
Abstract
Introduction
Studies on adherence to exercise therapy of patients with ankylosing spondylitis (AS) are rare, and the criteria for adherence to exercise are inconsistent. This study aimed to quantify patient-reported adherence to exercise therapy of Chinese outpatients with AS and investigate the factors related to poor adherence.
Methods
The subjects’ sociodemographic, disease-related, radiographic, and laboratory parameters were collected. Patients’ adherence to exercise therapy was assessed using the Exercise Attitude Questionnaire (EAQ) with a 4-point Likert scale. All cases were grouped as good adherence and poor adherence using a cutoff score of 60, according to a previous study. Univariate analysis was conducted to assess the intergroup differences. Then, we built a multivariate logistic regression model to identify possible significant factors related to poor adherence to exercise therapy.
Results
A total of 185 outpatients completed the questionnaire. The mean EAQ score was 49.4 (IQR, 40.7–59.3) and 146 patients (78.9%) were considered to have poor adherence, and 39 patients (21.1%) were considered to have good adherence. The rates of current nonsteroidal anti-inflammatory drugs (NSAIDs), conventional synthetic disease-modifying antirheumatic drugs (csDMARDs), and tumor necrosis factor-α inhibitor (TNF-i) use were significantly higher in the poor adherence group (p=0.001, p=0.027, p=0.018, respectively). Our multivariate logistic regression model revealed that the only significant associated factor was current use of NSAIDs (OR=3.517; p=0.016; 95% CI, 1.259–9.827).
Conclusions
Outpatients with AS had an unacceptable level of adherence to exercise therapy, and current use of NSAIDs was a significantly associated factor.
Key Points • Outpatients with AS had an unacceptable level of adherence to exercise therapy. • Current use of NSAIDs exerted a negative impact on patients’ adherence to exercise therapy. |
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Ankylosing spondylitis (AS) is a disease prototype of a heterogeneous group of inflammatory arthritis known as seronegative spondyloarthropathies [1, 2]. AS mainly affects the spine and sacroiliac joints, causing characteristic inflammatory back pain. If untreated, this may progress to severe damage to the spine, sacroiliac joint, and peripheral joints with functional impairment, reduction of physiological range of motion (ROM), deformity, disability, and compromised psychological status and quality of life [3,4,5].
Adherence, defined by the World Health Organization (WHO) as “the extent to which a person’s behavior-taking medications, following a diet, and/or executing lifestyle changes corresponds with agreed recommendations from the health care provider,” is an extremely important determinant in the good control of AS. High rates of poor adherence to prescribed medications by patients with AS have been reported in some previous studies [6,7,8,9] and the consequences of this include increased disease activity and disability, increased number of disease flares, and increased healthcare costs [10, 11].
Although the treatment of AS has been revolutionized with the advent of biological therapies, rehabilitation is still a promising nonpharmacological therapy in AS, which usually include aerobic exercise, respiratory kinesiotherapy, strengthening, stretching, and balance and gait training. In AS, the main goals of exercise focus on pain control, prevention and delay of stiffness, improvement of function and gait, and correction of deformity in combination with pharmacological therapy [12, 13]. However, reports on adherence to physical exercises in patients with AS are relatively rare [7, 8, 14], and the criteria for adherence to exercises have been inconsistent.
The Exercise Attitude Questionnaire (EAQ) was introduced previously for the evaluation of adherence to exercise therapy [15] and its reliability and validity have been confirmed [8, 15]. To the best of our knowledge, this was the first study to assess adherence to exercise therapy of Chinese outpatients with AS by EAQ. The aims of the study were to quantify patient-reported adherence to exercise therapy and to investigate the possible factors related to poor adherence.
Materials and methods
Patient enrollment
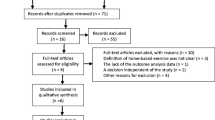
This cross-sectional study included 232 consecutive outpatients who fulfilled the modified New York criteria [16] for AS at Beijing Jishuitan Hospital from February 2019 to September 2021. All patients gave their informed consent prior to inclusion in the study. The exclusion criteria were as follows: (1) age ≥ 50 years or ≤ 18 years; (2) any diagnosis of psychiatric disorders and currently on psychiatric treatments, and cognitive dysfunction; and (3) incomplete questionnaires.
