
Abstract
Background
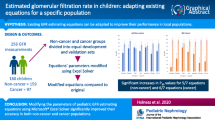
We have developed a simple and easy method of estimating the glomerular filtration rate (eGFR) of serum creatinine in Japanese children (eGFRUemura). The eGFR equation is for children aged 2–18 years. Therefore Uemura et al. developed an equation for children younger than 2 years (eGFRunder 2). The aim of the present study was to validate this new equation.
Methods
We collected the data of 13 patients from previous studies and compared the results of eGFRunder 2, eGFRUemura, and updated eGFR developed by Schwartz (eGFRSchwartz) with measured GFR using mean error (ME), root mean square error (RMSE), P30 and Bland–Altman analysis.
Results
The ME of eGFRunder 2, eGFRUemura and eGFRSchwartz were 2.3 ± 15.9, 7.7 ± 14.5, and 16.0 ± 18.2 ml/min/1.73m2, respectively. The RMSEs were 15.5, 15.9, and 49.6, respectively. The P30 values were 76.9%, 76.9%, and 53.8%, respectively. The graph of Bland–Altman bias analysis showed fan-shape. The eGFRunder 2 equation was the most accurate in the three equations.
Conclusion
The eGFRunder 2 equation was useful for Japanese children younger than 2 years.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The gold standard for evaluation of renal function is inulin clearance (Cin). However, the procedure of Cin is complicated and difficult, especially in younger children and/or patients with bladder dysfunction. Therefore, various simple and easy methods to determine the estimated GFR (eGFR) have been developed. Recently, the most known equation for eGFR used in children is the updated Schwartz (eGFRSchwartz) equation [1]. However, Uemura et al. reported that the eGFRSchwartz equation is not applicable for Japanese children [2]. Therefore, an original equation for eGFR (eGFRUemura) was developed using serum creatinine (Cr) in Japanese children [3], and its accuracy was validated [4]. However, the equation was for children aged 2–18 years. Therefore, an equation for children younger than 2 years was then developed by multiplying eGFRUemura by a coefficient (0.107 × ln(age[month]) + 0.656) [5]. In this study, we aimed to validate eGFRunder 2 equation.
Material and methods
Study population
We extracted the data of patients under 2 years of age from three studies. The first was 7 of 174 patients’ data when the eGFRUemura equation was created [3]. The second was 8 of 140 patients’ data when the accuracy of the eGFRUemura equation was validated [4]. The third was 1 of 59 patients’ data validated the safety of Inulide® for Japanese children (in press) (Table 1). All data were collected from pediatric patients with chronic kidney disease (CKD) in clinical need of Cin. Finally, we used data from 13 patients after excluding patients (Table1).
The measured GFR (mGFR) for each patient was obtained using Cin. The procedure is described in a previous report [6]. Cin values were measured in the same way in three studies.
The calculate method of eGFRunder 2 is as follows:
-
1.
The reference serum Cr level (ref Cr) is shown by the following two equations of body length (x):
males: ref Cr = − 1.259x5 + 7.815x4 – 18.57x3 + 21.39x2 – 11.71x + 2.628
females: ref Cr = − 4.536x5 + 27.16x4 – 63.47x3 + 72.43x2 – 40.06x + 8.778
-
2.
Provisional GFR = 110.2 × (ref Cr/ patient’s serum Cr) + 2.93
-
3.
R = 0.107 × ln [age (months)] + 0.656
-
4.
eGFR under 2 years of age (eGFRunder 2) = R × provisional GFR
Exclusion criteria and cases excluded
The exclusion criteria were as follows:
-
1.
Primary diseases including severe obstructive uropathy, infection during treatment, inflammatory disease, dehydration, neuromuscular disease, severe cardiac, hepatic, or pancreatic disease, and/or endocrine disease, including thyroid impairment.
-
2.
Cases in which the ratios of inulin excretion and intravenous inulin administration were < 0.5, or > 1.5, during the measurement of Cin. We determined the dose of intravenous inulin by assuming that the blood concentration was constant during testing. Ratios of inulin excretion and intravenous inulin that were not within 0.5 and 1.5 may have been due to failure to collect all urine.
-
3.
Cases in which the measured GFR (mGFR) was > 150 ml/min/1.73m2; pediatric patients with CKD due to a hyperfiltration disease such as diabetic nephropathy are rare. We were only interested in cases in which GFR was < 120 ml/min/1.73m2. Therefore, we excluded cases in which mGFR was > 150 ml/min/1.73m2.
Statistical analysis
To validate eGFR under 2 equation, we used four methods as follows:
-
1.
Mean error (ME): to evaluate the mean difference between each value for eGFR and mGFR values
-
2.
Root mean square error (RMSE): to evaluate the precision of eGFR and mGFR values.
-
3.
P30 (the percentage of eGFR value within 30% of mGFR): to evaluate the accuracy of eGFR and mGFR values.
-
4.
Bland–Altman analysis (difference versus average): to determine agreement with the estimation.
