
Abstract
This study directly compared the novel unexpected vection hypothesis and postural instability-based explanations of cybersickness in virtual reality (VR) using head-mounted displays (HMD) for the first time within a commercial VR game. A total of 40 participants (19 males and 21 females) played an HMD-VR game (Aircar) for up to 14 min, or until their first experience of cybersickness. Based on their self-reports, 24 of these participants were classified as being ‘sick’ during the experiment, with the remainder being classified as ‘well’. Consistent with the unexpected vection hypothesis, we found that: (1) ‘sick’ participants were significantly more likely to report unexpected vection (i.e., an experience of self-motion that was different to what they had been expecting), and (2) sickness severity increased (exponentially) with the strength of any unexpected (but not expected) vection. Our results also supported the predictions of postural instability theory, finding that the onset of cybersickness was typically preceded by an increase in participants’ postural instability. However, when both sway and vection measures were combined, only unexpected vection was found to significantly predict the occurrence of sickness. These findings highlight the importance of unusual vection experiences and postural instability in understanding cybersickness. However, they suggest that developers should be able to make use of expected experiences of vection to safely enhance HMD-VR.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
1 Introduction
In recent decades, head-mounted displays (HMD) have gained widespread acceptance and utility, with companies like Meta (formerly Facebook Reality Labs) providing their portable virtual reality (VR) systems as flagships for consumer entertainment, research, and industry applications. Regrettably, the problem of cybersickness (also known as simulator sickness, or VR sickness) persists with these HMDs, which continues to limit the widespread adoption of the technology. Furthermore, despite growing insights into the origins of this sickness, there has yet to be a universally accepted theory of cybersickness in HMD-VR (Lawson 2014; Palmisano et al. 2020). The two most widely cited causes of motion sickness are sensory conflict and postural instability (Reason and Brand 1975; Reason 1978; Riccio and Stoffregen 1991). In this paper on HMD-VR, we will examine the postural instability theory of motion sickness (Riccio and Stoffregen 1991), and further test our new sensory-conflict account of cybersickness during HMD-VR—the unexpected vection hypothesis (Teixeira et al. 2022).
1.1 The postural instability theory of motion sickness
According to this theory, motion sickness is likely to occur when an individual's mechanisms for maintaining postural stability are impaired or undermined (Riccio and Stoffregen 1991; Stoffregen and Smart 1998). The postural instability theory predicts that: (1) individuals who are naturally unstable will also be more susceptible to sickness in HMD-VR; (2) this sickness will be preceded by an increase in postural instability; and 3) symptoms will persist until their stability is restored (Risi and Palmisano 2019).
1.1.1 Empirical support for the postural instability theory
Consistent with the first prediction of the postural instability theory, many studies have found that a person’s spontaneous postural instability can predict their likelihood of experiencing motion sickness (Arcioni et al. 2019, Bonnet et al. 2006; Koslucher et al. 2015, 2016; Merhi et al. 2007; Munafo et al. 2017a, b; Risi and Palmisano 2019; Stoffregen and Smart 1998; Stoffregen et al. 2000, 2008, 2010, 2014; Teixeira and Palmisano 2021; Villard et al. 2008; Yokota et al. 2005). Although most of these studies were focused on the visually-induced motion sickness (VIMS)Footnote 1 induced by console video games, large moving rooms, and handheld devices, more recent studies have examined the cybersickness induced by HMD-VR. These latter studies found that differences in their participants’ spontaneous postural activity could be used to predict which of them would become sick (or remain well) during HMD-VR (e.g., based on forced-choice “yes/no” responses to the question “do you feel sick?”Arcioni et al. 2019; Munafo et al. 2017a, b; Risi and Palmisano 2019; Teixeira and Palmisano 2021). As predicted by the theory, the spatial magnitudes (e.g., the standard deviation of their centre of foot pressure [CoP]) and the temporal dynamicsFootnote 2 (e.g., DFA α) of their CoP fluctuations when standing were found to predict their sick/well status after HMD exposure. While the postural instability theory is focussed on identifying who will become sick (or remain well), Arcioni et al. (2019) also found a significant positive relationship between their participants’ spontaneous postural sway and the severity of their subsequent sickness (using the Fast Motion Sickness scale). That is, participants who were more posturally unstable before entering HMD-VR appeared to become sicker during the VR exposure. However, other HMD-VR studies have failed to find relationships between sway and cybersickness (e.g., Dennison and D'Zmura 2017 who assessed cybersickness using the Simulator Sickness Questionnaire—the SSQ)—possibly because they were focussed exclusively on examining the spatial magnitude of their participants’ sway (unlike Arcioni et al. 2019, Dennison and D’Zmura did not examine the temporal dynamics of their participants’ swayFootnote 3).
1.1.2 Predictions of the postural instability theory which require further testing
To date, most of the studies investigating the role of postural instability in cybersickness have focussed on their participants’ sway prior to HMD-VR exposure (Arcioni et al. 2019; Chardonnet et al. 2017; Clifton and Palmisano 2019a, 2019b; Cobb 1999; Cobb and Nichols 1998; Munafo et al. 2017a, b; Nishiike et al. 2013; Palmisano et al. 2018a, b, c; Risi and Palmisano 2019). Only a few studies have measured their postural sway during the HMD-VR exposure (Akiduki et al. 2003; Dennison and D'Zmura 2017; Merhi et al. 2007) – which is required to test the second and third predictions of the postural instability theory. The results of these other studies have thus far been inconclusive. However, as noted recently by Litleskare (2021), these studies failed to include baseline sway measurements, making it difficult to determine whether the VR exposure was responsible for any observed postural instability (and subsequent sickness). Further, these studies typically only examined spatial magnitude (as opposed to temporal dynamics) based postural measures. In order to fully evaluate the impact of postural stability on the experience of cybersickness, it is essential to assess the participant’s sway both: (1) before and during exposure to HMD-VR; and (2) in terms of its temporal dynamics, as well as its spatial magnitude.
1.2 Vection conflict and motion sickness
Sensory conflict is the most widely cited explanation of motion sickness, including cybersickness (Keshavarz et al. 2014). According to its proponents, multisensory motion stimulation can trigger sickness when it leads to sensory conflict or expectancy violations (see Reason and Brand 1975; Reason 1978). Motion sickness could conceivably be caused by either intersensory (e.g., between visual and inner ear-based motion stimulation) or intrasensory (e.g., between the otolith organs and the semicircular canals) conflicts (Reason and Brand 1975). However, according to Reason’s (1978) sensory conflict theory (the sensory rearrangement theory), expectancy violations are the major trigger of motion sickness. It predicts that individuals will be more likely to become sick when they experience a neural mismatch (i.e., a difference between their currently sensed motion and the expected pattern of motion stimulation based on their past experiences). The theory can therefore be used to explain why passengers in automobiles tend to be more susceptible to motion sickness than their drivers (because the drivers, who are responsible for generating the motion, should have a better sense of what to expect in terms of their future motion stimulation; By comparison, their passengers should be more prone to experience unexpected or unpredictable motion [Teixeira et al. 2022]). While they are widely cited, most sensory conflict theories (including sensory rearrangement theory) have been criticised for being difficult to test (Stoffregen and Riccio 1991). However, one version of sensory conflict theory—the vection conflict theory—should produce readily testable hypotheses (this was inspired by Hettinger et al.’s 1990 findings—see Palmisano et al. 2020 for a discussion). This theory, and its empirical support are described below.
1.2.1 Effects of sensory conflicts due to vection
The term vection is commonly used to describe illusions of self-motion (Palmisano et al. 2015). According to some theorists, visual motion should only induce cybersickness when the participant first experiences an illusion of self-motion (e.g., Hettinger et al. 1990; Kennedy et al. 1990; McCauley and Sharkey 1992). That is, the experience of vection should be a necessary prerequisite for cybersickness. Support for this theory primarily comes from a flight simulation study conducted by Hettinger et al. (1990). This study obtained subjective reports of vection and VIMS from fourteen participants. The researchers found that eight out of the nine participants who reported VIMS also experienced vection. Conversely, among the five participants who did not report vection, only one experienced VIMS. They therefore concluded that "visual displays that produce vection are more likely to produce simulator sickness" (p. 179). Consistent with this, Smart et al. (2002) subsequently found that when they moved a furnished room around twelve stationary participants: (1) eleven of them reported vection, with three of them also reporting VIMS; and (2) the last participant, who did not experience any vection, remained well throughout the simulation. However, as noted by Keshavarz et al. (2015), based on the numbers involved in these studies, support for vection conflict causing cybersickness is far from conclusive.