Patient demographics and clinical characteristics
The participants’ sociodemographic factors included body mass index (BMI), sex, age at outpatient visit, family history, education level (primary school, junior middle school, senior middle school or professional education, and university/graduate education), working status (employed, unemployed, or retired), and smoking habits (current or past).
The disease-related characteristics included age at onset of AS, duration of AS, diagnosis delay, visual analog scale (VAS) of global back pain, extra-articular manifestations (EAMs) (current or past) including uveitis, psoriasis, and inflammatory bowel disease (IBD), and medication status. Diagnosis delay was defined as the interval between a patient’s first spondyloarthritis symptoms and the correct diagnosis of AS. The use of medications including nonsteroidal anti-inflammatory drugs (NSAIDs), conventional synthetic disease-modifying antirheumatic drugs (csDMARDs), and tumor necrosis factor-α inhibitors (TNF-i) was recorded, and the patients were considered current users if usage was noted in the patient record for half a year or longer before the evaluation period. Disease activity and functional status were assessed using the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) [17] and Bath Ankylosing Spondylitis Functional Index (BASFI) [18], respectively. Patient-reported outcomes were assessed using the Ankylosing Spondylitis Quality of Life Index (ASQOL) [19] and the short form-12 (SF-12) [20], which have physical component summary (PCS) and mental component summary (MCS) scores. ASQOL is a validated 18-item questionnaire that assesses the quality of life of AS patients. Comorbidities were evaluated using the rheumatic disease comorbidity index (RDCI) (range 0–10), representing the weighted sum score of common comorbidities (myocardial infarction, stroke, other heart diseases, lung disease, diabetes mellitus, hypertension, cancer, fracture, gastrointestinal ulcer, other gastrointestinal problems, and depression) [21].
Data on clinical characteristics were collected and evaluated independently by two rheumatologists (L.H.C. and M.S.L.), who had not participated in the study design, using a face-to-face questionnaire and medical records.
Radiographic and laboratory data
The anteroposterior (AP) radiographs of the pelvis were obtained during outpatient visits, which were used to grade the damage of the sacroiliac joints (SIJs) according to the modified New York scoring method [16]. Radiographic damage of the spine was scored using the modified Stoke AS Spine Score (mSASSS) [22] from full-length radiographs of the spine. The bath ankylosing spondylitis radiology index of hip (BASRI-h) system was adopted to assess the severity of radiological involvement in the hip joint [23], which classifies the status of the hip joint into a 5-point scale from 0 to 4. The final score for radiographic damage of the SJI and hip was assessed on the side with more severe involvement. Laboratory data including human leukocyte antigen (HLA)-B27 status; serum erythrocyte sedimentation rate (ESR); and C-reactive protein (CRP), hemoglobin (HGB), and albumin (ALB) levels were also measured at enrollment.
Adherence evaluations
The 18-item EAQ measures patients’ adherence to exercise therapy using a 4-point Likert scale (strongly disagree, 1 point; somewhat disagree, 2 points; somewhat agree, 3 points; strongly agree, 4 points). The final score was calculated by adding up all items, subtracting 18, and then dividing it by 54 in order to take it to a 0–1 scale; finally, it was multiplied by 100, obtaining a final range from 0 (no adherence) to 100 (perfect adherence) [8, 15].
Statistical analysis
Descriptive data of categorical variables were expressed as percentages and frequencies, and of continuous variables, as mean and standard deviation (SD) or median and interquartile range ([IQR] 25–75%) if the data were skewed.
The correlations of EAQ score with clinical continuous variables and with ordinal variables were determined by correlation coefficient (r) in Pearson correlation analysis and Spearman rank correlation analysis, respectively. The cases in our series were grouped as good adherence and poor adherence using a cutoff score of 60, according to a previous study [7]. We conducted a univariate analysis to assess intergroup differences, using independent sample Student’s t tests or Mann–Whitney tests for continuous variables and chi-squared tests for dichotomous variables, respectively. All reported p values were two-tailed, with an alpha of 0.05. Next, a multivariate logistic regression model was used to assess the risk factors identified as significant in the analysis, and the odds ratio with 95% confidence interval (CI) and the associated p value were determined. In the multivariable binary logistic regression analysis, variables with a p value of ≤ 0.05 were assumed to be statistically significant determinants of poor adherence to exercise therapy. All analyses were performed using the IBM SPSS Statistics version 24.
