respectively, in the range of 5–120 min after application of hypertonicity.

Hypertonicity-induced HeLa cell shrinkage and RVI determined by electronic cell sizing. (a) The volume response of cells to increases in osmolality (from 300 mosmol/kg-H2O) to 330, 400, 500 and 600 mosmol/kg-H2O at time zero (arrow) are depicted. The insert gives the initial (passive) amount of cell shrinkage as a function of 1/osmolality (equivalent to a ‘Boyle-van’t Hoff plot’ of these data; see text for details). 3.33 kg-H2O/osmol = 1/(0.300 osmol/kg-H2O) is the 100% value under isotonic conditions. (b) The volume of HeLa cells at 120 min of various levels of hypertonic stress, after partial volume recovery (RVI) had been achieved. n = 10 for each experimental condition
It has become increasingly evident in recent years that persistent cell shrinkage is one of the hallmarks of apoptosis [6, 15]. Also, it has recently been found that after 2-h stimulation with staurosporine (STS), TNFα or Fas ligand, HeLa cells lose their ability to undergo RVI (12). To test whether HeLa cell shrinkage and/or RVI interferes with apoptotic volume decrease (AVD), 4 μM STS was used to induce apoptosis in HeLa cells [6], and a series of volume measurements was made. This was done under isotonic conditions (300 mosmol/kg-H2O) and under hypertonic conditions in which osmolality was increased to 330, 400, 500 and 600 mosmol/kg-H2O (n = 10). Within an experimental time frame of 120 min, STS was found to reduce cell volume to 65.8 ± 1.6% that of the control, under isotonic conditions (Fig. 2a: diamonds). 5 min after osmolality was increased to 330, 400, 500 and 600 mosmol/kg-H2O, cell volume equalled 89.6 ± 0.7, 81.4 ± 0.2, 71.4 ± 0.9 and 64.5 ± 0.8% of control, respectively. These values are virtually identical to the values of purely passive or physical responses to hypertonic stimulation in the absence of STS (cf. to Fig. 1a). Moreover, an osmotically inactive space of 35.4% could be calculated from these measurements; this value is very similar to that obtained in the control experiments (see above). Of note, no RVI followed hypertonicity-induced cell shrinkage when STS was present. This indicates that the RVI response was completely inhibited by STS (or surpassed by the STS-induced AVD process), a phenomenon which clearly holds for the full 2 h period after STS application. Using the respective values for volume at 5 min as passive reference values, AVD was computed to be 30.8 ± 0.7, 22.2 ± 0.7, 12.1 ± 0.5 and 7.2 ± 0.7% for 330, 400, 500 and 600 mosmol/kg-H2O, respectively (calculated as the volume at 5 min minus the volume at 120 min). So as summarized in Fig. 2b, a decrease of AVD was observed with increasing hypertonic stress. On the one hand, then, hypertonic stress appears to suppress STS-induced AVD; on the other hand, STS seems to abolish hypertonicity-induced RVI. Also of note, in this respect, is a recent study on HeLa cells in which tyrosine kinases, PKC, and p38 MAPK were identified as part of the signalling machinery employed in the activation of HICC and RVI [16]. Given the non-specificity of STS with respect to its inhibition of various protein kinases, it is not surprising that RVI is inhibited in the presence of the compound, while AVD is induced.