1.2.2 Is there a relationship between vection strength and cybersickness during HMD-VR?
While Hettinger et al. (1990) did not explicitly propose a scaling relationship between vection strength and sickness severity, many VIMS studies have explored this possibility. While several reported positive linear relationships between vection strength and VIMS (e.g., Hettinger et al. 1990; Flanagan et al. 2002; Smart et al. 2002; Bonato et al. 2004, 2005, 2008; Diels et al. 2007; Palmisano et al. 2007; Nooij et al. 2017, 2018; Clifton and Palmisano 2019b; Risi and Palmisano 2019), others have reported either non-significant or negative linear relationships between them (Webb and Griffin 2002, 2003; Lawson 2005; Bonato et al. 2008; Ji et al. 2009; Chen et al. 2011; Golding et al. 2012; Keshavarz et al. 2014; Riecke and Jordan 2015; Gavgani et al. 2017; Palmisano et al. 2018a, b, c; Palmisano and Riecke 2018a, b; Kuiper et al. 2019 − see Keshavarz et al. 2015 for a review). To date, only a few studies have examined the possible relationships between vection and cybersickness in HMD-VR. In the first of these studies, Palmisano et al. (2017) investigated the effects of experimentally induced sensory conflict on both cybersickness severity and vection strength. When HMD users in this study made continuous left–right head movements, their virtual environment was updated either ecologically or non-ecologically based on their tracked movements. The authors found a negative relationship between vection strength and cybersickness severity under maximum conflict conditions. In contrast, Risi and Palmisano (2019) reported that stronger vection was associated with increased cybersickness when they examined active and passive interactions with HMD-VR. Teixeira and Palmisano (2021), on the other hand, failed to find a significant association between vection strength and cybersickness severity when they investigated the impact of dynamic field-of-view restriction on cybersickness during HMD gameplay. Although experimental conditions and activities differed across these three studies, their inconsistent findings clearly demonstrate that cybersickness severity does not always increase with the strength of vection.
1.2.3 Are other characteristics of vection important for understanding cybersickness?
To date, researchers have only examined the influence of vection strength on cybersickness. This ignores other potentially important differences in the experiences of vection across these studies, which could explain the inconsistent (sometimes null) relationships observed between vection and cybersickness (see Teixeira et al. 2022 for a discussion). For example, there were marked differences in the types, speeds and directions of self-motion being simulated, as well as in the control and other movements being made by participants in these studies (e.g., Clifton and Palmisano 2019a, 2019b; Palmisano et al. 2017; Risi and Palmisano 2019; Teixeira and Palmisano 2021). Crucially, participants’ expectations about the nature and the characteristics of their vection were also neglected. When illusory self-motions are expected (e.g., based on priming/cognitions), participants tend to have stronger experiences of vection (Andersen and Braunstein 1985; Palmisano and Chan 2004; Palmisano and Riecke 2018a, b). In HMD-VR, illusions of self-motion are common (i.e., expected), due to the user’s stereoscopic first-person view, as well as the large areas of visual motion stimulation these headsets provide (see Palmisano 1996, 2002; Palmisano and Riecke 2018a, b; Palmisano et al. 2015, 2016, 2019). However, while HMD users often expect vection induction, the specific direction, speed, or intensity of this vection can still be unexpected. For example, their sensed self-motion might be different to what they had anticipated based on their control motions—resulting in discomfort and disorientation. Given that motion sickness is thought to be triggered by discrepancies between expected and sensed self-motion, it follows that such experiences (referred to here as ‘unexpected vection’) might be particularly provocative for cybersickness (Bonato et al. 2009). Despite this, there has only been one study to date that has explored the effects of vection type (expected/unexpected) on HMD-induced cybersickness.
1.2.4 The unexpected vection hypothesis
Recently, Teixeira et al (2022) proposed a new theory of cybersickness, which was inspired by the predictions of both sensory rearrangement theory and vection conflict (Reason 1978; Hettinger et al. 1990, 1992). According to this hypothesis, only one specific type of vection—unexpected vectionFootnote 4—should provoke cybersickness. Specifically, unexpected vection was proposed to be a necessary prerequisite for cybersickness during HMD-VR. By contrast, vection that is expected by the HMD user (based on their past, recent and/or current experiences) should not be problematic.Footnote 5 Unlike the postural instability theory, this unexpected vection hypothesis makes predictions about both the onset and the severity of cybersickness. It predicts that: (1) HMD users should only become sick after they experience unexpected self-motion (such as, a loss of control of their simulation causing experienced vection to differ from what they had anticipated); (2) cybersickness severity should increase with the strength of this unexpected vection; and (3) sickness severity should be largely independent of vection strength when the simulated self-motion is expected. Thus far, the hypothesis has only been examined by one HMD-VR study. In that study, Teixeira et al. (2022) obtained subjective self-report measures of both vection strength and type from participants while they played a commercially available HMD-VR game (Mission: ISS). Consistent with the hypothesis, they found that participants who became sick were significantly more likely to experience unexpected vection (typically a perceived loss of controlFootnote 6) than those who remained well. Importantly, vection strength and vection type (unexpected/expected) predictors were able to explain the occurrence of cybersickness with an accuracy of 83.3%. While vection strength ratings were not found to differ significantly for ‘sick’ and ‘well’ participants, relationships between vection strength and cybersickness were only significant for the ‘sick’ group (who reported experiencing unexpected – not expected – vection). These preliminary findings suggest that: 1) compelling vection alone is not sufficient to induce cybersickness; and 2) vection must be unexpected to produce such symptoms.
1.3 The Current Study
This study examined whether our participants’ postural activity, experiences of vection type, and vection strength could be used to predict their experiences of cybersickness during HMD-VR. Unlike our earlier exploratory study (Teixeira et al. 2022), where participants remained in VR until their symptoms became severe, participants in the current study were instructed to drop out at the very first signs of cybersickness. This allowed us to examine their experiences of vection and postural stability at the onset of this sickness. Additionally, while our previous study only exposed participants to simulated self-motion under microgravity conditions (in the international space station), the current study instead had participants pilot a hover car through a built-up futuristic cityscape. This change of game played should allow us to determine whether effects of unexpected vection on cybersickness generalise across different VR simulations. Based on the findings of Teixeira et al. (2022), we predicted that participants who became sick in our new study would be more likely to report unexpected vection (compared to those who remained well). For these sick participants, we predicted that there would be a significant positive relationship between the strength of their (unexpected) vection and the severity of their cybersickness. Furthermore, in line with the postural instability theory, our naturally unstable participants were expected to be the most susceptible to cybersickness when standing during HMD-VR exposure. We further predicted that the onset of their cybersickness would be preceded by an additional increase in their postural instability (compared to their own sway before experiencing cybersickness, and prior to HMD-VR exposure).
2 METHOD
2.1 Participants
The study examined 40 participants (19 males and 21 females; Age = 23.9 years ± 3.3 years) recruited from the general population. They all had normal or corrected-to-normal vision and no self-reported visual, vestibular, or neurological impairments. All reported feeling well at the start of the experiment. The study was approved in advance by the UOW Ethics Committee, and each participant provided informed written consent prior to participating in the study.
2.2 Materials
2.2.1 Hardware and software
Exposure to the virtual environment was delivered via an Oculus Rift S HMD, and two Oculus Touch (hand) controllers. The HMD had a resolution of 1280 × 1440 pixels for each eye and a refresh rate of 80 Hz via Fast-Switch LCD technology. The virtual environment was generated by a Microsoft Windows 10 Dell Optiplex 7090 computer, which contained a Nvidia GeForce RTX3070 graphics card with the latest stable driver software installed and an Intel 11th generation CPU. The HMD-VR game software used in this study was “Aircar” (https://www.oculus.com/experiences/rift/1204731822978255/). This program was chosen for the study after pilot tests confirmed that it was provocative for sickness under normal gameplay conditions ‒ which we hypothesised might have been due to its (somewhat counterintuitive) primary method of 3-dimensional locomotion (note: control of the vehicle’s movements was often reported to have unexpected/surprising consequences). During the game, participants drove their aircar along the pre-selected route (pictured in Fig. 1) through a high-rise, futuristic cityscape, guided verbally by the experimenter. They actively controlled: 1) the roll and pitch movements of their aircar with the thumb stick of their right-hand controller; and 2) the yaw and direct vertical translation movements with the joystick on their left-hand controller. Acceleration and deceleration of the aircar were controlled using the trigger buttons on the right- and left-hand remotes respectively. These controls were explained and demonstrated to the participant before the experiment began.

