
Abstract
Background
Hip replacement surgery is highly effective in relieving pain and improving mobility in patients with various hip conditions. However, some patients develop groin pain after surgery, often due to iliopsoas impingement (IPI), which can be challenging to diagnose. Conservative treatments are initially recommended, but when these are not effective, surgical options may be considered. This study aims to evaluate the clinical outcomes, success and failure rates, revision rates, and complications associated with arthroscopic and endoscopic surgery for IPI, thereby providing a comprehensive understanding of the effectiveness and risks of these surgical interventions.
Materials and methods
A systematic review was conducted following Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, including a thorough search of five main databases: PubMed, Scopus, Embase, Medline, and Cochrane. Eligible articles were meticulously evaluated according to predefined criteria for levels of evidence (LoE), with retrospective studies assessed using the Coleman Methodology Score (mCMS). This systematic review was registered in the International Prospective Registry of Systematic Reviews (PROSPERO).
Results
Among the 16 included studies, 431 patients with 434 hips underwent either endoscopic or arthroscopic tenotomy. Both techniques showed favorable outcomes, with arthroscopic tenotomy demonstrating slightly higher success rates than endoscopic tenotomy. Common complications included mild pain and occasional infections, with recurrence observed in some cases. Both techniques offer direct visualization of prosthetic components and potential preservation of psoas function.
Conclusions
Arthroscopic and endoscopic iliopsoas tenotomy are effective treatments for alleviating symptoms and improving hip function in patients with IPI post-total hip arthroplasty (THA).
Level of evidence
IV.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Hip replacement surgery effectively treats problems such as degeneration, arthritis, and severe pain. The surgery relieves pain, improves mobility and function, and increases overall well-being for many patients. However, after surgery, some patients experience groin pain with a prevalence ranging from 0.4 to 18.3% [1, 2]. Among the potentially most underdiagnosed causes of inguinal pain is iliopsoas impingement (IPI), which, according to the literature, has a frequency of 4.4% [2,3,4,5]. The IPI may be due to several factors: acetabular cup fixation screws that are too long and penetrate the ileum, osteophytes, excess cement in the case of cemented acetabular cups, large femoral heads, or protruding cups [6,7,8,9,10,11]. In some patients, those with acetabular dysplasia, hypoplasia of the anterior wall creates a higher risk of impingement with the iliopsoas tendon: a prominent cup induces friction and irritation on the iliopsoas tendon itself, resulting in bursal effusion, tendinitis, and sometimes partial rupture [4, 12, 13]. Patients with this condition present with groin pain while climbing stairs, lying in bed, or getting out of a car. It may be perceived as a snapping or clanking sensation [4, 8]. The onset of pain varies from immediately after surgery to several years afterward. Clinically there is no specific test, although a painful resisted straight-leg raise test or pain with passive hyperextension are common findings [4, 14, 15]. The diagnosis of IPI is clinical, but an anteroposterior (AP) X-ray of the pelvis and a lateral X-ray of the hip provide a better assessment of cup placement [4, 5, 8]. Other imaging examinations such as ultrasound, computed tomography (CT) scan, or magnetic resonance imaging (MRI) with metal artifact reduction sequence (MARS) provide a more accurate diagnosis and allow better study of the positioning of prosthetic components that may cause impingement [16,17,18].
For this pathology, the first line of treatment is conservative with non-steroidal anti-inflammatory drugs (NSAIDs), targeted physiotherapeutic stretching exercises and possible ultrasound-guided infiltrative therapy at the level of the iliopsoas with local anesthetics, corticosteroids or even botulinum toxin [19, 20]. Resolution of symptoms with nonsurgical treatment is expected in about 47–50% of patients [5, 21]. Surgical treatment is proposed for patients who do not respond to conservative therapy and with significant symptomatology. In the past, the most used surgeries were open tenotomy of the iliopsoas for patients with acetabular prominence < 8 mm or revision of the acetabular component for patients with acetabular prominence > 8 mm [4, 5]. In any case, open-release surgery is a moderately invasive procedure and can be technically challenging, particularly in the presence of a previous hip approach. All this has led to the increased use of minimally invasive arthroscopic techniques for iliopsoas tenotomy for this type of patient.
Several methods are used for arthroscopic and endoscopic iliopsoas tenotomy: a tenotomy at the level of the lesser trochanter, with access to the distal insertion of the iliopsoas tendon, as described by Ilizaliturri in 2005 and by Williams in 2018 [22, 23]; or a transcapsular release at the level of the psoas notch, as described by Wettstein in 2006 [24].