Effects of hypertonic stress on apoptotic volume decrease (AVD). (a) At time zero (arrow), 4 μM staurosporine (STS) was added to induce apoptotic shrinkage of HeLa cells under isotonic conditions (◆) or together with an increase of osmolality to 330 (■), 400 (▲), 500 (●) and 600 (▼) mosmol/kg-H2O. Hypertonic cell shrinkage, at 5 min, was very similar in the presence and absence (see Fig. 1) of STS. (b) AVD under isotonic conditions (volume at 0 min minus volume at 120 min) and hypertonic conditions (volume at 5 min minus volume at 120 min). n = 10 for each experimental condition
To study the interference of STS-induced AVD with hypertonicity-induced RVI in more detail, experiments were performed in which osmolality was increased from 300 to 500 mosmol/kg-H2O, at time zero (see Fig. 3a: arrow). In addition, 4 μM STS was applied either 2 h before (t = −120 min), 1 h before (t = −60 min), at the same time as (t = 0) or 1 h after (t = 60 min) hypertonic stimulation (see Fig. 3a: arrowheads). AVD was then computed from the overall changes in cell volume (i.e. the volume at 0, −60 or −120 min, respectively, minus the volume at 120 min) minus the amount of passive cell shrinkage (i.e. the volume at 0 min minus the volume at 5 min). Hypertonic stress (500 mosmol/kg-H2O) significantly reduced AVD from the control value of 34.2 ± 0.5% (Fig. 2b: 300; also marked as STS-ISO, in Fig. 3b) to 12.1 ± 0.5 or 12.5 ± 0.5% (Fig. 3b: STS-HYPER or HYPER/1hSTS) when given simultaneously with, or 1 h before, application of STS (n = 10, P < 0.001 each), respectively. Also apparent from these experiments is that no RVI occurred in the presence of STS. It is noteworthy that increasing the osmolality to 500 mosmol/kg-H2O after 1-h pretreatment with STS still led to a markedly reduced AVD of 25.9 ± 0.7% (P < 0.001; Fig. 3b: STS1h/HYPER). A hypertonic stimulation after 2-h pretreatment with STS, however, was not effective at suppressing AVD (Fig. 3b: STS2h/HYPER). These results suggest that hypertonic stimulation of HeLa cells is somehow interfering with the process of AVD when applied in the time range of 1 h before to 1 h after the application of STS.

Interference of AVD with RVI. (a) Osmolality was increased from 300 to 500 mosmol/kg-H2O at time zero (arrow), with 4 μM STS applied (at arrowheads) either 2 h before (STS2h/HYPER: ■), 1 h before (STS1h/HYPER: ●), at the same time as (STS-HYPER:▼) or 1 h after (HYPER/1hSTS: ▲) the start of hypertonic stress. (b) Total AVD computed from the overall volume changes shown in (a) minus the initial amount of passive cell shrinkage in the first 5 min of hypertonic stress (i.e. volume at 0 min minus volume at 5 min). STS-ISO refers to the AVD observed under isotonic conditions. n = 10 for each experimental series
Next, the effects of STS on activation of the HICC were tested. This was done by increasing osmolality at various times relative to STS application. As shown in Fig. 4 (STS-HYPER), STS had no significant short-term effect on activation of the HICC when given together with hypertonic stress, i.e. the peak activation of HICC current was virtually unaffected for 5–7 min by STS applied simultaneously with hypertonic stress. This finding fits with the observation that HICC activation appears to occur on a considerably faster time scale than the initiation of AVD does. In this respect, it is also of note that even with STS applied 1 h ahead of hypertonicity (STS1h/HYPER), the HICC was still activated to a level approximately half of the control value, i.e. to 1.59 ± 0.39 pA/pF. With STS given 2 h before hypertonic stress (STS2h/HYPER), HICC currents were almost completely inhibited (0.62 ± 0.20 pA/pF, n = 5–33).

Effects of STS on HICC activation. (a) HICC currents in the absence (Control) or presence of STS, which was applied simultaneously with hypertonic stress (STS-HYPER), 1 h ahead of hypertonic stress (STS1h/HYPER) or 2 h ahead of hypertonic stress (STS2h/HYPER). Representative traces of 5 to 33 experiments. (b) Typical I/V-relationships under these conditions. (c) Summary of HICC current densities obtained under the four different conditions shown in (a)
Whenever studied in a quantitative way, HICCs have been proven to be the main mechanism of the RVI of a given system [3–5]. This also holds for HeLa cells, in which the relative contribution of HICC activity and Na+/H+ antiport to RVI is approximately 2:1 (with no detectable contribution of Na+-K+-2Cl− symport at all) [5, 13]. This raises the question of whether the apparent interference of hypertonic stress with AVD may occur via activation of the HICC. In the experiments shown in Fig. 5a, osmolality was increased from 300 to 500 mosmol/kg-H2O, at time zero (arrow). Following 60 min of hypertonic stress, 300 μM flufenamic acid (FFA, an established blocker of the HICC in HeLa cells [4, 5, 13]), STS (4 μM) or FFA plus STS were then applied (arrowhead). As expected, FFA significantly blunted the progress of RVI, presumably by inhibition of the HICC. The volume change from 60 to 120 min (volume at 120 min minus volume at 60 min) was −2.0 ± 0.6% in the presence of FFA; in the control experiments, on the other hand, the 60-to-120 min volume change due to RVI equalled 10.2 ± 0.9% (n = 10, P < 0.001; Fig. 5b: Control). Of note, STS led to a pronounced decrease in cell volume of −12.5 ± 1.6% (Fig. 5b: STS), and the effects of FFA plus STS were additive, resulting in a decrease in cell volume of −19.0 ± 1.0% (P < 0.01; Fig. 5b: STS+FFA). Experiments with 1 mM 2-aminoethoxydiphenyl borate (2-APB) as an alternative blocker of the HICC [17] yielded virtually identical results. With 2-APB, the 60-to-120 min volume change equalled 2.9 ± 1.1% (Fig. 5b: 2-APB), and again, the effects of HICC blockage and STS (volume change of −16.3 ± 0.6%; P < 0.05) were additive (Fig. 5b: STS+2-APB).