Bird’s-eye view of the guided route in Aircar over the city’s various islands. These islands were densely packed with buildings of various heights. The participant’s task was to fly towards the landing pads on these islands and buildings in a specific order. Landing pads (LP) 1–8 are marked in order
2.2.2 Postural Measures
Before commencing the experiment, participant’s foot size, width, and arch lengths were measured using a Brannock Device. Their spontaneous postural sway (eyes-open) was then measured before the VR exposure trial. While standing in a quiet stance, a Bertec balance plate (http://bertec.com/products/balance-plates.html) recorded spontaneous fluctuations in their anterior/posterior (A/P) and medio/lateral (M/L) centre of foot pressure (CoP) for two 60 s periods (sampled at 500 Hz). This balance plate was also used to measure their standing postural sway while they were playing the HMD-VR game. For both pre-exposure and during-exposure recordings: 1) the standard deviations of the participant’s CoP data along their A/P and M/L axes (i.e., STDEV CoPA/P and STDEV CoPM/L) were used to estimate the spatial magnitudes of their sway; and 2) detrended fluctuation analyses (DFA) were also conducted on these CoPA/P and CoPM/L data to investigate how their postural activity evolved over time [The scaling exponents of these DFAs (i.e., DFA αA/P and DFA αM/L) provided indexes of the long-range auto correlations in these CoP data]. We also examined how our participants’ postural sway changed across the HMD-VR exposure, by comparing the spatial magnitudes and temporal dynamics of their sway at the start and the end of their gameplay. Specifically, we calculated standard deviation and DFA α difference scores for the CoP A/P and M/L data obtained in the first and last 30 s of their exposure.
2.2.3 Cybersickness severity and symptom profiling
At the end of their HMD-VR exposure, participants were first asked whether they felt sick or well (their response to this question was used to classify them into ‘sick’ and ‘well’ groups). Before and after this HMD-VR exposure, their nausea, disorientation, and oculomotor symptoms were also assessed using Kennedy et al.’s (1993) Simulator Sickness Questionnaire (SSQ). Based on Stanney et al. (2014), it was assumed that SSQ scores greater than 20.1 represented ‘functionally significant sickness’ during VR (see Lawson and Stanney 2021).
2.2.4 Vection type and strength
To be sure that participants could successfully distinguish between what expected/unexpected vection was, we carefully explained the concept of vection to them (both before and after their VR exposure).
Vection was described to participants as the sensation of self-motion while being physically stationary, typically induced by visual stimuli. We used layman-friendly terms and examples, such the train illusion (i.e., the illusory sensation of moving while standing still on a stationary train, when the train on the next track departs the station) to illustrate the concept. For a more relatable VR example, we showed participants footage of the game aircar, and described the vection that they might experience in this situation as the feeling that they were physically being moved with the virtual aircar through the digital cityscape (even though they were in reality seated and motionless).
Once we confirmed participants grasped the concept of vection as it relates to HMD-VR, we further distinguished between expected and unexpected vection. Expected vection was explained as the sensation of self-motion that aligns with the visual cues and anticipations of the participant. For instance, feeling that you are moving forward in the virtual environment when you press the ‘forward’ control button. Unexpected vection, on the other hand, was explained as a sensation of movement that does not correspond with the visual cues or the participant's anticipations. We used examples like feeling as though you are moving backward when the visual scene is moving forward, experiencing a sudden acceleration when expecting to move slowly, or feeling a rotational movement when only linear motion was anticipated. While we explained there could be other unexpected vection experiences in addition to these specific examples, they helped participants recognize and distinguish instances of vection that deviate from their expected interactions within the VR experience (some even offered their own examples to confirm their understanding).
We obtained an overall vection strength rating at the end of the trial (from 0 = “no vection” to 10 = “strong vection”). At the end of their exposure to HMD-VR, participants were also quizzed about the nature of their experience of vection. If they had reported being ‘sick’, they were asked:
-
1.
‘Did your feelings of being in control of your perceived self-movement change prior to sickness?’
-
2.
‘Was your perceived self-movement more or less expected/anticipated prior to sickness?’
-
3.
‘Is there anything else you wanted to add? Do you have any insights about why you think you became sick?’
Alternatively, if they reported remaining ‘well’ throughout the HMD-VR session, they were instead asked:
-
1.
‘Did you feel in control of your perceived self-movement during the simulation?’
-
2.
‘Was your perceived self-movement expected/anticipated during the simulation?’
-
3.
‘Is there anything else you wanted to add?’
Participants’ responses about their perceived body movement were double-checked during debriefing at the end of the experiment. This was to see whether they were referring to whole body self-motions relative to the virtual environment (rather than the motions of their various limbs or their postural sway while standing in place during HMD-VR). It was also to confirm when any experiences of unexpected vection had occurred. As our participants’ primary task was reporting occurrences of unexpected vection, this served to verify those occurrences, and they were also encouraged to discuss any interesting/unusual experiences.
2.3 Procedure
Participants first completed a demographics, VR and Gaming History sheet.Footnote 7 They were next given an information sheet that described the experiment, which they were asked to sign to indicate their consent. Participants’ height and foot size were then recorded, before they were instructed to step on a Bertec balance plate to assess their spontaneous postural instability (based on subsequent analyses of recorded fluctuations in their CoP). Their spontaneous postural activity was measured (eyes-opened, looking at a piece of paper attached to the laboratory wall 1 m in front of them) for two 60 s periods. Then, directly before their exposure to HMD-VR, they completed the pre-exposure sections of the SSQ to provide a baseline measure of their current sickness levels. Participants were then instructed to step back onto the balance plate, don the Oculus Rift S HMD and were given a quick tutorial by the experimenter on the game’s controls. They were then verbally guided through a pre-selected city travel route shown in Fig. 1Footnote 8 for either 14 min, or until they indicated any signs of sickness or discomfort, followed by a confirmatory ‘yes’ to the question: ‘Do you feel sick?’. During the VR gameplay, CoP data were constantly recorded as participants travelled along the route specified until they experienced cybersickness [i.e., landing at each of the 8 island/building checkpoints (landing pads LP 1–8) in order]. Directly after leaving HMD-VR, their post-exposure sickness status (sick or well), sickness severity and symptomology were assessed (using an additional “Yes/No” response to the question “do you feel sick?” and responses to the 16 items on the post-exposure SSQ). Participants also provided an overall (0–10) rating of the vection strength for the trial. Finally, they verbally responded to our three exploratory questions about the nature of their experiences of vection during HMD-VR.
3 Results
3.1 Examining cybersickness symptomology and confirming sick/well groupings
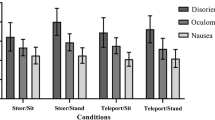
Our 40 participants were classified as either being ‘sick’ or ‘well’ based on their answers to the question: “Do you feel sick?”. The 24 ‘sick’ participants responded “yes” to this question, while the remaining 16 ‘well’ participants responded “no”. To check on the success of this classification, we conducted a Yuen’s trimmed means t-test, bootstrapped at 1000 samples to assess the difference between ‘sick’ and ‘well’ groups’ post-exposure total SSQ (SSQ-T) scores.‘Sick’ participants were found to have significantly higher post SSQ-T scores (M = 43, SD = 25.7) than ‘well’ participants (M = 11.2, SD = 9.75, t(20.9) = 4.46, p = < 0.001, ξ = 0.89). Based on Stanney et al. (2014), the SSQ-T scores of our ‘sick’ participants corresponded to ‘high’ or ‘extreme’ levels of sickness (please see Table 31.3 in that book chapter). As expected, our ‘well’ participants did not reach their identified threshold for functionally significant sickness (i.e., SSQ-T > 20.1). The SSQ was also used to assess our participants’ post-exposure nausea (SSQ-N), disorientation (SSQ-D) and oculomotor (SSQ-O) symptoms (see Fig. 2). For those classified as 'well', scores were reported as: SSQ-D (M = 9.57, SD = 12.2), SSQ-N (M = 14.9, SD = 13.9), and SSQ-O (M = 9, SD = 10.1). In contrast, participants identified as 'sick' recorded higher scores: SSQ-D (M = 52.2, SD = 36.6), SSQ-N (M = 40.5, SD = 13.9), and SSQ-O (M = 27.5, SD = 19.6). As expected for HMD-VR, overall post-exposure scores were found to be higher on average for the SSQ-D (M = 35.1, SD = 35.9) than for the SSQ-N (M = 30.3, SD = 25.3) and the SSQ-O (M = 20.1, SD = 18.7).