This systematic review aims to comprehensively analyze the clinical outcomes, success rates, failure rates, revision rates, and associated complications of arthroscopic and endoscopic surgery for IPI in patients who have undergone hip replacement. By providing a detailed understanding of the effectiveness and risks of this surgical intervention, the findings will guide clinical decisions and enhance patient car.
Materials and methods
Search strategy and study screening
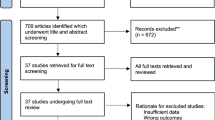
A comprehensive and systematic literature search was conducted across five databases (PubMed, Scopus, Embase, Medline and Cochrane) utilizing the following MeSH terms: ((psoas) OR (iliopsoas)) AND ((tenotomy) OR (release)) AND ((endoscopy) OR (arthroscopy)) AND ((THR) OR (Total hip replac*) OR (THA) OR (total hip arthroplast*)). Three authors (RGV, AE and AD) independently conducted a literature search and evaluated studies to minimize mistakes. Uncertainties were resolved through consultation with a fourth author (MG). The search included 114 studies published from 2000 to February 2024. After removing duplicates, 53 studies were included. Following a review of the title and abstract of these studies, 34 studies were excluded, yielding 19 eligible studies. After full-text evaluation, 16 clinical studies met the qualitative analysis eligibility criteria. The included studies directly reported functional outcomes, time for resolution and improvement of symptoms, and differences in complication rates among patients undergoing arthroscopic iliopsoas tenotomy with a prior hip replacement surgery. This study adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [25] (Fig. 1).

Preferred reporting items for systematic reviews and meta-analyses (PRISMA) flow diagram
Inclusion and exclusion criteria
The inclusion criteria for the reviewed studies were articles about patients with prior hip replacement surgery undergoing arthroscopic surgery for iliopsoas tenotomy. These articles, published in English, involved human subjects, with publication dates falling between 2000 and February 2024 and a minimum mean follow-up of six months. Randomized controlled trials (RCTs) and prospective and retrospective studies with levels of evidence (LoE) between 1 and 4 were considered [26]. Biochemical and in vitro studies, case reports, editorials, book chapters, technical reports, pre-clinical studies, review articles and studies with LoE 5 were excluded for better-quality research.
Methodological quality assessment
Each included article was evaluated according to the Oxford Centre for Evidence-Based Medicine 2011 LoE, which range from 1 to 5. The Coleman Methodology Score (mCMS), modified by Ramponi et al. [27], was used for retrospective studies (Fig. 2). Two authors (RGV, AE) employed this tool, with a third author (SDV) consulted for uncertainty resolution. All authors contributed substantially to the ideation and design of the study, data acquisition, manuscript writing, and final editing, and approved the final version of the article. This systematic review was registered in the International Registry of Systematic Reviews (PROSPERO), in March 2024 [28].

The coleman methodology score (mCMS), modified by ramponi et al. [27]
Data extraction
Data extracted from the included articles were meticulously recorded in Excel spreadsheets by two independent authors (RGV and AE) and then subsequently unified. This included details such as the author and year of publication, study design, patient sample size, mean age, mean BMI, mean interval time between hip replacement surgery and symptoms onset, mean follow-up time, type of hip prosthesis, cup inclination and anteversion, type of anesthesia, rates of complications and recurrence, pre and post-operative subjective scores such as modified Harris Hip Score (mHSS), Visual Analogue Scale (VAS), Western Ontario and McMaster Universities Arthritis Index (WOMAC), Oxford Hip Score (OHS), International Hip Outcome Tool (iHOT33) or Copenhagen Hip and Groin Outcome Score (HAGOS). This facilitated organized data extraction and analysis, providing a comprehensive understanding of the study results.
Data analysis
Statistical analysis used R software (version 4.1.3 from 2022), developed by the R Core Team in Vienna, Austria. Descriptive statistical methods were used for the data obtained from the included studies. Mean values were calculated for continuous variables, while variability was assessed through standard deviation (SD) or range (minimum–maximum) measures. Absolute numbers and frequency distributions were determined for categorical variables.
Results
Study characteristics
From the 114 studies initially retrieved, 16 studies met the inclusion criteria according to PRISMA flow chart [2, 23, 29,30,31,32,33,34,35,36,37,38,39,40,41,42]. Among these, seven studies focused on arthroscopic intracapsular iliopsoas tenotomy, seven on endoscopic extracapsular iliopsoas tenotomy, and two on both techniques. All patients underwent prior THR (primary or revision) or hip resurfacing and experienced post-operative iliopsoas tendinitis and failed conservative management that included physical therapy, injections, watchful waiting, or activity modification. Most studies were classified as level IV evidence and were predominantly retrospective (Table 1).