Results
A total of 185 outpatients completed the questionnaire. The mean EAQ score was 49.4 (IQR, 40.7–59.3); 146 patients (78.9%) were considered to have poor adherence (EAQ score ≤ 60), and 39 patients (21.1%) were considered to have good adherence (EAQ score >60). The patient sociodemographic, disease-related, radiographic, and laboratory parameters in the two groups are summarized in Table 1. The percentages of current NSAIDs, csDMARDs, and TNF-i use were significantly higher in the poor adherence group (p=0.001, p=0.027, p=0.018, respectively). The ESR and CRP levels were also significantly higher in the poor adherence group (p=0.025 and p=0.014, respectively). We found a statistically significant correlation between the EAQ score and age at outpatient visit (r=−0.203; p=0.005) and CRP (r=−0.250; p=0.001).
The related factors identified as significant were introduced into the multivariate logistic regression model to assess the possible effects of these parameters on poor adherence to exercise therapy. The model revealed that only the current use of NSAIDs was a significantly associated factor (OR, 3.517; p=0.016; 95%CI, 1.259–9.827) (Table 2).
Discussion
Exercise therapy is a cornerstone of current global treatment strategies for patients with AS. The primary goals of exercise therapy for patients with AS are to control pain, improve the mobility and strength of the involved joints, prevent or decrease deformity of the axial skeleton and peripheral joints, and ultimately improve the overall function and quality of life [24, 25]. Our research was the first cross-sectional study to assess adherence to exercise therapy of outpatients with AS and analyze its relationship with sociodemographic, disease-related, radiographic, and laboratory parameters.
There is no gold standard for the evaluation of adherence. Clinically, adherence to exercise therapy is measured using various methods, making direct evaluation difficult [26]. In a study by Sang et al. [14], the criterion they selected as adherence to the standard exercise therapy was to exercise at least 30 min per day and perform back exercise at least 5 days per week. Obviously, this was only a qualitative evaluation criterion. The EAQ is an easy-to-understand, quick, and self-administered questionnaire; its reliability and validity in clinical settings have been confirmed in previous studies [8, 15]. Consequently, we used EAQ as our assessment tool for adherence to exercise therapy in patients with AS.
The percentage of adherence to exercise therapy varied widely from 51 to 95% in published literature [15, 26]. Arturi et al. [8] investigated the adherence of exercise among 59 patients with AS using the EAQ. The median value of EAQ was 40.7 (IQR, 5.6–77.8). Using a cutoff EAQ value higher than 60, they dichotomized the patients as adherent and non-adherent, and 53 patients adhered to the exercise regimen. In contrast, the percentage of adherence to exercise therapy in our series was only 79% (146/185), well below the level mentioned above.
Medication adherence of patients with AS has been evaluated in previous studies, and the associated factors include advanced age, quality of life, patients’ beliefs about medicines and illness perceptions, choice of drugs, and route of administration [6,7,8,9, 27]. Unfortunately, no study has specifically addressed the determinant factors for adherence to exercise therapy. In our series, patient sociodemographic, disease-related, radiographic, and laboratory parameters were identified. We found a weak correlation between EAQ score and age at outpatient visits (r=−0.203; p=0.005), but the latter was not statistically significantly different between the good and poor adherence group. The level of CRP was negatively correlated with the EAQ score (r=−0.250; p=0.001), and the intergroup difference was also statistically significant (p=0.014). Unfortunately, we did not find any statistical significance for CRP (p=0.241) in our multivariate logistic regression model. Measurement of CRP level is one of the most widely used methods to assess disease activity of AS and was confirmed an independent risk factor for axial physical mobility and radiographic progression in patients with AS [28, 29]. AS patients with elevated CRP levels present poor physical mobility and new bone formation of spine, which may have an adverse effect on the adherence to exercise therapy.