Post-exposure SSQ-D (disorientation), SSQ-N (nausea), and SSQ-O (oculomotor) sub-scores for Sick and Well Participants
3.2 Analysis of dropout times for sick participants
Dropout times were analysed for those participants who reported experiencing sickness during the session (N = 24). The mean dropout time was approximately 4 min and 38 s, with a standard deviation of approximately 2 min and 39 s. The median dropout occurred after approximately 4 min and 13 s. Dropout times ranged from as early as 35 s to as late as 10 min and 36 s. Additionally, the interquartile range (IQR) indicated that the central 50% of participants discontinued their session within 3 min and 27 s. As sickness onset was the sole criterion for dropout, no well participants were considered in this analysis (Fig. 3).

Occurrence of dropout times for sick participants
3.3 Predicting the occurrence of cybersickness based on vection type and strength
To investigate our hypothesis that ‘sick’ participants in the study would be more likely to report unexpected vection (compared to those who remain well) we used the following logistic model (jamovi 2.3, GAMLj package), where our participants’ Sick/Well group membership was predicted by the type and strength of the vection that they experienced (plus their interaction) as fixed effects:
We found a significant main effect of vection type (z = -1.98, p = 0.047, estimate = -5.879) on Sick/Well group membership, indicating that participants were more likely to be ‘sick’ when their vection was unexpected (rather than expected). This effect of unexpected vection on Sick/Well group membership appeared to be independent of the strength of the vection experienced.
3.4 Predicting the occurrence of cybersickness based on postural sway
To examine the possible associations between postural instability and cybersickness occurrence, we performed t-tests on the spatial magnitude and temporal dynamics-based CoP measures obtained for the ‘sick’ and ‘well’ groups. Separate t-tests were performed on the anterior–posterior (A/P) and medial–lateral (M/L) CoP measures obtained from these two groups: (1) before their HMD-VR exposure (i.e., eyes open spontaneous postural sway in an otherwise static real-world environment); and (2) during their HMD-VR exposure (i.e., the postural sway generated by the interactive simulation).
3.4.1 Pre-exposure (spontaneous) postural activity in ‘sick’ and ‘well’ groups
To examine whether more naturally unstable individuals would be more susceptible to sickness in HMD-VR (compared to those who remain well) we conducted four independent samples t-tests (on the STDEV COPA/P, STDEV COPM/L, DFA αA/P and DFA αM/L data). Each of these tests examined whether our 24 ‘sick’ and 16 ‘well’ participants differed in terms of their eyes-open spontaneous postural activity before exposure. Participants classified as ‘sick’ (M = 0.00186, SD = 0.000656) were found to produce significantly smaller eyes-opened STDEV COPM/L values than participants classified as ‘well’ (M = 0.00260, SD = 0.00134) before exposure, t(38) = -2.327, p = 0.025, two-tailed (see Table 1). However, this finding did not remain significant after Bonferroni correction was applied for four comparisons (i.e., with a Bonferroni-corrected pcritical = 0.0125).
3.4.2 Changes in the postural sway for ‘sick’ and ‘well’ groups during exposure
To examine whether cybersickness was preceded by an increase in postural instability, we conducted separate paired sample t-tests for our ‘sick’ and ‘well’ participants to compare their postural activity in the initial and final stages of the HMD exposure (i.e., the first, and last 30 s of their VR exposure). For ‘sick’ participants: 1) STDEV CoPA/P were significantly larger in the final moments of exposure (M = 0.00988 SD = 0.00330) compared to the beginning of the exposure (M = 0.00699, SD = 0.00332) [t(23) = 4.265, p < 0.001, two-tailed]; 2) STDEV COPM/L was also significantly larger in the final moments of exposure (M = 0.00703, SD = 0.00878) compared to the beginning of the exposure (M = 0.00382, SD = 0.00427) [t(23) = 2.958, p = 0.007, two-tailed]; 3) DFA α was similar across both times in the exposure (see Table 2). While ‘well’ participants also had larger STDEV CoPA/P in the final moments of exposure (M = 0.00805 SD = 0.00311) compared to the beginning of the exposure (M = 0.00622, SD = 0.00187), this effect did not remain significant after Bonferroni correction was applied for four comparisons (see Table 3).
3.5 Predicting the occurrence of cybersickness based on both vection and postural sway
Next, we investigated whether vection and sway-based measures contributed significantly to predicting the occurrence of cybersickness when they were both combined into a single model. We used the following logistic model (jamovi 2.3, GAMLj package), where participants’ Sick/Well group memberships were predicted by the changes in the spatial magnitude and temporal dynamics of their sway (by calculating standard deviation and DFA α change scores based on the differences in the first and last 30 s of the exposure) as well as the type and strength of the vection they experienced (plus their interaction) as fixed effects:
We found a significant main effect of vection type (z = − 2.0623, p = 0.039, estimate = − 5.964) on Sick/Well group membership, again indicating participants were more likely to be sick when vection was unexpected, rather than expected. No other significant main effects were found.
3.6 Predicting the severity of cybersickness based on vection
The above analyses all focussed on the occurrence of cybersickness (whether someone was classified as ‘sick’ instead of ‘well’). We next examined whether the severity of cybersickness could be predicted by our participants’ experience of vection. As with Teixeira et al. (2022), we used a generalised linear model (Poisson distribution) to test our hypothesis that there would be a positive relationship between vection strength and cybersickness severity for our participants who experienced unexpected types of vection. Cybersickness severity (as measured by the post-exposure SSQ-T) was modelled in terms of the vection strength (i.e., reported vection strength prior to dropout), vection type (whether it was expected/unexpected) and their interaction, as fixed effects:
As illustrated in Fig. 4, this model revealed a significant interaction between vection strength and vection type, z = 4.301, p < 0.001, estimate = 0.1085. Thus, the main effects of vection type and vection strength on SSQ-T ratings were not investigated further. The simple effects of vection strength, vection type, and their effect sizes, confirmed a positive relationship between vection strength and cybersickness severity for those who experienced unexpected vection (z = 6.947, p < 0.001, estimate = 0.1197), but not for those who only experienced expected vection (z = 0.605, p = 0.545).

Modelled non-linear relationships between vection strength and cybersickness severity (post SSQ-T) as a function of vection type (unexpected/expected). Shaded areas represent standard error
3.7 Predicting the severity of cybersickness based on postural sway
We also used a generalised linear model (Poisson distribution) to explore whether there might be scaling relationships between our spatial magnitude and temporal dynamics based postural sway change measures and cybersickness severity (using jamovi 2.3, GAMLj package). Cybersickness Severity (post-SSQ-T) was modelled in terms of late-early changes in our spatial magnitude and temporal dynamics sway measures (i.e., last 30 s – first 30 s STDEV CoPA/P, STDEV CoPM/L, DFA αA/P and DFA αM/L):
As shown in Fig. 5, we found significant negative main effects of ΔDFA αA/P (z = − 3.43, p < 0.001, estimate = − 1.02) and ΔDFA αM/L (z = − 4.20, p < 0.001, estimate = − 1.07) on sickness severity, indicating that decreases in late-early DFA α values were associated with increases in SSQ-T scores. We also found positive main effects of ΔSTDEV CoPA/P (z = 6.12, p < 0.001, estimate = 54.76) and ΔSTDEV CoPM/L (z = 3.34, p < 0.001, estimate = 17.68) on sickness severity, indicating increases in late-early standard deviations of the CoP were associated with increases in SSQ-T scores.

Modelled non-linear (exponential) relationships between temporal dynamics (late-early DFA αM/L or DFA αA/P)/spatial magnitude (late-early STDEV CoPM/L or STDEV CoPA/P) measures and cybersickness severity (post SSQ-T). Shaded areas represent standard error
3.8 Predicting the severity of cybersickness based on both vection and postural sway
Finally, we investigated whether vection and sway-based measures both contributed significantly to predicting the severity of cybersickness when they were combined into a single model. We used a generalised linear model (Poisson distribution—jamovi 2.3, GAMLj package). Cybersickness Severity (post SSQ-T) was modelled in terms of the late-early changes in our spatial magnitude and temporal dynamics-based sway measures, as well as vection type, vection strength and their interaction, as fixed effects:
The main effect of ΔSTDEV CoPM/L was significant for sickness severity (z = 4.551, p < 0.001, estimate = 28.1941), with SSQ-T scores increasing with the size of the late-early change in STDEV CoPM/L (see Fig. 6 Left). The main effect of ΔDFA αM/L was also significant for sickness severity (z = − 2.390, p = 0.017, estimate = − 0.6652), with SSQ-T scores decreasing as late-early changes in these α values increased (see Fig. 6 Left). As hypothesised, there was a significant positive relationship between vection strength and cybersickness severity for those who experienced unexpected vection (z = 5.77, p < 0.001, estimate = 0.1131), but not for those who only experienced expected vection (z = 1.77, p = 0.076 (see Fig. 7)).