Demographics
This systematic review included 431 patients and 434 hips with IPI; 139 patients underwent arthroscopic intracapsular tenotomy, and 292 patients underwent endoscopic extracapsular tenotomy. The mean age of the patients varied between studies, as shown in Table 1. The sex distribution comprised 145 males and 240 females, with two studies omitting this information. Some studies reported the time from THA to tenotomy, and others mentioned the symptomatic period or both. Most studies reported body mass index (BMI) with mean values ranging from 25.7 to 30.6. All studies had a follow-up duration of at least six months (Table 1).
Diagnosis of IPI was established by clinical presentation, diagnostic injections, and imaging studies detecting acetabular prominence. Typical clinical presentation included groin pain during hip flexion as well as during the straight leg raise test. Radiographs included AP and latearal pelvis X-rays and pelvic CT scans to identify the prominence of acetabular components as a source of mechanical impingement. Pain provocation tests in the iliopsoas sheath were used in most studies for diagnostic confirmation (Table 1). Only two studies mentioned the American Society of Anesthesiologists (ASA) classification. In Williams et al., the mean was 1.8; however, in Bonano et al., the mean was 2 [23, 32].
Table 2 provides an overview of the characteristics of hip arthroplasty reported in the included studies. Most of the studies included were IPI after THA, except in five studies, which included ten patients with impingement after hip resurfacing. One study omitted data regarding the prosthesis [2]. Indications for surgery included failure of nonsurgical management, positive infiltration test, and signs of mechanical impingement on radiographs [2, 23, 32].
Procedures performed
There were two main different techniques reported in the included studies as shown in Table 3.
Endoscopic iliopsoas tenotomy
Seven studies used an endoscopic technique initially described by Ilizaliturri et al. involving extra-articular release against the lesser trochanter with the patient in the supine position [22]. In this technique an inferior visual portal and a superior working portal were used with the hip in flexion and external rotation. An extra-articular approach was used to limit the potential for damage to the prosthetic components. Variations in technique were noted, such as Williams et al. described release of psoas tendon 1–2 cm from LT with or without distal tendon stump (1 cm) removal [23].
Arthroscopic iliopsoas tenotomy
Seven studies used a transcapsular arthroscopic technique with the patient supine and hip flexed at 30° to relax the anterior capsule. Anterolateral (AL) and mid-anterior (MA) portals were created for transcapsular tenotomy. After an extensive debridement, a transcapsular tenotomy was performed according to the Wettstein technique [24] with a radiofrequency probe while keeping the musculature intact. Di Benedetto et al. mentioned one hip endoprosthesis patient with significant periprosthetic ossification that underwent excision [31].
Guicherd et al. and Valenzuela et al. mentioned using both techniques (endoscopic and arthroscopic release). Seven studies stated the type of anesthesia; five were general, and one was spinal [2, 23, 29, 30, 34, 40]. Only 1 study reported the duration of surgery time, which was 23.7 ± 10.6, ranging from 6 to 55 min [34].
Outcome data
The studies included in this systematic review used a variety of subjective outcome scores, as reported in Table 4. A successful outcome was defined as complete pain relief or lack of significant residual pain as assessed by the authors [2, 23, 29,30,31,32,33,34,35,36,37,38,39,40,41,42] at the final follow-up. In the case of arthroscopy, 89.4% of patients experienced favorable outcomes, while for endoscopic tenotomy, the successful outcome rate was 81.3%. For the two studies that used both arthroscopic and endoscopic techniques, one of them didn’t categorize the results of the two techniques [35]. Whereas the study from Valenzuela et al. mentioned that both modified Harris hip score (mHHS) and Non-Arthritic Hip Score (NAHS) showed superiority in the endoscopic group, though with no statistical significance (p = 0.06) [37]. Only one study, conducted by Williams et al., provided the timeframe for improvement, which ranged from 6 to 12 weeks [23].
Regarding the recovery of hip flexion strength after iliopsoas tenotomy, several qualitative methods have been used [30, 31, 35, 39]. Specifically, the MRC (Medical Research Council) score has been used in several studies [30, 31, 35, 39], showing good results, especially at six months follow-up. These results were comparable to the contralateral healthy side after surgery and showed statistically significant improvement over preoperative scores when applicable. Other studies have found improvements in flexion strength after surgery simply through clinical examinations at follow-up visits [32, 37]. Only one study, conducted by Finsterwald [36], used a quantitative method to analyze iliopsoas strength recovery using a dynamometer. This study [36] evaluated the recovery of strength in hip flexion both in supine position with the lower limb extended and in sitting position. The results demonstrated a reduction in flexion strength only in the sitting position, while no reduction was observed in the supine position.