In our study, the current use of NSAIDs was identified as the statistically significant factor for poor adherence to exercise therapy. This was an interesting finding, and our explanations are as follows. NSAIDs have always been considered the first-line therapy for patients with AS and can be highly effective for treating axial and peripheral symptoms, including pain, stiffness, and limited range of motion. Moreover, a series of studies provided supportive evidence that NSAIDs may slow the progression of bony changes in the spine in AS [30, 31]. Consequently, patients with AS tend to have better symptom control after receiving NSAIDs, including relief of pain and morning stiffness, and improvement of range of motion, which negatively impacts adherence to exercise therapy. Similarly, we also noted significant differences in the current use of csDMARDs and TNF-i between the good adherence and poor adherence groups, although they were not significant determinant factors in our multivariate logistic regression model.
The main limitation of our study was its single-center cross-sectional nature. In fact, adherence is a dynamic process that tends to decline over time. The results of the current study may not be generalizable to the population at large or to other regions, as our patients were enrolled from a single center. Second, the sample size was too small to find significant correlations with other risk factors. Third, it was impossible to assess all risk factors for poor adherence to physical exercise, including some sociodemographic factors, such as marital status, income level, and dietary pattern, and disease-related parameter, such as the Bath Ankylosing Spondylitis Metrology Index (BASMI).
In conclusion, lack of adherence to exercise therapy is a major concern in the treatment of patients with AS. According to our study, outpatients with AS have an unacceptable level of adherence to exercise therapy, and current use of NSAIDs was identified as the only significant associated factor with poor adherence. Clinically, there is an urgent need to develop comprehensive strategies to improve adherence to exercise therapy in patients with AS, and future studies can aim to determine the reasons behind the lack of adherence to exercise therapy.
Data availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Sieper J, Poddubnyy D (2017) Axial spondyloarthritis. Lancet 390:73–84. https://doi.org/10.1016/S0140-6736(16)31591-4
Taurog JD, Chhabra A, Colbert RA (2016) Ankylosing spondylitis and axial spondyloarthritis. N Engl J Med 375:1303. https://doi.org/10.1056/NEJMc1609622
Ritchlin C, Adamopoulos IE (2021) Axial spondyloarthritis: new advances in diagnosis and management. BMJ 372:m4447. https://doi.org/10.1136/bmj.m4447
van der Heijde D, Sieper J, Elewaut D, Deodhar A, Pangan AL, Dorr AP (2014) Referral patterns, diagnosis, and disease management of patients with axial spondyloarthritis: results of an international survey. J Clin Rheumatol 20:411–417. https://doi.org/10.1097/RHU.0000000000000180
Mangone M, Paoloni M, Procopio S, Venditto T, Zucchi B, Santilli V, Paolucci T, Agostini F, Bernetti A (2020) Sagittal spinal alignment in patients with ankylosing spondylitis by rasterstereographic back shape analysis: an observational retrospective study. Eur J Phys Rehabil Med 56:191–196. https://doi.org/10.23736/S1973-9087.20.05993-6
Tolu S, Rezvani A, Karacan İ, Bugdayci D, Küçük HC, Bucak ÖF, Aydin T (2020) Self-reported medication adherence in patients with ankylosing spondylitis: the role of illness perception and medication beliefs. Arch Rheumatol 35:495–505. https://doi.org/10.46497/ArchRheumatol.2020.7732
Smolen JS, Gladman D, McNeil HP, Mease PJ, Sieper J, Hojnik M, Nurwakagari P, Weinman J (2019) Predicting adherence to therapy in rheumatoid arthritis, psoriatic arthritis or ankylosing spondylitis: a large cross-sectional study. RMD Open 5:e000585. https://doi.org/10.1136/rmdopen-2017-000585
