
Abstract
Purpose
This study aimed to identify findings on non-ECG-gated CT pulmonary angiography (CTPA) indicating decreased left ventricle (LV) systolic function, later confirmed by echocardiogram.
Methods
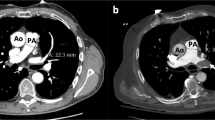
After obtaining institutional review board approval, review was performed of emergency department (ED) patients who had CTPA and follow-up echocardiogram within 48 h, over 18 months. Patients with pulmonary embolus, suboptimal CTPA, arrhythmias or pericardial tamponade were excluded. One hundred thirty-seven patients were identified and divided into cases (LVEF <40%, n = 52) and controls (LVEF >50%, n = 85). Two reviewers performed these analyses: measurement of enhancement in main pulmonary artery (MPA), LV, and aorta; subjective enhancement of LV and aorta (Ao) relative to MPA using a four-point Likert scale; contrast transit time (TD) to trigger CTPA and LV short & long axis dimensions. When available, the most recent N-terminal pro–B-type natriuretic peptide (NT-proBNP) level was recorded.
Results
Decreased aortic and LV subjective enhancement were the best predictors of LV systolic dysfunction. For Ao/MPA ratio, an optimal cutoff value of 0.20 resulted in a sensitivity of 0.54 and specificity of 0.93 (AUC = 0.83, 0.78–0.88 95% CI). A threshold of 86.7 HU for Ao enhancement resulted in a sensitivity of 0.68 and specificity of 0.90 (AUC = 0.82, 0.77–0.88 95% CI). A LV short axis diameter of more than 54.3 mm had a sensitivity of 0.62 and specificity of 0.98 (AUC = 0.88, 0.83–0.92 95% CI). For the LV long axis diameter, a cutoff of 87.5 mm resulted in a sensitivity of 0.66 and specificity of 0.84 (AUC = 0.78, 0.72–0.84 95% CI). With bolus timing, cases had a longer TD (13.4 vs. 10.4 s, p < 0.0001).
Conclusion
Unsuspected LV systolic dysfunction can be recognized on a CTPA by identification of decreased aortic enhancement, LV enlargement and increased TD. This has important diagnostic implications for the patient presenting with shortness of breath, chest pain, or dyspnea.




Similar content being viewed by others

Abbreviations
- AB:
-
Abhishek Chaturvedi
- TB:
-
Timothy Baran
- JT:
-
Joel Thompson
- KKJ:
-
Katherine Kaproth-Joslin
- SKH:
-
Susan K Hobbs
- AP:
-
Apeksha Chaturvedi
References
Kocher KE et al (2011) National trends in use of computed tomography in the emergency department. Ann Emerg Med 58(5):452–462 e3
National Center for Health Statistics, Emergency Department Summary Tables. 2011: p. 17.
Henzler T et al (2011) CT imaging of acute pulmonary embolism. J Cardiovasc Comput Tomogr 5(1):3–11
Mamlouk MD et al (2010) Pulmonary embolism at CT angiography: implications for appropriateness, cost, and radiation exposure in 2003 patients. Radiology 256(2):625–632
Lu MT et al (2009) Comparison of ECG-gated versus non-gated CT ventricular measurements in thirty patients with acute pulmonary embolism. Int J Cardiovasc Imaging 25(1):101–107
Lin FY et al (2008) Cardiac chamber volumes, function, and mass as determined by 64-multidetector row computed tomography: mean values among healthy adults free of hypertension and obesity. JACC Cardiovasc Imaging 1(6):782–786
Kathiria NN et al (2015) Assessment of left ventricular enlargement at multidetector computed tomography. J Comput Assist Tomogr 39(5):794–796
Lu MT et al (2012) Axial and reformatted four-chamber right ventricle-to-left ventricle diameter ratios on pulmonary CT angiography as predictors of death after acute pulmonary embolism. AJR Am J Roentgenol 198(6):1353–1360
Kang DK et al (2011) CT signs of right ventricular dysfunction: prognostic role in acute pulmonary embolism. JACC Cardiovasc Imaging 4(8):841–849
Bae KT (2010) Intravenous contrast medium administration and scan timing at CT: considerations and approaches. Radiology 256(1):32–61
Husmann L et al (2006) Influence of cardiac hemodynamic parameters on coronary artery opacification with 64-slice computed tomography. Eur Radiol 16(5):1111–1116
John G et al (2016) Contrast circulation time to assess right ventricular dysfunction in pulmonary embolism: a retrospective pilot study. PLoS One 11(8):e0159674
Lang RM et al (2015) Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J Am Soc Echocardiogr 28:1–39
Raja AS et al (2012) Effect of computerized clinical decision support on the use and yield of CT pulmonary angiography in the emergency department. Radiology 262(2):468–474
Roger VL (2013) Epidemiology of heart failure. Circ Res 113(6):646–659
Schellenbaum GD et al (2004) Survival associated with two sets of diagnostic criteria for congestive heart failure. Am J Epidemiol 160(7):628–635
Chen WC, Tran KD, Maisel AS (2010) Biomarkers in heart failure. Heart 96(4):314–320
Cowie MR et al (2003) Clinical applications of B-type natriuretic peptide (BNP) testing. Eur Heart J 24(19):1710–1718
Udelson JE (2011) Heart failure with preserved ejection fraction. Circulation 124(21):e540–e543
Minkowitz S et al (2014) Can left ventricular function be assessed on non-ECG-gated CT? Clin Imaging 38(5):669–674
Lakoma A et al (2010) Measurement of pulmonary circulation parameters using time-resolved MR angiography in patients after Ross procedure. AJR Am J Roentgenol 194(4):912–919
Manghat NE et al (2007) Multi-detector row CT coronary angiography in patients with cardiomyopathy—initial single-centre experience. Clin Radiol 62(7):632–638
Mahnken AH et al (2003) Measurement of cardiac output from a test-bolus injection in multislice computed tomography. Eur Radiol 13(11):2498–2504
Hetal H. Mehta, Brian G. Choi, Reza Sanai, Raman S. Dusaj, Amr Mohsen, Chunlei Liang, Jannet F. Lewis, Robert K. Zeman, Validation of a novel method for cardiac output estimation by CT coronary angiography. Scientific Research, 2012. 1(2).
Bae KT (2005) Test-bolus versus bolus-tracking techniques for CT angiographic timing. Radiology 236(1):369–370 author reply 370
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Informed consent
Informed consent from individuals was waived by the IRB in this retrospective study.
Electronic supplementary material
Supplementary Figure 1a
Box plots, separated by Ao subjective score, showing differences in LV diameters (TIFF 56 kb)
Supplementary Figure 1b
contrast enhancement (TIFF 70 kb)
Supplementary Figure 1c
contrast enhancement ratios (TIFF 51 kb)
Supplementary Figure 1d
bolus triggering time (TIFF 56 kb)
Supplementary Figure 1e
BNP. Center lines correspond to median values, boxes span from the first to third quartiles, and whiskers represent minimum and maximum values. (TIFF 55 kb)
Rights and permissions
About this article

Cite this article
Chaturvedi, A., Thompson, J.P., Kaproth-Joslin, K. et al. Identification of Left Ventricle Failure on Pulmonary Artery CTA: Diagnostic Significance of Decreased Aortic & Left Ventricle Enhancement. Emerg Radiol 24, 487–496 (2017). https://doi.org/10.1007/s10140-017-1494-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10140-017-1494-6