Complications
Post-operative complications, such as mild pain, were noted in the studies included in the systematic review, as reported in Table 4.
Bonano et al. documented two cases of post-operative infection that occurred at 7 and 10 months after surgery, necessitating a two-stage revision THA. One of these patients had previously undergone revision surgery for aseptic mobilization of the femoral stem one year before undergoing endoscopic psoas tenotomy. Notably, infections were not found to be related to the endoscopic procedure. In addition, recurrence occurred in two patients in the series: one underwent open tenotomy of the psoas due to persistent impingement. In contrast, the other patient showed no improvement in the mHHS. The authors suggested that both patients experienced relief from a preoperative steroid provocation test, and complete tendon release at the lesser trochanter level was confirmed in both cases, in addition to cup design/position, muscle tension/unbalance, posture or capsular tethering may have contributed to the recurrence. Specifically, the cup prominence in both cases was less than 8 mm, associated with less improvement in mHHS [32]. Guicherd et al. reported a case of anterior dislocation probably attributable to transcapsular tenotomy, along with a case of compressive hematoma involving the peroneal nerve, both promptly resolved by surgical drainage [35]. Amellal et al. observed three post-operative hematomas, all resolved spontaneously [34]. Nevertheless, Bell et al. reported four patients whose pain persisted after tenotomy. Among them, one patient had a recurrence of pain following a post-operative fall, another had aseptic loosening, and one patient developed a complex regional pain syndrome (CRPS). [38]. Gédouin et al. reported recurrence in two patients unresolved by infiltration, one of whom had periprosthetic ossification [41]. In addition, Filanti et al. documented one case of recurrence and post-operative dissatisfaction. [42]
Discussion
The most important finding of this systematic review is that arthroscopic and endoscopic iliopsoas tenotomy in patients with THA may be an effective surgical procedure for treating symptoms and improving hip flexor weakness and functional outcomes. Two main techniques allow tenotomy of the iliopsoas: extracapsular (endoscopic) [22, 23] or transcapsular (arthroscopic) [24].
The studies analyzed in this systematic review show excellent outcomes for arthroscopic and endoscopic treatment. Of the seven studies analyzed in which patients were treated with extracapsular endoscopic technique, the average percentage of favorable outcomes was 81.3% (62–97.2%). Out of the seven studies that used transcapsular arthroscopic treatment, the average favorable outcome rate was 89.4% (ranging from 81 to 100%).
The transcapsular arthroscopic technique (Fig. 3) has the advantage of directly visualizing the prosthetic bearing surface and anterior margin of the cup irritating the psoas tendon; thus, also having diagnostic value [35], it also allows the theoretical advantage of preserving greater function of the psoas since much of the muscle is at the intra articular level [29].

Illustration of the arthroscopic transcapsular technique for iliopsoas release surgery
The endoscopic technique may be more accessible since it allows more direct identification of the iliopsoas tendon and reduces the risk of damaging the friction couple [35].
The main indication to recur to psoas release rather than directly to cup revision has usually been recognized as 8 mm maximum cup protrusion [4, 5]; it is interesting to observe that in the study of Tassinari et al., excellent results were recorded from arthroscopic release having an average cup protrusion of about 13 mm [30]. This is a significant finding because it allows this pathology to be approached even in cases with cup protrusion greater than 8 mm. It avoids direct recourse to cup revision, a more complex, invasive procedure burdened by a higher rate of complications.
None of the two studies [35, 37] that compared arthroscopic versus endoscopic treatment found statistically significant differences between one technique and the other, deferring the choice of technique preference to the surgeon. Guicherd et al. recommend giving an intracapsular look in case of diagnostic doubts in the case of iliopsoas tenotomy with an extracapsular endoscopic technique; in fact, they report instances of psoitis secondary to metallosis undiagnosed before surgery [35].
Concerning the recovery of hip flexion strength, Tassinari et al. reported superior outcomes in patients undergoing arthroscopic release [30]. Their findings indicated that this technique preserves a larger portion of the muscle belly, with 47% preserved in transcapsular tenotomy compared to 40% in endoscopic tenotomy [30]. Conversely, Valenzuela et al. observed an overall improvement in strength but did not find significant differences between the arthroscopic and endoscopic surgery groups [37]. In contrast, Guicherd et al. reported better recovery of hip flexion strength in patients who underwent physiotherapy [35].
