
Abstract
Background
Regular exercise is essential in the treatment of Ankylosing Spondylitis (AS), as the main goals of the treatment are to reduce pain, restore function, avoid disability and structural deterioration, and improve quality of life (QoL). The purpose of this study is to ascertain whether patients adhere to exercise recommendations and to evaluate the effects of consistent exercise on patients' pain, function, disease activity, mood, and quality of life. Many studies emphasize the need for exercise in treatment of AS, but none reveal whether patients follow prescribed practices and the results of doing so.
Results
Exercising group had significantly decreased pain, erythrocyte sedimentation rate and Bath ankylosing spondylitis functional index and Bath ankylosing spondylitis disease activity index (BASDAI) scores (p < 0.05). There was no significant difference between the two groups in morning stiffness, mood, spinal mobility, and QoL parameters (p > 0.05). Regular exercise was positively correlated with physiotherapy history. Regression analysis revealed that with an increase of 1 unit in visual analog scale and BASDAI, regular exercise decreased by 0.087 and 0.116 units, respectively.
Conclusion
Our study revealed how much the patients considers and follows the recommended exercises and concluded that regular exercise habits should be developed since they offer promising effects in treatment of AS, hence, patients should be educated in this area, and particular exercise routines should be developed to encourage them to exercise.
Similar content being viewed by others

Background
Ankylosing Spondylitis (AS) is an autoimmune disease of unknown origin that belongs to the HLA B27-associated spondylarthritis group. This disease can affect the spinal and sacroiliac joints as well as peripheral joints and different organs [1].
Treatment of AS should not only include pharmacological but should also include non-pharmacological treatment approaches [2]. Non-pharmacological treatment includes exercise, physiotherapy and education, lifestyle changes and surgical treatment [3].
Because of the variety of assessment methods used, meta-analyses have demonstrated that home exercise therapies significantly reduce BASFI scores, depression scores, and pain ratings; therefore, a subgroup analysis should be performed for comparison. The findings show that home activities can help patients with AS improve their quality of life [4].
Patients with AS may benefit from exercise to reduce pain and improve joint mobility. In advanced stages of the disease, exercise has a great contribution in preventing the decrease in joint mobility due to ankylosis [5]. Regular exercise should be a part of the main treatment in patients with AS [6]. In line with these studies, while regular exercise is encouraged in patients with AS, this study was planned to determine and highlight how many patients followed and continued the recommended exercises.
The aim of this study is to identify AS patients who regularly perform the recommended exercises and to evaluate the effects of regular exercise on pain, disease activity, function, emotional status, and quality of life.
Methods
This study was conducted after obtaining approval from the local ethics committee and in accordance with the Declaration of Helsinki. Written consent was obtained from all patients participating in the study.
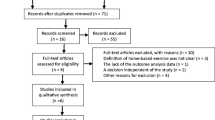
This study included 68 patients diagnosed with AS using the American College of Rheumatology’s (ACR’s) Modified New York criteria and followed in our Rheumatology outpatient clinic between December 2021 and January 2022. Patients diagnosed with AS with or without accompanying peripheral joint involvement were included.
Demographic (age, gender, duration of education, marital-job status, comorbidity, smoking) and clinical characteristics (duration of diagnosis, morning stiffness, drug use, peripheral joint—extra-articular involvement, sacroiliitis stages, physiotherapy history) of the patients were registered. ESR and C-Reactive Protein (CRP) levels were recorded.
Pain level was evaluated with a 10 cm scaled horizontal VAS [7]. Morning stiffness duration was reported in minutes. Bath Ankylosing Spondylitis Metrology Index (BASMI) [8], BASDAI) [9], BASFI [10], BDI [11], AS QoL [12] were used to evaluate spinal mobility, disease activity, function, mood, and quality of life, respectively.
Each patient diagnosed with AS in the Rheumatology outpatient clinic was advised to have a home-based exercise program according to the results of the 6-min walk test [13]. A program consisting of aerobics, range of motion, breathing, posture, balance and strengthening activities was instructed for 20–30 min, five days a week. These exercises were shown to the patients by the physiotherapist at their every two-month follow-up and they were advised to do them again.
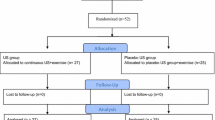
The patients were asked whether they performed the exercises and those who practiced them regularly for at least 1 year were included in the Exercise group (n = 24), and those who did not (n = 44) were included in the non-exercise group (n = 44).
