
Abstract
The widespread accessibility of smart devices, even if not designated as medical devices, coupled with the critical need for ongoing monitoring of patients taking anti-seizure medication or undergoing new stimulation therapies highlights the urgent need for collaborative research across disciplines. These therapies, while beneficial, may cause sporadic or temporally dynamic side effects affecting cognition and behavior that cannot be adequately assessed by traditional neuropsychological testing methods at certain time points. This scenario highlights the importance of developing innovative approaches to fully monitor and understand these dynamic effects.
Zusammenfassung
Die weit verbreitete Verfügbarkeit intelligenter Geräte, selbst wenn sie nicht als medizinische Geräte eingestuft werden, in Verbindung mit der entscheidenden Notwendigkeit einer fortlaufenden Überwachung von Patienten, die anfallssuppressive Medikamente einnehmen oder bei denen neuartige Stimulationstherapien durchgeführt werden, unterstreicht den dringlichen Bedarf an gemeinsamer Forschung über die Fachgebiete hinweg. Obwohl diese Therapien nutzbringend sind, können sie sporadisch und vorübergehend dynamische Nebenwirkungen hervorrufen, welche die Kognition und das Verhalten betreffen und die nicht mithilfe herkömmlicher neuropsychologischer Testmethoden zu festen Zeitpunkten untersucht werden können. Dieses Szenario macht die Bedeutung der Entwicklung innovativer Ansätze deutlich, um diese dynamischen Auswirkungen vollständig zu erfassen und zu verstehen.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Background
Patients with epilepsy, regardless of epilepsy type, etiology, and localization, often suffer from cognitive and sensorimotor impairments. These impairments affect a wide range of functions and are usually not specific to epilepsy [1]. They often impact psychomotor speed, memory, attention, and executive function in both verbal and nonverbal modalities. The severity of these cognitive impairments may vary over time depending on the current seizure burden, the frequency of interictal epileptic activity, and the dosage and number of anti-seizure medications (ASM). In addition, psychiatric comorbidities may affect mood and drive/motivation and secondarily modulate test performance to a relevant extent [1]. Similarly, alterations in circadian rhythms and sleep disturbances are commonly observed in patients with epilepsy, further impinging on cognitive and sensorimotor performance at multiple time scales [2].
Therefore, a comprehensive neuropsychological assessment of the neurocognitive and sensorimotor status of a patient with epilepsy at one point in time will always represent both current transient, dynamic impairments and chronic states of impairment in a combined fashion, without being able to differentiate between these two components. Disentangling this interaction over time would require multiple, comprehensive follow-up studies under well-controlled conditions.
Neuropsychological testing
The purpose of most neuropsychological tests is to psychometrically assess the level of neurocognitive functions relative to population norms. Intraindividually, intact functions can ideally be dissociated from impaired functions. This means that clinical neuropsychology, which is still characterized by the test methodology of the first half of the 20th century, fulfils many of the normative diagnostic requirements of neurology and psychiatry and its taxonomies of disorders. This also applies to questions about the neurocognitive status of an epilepsy patient or specific impairments of episodic memory residing in the temporal lobes or prefrontal executive functioning.
However, most epilepsies, more than other neurological diseases, show high temporal dynamics of seizure-related changes in cognitive and affective functioning [3]. Mapping these dynamics in their effects on cognitive, affective, and sensorimotor functions would be a major step forward for individualized optimization of therapies for several reasons [3]. Temporally discrete long-term point measurements have the fundamental problem that the actual difference between test scores at different measurement times can be masked by short-term interference from daily form, mood, circadian modulations, etc. This is particularly true in the case of epilepsy.
Although highly significant changes in performance can be detected by long-term point interval follow-up measurements using neuropsychological tests, changes of less than one standard deviation are rarely identified as statistically significant by reliable indices of change but may still be significant for the patient in terms of coping with everyday life.
Systematic follow-up is comparatively rare in epileptology, with the exception of epilepsy surgery.
Repeated assessments are rarely performed when ASM is changed. Patients often experience anosognosia regarding the cognitive effects of ASM or may be imprecise in their subjective reports. Furthermore, depending on the chosen drug, ASM blood levels and thus their potential to cause cognitive side effects may undergo relevant diurnal fluctuations. These fluctuations may mask the true effect on cognition and would require repeated testing of cognition in short intervals. The reluctance to perform repeated cognitive testing can be attributed to several factors: the significant cost and often scarce availability of neuropsychological testing resources, as well as the inherent limitations of neuropsychological instruments, which are usually not suitable for repeated measures due to the lack of parallel forms and their unique standardizations.