We also compared these statistical results of eGFRunder 2 equations, with the results of eGFRUemura, and eGFRSchwartz.
The formula for eGFR Uemura equation is mentioned above in the calculation method of eGFRunder 2 from (1) to (2). First, calculate the reference Cr level as described (1), and then the eGFRUemura from reference Cr and patient’s serum Cr using the method described in (2).
The updated Schwartz equation is as follows: eGFR (ml/min/1.73 m2) = 0.413 × body length (cm)/serum Cr value (mg/dL) by enzymatic Cr determination in children aged 1–16 years [1]. Therefore, in the second analysis, the data of three patients under 1 year of age were excluded. Finally, data from 10 patients were used for comparison between eGFRunder 2 and eGFRSchwartz.
All analyses were performed using GraphPad Prism for Mac OS X (version 7.0).
Results
Characteristics of the study population (Table 1)
Data of 6 patients were extracted from the three studies. Data of three patients were excluded because the ratios of urinary inulin excretion to intravenous inulin administration were < 0.5 or > 1.5. None of the patients were included in the 1 or 3 exclusion criteria. Finally, 13 patients’ data (2 female, median 17.0 months of age [interquartile range (IQR) 10.0–20.5 months, range 1–23 months]) were used for analysis (Fig. 1). The number of chronic kidney disease (CKD) stages 1, 2, 3, 4, and 5 were 2, 4, 6, 1, and 0, respectively. The number of renal abnormalities, congenital anomalies of the kidney and urinary tract (CAKUT), solitary kidney, reflux nephropathy, hydronephrosis, and small kidney were 6, 3, 2, 1, and 1, respectively.

Flow chart of included data
Result of statistical analysis
Figure 2 shows a scatter plot of mGFR versus each of the three eGFR equations. The straight line shows the equivalent values of mGFR and eGFR. The open circles represent the patient data under 1 year of age. The scatter plots of eGFRunder 2 and eGFRUemura seem to be similar. Figure 3 shows the Bland–Altman plot of the difference versus the average for both mGFR and each 3 eGFR equations.

Scatter plot of mGFR versus each 3 eGFR equations. a eGFRunder 2, b eGFRUemura, c eGFRSchwartz. Straight line: Y = X, Open circle: data of children under 1-year-old

Bland–Altman plot. Difference versus average mGFR and each 3 eGFR equations. a eGFRunder 2, b eGFRUemura, c eGFRSchwartz. Open circle: data of children under 1 year old
Table 2a shows the numerical values for each examination in all 13 patients. The ME values for eGFRunder 2, eGFRUemura, and eGFRSchwartz were 2.3 ± 15.9, 7.7 ± 14.5, and 16.0 ± 18.2 ml/min/1.73m2, respectively. The RMSE values were 15.5, 15.9, and 49.6 ml/min/1.73m2, respectively. The P30 values were 76.9%, 76.9%, and 53.8%, respectively. Table 2b shows the numerical values for the results of eGFRunder 2 and eGFRSchwartz in 10 patients aged between 1 and 2 years. The ME values for eGFRunder 2, and eGFRSchwartz were 5.3 ± 17.0 and 16.0 ± 20.7 ml/min/1.73m2, respectively. The RMSE values were 16.9 and 50.0 ml/min/1.73 m2, respectively. The P30 values were 70.0%, and 50.0%, respectively.
Figure 3 shows a scatter plot of the Bland–Altman analysis. In all three equations, the spread of the graph of the Bland–Altman analysis was fan-like shaped, with systematic error.
In the three equations, the values using eGFRunder 2 equation showed the lowest value for ME and Bland–Altman analysis, and showed the larger values for P30 than that for eGFRSchwartz.
Discussion
We evaluated a new eGFR equation for children under 2 years of age. Using several statistical techniques, we confirmed that the eGFRunder 2 equation could be useful.
For Japanese children, there are several eGFR equations with surrogate markers, serum Cr [3], cystatin C [7], and β2 microglobulin [8]. The Cr-based eGFR Uemura equation is the most commonly used method for children aged 2–18 years. Cystatin C and β2 microgrobulin based eGFR are not always available for retrospective epidemiologic studies or common clinical practice. Therefore, we developed Cr-based eGFR for children younger than 2 years using eGFRUemura using a coefficient. The method reported in a previous article [5] is based on the following idea. Physiologically, kidney function gradually increases from birth and reaches adult stage at the age of 2 years. Using the median normal reference values of GFR for each age (months) up to 2 years examined previously, we estimated the percentage of the normal adult GFR that corresponds to and calculated a regression curve using a logarithmic function. As a result, the coefficient was calculated as 0.107 × ln [age (months)] + 0.656. The aim of this study was to evaluate the eGFR under 2 equations. We compared the values of eGFRunder 2, eGFRUemura, and eGFRSchwartz equation using ME, RMSE, P30, and Bland–Altman analysis. We divided the patients according to age: 13 patients under 2 years of age and 10 patients aged between 1 and 2 years; patient data underwent two analyses. Because eGFRunder 2 equation is for children under 2 years old, the eGFRUemura equation is for children aged 2–18 years and eGFRSchwartz is for children aged 1–16 years. Therefore, in the comparison of 10 patients at the age of 1 to 2 years, we only compared eGFRunder 2 equation and eGFR Schwartz. In the analysis of 13 patients, the ME value of eGFRunder 2 was the smallest among the three equations. The RMSE value and percent of P30 of eGFRunder 2 and eGFRUemura were similar. On the other hand, the ME and RMSE values of eGFR Schwartz were the highest, and the percentage of P30 was the lowest among the three eGFR equations. In the analysis of 10 patients, the ME and RMSE values of eGFRunder 2 were lower than that of eGFRSchwartz. The percentage of P30 of eGFRunder 2 was higher than that of eGFRSchwartz.