Effects of HICC channel blockers and STS on RVI and AVD. (a) Osmolality was increased from 300 to 500 mosmol/kg-H2O at time zero (arrow) for all groups. 300 μM flufenamic acid (FFA), STS or FFA plus STS were applied at t = 60 min of hypertonic stress (arrowhead) as indicated. (b) Summary of the volume changes from 60 to 120 min (volume at 120 min minus volume at 60 min) observed in the experiments shown in (a) and two additional experiments in which 1 mM 2-aminoethoxydiphenyl borate (2-APB) was used as a blocker of HICC channels, alone or in combination with STS. n = 10 for each experimental condition. *** Significantly different from Control with P < 0.001; #,## significantly different from STS with P < 0.05 and P < 0.01, respectively
It may be argued that, due to the limited specificity of FFA and 2-APB, the effects of both compounds described above may be due to an inhibition of volume-sensitive outwardly rectifying (VSOR) Cl− channels (see [2, 18] for review), rather than blockage of the HICC. In an additional series of measurements, however, it was found that even with application of 10 μM DCPIB (4-(2-butyl-6,7-dichlor-2-cyclopentyl-indan-1-on-5-yl) oxybutyric acid), an effective blocker of the VSOR Cl− channel [19], an RVI value of 10.6 ± 0.6% (when added at t = 60 min; n = 10) was obtained; this is virtually identical to the value of 10.2 ± 0.9% observed under control conditions (see above). Furthermore, 10 μM DCPIB inhibited VSOR currents in HeLa cells by 67.6 ± 3.6% (n = 6) whereas it did not exhibit an effect on HICC currents at all (n = 8; Wehner and Numata, unpublished results).
These data strongly imply that, even in early-stage apoptosis, HICC activation is an effective mechanism of RVI in HeLa cells. Furthermore, they provide additional strong evidence for the functional interplay of AVD and RVI. In this regard, the apparent lack of RVI in HeLa cells undergoing AVD (Fig. 2a) could be accounted for as follows: In early-stage apoptosis (say, within 1 h after STS application) the AVD process surpasses the RVI process, which involves HICC activity, whereas in the later stage of apoptosis, the RVI process is suppressed because of inhibition of the HICC by STS.
Finally, we characterized the interplay between HICC activation and STS-induced cell death and apoptosis. As determined by an MTT assay (Fig. 6a), a caspase-3/7 activity assay (Fig. 6b), and an apoptosis assay measuring nucleosome-bound DNA (Fig. 6c), increasing osmolality from 300 mosmol/kg-H2O to 400, 500, and 600 mosmol/kg-H2O led to significant and parallel reductions of both cell death and apoptosis observed 6 h after STS application; the maximal effect was observed at 500 mosmol/kg-H2O and above. This is a surprising finding because, based on what has been reported so far concerning the interplay of cell volume and apoptosis, one might expect a synergistic effect of cell shrinkage on the induction of programmed cell death [15]. Furthermore, FFA and 2-APB almost completely blocked these effects, the fact providing strong further evidence that it is the activation of the HICC that is actually rescuing HeLa cells from apoptosis.