Brain stimulation techniques
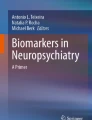
Today, innovative invasive and noninvasive brain stimulation techniques are emerging, and their availability is expected to increase in the coming years, particularly for the treatment of patients who are resistant to drug therapies. Importantly, recent developments in vagus nerve stimulation (VNS) and deep brain stimulation (DBS) for epilepsy aim to adapt stimulation protocols to minimize side effects. For example, in the latest generation of devices, reduced VNS amplitudes can be preprogrammed with circadian adaptations, for instance, to prevent stimulation-dependent side effects in sleep. Furthermore, brain stimulation methods carry the risk of intermittent, reversible cognitive impairment, depending on the multiple stimulation parameters and locations that may be changed over different time scales. It is therefore important to assess both the immediate and delayed adverse effects of these techniques using standard neuropsychological tests at different time points as illustrated in Fig. 1.

Cognitive performance in a particular domain (e.g., memory) fluctuates over time and is influenced by the interaction of seizure burden, pharmacotherapy, or neuromodulation. Point measurements over long periods of time (T1–T3) do not reveal the true fluctuating time course. For example, a seizure cluster at time point T2 will result in poor performance compared to baseline (T1), whereas a seizure-free interval will significantly improve cognition (T3)
Of note, current research in DBS of the anterior nucleus of the thalamus (ANT-DBS) and the development of stimulation hardware with the capability to sense deep brain signals and stimulate deep brain targets “on demand” lead the way toward biomarker-guided closed-loop adaptive DBS. This type of adaptive DBS is therefore expected to produce immediate and unpredictable changes in brain electrical activity during the day. These changes may also affect an individual’s typical cognitive processing. In addition, reactive neuroplastic changes may occur over hours or weeks. All these temporal changes may interact with seizures of varying frequency, duration, and severity as well as with pharmacotherapy, for example, through synergistic effects that reduce compensatory cognitive reserve capacity (illustrated in Fig. 1). At present, epileptologists using DBS can only rely on patient feedback or neuropsychological screening tests with limited sensitivity for mild to moderate changes.
This problem of inaccurate cognitive monitoring over time is well illustrated for memory dysfunction associated with ANT-DBS treatment. In the most comprehensive prospective study, an acute adverse effect on memory was observed in approximately 15% of patients after the onset of stimulation [4], and similar findings were reported in a 2-year real-world European follow-up study [5]. However, long-term follow-up of the original SANTE cohort showed that almost twice as many patients (27%) reported memory problems at some point after DBS implantation [6]. Importantly, these subjective memory problems were not confirmed by repeated neuropsychological testing, while some patients even showed higher scores in measures of executive function and attention. [6, 7]. The latter observation might have been biased by the open-label study design over 7 years with a high drop-out rate (59 patients remaining out of 110 in the ITT cohort) potentially biasing the results toward more favorable outcome. Nevertheless, it ultimately remains unclear whether memory problems tend to increase or decrease with chronic ANT-DBS, or whether they simply show a fluctuating time course and are not properly represented by infrequent point assessments over time.
Patient monitoring via digital biomarkers and cognitive proxies
What are the current options for monitoring the rapid cognitive and affective changes in epilepsy patients so as to assess the influence of time-dynamic factors, for example, DBS, seizures, pharmacological polytherapy, and its titration? The monitoring and treatment of epilepsy patients can be significantly improved by using digital biomarkers and cognitive proxies that are automatically recorded by smart devices such as smart watches, smart phones, and smart rings. These technologies enable continuous and discrete monitoring and provide important insights into patients’ motor and cognitive functioning.
Here, we list some examples of candidate digital biomarkers and proxies, some of which are already being used in smart devices. It is important to distinguish digital cognitive proxies from biomarkers. Biomarkers focus on measuring physical parameters associated with biological activity, such as movement or heart rate. By contrast, digital cognitive proxies infer mental capacity from the speed, results, and errors in cognitive tasks such as navigation, memory (codes, names, shortcuts), reading speed, and writing errors. A further distinction must be made between active and passive biomarkers and proxies. Active biomarkers and proxies act as tasks to be completed by the individual and have similarities to psychological performance tests. On the other hand, passive biomarkers, which are often more readily accepted by patients, collect information about the user’s cognitive and sensorimotor status through signals and parameters continuously derived from regular user behavior.
-
A.
Passive measurement strategies
-
1.
Seizure detection: Modern smartwatches and smartphones are equipped with accelerometers and gyroscopes that can detect motor seizures by identifying unusual or repetitive movement patterns. These devices also have the ability to record atypical vocalizations and heart rate patterns, providing a comprehensive approach to seizure monitoring.