This study has several limitations. First, the sampling data was small particular under 1 year of age. Although we collected patients’ data from our three previous studies, there were only 13 among 373 patients (3.5%) under 2 years of age. Further, it is very rare to perform inulin clearance in patients under 2 years of age, thus limiting data collection. In addition to that, there were only two patients of a female under the age of two. However, since there was no gender difference in normal Cr values at younger ages [9], we believed that this result was not affected. Second, to add to the data as much as possible, we also used the patient data when creating the equation of eGFRUemura. Third, we did not exclude preterm infants and low birth weight infant because we had no information for them. We don’t know whether the eGFRunder 2 equation can be applied to such cases or not.
Conclusion
We evaluated the eGFRunder 2 equation for Japanese children aged 2 years or less. The results suggest that eGFRunder 2 equation could be a useful parameter.
References
Schwartz GJ, Muoz A, Schneider MF, Mak RH, Kaskel F, Warady BA, Furth SL. New equations to estimate GFR in children with CKD. J Am Soc Nephrol. 2009;20(3):629–37.
Uemura O, Honda M, Matsuyama T, Ishikura K, Hataya H, Nagai T, Ikezumi Y, Fujita N, Ito S, Iiijima K. Is the new Schwartz equation derived from serum creatinine and body length suitable for evaluation of renal function in Japanese children? Eur J Pediatr. 2012;171(9):1401–4.
Uemura O, Nagai T, Ishikura K, Ito S, Hataya H, Gotoh Y, Fujita N, Akioka Y, Kaneko T, Honda M. Creatinine-based equation to estimate the glomerular filtration rate in Japanese children and adolescents with chronic kidney disease. Clin Exp Nephrol. 2014;18(4):626–33.
Gotoh Y, Uemura O, Ishikura K, Sakai T, Hamasaki Y, Araki Y, Hamada R, Honda M. Validation of estimated glomerular filtration rate equations for Japanese children. Clin Exp Nephrol. 2018;22(4):931–7.
Uemura O, Ishikura K, Gotoh Y, Honda M. Creatinine-based estimated glomerular filtration rate for children younger than 2 years. Clin Exp Nephrol. 2018;22(2):483–4.
Nagai T, Uemura O, Ishikura K, Ito S, Hataya H, Gotoh Y, Fujita N, Akioka Y, Kaneko T, Honda M. Creatinine-based equations to estimate glomerular filtration rate in Japanese children aged between 2 and 11 years old with chronic kidney disease. Clin Exp Nephrol. 2013;17(6):877–81.
Uemura O, Nagai T, Ishikura K, Ito S, Hataya H, Gotoh Y, Fujita N, Akioka Y, Kaneko T, Honda M. Cystatin C-based equation for estimating glomerular filtration rate in Japanese children and adolescents. Clin Exp Nephrol. 2014;18(5):718–25.
Ikezumi Y, Uemura Y, Nagai T, Ishikura K, Ito S, Hataya H, Fujita N, Akioka Y. Beta-2 microglobulin-based equation for estimating glomerular filtration rates in Japanese children and adolescents. Clin Exp Nephrol. 2015;19(3):450–7.
Uemura O, Honda M, Matsuyama T, Ishikura K, Hataya H, Yata N, Nagai T, Ikezumi Y, Fujita N, Ito S, Iijima K, Kitagawa T. Age, gender, and body length effects on reference serum creatinine levels determined by an enzymatic method in Japanese children: a multicenter study. Clin Exp Nephrol. 2011;15(5):694–9.
Author information
Authors and Affiliations
Consortia
Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by YG, OU. The first draft of the manuscript was written by YG and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that no conflict of interest exists.
Human and animal rights
All procedures involving human participants were in accordance with ethical standards of the institution at which the studies were conducted (approval number in Japanese Red Cross Aichi Medical Center Nagoya Daini Hospital: 1447S), and with standards of the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Written informed consent was not obtained because of the use of retrospective data for clinical use. This information is available on the website (opt-out).
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Gotoh, Y., Uemura, O., Fujita, N. et al. Validation of the estimated glomerular filtration rate equation for Japanese children younger than 2 years. Clin Exp Nephrol 26, 266–271 (2022). https://doi.org/10.1007/s10157-021-02165-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10157-021-02165-x