Rescue from STS-induced apoptosis by hypertonic stimulation and inhibition of rescue by HICC blockers. (a) Cell death observed 6 h after STS treatment at various osmolalities, and at 500 mosmol/kg-H2O with 300 μM FFA or 1 mM 2-APB as indicated (n = 12–34). (b) Apoptosis monitored as caspase-3/7 activity induced by 6-h exposure to STS at various osmolalities, and when FFA or 2-APB was also applied, at 500 mosmol/kg-H2O (n = 12–26). (c) DNA fragmentation analyzed with a nucleosomal ELISA assay after a 6-h exposure to STS at various osmolalities, and when FFA or 2-APB was also applied, at 500 mosmol/kg-H2O (n = 6)
To insure that the above measurements were not corrupted by the necrosis of cells, propidium iodide staining was performed. Propidium iodide is known to selectively bind to cell nuclei, and because it does not permeate intact cell membranes, it provides a reliable measure for the necrosis and late apoptosis of cells. Following a 6-h incubation, the percentages of necrotic cells were 0.1 ± 0.1% (for 300 mosmol/kg-H2O), 1.8 ± 0.3% (for 300 mosmol/kg-H2O—STS), 0.8 ± 0.1% (for 400 mosmol/kg-H2O—STS), 0.6 ± 0.1% (for 500 mosmol/kg-H2O—STS), and 0.5 ± 0.1% (for 600 mosmol/kg-H2O—STS; n = 8–10, for each condition). It is concluded from these experiments that STS, at 4 μM, is an effective and reliable tool for the induction of apoptosis in HeLa cells, as reported also in an earlier study from this laboratory [6].
It may be argued that hypertonic stress (and HICC activation) just delays, rather than prevents, STS-induced cell death in HeLa cells. As propidium iodide staining after 24 h of STS exposure revealed, however, the necrosis or late apoptosis of cells was 94.7 ± 0.7% for 300 mosmol/kg-H2O, and 76.1 ± 2.8% for 500 mosmol/kg-H2O. Clearly, even under these harsh experimental conditions (i.e. stimulation with STS for 1 day), hypertonicity rescued HeLa cells from death to a significant degree (P < 0.001; n = 8).
In the last series of measurements, the timing of apoptosis induction by STS versus hypertonic stress was analysed. As depicted in Fig. 7, increasing osmolality from 300 to 500 mosmol/kg-H2O rescued HeLa cells from apoptosis induced by 6-h application of STS if this maneuver was performed 2 h before (HYPER2h/STS), 1 h before (HYPER1h/STS) or at the same time as the application of STS (STS-HYPER). Moreover, even with STS given 1 h ahead of hypertonic stress, apoptotic cell death was reduced to some 50% of the isotonic control value (Fig. 7). Of note, the overall profiles of the effects of the timing of STS application versus hypertonic stress on cell death and apoptosis, as shown in the figure, are undistinguishable from those observed on AVD (see Fig. 3) as well as on HICC activation (Fig. 4).

Interference of HICC activation with STS-induced apoptosis. For the control, STS was applied for 6 h under isotonic conditions (STS-ISO). For the other groups, it was applied 2 h before (STS2h/HYPER), 1 h before (STS 1h/HYPER), at the same time as (STS-HYPER), 1 h after (HYPER1h/STS) or 2 h after (HYPER2h/STS) osmolality was increased from 300 to 500 mosmol/kg-H2O. Apoptosis was monitored as a decrease of cell viability (a, n = 12 to 42), caspase-3/7 activity expressed as relative fluorescence units (FU; b, n = 6 and 12), and DNA fragmentation measured in an enzyme-linked (ELISA) assay as absorbance values (OD, optical density; c, n = 6)
It has long been known that AVD occurs in parallel with a loss of cellular K+ and a gain of cellular Na+ [20–22]. To some extent, these effects might reflect reduced activity of the Na+/K+-ATPase [23]. Nevertheless, if the activation of the HICC were triggered as a consequence of conductive K+ export and AVD, this would lead to very similar results. Also of interest in this respect is a recent study on human leukemia U937 cells reporting two distinct phases during STS-induced apoptosis: an initial phase in which cellular K+ and Cl− decreased in parallel, followed by a second phase in which there was a further decrease in cellular K+ and an enormous increase in cellular Na+ (accompanied by a rise in cellular Cl−) [24]. Of note, U937 cells were shown to express HICC currents [25]. Thus, the ionic scenario described could also reflect the interplay of HICC activation and AVD, as proposed in the present study.