Modelled non-linear (exponential) relationships between temporal dynamics (late-early DFA αM/L)/spatial magnitude (late-early STDEV CoPM/L) measures and cybersickness severity (post SSQ-T). Shaded areas represent standard error

Modelled non-linear (exponential) relationships between vection strength (overall vection) and cybersickness severity (post SSQ-T) as a function of vection type (unexpected/expected) for the “combined vection and changes in sway model”. Shaded areas represent standard error
4 Discussion
This HMD-VR study tested the predictions of both the unexpected vection hypothesis and the postural instability theory. Below we review the empirical support for each theory—in terms of their ability to predict: (1) who would become sick (or remain well); and (2) the severity of that sickness. We also discuss some additional exploratory analyses which examined how well models that combined the predictors from both theories (i.e., both vection type and strength, as well as postural sway-based measures) accounted for the current sickness findings.
4.1 Can unexpected vection predict occurrence and severity of cybersickness?
Vection is a common experience during HMD-VR that can enhance feelings of presence and immersion in virtual environments (Teixeira et al. 2022). Advocates of vection conflict theories often assume that: (1) any type of vection can cause cybersickness or: (2) there is a general scaling relationship between vection strength and cybersickness severity—despite evidence to the contrary in Hettinger et al.’s (1991) original study, and the fact that they never explicitly claimed the latter relationship. Recently, it has been argued that only some types of vection should trigger cybersickness (Teixeira et al. 2022). According to this unexpected vection hypothesis: (1) participants should only become sick after they experience unexpected (but not expected) vection; and 2) the severity of their sickness should only increase with the strength of unexpected (not expected) vection.
Consistent with the first prediction of the unexpected vection hypothesis and the recent findings of Teixeira et al. (2022), we found that reported experiences of unexpected vection in the current study were very strongly associated with participants becoming sick. Specifically, 79% of our ‘sick’ participants reported experiencing unexpected vection, compared to only 6% of our ‘well’ participants. When vection type (expected/unexpected) and strength (0–10) were both used to predict the sick/well group membership of our participants, only vection type was a significant predictor. That is, participants were found to be significantly more likely to become sick after experiencing unexpected vection. The likelihood of unexpected vection triggering cybersickness also appeared to be largely independent of the strength of this vection. However, while these findings generally supported the first prediction of the unexpected vection hypothesis, it did appear possible (on occasion) to experience sickness without experiencing unexpected vection.
Based on our unexpected vection hypothesis, we also predicted that cybersickness severity would increase with the strength of unexpected (but not expected) experiences of vection. We found a significant positive overall relationship between vection strength and sickness severity in the current study. As with Teixeira et al. (2022), the best model fit for this relationship appeared to be non-linear/exponential in nature. Critically, we found that this relationship was being driven only by unexpected vection. That is, supporting the second prediction of the unexpected vection hypothesis, the relationship between vection strength and sickness severity was only found to be significant for participants who experienced unexpected vection (i.e., prior to sickness onset).
Taken together, these results clearly demonstrate the important roles that unexpected vection can play in cybersickness. As predicted, experiences of unexpected vection significantly increased the likelihood of HMD users becoming sick (relative to experiences of expected vection). While the strength of the unexpected vection did not appear to alter the likelihood of participants becoming sick (i.e., weak and strong unexpected vection appear to be equally provocative in terms of triggering this sickness), it did appear to significantly affect the subsequent severity of any symptoms induced—with stronger experiences of unexpected vection tending to result in more severe experiences of cybersickness.
The current results confirm our recent findings that only certain types of vection are provocative of cybersickness (Teixeira et al. 2022). They also may explain the mixed findings of past studies which looked for general relationships between vection and cybersickness (i.e., without considering vection type—Palmisano et al. 2017; Risi and Palmisano 2019; Teixeira et al. 2021). Our results instead confirm that unexpected vection is particularly provocative of cybersickness, even at the very onset of these symptoms (whereas expected vection is not). These past studies also generally looked for linear relationships between vection strength and sickness severity. However, like Teixeira et al. (2022), our results suggested that the positive monotonic relationships between vection strength and cybersickness severity were best described by non-linear/exponential model fits. Taken together, our results again emphasize the importance of understanding the complexity between vection strength, type, and individual susceptibility in predicting cybersickness severity in HMD-VR.
4.2 Does postural instability theory predict cybersickness occurrence/severity?
We also investigated several predictions of the postural instability theory. The first of these predictions was that participants who were more naturally unstable would be more prone to experiencing sickness when exposed to HMD-VR. Contrary to this prediction, we did not find significant differences in the (eyes open) spontaneous standing postural activity of people who later became sick versus, those who remained well (either in terms of the spatial magnitudes, or the temporal dynamics, of their sway). We next examined its prediction that experiences of cybersickness during simulation would be preceded by a decrease in the HMD user's postural stability. To test this prediction, we: (1) estimated the spatial magnitude and temporal dynamics of our participants’ standing sway in VR during the first, and the last, 30 s of their exposure; and (2) then compared (late-early) changes in these sway measures for our ‘sick’ and ‘well’ groups. Consistent with the postural instability theory, the standard deviations of their sway (i.e., STDEV CoPM/L and STDEV CoPA/P) were significantly larger in the last 30 s (compared to the first 30 s) of the HMD-VR exposure, for ‘sick’, but not ‘well’, participants.
We further explored possible scaling relationships between our postural sway measures and cybersickness severity. Although such relationships were not key predictions of the postural instability theory (Stoffregen and Smart 1998), our results revealed significant relationships between sickness severity and amount of change in our participants’ sway over the course of the trial. Specifically, we found that cybersickness became more severe when the spatial magnitude of our participants’ sway increased over the HMD-VR exposure (i.e., both in terms of changes in the STDEV CoPM/L and STDEV CoPA/P in the last 30 s compared to the first 30 s). The severity of this cybersickness increased as the changes in our participants’ late-early DFA αM/L values decreased (i.e., sickness was greater as the original CoP time series data became “rougher” as opposed to “smoother”). These findings highlight that, despite not being a key component of the theory, the assessment of changes in postural stability may still be a useful tool for predicting and monitoring cybersickness severity.
4.3 Combined models of cybersickness
We next explored combined models that attempted to predict the current cybersickness findings based on both the participants’ reported experience of vection (its strength and type) and their postural sway (its temporal dynamics and positional variability).
We first examined the ability of a combined model to predict our participants’ sick/well group membership. The results showed that participants were significantly more likely to report becoming sick after they had experienced unexpected (as opposed to expected) vection. This particular vection type effect was again found to be independent of vection strength in the combined model. However, postural sway was not found to significantly contribute to sick/well predictions in the presence of vection based measures (despite previously contributing to such predictions when examined in isolation). One possible explanation for these findings was that vection type effects simply overshadowed postural instability based contributions to the combined model. However, the sickness experienced in our study could still have conceivably been produced by changes in our participants’ postural instability—despite their apparent null findings in this combined model. According to this view, the reported experiences of unexpected vection might actually have been conscious sensations related to provocative changes in postural activity.
We next investigated the ability of a combined (vection and sway based) model to predict our cybersickness severity data. Unlike the combined model for sick/well group membership described above, we found that both vection and sway based measures contributed significantly to predicting our participants’ experiences of cybersickness severity. We again found evidence of a positive relationship between vection strength and sickness severity, which was best explained by a non-linear exponential fit. On further analysis of the simple effects, we also found that this relationship was only significant among participants who had experienced unexpected vection. We also found that sickness severity increased with increases in the sway along the M/L axis over the course of the HMD-VR exposure, and as the late-early changes in their DFA αM/L values decreased. We did not however find any significant predictions based on their A/P sway measures.
These findings suggest that an HMD user’s sway is important for predicting and monitoring their experiences of sickness severity, which is consistent with postural instability based explanations of cybersickness. However, our results also suggest that subjective reports of unexpected vection might be better predictors of the onset/occurrence of their cybersickness (at least compared to the two objectively measured indices of postural instability examined in the current study).