-
2.
Heart rate variability, blood pressure, pulse oximetry: Smartwatches and, more recently, smart rings are capable of monitoring various cardiovascular biomarkers, providing valuable data on sudden changes that may signal the onset of certain seizure types, particularly autonomic seizures.
-
3.
Sleep pattern analysis: Given the prevalence of sleep disorders in individuals with epilepsy, smart devices play a critical role in monitoring sleep patterns. This technology can detect sleep irregularities that may indicate an increased risk of seizures or the occurrence of seizures during sleep.
-
4.
Macroscopic movement patterns: Analysis of topographic movement patterns, including changes in movement speed, unusual asymmetry, variations in the duration of bipedal support, and deviations from routine activities, can reveal potential epileptic events and the effects of treatment interventions such as DBS.
-
5.
Microscopic movement patterns: Examining subtle changes in tapping and swiping movements on smartphones can reveal cerebral dysfunction and tremors. These microscopic patterns of movement during smartphone interaction correlate with epileptiform activity as registered on EEG. They may also indicate side effects of ASM adjustments [8].
-
6.
Alterations in oral communication: This encompasses a range of speech and language disturbances, including variations in prosody, the presence of dysarthria, difficulties with word retrieval, changes in sentence construction, and changes in overall length and frequency of speech, providing parametric descriptions of symptom severity. Such symptoms may be associated with expressive language impairments involving both frontal and temporal lobes.
-
7.
Alterations in written communication: This includes a range of changes that affect the ability to communicate in written form, such as challenges with word retrieval, adherence to grammatical norms, sentence structure, and consistency in the length and frequency of written language. Other indicators include variations in reading and writing speed, increased incidence of spelling errors and overall fluency. Although fluctuations in attention play a role, these changes are especially symptomatic of expressive language disturbances affecting frontal and temporal regions.
-
8.
Smartphone camera detection of oculomotor abnormalities: Use of the smartphone camera to observe oculomotor irregularities during standardized interactions. Such abnormalities, including deviations in saccades, smooth pursuit movements, fixation stability, convergence ability, and the presence of nystagmus, may indicate underlying neural dysfunction. These may result from lesions, seizure activity, or adverse reactions to ASM. The ALTOIDA app is at the forefront of this application [9].
-
9.
Monitoring through smartphone games: Analyzing changes in playing frequency and performance in smartphone games such as Candy Crush or Chess (as assessed by ELO ratings) can serve as measures to assess cognitive and sensorimotor function. Significant changes in gaming behavior not only reflect potential impairments in these areas, but may also indicate shifts in an individual’s drive and motivation. This approach provides a noninvasive, engaging way to monitor through enjoyable everyday activities.
-
10.
Combined integrated measures: Modern smart devices are capable of capturing a wide range of digital biomarkers and cognitive proxies over different time scales. The key challenge is to distinguish clinically relevant biomarkers from those that are not. Achieving this distinction requires thorough validation studies to establish the reliability and relevance of each biomarker. At the same time, artificial intelligence (AI) plays a critical role in streamlining the vast data landscape to enable more efficient and accurate analysis. The Altoida app exemplifies this approach by using AI to evaluate over 800 biomarkers across 13 functional domains [9]. This integration of AI and digital biomarkers paves the way for potential breakthroughs in personalized medicine and diagnostic precision.
-
1.
-
B.
Active measurement strategies
-
11.
Gamification of cognitive assessments via smart devices: Transform traditional cognitive tests by incorporating elements of gamification into smart device-based test tasks. This approach may target key cognitive areas on a daily or weekly basis such as memory and executive function, engaging users in a more interactive and enjoyable testing experience.
-
12.
Surveys on well-being and complaints to assess quality of life (QoL): Utilize comprehensive surveys delivered through smart devices on a daily, weekly, or monthly basis to gauge individual well-being and specific health complaints.
-
13.
Explicit sensorimotor tasks: Implement a variety of explicit sensorimotor tasks within smart device platforms on a daily to weekly basis to monitor individually defined sensorimotor domains.
-
11.
The use of digital biomarkers and cognitive proxies, as outlined earlier, represents a promising avenue for personalized monitoring of neurocognitive and sensorimotor functions in patients with epilepsy. Although these cognitive proxies are not intended to replace comprehensive traditional neuropsychological assessment, they can significantly enhance neuropsychological diagnostics. They do so by providing insight into performance variability within specific functional domains that may be influenced by transient pathogenic events such as epileptic activity. However, the effective integration of these tools into clinical practice depends on rigorous longitudinal validation studies. These studies must include repeated administration of a full neuropsychological test battery to identify the most specific and sensitive cognitive proxies in the relevant functional domains.