Arturi P, Schneeberger EE, Sommerfleck F, Buschiazzo E, Ledesma C, Maldonado Cocco JA, Citera G (2013) Adherence to treatment in patients with ankylosing spondylitis. Clin Rheumatol 32:1007–1015. https://doi.org/10.1007/s10067-013-2221-7
Goh H, Kwan YH, Seah Y, Low LL, Fong W, Thumboo J (2017) A systematic review of the barriers affecting medication adherence in patients with rheumatic diseases. Rheumatol Int 37:1619–1628. https://doi.org/10.1007/s00296-017-3763-9
Raghunath S, Hijjawi R, Hoon E, Shanahan EM, Goldblatt F (2019) Qualitative assessment of medication adherence in patients with rheumatic diseases on biologic therapy. Clin Rheumatol 38:2699–2707. https://doi.org/10.1007/s10067-019-04609-y
López-González R, León L, Loza E, Redondo M, Garcia de Yébenes MJ, Carmona L (2015) Adherence to biologic therapies and associated factors in rheumatoid arthritis, spondyloarthritis and psoriatic arthritis: a systematic literature review. Clin Exp Rheumatol 33:559–569
Zão A, Cantista P (2017) The role of land and aquatic exercise in ankylosing spondylitis: a systematic review. Rheumatol Int 37:1979–1990. https://doi.org/10.1007/s00296-017-3829-8
O’Dwyer T, McGowan E, O’Shea F, Wilson F (2016) Physical activity and exercise: perspectives of adults with ankylosing spondylitis. J Phys Act Health 13:504–513. https://doi.org/10.1123/jpah.2015-0435
Sang Y, Dong C, Fu T, Zhao R, Ge X, Zhou W, Ji J, Gu Z (2020) Associated factors with adherence to standard exercise therapy and health-related quality of life in Chinese patients with ankylosing spondylitis. Mod Rheumatol 30:149–154. https://doi.org/10.1080/14397595.2018.1559966
Manigandan C, Charles J, Divya I, Edward SJ, Aaron A (2004) Construction of exercise attitude questionnaire-18 to evaluate patients’ attitudes toward exercises. Int J Rehabil Res 27:229–231. https://doi.org/10.1097/00004356-200409000-00008
van der Linden S, Valkenburg HA, Cats A (1984) Evaluation of diagnostic criteria for ankylosing spondylitis. A proposal for modification of the New York criteria. Arthritis Rheum 27:361–368
Garrett S, Jenkinson T, Kennedy LG, Whitelock H, Gaisford P, Calin A (1994) A new approach to defining disease status in ankylosing spondylitis: the Bath Ankylosing Spondylitis Disease Activity Index. J Rheumatol 21:2286–2291
Calin A, Garrett S, Whitelock H, Kennedy LG, O’Hea J, Mallorie P, Jenkinson T (1994) A new approach to defining functional ability in ankylosing spondylitis: the development of the Bath Ankylosing Spondylitis Functional Index. J Rheumatol 21:2281–2285
Leung YY, Lee W, Lui NL, Rouse M, McKenna SP, Thumboo J (2017) Adaptation of Chinese and English versions of the Ankylosing Spondylitis Quality of Life (ASQoL) scale for use in Singapore. BMC Musculoskelet Disord 18:353. https://doi.org/10.1186/s12891-017-1715-x
Busija L, Pausenberger E, Haines TP, Haymes S, Buchbinder R, Osborne RH (2011) Adult measures of general health and health-related quality of life: medical outcomes study Short Form 36-Item (SF-36) and Short Form 12-Item (SF-12) Health Surveys, Nottingham Health Profile (NHP), Sickness Impact Profile (SIP), Medical Outcomes Study Short Form 6D (SF-6D), Health Utilities Index Mark 3 (HUI3), Quality of Well-Being Scale (QWB), and Assessment of Quality of Life (AQoL). Arthritis Care Res 63(Suppl 11):S383–S412. https://doi.org/10.1002/acr.20541
Stolwijk C, van Tubergen A, Ramiro S, Essers I, Blaauw M, van der Heijde D, Landewé R, van den Bosch F, Dougados M, Boonen A (2014) Aspects of validity of the self-administered comorbidity questionnaire in patients with ankylosing spondylitis. Rheumatology (Oxford) 53:1054–1064. https://doi.org/10.1093/rheumatology/ket354
Creemers MC, Franssen MJ, van’t Hof MA, Gribnau FW, van de Putte LB, van Riel PL (2005) Assessment of outcome in ankylosing spondylitis: an extended radiographic scoring system. Ann Rheum Dis 64:127–129. https://doi.org/10.1136/ard.2004.020503