In rat hepatocytes, 405 mosmol/kg-H2O was insufficient to induce apoptosis but it sensitized cells to CD95-triggered cell death, whereas 505 mosmol/kg-H2O functioned as an effective apoptosis inducer per se [26–29]. Since rat hepatocytes express (amiloride-sensitive) HICC currents [4, 30–32], it would be interesting to examine the degree to which blockage of the HICC might interfere with the induction of cell death in this system.
Conclusions
Taken together, our results indicate that hypertonic stress caused a significant reduction in the staurosporine (STS)-induced apoptosis of HeLa cells. When analysing the functional interplay between apoptotic volume decrease (AVD) and regulatory volume increase (RVI) through the use of different activation protocols and effective blockers, the activation of hypertonicity-induced cation channels (HICCs) could be identified as the molecular mechanism by which HeLa cells are actually rescued from STS-induced apoptosis in hypertonic conditions. The precise mechanism by which HICC activation inhibits AVD and apoptosis remains to be elucidated.
Nevertheless, the results reported herein demonstrate a novel role of the HICC in the induction of programmed cell death. They are also in perfect agreement with a recent study in which inhibition of the HICC was found to sensitize HeLa cells to shrinkage-induced apoptosis [33]. We have only begun to understand the role of the HICC in these processes [4, 5], and the general relevance of the channel in cell proliferation and apoptosis remains a question of considerable interest.
References
Bortner CD, Cidlowski JA (2004) The role of apoptotic volume decrease and ionic homeostasis in the activation and repression of apoptosis. Pflugers Arch 448:313–318
Okada Y, Maeno E, Shimizu T, Manabe K, Mori S, Nabekura T (2004) Dual roles of plasmalemmal chloride channels in induction of cell death. Pflugers Arch 448:287–295
Wehner F, Olsen H, Tinel H, Kinne-Saffran E, Kinne RKH (2003) Cell volume regulation: osmolytes, osmolyte transport, and signal transduction. Rev Physiol Biochem Pharmacol 148:1–80
Wehner F (2006) Cell volume-regulated cation channels. Contrib Nephrol 152:25–53
Wehner F, Bondarava M, ter Veld F, Endl E, Nürnberger HR, Li T (2006) Hypertonicity-induced cation channels. Acta Physiol 187:21–25
Maeno E, Ishizaki Y, Kanaseki T, Hazama A, Okada Y (2000) Normotonic cell shrinkage because of disordered volume regulation is an early prerequisite to apoptosis. Proc Natl Acad Sci USA 97:9487–9492
Wang Z (2004) Roles of K+ channels in regulating tumour cell proliferation and apoptosis. Pflugers Arch 448:274–286
Burg ED, Remillard CV, Yuan JXJ (2006) K+ stop channels in apoptosis. J Membr Biol 209:3–20
Porcelli AM, Ghelli A, Zanna C, Valente P, Ferroni S, Rugolo M (2003) Staurosporine induces apoptotic volume decrease (AVD) in ECV304 cells. Ann NY Acad Sci 1010:342–346
Lang F, Foller M, Lang KS, Lang PA, Ritter M, Gulbins E, Vereninov A, Huber SM (2005) Ion channels in cell proliferation and apoptotic cell death. J Membr Biol 205:147–157
Krumschnabel G, Maehr T, Nawaz M, Schwarzbaum PJ, Manzl C (2007) Staurosporine-induced cell death in salmonid cells: the role of apoptotic volume decrease, ion fluxes and MAP kinase signaling. Apoptosis 12:1755–1768
Heimlich G, Cidlowski JA (2006) Selective role of intracellular chloride in the regulation of the intrinsic but not extrinsic pathway of apoptosis in Jurkat T-cells. J Biol Chem 281:2232–2241
Wehner F, Shimizu T, Sabirov R, Okada Y (2003) Hypertonic activation of a non-selective cation conductance in HeLa cells and its contribution to cell volume regulation. FEBS Lett 551:20–24
Lucké B, McCutcheon M (1932) The living cell as an osmotic system and its permeability to water. Physiol Rev 12:68–139
Okada Y, Maeno E, Shimizu T, Dezaki K, Wang J, Morishima S (2001) Receptor-mediated control of regulatory volume decrease (RVD) and apoptotic volume decrease (AVD). J Physiol (Lond) 532:3–16