Statistical method
Data were analyzed using the "Statistical Package for the Social Sciences" (SPSS 25.0 for Windows) software package. Kolmogorov Smirnov test was used to determine whether continuous variables had a normal distribution. In descriptive statistics, data were expressed as mean ± standard deviation (SD) and median (minimum–maximum) for continuous variables, and frequency and percentage (%) for nominal variables. The Mann–Whitney U test and the Independent Simple T test for age were used to look for statistically significant differences between groups for normal intact continuous variables (normal distribution). The significance of the difference for nominal variables was examined using χ2 and Fisher's exact test. Spearman correlation coefficient was used to measure the association between the evaluation parameters other than age data (Pearson correlation test). For significant correlations: univariate binary logistic regression analyzes were applied for independent nominal variables, with “exercise” as the dependent variable, and univariate simple linear regression analyzes for continuous variables. p < 0.05 values were considered statistically significant.
Results
Demographic and clinical characteristics of the patients were presented respectively in Tables 1 and 2. The mean age of the patients was 39.14 ± 12.15 years. The patient groups were homogeneously distributed in demographic and disease characteristics. When those who exercised regularly (Exercise group = 24) and those who did not (non-exercise group = 44) were compared, significant differences were obtained in terms of physiotherapy history (p = 0.033), ESR levels (p = 0.038), VAS (p = 0.001), BASDAI (p = 0.001), and BASFI (p = 0.022) results.
The relationship between the demographic and clinical characteristics of the patients according to exercise status was demonstrated in Table 3. Regular exercise was positively correlated with physiotherapy history (p = 0.023) and negatively correlated with VAS (p = 0.001) and BASDAI (p = 0.008). Regression analysis revealed that physiotherapy history increased regular exercise by 1.335 times. With an increase of 1 unit in VAS and BASDAI, regular exercise decreased by 0.087 and 0.116 units, respectively.
Discussion
In this study, which was conducted to determine whether AS patients regularly perform the recommended exercises and to evaluate the effect of regular exercise on pain, function, disease activity, emotional status and quality of life in these patients, it was determined that 35.3% of the patients had regular exercise habits. Home-based exercise programs have positive effects, particularly on pain and disease activity in AS.
Ankylosing spondylitis is a chronic inflammatory disease of unknown etiology that usually starts with inflammation in the sacroiliac joints in the early period and may spread to the axial spine as the disease progresses [14]. As a result of the reviews, there is a consensus that exercise is an important part of AS management [15]. It is essential to improve mobility, strength, cardiovascular health, function, and quality of life [16].
A review suggested that individual home exercise or a supervised exercise program is better than no exercise at all; supervised group physiotherapy showed more positive results than home exercises, and the combination of group physiotherapy and inpatient spa exercise therapy achieved more significant findings than group physiotherapy alone [15]. This study showed that regular exercise routines were positively affected by those with a history of physiotherapy. This shows the importance of exercising with a physiotherapist in the past in gaining exercise habits.
In a study evaluating kinesiophobia in AS, VAS was found to be proportional to kinesiophobia [17]. In this study, VAS values were found to be significantly higher in the non-exercise group, which reflects the positive effects of movement on pain.
A 12-month follow-up in one trial revealed significant improvements in chest expansion, BASDAI, cervical rotation, thoraco-lumbar rotation, and goniometric assessments of additional cervical motions in exercise group [18]. In a randomized controlled trial evaluating individuals with AS before and after a 6-week exercise program, significant improvements in BASDAI and BASFI were obtained in the exercise group compared to control group [19]. Altan et al. examined the effects of pilates on AS and noted that the pilates group made significant improvements in BASFI compared to the control group. In addition, at 24 weeks, the pilates group achieved much better results (BASFI and BASMI) than the other group [20]. Studies reviewed in a meta-analysis showed that overall, most had lower BASDAI and BASFI scores with exercise [21]. Another meta-analysis found that controlled exercise on BASFI, BASDAI, and BASMI resulted in significant reductions compared to programmed exercise at home [22]. Although we could not find a difference in terms of BASMI, BASDAI results were found to be lower in the exercise group.
Evaluating pulmonary function and exercise capacity in patients with AS showed that respiratory function and pulmonary muscle strength values were similar in smokers and non-smokers, but the physical function and social function categories of the quality-of-life questionnaire were found to be lower in smokers compared to non-smokers [23]. This study showed no difference between the two groups in terms of smoking and quality of life.
In one study, the BASFI score was correlated with smoking, exercise, morning stiffness, BASMI, and BASDAI. In regression analysis, BASDAI was found to be associated with the BASFI score, and AS QoL with morning stiffness, education status, smoking, exercise, BASDAI and BASFI. BASFI was found to have a substantial impact on AS QoL [24]. However, the conventional exercise program showed significant improvements when applied as a supervised or home exercise program, it was observed that these effects decreased in the long term and there was no difference between them at the 12th week [25]. Our study could not reveal a significant relationship between exercise and AS QoL or BASFI.