MacKay K, Brophy S, Mack C, Doran M, Calin A (2000) The development and validation of a radiographic grading system for the hip in ankylosing spondylitis: the bath ankylosing spondylitis radiology hip index. J Rheumatol 27:2866–2872
Das P, Haldar R, Santhanam S, Ravindran V (2021) Therapeutic exercises and rehabilitation in axial spondyloarthropathy: balancing benefits with unique challenges in the Asia-Pacific countries. Int J Rheum Dis 24:170–182. https://doi.org/10.1111/1756-185X.14035
O’Dwyer T, O’Shea F, Wilson F (2015) Physical activity in spondyloarthritis: a systematic review. Rheumatol Int 35:393–404. https://doi.org/10.1007/s00296-014-3141-9
McDonald MT, Siebert S, Coulter EH, McDonald DA, Paul L (2019) Level of adherence to prescribed exercise in spondyloarthritis and factors affecting this adherence: a systematic review. Rheumatol Int 39:187–201. https://doi.org/10.1007/s00296-018-4225-8
Hromadkova L, Soukup T, Vlcek J (2015) Quality of life and drug compliance: their interrelationship in rheumatic patients. J Eval Clin Pract 21:919–924. https://doi.org/10.1111/jep.12399
Poddubnyy D, Haibel H, Listing J, Märker-Hermann E, Zeidler H, Braun J, Sieper J, Rudwaleit M (2012) Baseline radiographic damage, elevated acute-phase reactant levels, and cigarette smoking status predict spinal radiographic progression in early axial spondylarthritis. Arthritis Rheum 64:1388–1398. https://doi.org/10.1002/art.33465
Chen CH, Chen HA, Liao HT, Liu CH, Tsai CY, Chou CT (2015) The clinical usefulness of ESR, CRP, and disease duration in ankylosing spondylitis: the product of these acute-phase reactants and disease duration is associated with patient’s poor physical mobility. Rheumatol Int 35:1263–1267. https://doi.org/10.1007/s00296-015-3214-4
Wanders A, Dv H, Landewé R, Béhier JM, Calin A, Olivieri I, Zeidler H, Dougados M (2005) Nonsteroidal antiinflammatory drugs reduce radiographic progression in patients with ankylosing spondylitis: a randomized clinical trial. Arthritis Rheum 52:1756–1765. https://doi.org/10.1002/art.21054
Poddubnyy D, Rudwaleit M, Haibel H, Listing J, Märker-Hermann E, Zeidler H, Braun J, Sieper J (2012) Effect of non-steroidal anti-inflammatory drugs on radiographic spinal progression in patients with axial spondyloarthritis: results from the German Spondyloarthritis Inception Cohort. Ann Rheum Dis 71:1616–1622. https://doi.org/10.1136/annrheumdis-2011-201252
Funding
Project supported by Beijing JST Research Funding (ZR-202223).
Author information
Authors and Affiliations
Contributions
All authors were involved in the drafting of this article or the critical revising for the important intellectual content, and all authors approved the final version to be published. All authors had full access to all the data in the study and are responsible for the integrity of the data and the accuracy of data analysis. Study conception and design: Sai Ma and Liang Zhang. Acquisition of data: Siliang Man, Hongchao Li, Tao Bian, and Weiyi Li. Analysis and interpretation of data: Sai Ma and Liang Zhang.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All procedures involving human participants carried out in the studies were in accordance with the ethical standards of the institutional and/or national research committee and the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This study was approved by the Beijing Jishuitan Hospital Institutional Review Board (project number 202004-08), and the informed consent was obtained from each participant before the enrollment of this study.
Consent for publication
Not applicable
Disclosures
None.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Ma, S., Zhang, L., Man, S. et al. Patient-reported adherence to physical exercises of patients with ankylosing spondylitis. Clin Rheumatol 41, 2423–2429 (2022). https://doi.org/10.1007/s10067-022-06189-w
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10067-022-06189-w