4.4 Implications and relevance of findings
Compelling vection has been a highly effective tool in enhancing the immersive experience of HMD-VR. By inducing vection through visual stimuli, such as moving patterns or simulated motion, HMD-VR can create a greater sense of presence and immersion in virtual environments than other mediums (Teixeira et al. 2021). In some contexts, a compelling sense of vection may be critical to accurately/convincingly simulating experiences in VR, such as flight and driving simulations. Yet, vection is still often regarded as a problem to be avoided. This persistent belief has led to a reluctance to incorporate compelling vection into HMD-VR experiences, ultimately limiting the potential benefits of the technology. Our current findings challenge the belief that compelling vection is always an issue for cybersickness. Thus, we propose that only unexpected types of vection should be avoided to minimize cybersickness occurrence. To achieve this, we propose a few strategies. Developers could approach game design with the prevention of unexpected vection in mind. In addition, optional ‘comfort’ modes with clear indications, such as directional arrows or preparatory animations, could help prepare the user for upcoming simulated self-motions (reducing the likelihood of unexpected vection experiences). Moreover, beta testing could be used to tailor game experiences of vection based on user feedback (with the aim being to identify and rectify any reported instances of unexpected vection).
As with Teixeira et al. (2022), our findings show that non-linear models better capture the relationships between vection strength and cybersickness severity (rather than the strictly linear models used by most previous studies—see Teixeira et al. 2022 for more details). In the future, if clear links are only found between specific types of vection and cybersickness, then designers would be free to explore the use of other types of vection to enhance their programs and designs. This could open further avenues for enhancing presence (which is often positively associated with vection strength—see Teixeira and Palmisano 2021), and in turn the fidelity, realism, and quality of the sensory stimulation provided by HMD-VR.
In this study, we also found support for the postural instability theory ‒ most notably, we found that the positional variability of our participants’ sway increased just before their first experience of sickness (i.e., their sway variability was greater when they dropped out of the simulation compared to the beginning of the HMD-VR exposure). We also found that the size of these late-early changes in their sway scaled with the severity of their cybersickness symptoms. Taken together, these findings suggest that the physical demands of VR experiences, particularly the challenges to the HMD user’s postural control, could be a significant factor in the development of cybersickness. To address this issue, a range of strategies could be implemented, such as: (1) designing VR devices that provide additional support or stabilization to reduce the demands on the HMD user's postural control system, or (2) incorporating exercises to improve their balance and stability as a pre-VR warm-up. By proactively addressing these postural instability concerns, it may be possible to reduce the occurrence and severity of cybersickness symptoms, ultimately enhancing the HMD user's VR experience. However, in our combined models we found that unexpected vection and vection strength appeared to explain more of the variance in the current cybersickness data, suggesting that inducing vection in a more controlled and predictable manner might be the most effective strategy for managing cybersickness symptoms.
The possibility remains that unexpected vection could exacerbate postural instability, which in turn could trigger the symptoms of cybersickness. For example, if a virtual environment suddenly generated an unexpected type or experience of vection, then the HMD user might involuntarily shift their posture (to attempt to maintain their balance), leading to postural instability, and in turn sickness. To avoid such problems, VR designers would therefore need to carefully manipulate their visual simulations in order to induce vection in a controlled and gradual manner and avoid eliciting sudden, or unpredictable user movements (that could provoke unexpected vection).
Overall, our findings: (1) highlight the importance of considering both postural stability/instability and vection based factors in the design of VR experiences; and (2) suggest that a combination of strategies which address both factors would be most effective in managing cybersickness symptoms. By doing so, we would likely enhance the overall quality and effectiveness of VR experiences and reduce the negative impact of cybersickness on HMD users.
4.5 Limitations and future directions
While we do acknowledge the possibility that demand characteristics might have influenced our study’s outcomes (particularly our assessments of expected and unexpected vection), the risk of such problems was deemed to be low. In order to minimise this particular risk: (1) our participants were only given a single exposure to HMD-VR; and (2) we only questioned them about the type of vection that they had experienced after the exposure had ceased (with the exact question text provided in 2.2.4). Future studies could also test our unexpected vection hypothesis using more deliberate experimental manipulations. For example, in such an experiment, participants might be instructed to discontinue HMD-VR as soon as they experience any unexpected vection; continuing in the simulation only as long as their experience of vection was expected. This method might provide a more controlled and rigorous evaluation of the unexpected vection-sickness relationship, increasing the validity of subsequent findings.
In our study, participants interacted with their virtual environment while standing on a balance board (which was 60 cm wide × 40 cm deep). Their up to 14-min exposures to this simulation ensured that they could fully engage with all of the interactive material that this game provided. While the current experimental design was appropriate for Aircar’s game content and average play duration, it might not be optimal for other HMD VR games – especially those with more content and which support seated user experiences or free room-scale movement. Future research on unexpected vection should explore how gameplay in different contexts affects its relationship with cybersickness.
Additionally, it has also been shown that passive self-motion is often associated with higher levels of motion sickness compared to active self-motion, where users have control over their locomotion (Dong and Stoffregen 2010; Stanney and Hash 1998; Littman et al. 2010; Risi and Palmisano 2019). This difference is primarily attributed to the user's level of control; as active self-motion allows for more predictable and controllable experiences, thereby potentially reducing the incidence of cybersickness. Building on this understanding, we hypothesize that the effect of expected versus unexpected vection may also be influenced by whether the VR experience is passive or active. In active VR scenarios, where users have control over their motion, the predictability of vection might reduce the likelihood of cybersickness. Conversely, in passive VR scenarios, where motion is externally controlled and less predictable, unexpected vection might contribute more significantly to cybersickness. We recommend future research should aim to investigate the effects of vection and sway on cybersickness in both active and passive VR settings.
Finally, our investigation focused on determining the occurrence of unexpected vection prior to the initial onset of cybersickness symptoms. Although this provided valuable insights into the early stages of vection and its potential role in cybersickness, we did not track the frequency or duration of vection episodes throughout the entire exposure period. For a more thorough exploration of the phenomenon, future studies should monitor and assess unexpected/expected vection continuously during VR exposure. This would allow for a detailed analysis of vection in relation to the progression of cybersickness experiences over time.
4.6 Conclusions
In this study, we investigated the effects of unexpected vection and postural instability on the cybersickness produced by a commercially available HMD-VR game. We found that participants were significantly more likely to become sick after experiencing unexpected vection (compared to when their vection was always expected). The severity of this cybersickness was also found to increase with reported vection strength, but again only when this vection was unexpected. In addition, we also found some support for the postural instability theory ‒ specifically, that the positional variability of the HMD user’s sway increased just prior to the onset of sickness (compared to their sway at the beginning of the HMD-VR exposure). When modelling the effects of these vection and sway measures together, we found that unexpected vection appeared to explain more of the variance in the cybersickness data than the postural measures. Understanding the role of unexpected vection in cybersickness appears to be important for both improving user experiences and reducing the prevalence of cybersickness. Further research is needed to explore the unexpected vection hypothesis in an experimental manner–in order to develop effective strategies for mitigating cybersickness symptoms. It is hoped that the current study provides a suitable foundation for future research on this hypothesis.
Data availability
Availability of data and material: Data will be made available upon request.
Code availability
We used a commercially available video game in this study.
Notes
Visually induced motion sickness (VIMS) refers to motion sickness symptoms that are triggered by visual motion stimulation (often without any corresponding physical movement). Specifically, VIMS can be induced by changes in patterns of apparent motion in surfaces, objects, and edges within an individual’s visual field. For example, someone might experience VIMS while playing a first-person video game when the virtual environment moves rapidly, even though they are physically stationary (Hettinger and Riccio 1992).
Dennison and D’Zmura also did not use a forced-choice response to discriminate sick from well participants. Instead, participants were classified as either “less comfortable” and “more comfortable” based on having a SSQ score greater than the median score.
Unexpected Vection occurs when: 1) an individual feels as that they are moving even though they are physically stationary; and 2) this perceived movement is occurring in an unexpected/unanticipated manner. This is distinct from unexpected visual motion. While abrupt visual object motions can be unsettling, they do not inherently generate the multisensory conflict associated with unexpected vection, making the latter a more likely trigger for cybersickness.
Support for this idea also appears to be provided by recent findings from Nooij et al. (2021).
Specifically, those who had difficulty with game controls frequently encountered unexpected movements in the VR environment, resulting in a higher incidence of unexpected vection. Analyses revealed highly similar patterns, suggesting a strong inter-correlation between control difficulties and unexpected vection.