Wehner F, Numata T, Subramanyan M, Takahashi N, Okada Y (2007) Signalling events employed in the hypertonic activation of cation channels in HeLa cells. Cell Physiol Biochem 20:75–82
Numata T, Wehner F, Okada Y (2007) 2-aminoethoxydiphenyl borate is an effective blocker of hypertonicity-induced cation channels in HeLa cells. J Physiol Sci 57:235–238
Okada Y (2006) Cell volume-sensitive chloride channels: phenotypic properties and molecular identity. Contrib Nephrol 152:9–24
Decher N, Lang HJ, Nilius B, Bruggemann A, Busch AE, Steinmeyer K (2001) DCPIB is a novel selective blocker of I(Cl,swell) and prevents swelling-induced shortening of guinea-pig atrial action potential duration. Br J Pharmacol 134:1467–1479
Bortner CD, Sifre MI, Cidlowski JA (2008) Cationic gradient reversal and cytoskeleton-independent volume regulatory pathways define an early stage of apoptosis. J Biol Chem 283:7219–7229
Bortner CD, Cidlowski JA (2007) Cell shrinkage and monovalent cation fluxes: role in apoptosis. Arch Biochem Biophys 462:176–188
Bortner CD, Gomez-Angelats M, Cidlowski JA (2001) Plasma membrane depolarization without repolarization is an early molecular event in anti-Fas-induced apoptosis. J Biol Chem 276:4304–4314
Panayiotidis MI, Bortner CD, Cidlowski JA (2006) On the mechanism of ionic regulation of apoptosis: would the Na+/K+-ATPase please stand up? Acta Physiol (Oxf) 187:205–215
Arrebola F, Canizares J, Cubero MA, Crespo PV, Warley A, Fernandez-Segura E (2005) Biphasic behavior of changes in elemental composition during staurosporine-induced apoptosis. Apoptosis 10:1317–1331
Gamper N, Huber SM, Badawi K, Lang F (2000) Cell volume-sensitive sodium channels upregulated by glucocorticoids in U937 macrophages. Pflugers Arch 441:281–286
Reinehr R, Graf D, Fischer R, Schliess F, Häussinger D (2002) Hyperosmolarity triggers CD95 membrane trafficking and sensitizes rat hepatocytes toward CD95-induced apoptosis. Hepatology 36:602–614
Reinehr R, Schliess F, Häussinger D (2003) Hyperosmolarity and CD95L trigger CD95/EGFR association and tyrosine phosphorylation of CD95 as prerequisites for CD95 membrane trafficking and DISC formation. FASEB J 17:731–733
Reinehr R, Häussinger D (2007) Hyperosmotic activation of the CD95 system. Methods Enzymol. 428:145–160
Reinehr R, Becker S, Hongen A, Häussinger D (2004) The Src family kinase Yes triggers hyperosmotic activation of the epidermal growth factor receptor and CD95. J Biol Chem 279:23977–23987
Wehner F, Tinel H (2000) Osmolyte and Na+ transport balances of rat hepatocytes as a function of hypertonic stress. Pflugers Arch 441:12–24
Wehner F, Tinel H (1998) Role of Na+ conductance, Na+-H+ exchange, and Na+- K+-2Cl- symport in the regulatory volume increase of rat hepatocytes. J Physiol (Lond) 506:127–142
Wehner F, Sauer H, Kinne RKH (1995) Hypertonic stress increases the Na+ conductance of rat hepatocytes in primary culture. J Gen Physiol 105:507–535
Shimizu T, Wehner F, Okada Y (2006) Inhibition of hypertonicity-induced cation channels sensitizes HeLa cells to shrinkage-induced apoptosis. Cell Physiol Biochem 18:295–302
Acknowledgments
This work was supported by Grants-in-Aid for Scientific Research from the Ministry of Education, Culture, Sports, Science and Technology of Japan (MEXT), from the Japan Society for the Promotion of Science (JSPS), by the Foundation for Promotion of Material Science and Technology of Japan (MST Foundation) and by the Deutsche Forschungsgemeinschaft. The authors thank E.L. Lee for manuscript preparation.
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License (https://creativecommons.org/licenses/by-nc/2.0), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
About this article
Cite this article
Numata, T., Sato, K., Okada, Y. et al. Hypertonicity-induced cation channels rescue cells from staurosporine-elicited apoptosis. Apoptosis 13, 895–903 (2008). https://doi.org/10.1007/s10495-008-0220-y
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10495-008-0220-y