ESR was found to be significantly lower in the exercise group. This difference was not observed in CRP. This difference in ESR may also be affected by complete blood count parameters.
Strengths and limitations of the study
The small number of patients, the evaluation of regular exercise with the patient's statement, and the recommendation of exercise as a home program were the limitations of the study. Every patient is advised to exercise regularly during follow-ups, and we think this is an exceptional study in terms of how much the patient considers and follows our recommendations.
Conclusions
Our study showed that regular implementation of home-based exercise program in AS had positive effects especially on pain and disease activity. Therefore, regular exercise should be considered as one of the cornerstones of treatment in patients with AS, as it offers promising results. Patients should be educated in this area and encouraged to exercise by developing specific exercise regimens.
Availability of data and materials
The authors confirm that the data supporting the findings of this study are available within the article.
Abbreviations
- ACR:
-
American College of Rheumatology
- AS:
-
Ankylosing spondylitis
- BASDAI:
-
Bath ankylosing spondylitis disease activity index
- BASFI:
-
Bath ankylosing spondylitis functional index
- BASMI:
-
Bath ankylosing spondylitis metrology index
- BDI:
-
Beck depression inventory
- CRP:
-
C-reactive protein
- ESR:
-
Erythrocyte sedimentation rate
- QoL:
-
Quality of life
- VAS:
-
Visual analog scale
References
Wolf J, Fasching P (2010) Ankylosing spondylitis. Wien Med Wochenschr 160:211–214. https://doi.org/10.1007/s10354-010-0793-2
Weisman MH, Reveille JD, Heijde D (2006) Ankylosing Spondylitis and the Spondyloarthropathies. Mosby, Elsevier. Turkish Edition: Ozgocmen S (2008) Veri Medikal Yayincilik, Ankara.
Elbey B (2015) Ankilozan spondilitli hastalarda guncel tedavi yaklasimlari. Dicle Tip Derg 42:123–127. https://doi.org/10.5798/diclemedj.0921.2015.01.0546
Liang H, Zhang H, Ji H, Wang C (2015) Effects of home-based exercise intervention on health-related quality of life for patients with ankylosing spondylitis: a meta-analysis. Clin Rheumatol 34:1737–1744. https://doi.org/10.1007/s10067-015-2913-2
Dagfinrud H, Kvien TK, Hagen KB (2001) Physiotherapy interventions for ankylosing spondylitis. Cochrane Database Syst Rev. CD002822. https://doi.org/10.1002/14651858.CD002822. Update in: Cochrane Database Syst Rev. 2004;(4):CD002822
Aytekin E, Caglar NS, Ozgonenel L, Tutun S, Demiryontar DY, Demir SE (2012) Home-based exercise therapy in patients with ankylosing spondylitis: effects on pain, mobility, disease activity, quality of life, and respiratory functions. Clin Rheumatol 31:91–97. https://doi.org/10.1007/s10067-011-1791-5
Miller MD, Ferris DG (1993) Measurement of subjective phenomena in primary care research: the Visual Analogue Scale. Fam Pract Res J 13:15–24
Jenkinson TR, Mallorie PA, Whitelock HE, Kennedy LG, Garrett SL, Calin A (1994) Defining spinal mobility in ankylosing spondylitis AS The Bath AS Metrology Index. J Rheumatol 21(9):1694–8
Jenkinson TR, Mallorie PA, Whitelock HC, Kennedy LG, Garrett SL, Calin A (1994) A new approach to defining disease status in ankylosing spondylitis: the Bath Ankylosing Spondylitis Disease Activity Index. J Rheumatol 21:2286–2291
Calin A, Garrett S, Whitelock H, Kennedy LG, O’Hea J, Mallorie P et al (1994) A new approach to defining functional ability in ankylosing spondylitis: the development of the Bath Ankylosing Spondylitis Functional Index. J Rheumatol 21:2281–2285
Beck AT, Ward CH, Mendelson M, Mock J, Erbaugh J (1961) An inventory for measuring depression. Arch Gen Psychiatry 4:561–571. https://doi.org/10.1001/archpsyc.1961.01710120031004
Doward LC, Spoorenberg A, Cook SA, Whalley D, Helliwell PS, Kay LJ et al (2003) Development of the ASQoL: a quality of life instrument specific to ankylosing spondylitis. Ann Rheum Dis 62:20–26. https://doi.org/10.1136/ard.62.1.20