While prior studies have reported less VIMS (e.g., Ujike et al. 2008; Keshavarz 2016; Pöhlmann et al., 2022) and stronger vection experiences (Pöhlmann et al. 2022) among regular gamers, we did not find significant differences between gamers and non-gamers in vection and cybersickness (see Tables 4–9 in Appendix A). Conceivably, the current findings might have been due to unique features of our VR setup (such as the independent control of the aircar’s yaw, pitch, and roll movements), which could have similarly challenged both groups.
If participants completed the travel route before the 14 min elapsed, they were instructed to return to the starting point and begin the route again.
5. References
Akiduki H, Nishiike S, Watanabe H, Matsuoka K, Kubo T, Takeda N (2003) Visual-vestibular conflict induced by virtual reality in humans. Neurosci Lett 340(3):197–200
Andersen GJ, Braunstein ML (1985) Induced self-motion in central vision. J Exp Psychol: Hum Percept Performan 11(2):122
Arcioni B, Palmisano S, Apthorp D, Kim J (2019) Postural stability predicts the likelihood of cybersickness in active HMD-based virtual reality. Displays 58:3–11. https://doi.org/10.1016/j.displa.2018.07.001
Bonato F, Bubka A, Alfieri L (2004) Display color affects motion sickness symptoms in an optokinetic drum. Aviat Space Environ Med 75(4):306–311
Bonato F, Bubka A, Story M (2005) Rotation direction change hastens motion sickness onset in an optokinetic drum. Aviat Space Environ Med 76(9):823–827
Bonato F, Bubka A, Palmisano S, Phillip D, Moreno G (2008) Vection change exacerbates simulator sickness in virtual environments. Presence Teleoper Virtual Environ 17(3):283–292
Bonato F, Bubka A, Palmisano S (2009) Combined pitch and roll and cybersickness in a virtual environment. Aviat Space Environ Med 80(11):941–945
Bonnet CT, Faugloire E, Riley MA, Bardy BG, Stoffregen TA (2006) Motion sickness preceded by unstable displacements of the center of pressure. Hum Mov Sci 25(6):800–820
Chardonnet JR, Mirzaei MA, Merienne F (2017) Features of the postural sway signal as indicators to estimate and predict visually induced motion sickness in virtual reality. Int J Hum Comput Interact 33(10):771–785. https://doi.org/10.1080/10447318.2017.1286767
Chen DJ, Chow EH, So RH (2011) The relationship between spatial velocity, vection, and visually induced motion sickness: an experimental study. i-Percept 2(4):415–415
Clifton J, Palmisano S (2019a) Comfortable locomotion in vr: teleportation is not a complete solution. In: 25th ACM symposium on virtual reality software and technology, pp 1–2
Clifton J, Palmisano S (2019b) Effects of steering locomotion and teleporting on cybersickness and presence in hmd-based virtual reality. Virtual Real 24(3):453–468
Cobb SV (1999) Measurement of postural stability before and after immersion in a virtual environment. Appl Ergon 30(1):47–57. https://doi.org/10.1016/s0003-6870(98)00038-6
Cobb SV, Nichols SC (1998) Static posture tests for the assessment of postural instability after virtual environment use. Brain Res Bull 47(5):459–464. https://doi.org/10.1016/s0361-9230(98)00104-x
Dennison MS, D’Zmura M (2017) Cybersickness without the wobble: experimental results speak against postural instability theory. Appl Ergon 58:215–223. https://doi.org/10.1016/j.apergo.2016.06.014
Diels C, Ukai K, Howarth PA (2007) Visually induced motion sickness with radial displays: effects of gaze angle and fixation. Aviat Space Environ Med 78(7):659–665
Dong X, Stoffregen T A (2010). Postural activity and motion sickness among drivers and passengers in a console video game. In: Proceedings of the human factors and ergonomics society annual meeting 54(18):1340–1344. https://doi.org/10.1177/1541931210054018
Flanagan MB, May JG, Dobie TG (2002) Optokinetic nystagmus, vection, and motion sickness. Aviat Space Environ Med 73(11):1067–1073
Golding JF, Doolan K, Acharya A, Tribak M, Gresty MA (2012) Cognitive cues and visually induced motion sickness. Aviat Space Environ Med 83(5):477–482
Hadidon T J (2016). An optimized algorithm for prediction of virtual environment motion sickness using postural sway. Unpublished master’s thesis, Miami University, Oxford, OH.
Hettinger LJ, Berbaum KS, Kennedy RS, Dunlap WP, Nolan MD (1990) Vection and simulator sickness. Mil Psychol 2(3):171–181. https://doi.org/10.1207/s15327876mp0203_4
Hettinger LJ, Riccio GE (1992) Visually induced motion sickness in virtual environments. Presence Teleoper Virtual Environ 1:306–310. https://doi.org/10.1162/pres199213306
Ji JT, So RH, Cheung RT (2009) Isolating the effects of vection and optokinetic nystagmus on optokinetic rotation-induced motion sickness. Hum Factors 51(5):739–751
Kennedy RS, Hettinger LJ, Lilienthal MG (1990) Simulator sickness. In: Crampton GH (ed) Motion and space sickness. CRC Press, Boca Raton, pp 317–342
Kennedy RS, Lane NE, Berbaum KS, Lilienthal MG (1993) Simulator sickness questionnaire: an enhanced method for quantifying simulator sickness. Int J Aviat Psychol 3(3):203–220
Keshavarz B (2016) Exploring behavioral methods to reduce visually induced motion sickness in virtual environments. In: Virtual, augmented and mixed reality: 8th international conference, VAMR 2016, pp. 147–155. https://doi.org/10.1007/978-3-319-39907-2_14
Keshavarz B, Hettinger LJ, Vena D, Campos JL (2014) Combined effects of auditory and visual cues on the perception of vection. Exp Brain Res 232(3):827–836
Keshavarz B, Riecke BE, Hettinger LJ, Campos JL (2015) Vection and visually induced motion sickness: How are they related? Front Psychol. https://doi.org/10.3389/fpsyg.2015.00472
Koslucher FC, Haaland E, Malsch A, Webeler J, Stoffregen TA (2015) Sex differences in the incidence of motion sickness induced by linear visual oscillation. Aviat Med Hum Perform 86:787–793
Koslucher F, Haaland E, Stoffregen TA (2016) Sex differences in visual performance and postural sway precede sex differences in visually induced motion sickness. Exp Brain Res 234:313–322
Kuiper OX, Bos JE, Diels C (2019) Vection does not necessitate visually induced motion sickness. Displays 58:82–87
Lawson B (2014) Motion sickness symptomatology and origins. In: Hale KS, Stanney KM (eds) Handbook of virtual environments: design, implementation, and applications. CRC Press, Boca Raton, FL, pp 532–587
Lawson B, Stanney KM (2021) Editorial: cybersickness in virtual reality and augmented reality. Front Virtual Real. https://doi.org/10.3389/frvir2021759682
Lawson B D (2005) Exploiting the illusion of self-motion (vection) to achieve a feeling of ‘virtual acceleration’ in an immersive display. In: Proceedings of the 11th international conference on human–computer interaction. HCI, Las Vegas, pp 1–10
Litleskare S (2021) The relationship between postural stability and cybersickness: it’s complicated–an experimental trial assessing practical implications of cybersickness etiology. Physiol Behav 236:113422
Littman EM, Otten EW, Smart LJ Jr (2010) Consequence of self versus externally generated visual motion on postural regulation. Ecol Psych 22(2):150–167. https://doi.org/10.1080/10407411003720106
Mazloumi Gavgani A, Hodgson DM, Nalivaiko E (2017) Effects of visual flow direction on signs and symptoms of cybersickness. PLoS ONE. https://doi.org/10.1371/journal.pone.0182790
McCauley ME, Sharkey TJ (1992) Cybersickness: perception of self-motion in virtual environments. Presence: Teleoper Virtual Environ 1:311–318. https://doi.org/10.1162/pres.1992.1.3.311
Merhi O, Faugloire E, Flanagan M, Stoffregen TA (2007) Motion sickness, console video games, and head-mounted displays. Hum Factors. https://doi.org/10.1518/001872007X230262
Munafo J, Diedrick M, Stoffregen TA (2017a) The virtual reality head-mounted display Oculus Rift induces motion sickness and is sexist in its effects. Exp Brain Res. https://doi.org/10.1007/s00221-016-4846-7
Munafo J, Diedrick M, Stoffregen TA (2017b) The virtual reality head-mounted display Oculus Rift induces motion sickness and is sexist in its effects. Exp Brain Res 235:889–901