A pioneering approach to comprehensive smartphone-based monitoring of cognitive and sensorimotor functions for diagnostic purposes is the development of the ALTOIDA app (altoida.com 80 M Street SE, Suite 100 Washington, DC 20003 USA). This application, designed to assess an individual’s risk of developing Alzheimer’s dementia, incorporates both active and passive biomarkers. Its effectiveness and reliability have been demonstrated in a longitudinal validation study conducted alongside standard neuropsychological tests. This highlights the potential of such technologies to revolutionize diagnostics in neurological disciplines.
However, the development and use of digital biomarkers and cognitive proxies requires strict adherence to national and international privacy standards. As the continuous monitoring of patient behavior through these technologies represents a significant intrusion into personal privacy, ensuring robust data protection measures is paramount. This is particularly critical in the expanding realm of global digital interactions, where the protection of patient privacy must be a priority. Such ethical considerations are integral to the responsible development and application of digital health monitoring tools in neurology and beyond.
Conclusion
The ubiquity of smart devices, which are not inherently medical tools, has opened up new avenues for patient monitoring, especially for those undergoing novel stimulation therapies. Here, we emphasize the critical need for interdisciplinary research collaborations to leverage these devices effectively. The primary focus is on addressing the gap in monitoring sporadic cognitive and behavioral side effects arising from such therapies, which traditional neuropsychological testing methods fail to capture adequately. We argue for the development of innovative methodologies that integrate smart technology for continuous and comprehensive monitoring. This approach is vital for a more nuanced understanding of the side effects associated with new stimulation therapies, ensuring patient safety and optimizing treatment outcomes.
References
Kanner AM, Helmstaedter C, Sadat-Hossieny Z, Meador K (2020) Cognitive disorders in epilepsy I: clinical experience, real-world evidence and recommendations. Seizure 83:216–222. https://doi.org/10.1016/j.seizure.2020.10.009
Roliz AH, Kothare S (2023) The relationship between sleep, epilepsy, and development: a review. Curr Neurol Neurosci Rep 23(9):469–477. https://doi.org/10.1007/s11910-023-01284-0
Hermann B, Loring DW, Wilson S (2017) Paradigm shifts in the neuropsychology of epilepsy. J Int Neuropsychol Soc 23(9–10):791–805. https://doi.org/10.1017/S1355617717000650
Fisher RS (2023) Deep brain stimulation of thalamus for epilepsy. Neurobiol Dis 179:106045. https://doi.org/10.1016/j.nbd.2023.106045
Peltola J, Colon AJ, Pimentel J et al (2023) Deep brain stimulation of the anterior nucleus of the thalamus in drug-resistant epilepsy in the MORE multicenter patient registry. Neurology 100(18):e1852–e1865. https://doi.org/10.1212/WNL.0000000000206887
Salanova V, Witt T, Worth R et al (2015) Long-term efficacy and safety of thalamic stimulation for drug-resistant partial epilepsy. Neurology 84(10):1017–1025. https://doi.org/10.1212/WNL.0000000000001334
Tröster AI, Meador KJ, Irwin CP, Fisher RS, SANTE Study Group (2017) Memory and mood outcomes after anterior thalamic stimulation for refractory partial epilepsy. Seizure 45:133–141. https://doi.org/10.1016/j.seizure.2016.12.014
van Nieuw Amerongen AR, Meppelink AM, Ghosh A, Thijs RD Real-world smartphone data can trace the behavioural impact of epilepsy: a case study. medRxiv 2024.01.01.23300494. https://doi.org/10.1101/2024.01.01.23300494
Seixas AA, Rajabli F, Pericak-Vance MA, Jean-Louis G, Harms RL, Tarnanas I (2022) Associations of digital neuro-signatures with molecular and neuroimaging measures of brain resilience: The altoida large cohort study. Front Psychiatry 13:899080. https://doi.org/10.3389/fpsyt.2022.899080
Funding
Open access funding provided by University of Zurich
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
H. Jokeit, E. Kaufmann, J. Peltola and L. Imbach declare that they have no competing interests.
For this article no studies with human participants or animals were performed by any of the authors. All studies mentioned were in accordance with the ethical standards indicated in each case.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.

Scan QR code & read article online
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Jokeit, H., Kaufmann, E., Peltola, J. et al. Precision epileptology: digital biomarkers and cognitive proxies for personalized care. Clin Epileptol (2024). https://doi.org/10.1007/s10309-024-00682-9
Accepted:
Published:
DOI: https://doi.org/10.1007/s10309-024-00682-9