
Abstract
Purpose
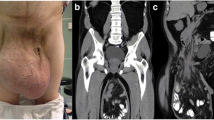
Giant inguinoscrotal hernias represent a real public health problem in the Ivory Coast that can dramatically impair patients’ quality of life. Limited resources require a simplified surgical strategy including, in our experience, not using a mesh and leaving the distal hernia sac. The aim of this study was to evaluate the benefits of this technique in terms of complications (seroma, haematoma, trophic troubles) and the ability to recover from surgery and return to work at 1 month postsurgery.
Methods
Between January and May 2012, all patients who presented with a giant primary inguinoscrotal hernia that was spontaneously reducible in the decubitus position and who did not have any trophic changes in the scrotal skin were prospectively studied. The surgical procedure was a herniorrhaphy as described by Bassini. All patients received follow-up examinations on postoperative days 5, 12 and 30.
Results
Twenty-five males with a median age of 42 years (range 18–60) underwent surgery. Three patients (12 %) presented with a superficial skin infection and four (16 %) with early scrotal swelling without seroma, spontaneously resolved by postoperative day 30. Three patients (12 %) presented with scrotal swelling and seroma; two required aspiration. No early recurrence was observed at the end of follow-up, and all patients were able to return to work.
Conclusion
Leaving the distal hernial sac in the scrotum does not interfere with the type of hernia repair and can limit the occurrence of complications. This technique is reliable, reproducible and does not incur additional morbidity when used in selected patients.





Similar content being viewed by others


References
Hodgkinson DJ, McIltrath DC (1984) Scrotal reconstruction for giant hernias. Surg Clin N Am 64:301–313
Vano-Galvan S, Guisado-Vasco P, Jaén P (2009) Giant inguinoscrotal hernia. Aust Fam Physician 38:222–223
Vasiliadis K, Knaebel HP, Djakovic N, Nyarangi-Dix J, Schmidt J, Büchler M (2010) Challenging surgical management of giant inguinoscrotal hernia: report of case. Surg Today 40:684–687
Mchendale FV, Taams KO, Kingsnorth AN (2000) Repair of a giant inguinoscrotal hernia. Br J Plast Surg 53:525–529
Coetzee E, Price C, Boutall A (2011) Simple repair of a giant inguinoscrotal hernia. Int J Surg Case Rep 2:32–35
Ohene-Yeboah M, Abantanga FA (2011) Inguinal hernia disease in Africa: a common but neglected surgical condition. West Afr J Med 30:77–83
Yang J, Papandria D, Rhee D, Perry H, Abdullah F (2011) Low-cost mesh for inguinal hernia repair in resource-limited settings. Hernia 15:485–489
Patsas A, Tsiaousis P, Papaziogas B, Koutelidakis I, Goula C, Atmatzidis K (2010) Repair of a giant inguinoscrotal hernia. Hernia 14:305–307
El Saadi AS, Al Wadan AH, Hamerna S (2005) Approach to a giant inguinoscrotal hernia. Hernia 9:277–279
Kovachev LS, Paul AP, Chowdhary P, Choudhary P, Filipov ET (2010) Regarding extremely large inguinal hernias with a contribution of two cases. Hernia 14:193–197
Gaines RD (1978) Complications of groin hernia repair: their prevention and management. J Natl Med Assoc 70:195–198
Tahir M, Ahmed FU, Seenu V (2008) Giant inguinoscrotal hernia: case report and management principles. Int J Surg 6:495–497
Amid PK (2005) Groin hernia repair: open techniques. World J Surg 29:1046–1051
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Savoie, PH., Abdalla, S., Bordes, J. et al. Surgical repair of giant inguinoscrotal hernias in an austere environment: leaving the distal sac limits early complications. Hernia 18, 113–118 (2014). https://doi.org/10.1007/s10029-013-1049-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10029-013-1049-z