Nishiike S, Okazaki S, Watanabe H, Akizuki H, Imai T, Uno A, Kitahara K, Horii A, Takeda N (2013) The effect of visual-vestibulosomatosensory conflict induced by virtual reality on postural stability in humans. J Med Investig 60:236–239
Nooij SA, Pretto P, Oberfeld D, Hecht H, Bülthoff HH (2017) Vection is the main contributor to motion sickness induced by visual yaw rotation: implications for conflict and eye movement theories. PLoS ONE 12(4):0175305. https://doi.org/10.1371/journal.pone.0175305
Nooij SA, Pretto P, Bülthoff HH (2018) More vection means more velocity storage activity: a factor in visually induced motion sickness? Exp Brain Res 236:3031–3041
Nooij SA, Bockisch CJ, Bülthoff HH, Straumann D (2021) Beyond sensory conflict: the role of beliefs and perception in motion sickness. PLoS ONE 16(1):e0245295. https://doi.org/10.1371/journal.pone.0245295
Palmisano S (1996) Perceiving self-motion in depth: The role of stereoscopic motion and changing-size cues. Percept Psychophys 58(8):1168–1176. https://doi.org/10.3758/BF03207550
Palmisano S, Chan AY (2004) Jitter and size effects on vection are immune to experimental instructions and demands. Percept 33(8):987–1000
Palmisano S, Riecke BE (2018a) The search for instantaneous vection: an oscillating visual prime reduces vection onset latency. PLoS ONE 13(5):e0195886
Palmisano S, Bonato F, Bubka A, Folder J (2007) Vertical display oscillation increases vection in depth and simulator sickness. Aviat Space Environ Med 78(10):951–956
Palmisano S, Allison RS, Schira MM, Barry RJ (2015) Future challenges for vection research: definitions, functional significance, measures, and neural bases. Front Psychol 6(193):1–15. https://doi.org/10.3389/fpsyg.2015.00193
Palmisano S, Mursic R, Kim J (2017) Vection and cybersickness generated by head-and-display motion in the oculus rift. Displays 46:1–8. https://doi.org/10.1016/j.displa.2016.11.001
Palmisano S, Arcioni B, Stapley PJ (2018a) Predicting vection and visually induced motion sickness based on spontaneous postural activity. Exp Brain Res 236(1):315–329. https://doi.org/10.1007/s00221-017-5130-1
Palmisano S, Arcioni B, Stapley PJ (2018b) Predicting vection and visually induced motion sickness based on spontaneous postural activity. Exp Brain Res 236:315–329
Palmisano S, Davies R, Brooks K (2018c) Vection strength increases with simulated eye-separation. Atten Percept Psychophys 81(1):281–295. https://doi.org/10.3758/s13414-018-1609-5
Palmisano S, Allison RS, Kim J (2020) Cybersickness in head-mounted displays is caused by differences in the user’s virtual and physical head pose Front. Virtual Real 1:24
Palmisano S, Riecke BE (2018b) The search for instantaneous vection: An oscillating visual prime reduces vection onset latency. PLoS ONE 13(5):e0195886. https://doi.org/10.1371/journalpone0195886
Palmisano S (2002) Consistent stereoscopic information increases the perceived speed of vection in depth. Percept 31(4):463–480. https://doi.org/10.1068/p3321
Pöhlmann KMT, O’Hare L, Dickinson P, Parke A, Föcker J (2022) Action video game players do not differ in the perception of contrast-based motion illusions but experience more vection and less discomfort in a virtual environment compared to non-action video game players. J Cogn Enhanc. https://doi.org/10.1007/s41465-021-00215-6
Reason JT (1978) Motion sickness adaptation: a neural mismatch model. J R Society Med 71(11):819–829
Reason J, Brand J (1975) Motion sickness. Academic Press, London
Riccio GE, Stoffregen TA (1991) An ecological theory of motion sickness and postural instability. Eco Psychol 3(3):195–240. https://doi.org/10.1207/s15326969eco0303_2
Riecke BE, Jordan JD (2015) Comparing the effectiveness of different displays in enhancing illusions of self-movement (vection). Front Psychol 6:713
Risi D, Palmisano S (2019) Effects of postural stability, active control, exposure duration and repeated exposures on HMD induced cybersickness. Displays 60:9–17. https://doi.org/10.1016/jdispla201908003
Smart LJ Jr, Stoffregen TA, Bardy BG (2002) Visually induced motion sickness predicted by postural instability. Hum Factors 44(3):451–465
Smart LJ Jr, Otten EW, Strang AJ, Littman EM, Cook HE (2014) Influence of complexity and coupling of optic flow on visually induced motion sickness. Ecol Psych 26(4):301–324
Smart LJ Jr, Drew A, Hadidon T, Teaford M, Bachmann E (2021) Using nonlinear kinematic parameters as a means of predicting motion sickness in real-time in virtual environments. Hum Factors. https://doi.org/10.1177/00187208211059623
Stanney KM, Kennedy RS, Hale KS (2014) Virtual environment usage protocols. In: Hale KS, Stanney KM (eds) Handbook of virtual environments: design, implementation and applications. CRC Press, Boca Raton, pp 532–587
Stanney KM, Hash P (1998) Locus of user-initiated control in virtual environments: Influences on cybersickness. Presence 7(5):447–459. https://doi.org/10.1162/105474698565848
Stoffregen TA, Riccio GE (1991) An ecological critique of the sensory conflict theory of motion sickness. Eco Psychol 3(3):159–194. https://doi.org/10.1207/s15326969eco0303_2
Stoffregen TA, Smart LJ Jr (1998) Postural instability precedes motion sickness. Brain Res Bull 47(5):437–448
Stoffregen TA, Hettinger LJ, Haas MW, Roe MM, Smart LJ (2000) Postural instability and motion sickness in a fixed-base flight simulator. Hum Factors 42(3):458–469
Stoffregen TA, Faugloire E, Yoshida K, Flanagan MB, Merhi O (2008) Motion sickness and postural sway in console video games. Hum Factors 50(2):322–331
Stoffregen TA, Yoshida K, Villard S, Scibora L, Bardy BG (2010) Stance width influences postural stability and motion sickness. Eco Psychol 22(3):169–191
Stoffregen TA, Chen YC, Koslucher FC (2014) Motion control, motion sickness, and the postural dynamics of mobile devices. Exp Brain Res 232:1389–1397
Teixeira J, Miellet S, Palmisano S (2022) Unexpected vection exacerbates cybersickness during HMD-based virtual reality. Front Virtual Real 3:43
Teixeira J, Palmisano S (2021) Effects of dynamic field-of-view restriction on cybersickness and presence in HMD-based virtual reality. Virtual Real 25:433–445. https://doi.org/10.1007/s10055-020-00466-2
Ujike H, Ukai K, Nihei K (2008) Survey on motion sickness-like symptoms provoked by viewing a video movie during junior high school class. Displays 29(2):81–89. https://doi.org/10.1016/j.displa.2007.09.003
Villard SJ, Flanagan MB, Albanese GM, Stoffregen TA (2008) Postural instability and motion sickness in a virtual moving room. Hum Factors 50(2):332–345
Webb NA, Griffin MJ (2002) Optokinetic stimuli: motion sickness, visual acuity and eye movements. Aviat Space Environ Med 73(4):351–358
Webb NA, Griffin MJ (2003) Eye movement, vection, and motion sickness with foveal and peripheral vision. Aviat Space Environ Med 74(6):622–625
Yokota Y, Aoki M, Mizuta K, Ito Y, Isu N (2005) Motion sickness susceptibility associated with visually induced postural instability and cardiac autonomic responses in healthy subjects. Acta Otolaryngol 125:280–285. https://doi.org/10.1080/00016480510003192
Funding
Open Access funding enabled and organized by CAUL and its Member Institutions. This research was supported by an Australian Research Council (ARC) Discovery Project (DP210101475).
Author information
Authors and Affiliations
Contributions
JT, SM and SP formed the original conceptualization for the study. JT collected the data. JT, SM and SP analysed the data, interpreted the results and wrote the article.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Appendix A
Appendix A
See Table 4, 5, 6, 7, 8 and 9.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Teixeira, J., Miellet, S. & Palmisano, S. Effects of vection type and postural instability on cybersickness. Virtual Reality 28, 82 (2024). https://doi.org/10.1007/s10055-024-00969-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s10055-024-00969-2