American Thoracic Society Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories (2002) ATS statement: guidelines for the six-minute walk test. Am J Respir Crit Care Med 166:111–117. https://doi.org/10.1164/ajrccm.166.1.at1102.Erratum.In:(2016)AmJRespirCritCareMed193:1185
van der Linden S, van der Heijde D (1998) Ankylosing spondylitis. Clinical features. Rheum Dis Clin North Am 24:663–676. https://doi.org/10.1016/s0889-857x(05)70036-3
Dagfinrud H, Kvien TK, Hagen KB (2008) Physiotherapy interventions for ankylosing spondylitis. Cochrane Database Syst Rev 2008:CD002822. https://doi.org/10.1002/14651858.CD002822.pub3
Farisogullari B, Karadag O (2020) Ankilozan spondilit tedavisi. J Turk Soc Rheumatol 12:32–45
Oskay D, Tuna Z, Duzgun I, Elbasan B, Yakut Y, Tufan A (2017) Relationship between kinesiophobia and pain, quality of life, functional status, disease activity, mobility, and depression in patients with ankylosing spondylitis. Turk J Med Sci 47:1340–1347. https://doi.org/10.3906/sag-1702-93
Masiero S, Poli P, Bonaldo L, Pigatto M, Ramonda R, Lubrano E et al (2014) Supervised training and home-based rehabilitation in patients with stabilized ankylosing spondylitis on TNF inhibitor treatment: a controlled clinical trial with a 12-month follow-up. Clin Rehabil 28:562–572. https://doi.org/10.1177/0269215513512214
Nolte K, van Rensburg DCJ, Fletcher L (2021) Effects of a 6-month exercise programme on disease activity, physical and functional parameters in patients with ankylosing spondylitis: Randomised controlled trial. S Afr J Physiother 77:1546. https://doi.org/10.4102/sajp.v77i1.1546
Altan L, Korkmaz N, Dizdar M, Yurtkuran M (2012) Effect of Pilates training on people with ankylosing spondylitis. Rheumatol Int 32:2093–2099. https://doi.org/10.1007/s00296-011-1932-9
Pécourneau V, Degboé Y, Barnetche T, Cantagrel A, Constantin A, Ruyssen-Witrand A (2018) Effectiveness of Exercise Programs in Ankylosing Spondylitis: A Meta-Analysis of Randomized Controlled Trials. Arch Phys Med Rehabil 99:383–389. https://doi.org/10.1016/j.apmr.2017.07.015
Liang H, Xu L, Tian X, Wang S, Liu X, Dai Y et al (2020) The comparative efficacy of supervised- versus home-based exercise programs in patients with ankylosing spondylitis: A meta-analysis. Medicine (Baltimore) 99:e19229. https://doi.org/10.1097/MD.0000000000019229
Akyol G, Ozalevli S, Ucan ES (2013) The relationship between pulmonary function and exercise capacity and quality of life in patients with ankylosing spondylitis. Tuberk Toraks 61:227–234. https://doi.org/10.5578/tt.4272
Gurer G, Tasci Bozbas G, Iyiyapici Unubol A, Tuncer T, Butun B (2017) Which Factors Affect the Functional Situation and Quality of Life in Patients with Ankylosing Spondylitis? Ankara Medical Journal 17:235–244
Atik T (2012) Ankilozan spondilitli hastalarda tedavi edici egzersizlerin hastalik aktivitesi, fonksiyonel durum ve yasam kalitesine etkileri. Dissertation, Uludag University, Faculty of Medicine, Bursa, Turkey. https://tez.yok.gov.tr/UlusalTezMerkezi/tezDetay.jsp?id=nnMHb11a5a2tqDSUetjIEg&no=VJi5Ls_EzvgmA4SK4qXUEg
Acknowledgements
None.
Code availability
N/A.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
YT, EUA and EG designed the study, contributed to study design, and wrote the first draft. YT and OZK contributed to data collection. EU contributed to data preparation and analysis. EUA and EG reviewed the final version of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study protocol received institutional review board approval (dated: 18.10.2021, Protocol no: 122/11) and all participants provided informed written consent in the format required by the clinical research ethics committee of University of Health Sciences, Diskapi Yildirim Beyazit Training and Research Hospital, Ankara, Turkey.
Consent for publication
Not applicable.
Competing interests
The authors declare no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Tombak, Y., Karaahmet, O.Z., Umay, E. et al. Home exercise is considered essential, but patient compliance remains a mystery. Egypt Rheumatol Rehabil 51, 24 (2024). https://doi.org/10.1186/s43166-024-00257-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43166-024-00257-6