Several studies report favorable outcomes, with no observed loss of strength following arthroscopic iliopsoas release, even in patients with painful internally snapping hips, whether associated with chondrolabral lesions or femoroacetabular impingement (FAI), in both general patients and athletes [43,44,45]. While most studies [30, 31, 35, 39] provide qualitative assessments, quantitative analysis using a dynamometer has been proposed by Finsterwald et al. [36]. This study [36] demonstrated that arthroscopic release of the iliopsoas was associated with a reduction in muscle volume and a decrease in hip flexion strength while seated. Nonetheless, the positive outcomes in hip flexion strength recovery reported in the literature may be attributed to findings by Márquez Arabia [46], which demonstrated via MRI that approximately six months post-surgery, a repair and reconstitution process of the iliopsoas tendon tissue occurs.
Regardless of the technique, full weight-bearing and free ROM are usually granted after surgery to reduce patient immobilization. These are typically associated with stretching and strengthening exercises of the iliopsoas to avoid adhesions and recover flexion strength limitation [36, 42].
Both arthroscopic and endoscopic techniques are not without risks; Guicherd et al. found anterior dislocation of the prosthesis due to excessive capsular debridement and a hematoma with compression and neuropraxia of the femoral nerve completely resolved after the hematoma was drained [35].
Overall, in the studies analyzed, except for the case of dislocation, no complications were reported, and the clinical outcomes were excellent for endoscopic and arthroscopic treatment. These techniques are, therefore, shown to be viable, safe, and reproducible for the management of IPI in patients with THA with a low grade of bias, as demonstrated by Coleman scores.
This systematic review is not without limitations, which must therefore be emphasized. First, most of the studies are retrospective. Second, there is no homogeneity of groups, patient selection, and post-operative program, nor follow-up. Third, not all studies performed an injection test before indication for surgery, a significant test in our opinion. Fourth, these studies are subject to various sources of bias in data collection and reporting, participant selection, and unblinded outcomes assessment that could affect the validity and reliability of the study conclusions. Five, a wide variety of follow-ups with 5.5–144 months were reported in the different studies. A more homogeneous and standardized clinical follow-up could improve the data’s validity. Therefore, it is essential to interpret the results cautiously and consider further research to confirm the results obtained in this systematic review.
Nevertheless, the findings presented in this systematic review lay the groundwork for formulating hypotheses in forthcoming high-caliber studies, as arthroscopic and endoscopic iliopsoas release are proving to be a reliable and productive approach for reducing pain, improving hip flexor function, and avoiding the need for cup revision in patients with symptomatic IPI after THA.
Conclusions
This systematic review demonstrated that arthroscopic and endoscopic iliopsoas tenotomy effectively treat symptoms and improve hip function in patients with IPI after THA. Arthroscopic techniques allow direct visualization of prosthetic components and potential preservation of psoas function, while endoscopic techniques may be more straightforward. Both techniques show promise as alternatives to cup revision surgery. Further research with large-scale prospective randomized studies with carefully selected control groups and standardized protocols is needed to confirm these findings and optimize outcomes.
Data availability
Dataset analyzed in this study is available from the corresponding author on reasonable request.
Code availability
Not applicable.
References
Forster-Horvath C, Egloff C, Valderrabano V, Nowakowski AM (2014) The painful primary hip replacement - review of the literature. Swiss Med Wkly 144:w13974
Jerosch J, Neuhäuser C, Sokkar SM (2013) Arthroscopic treatment of iliopsoas impingement (IPI) after total hip replacement. Arch Orthop Trauma Surg 133(10):1447–1454
Duffy P, Masri BA, Garbuz D, Duncan CP (2006) Evaluation of patients with pain following total hip replacement. Instr Course Lect 55:223–232
Lachiewicz PF, Kauk JR (2009) Anterior iliopsoas impingement and tendinitis after total hip arthroplasty. J Am Acad Orthop Surg 17(6):337–344
Chalmers BP, Sculco PK, Sierra RJ, Trousdale RT, Berry DJ (2017) Iliopsoas impingement after primary total hip arthroplasty: operative and nonoperative treatment outcomes. J Bone Joint Surg Am 99(7):557–564
Postel M (1975) Les prothèses douloureuses [Painful prosthesis. I. possible causes]. Rev Chir Orthop Reparatrice Appar Mot 61(Suppl 2):57–61
Lequesne M, Dang N, Montagne P, Lemoine A, Witvoet J (1991) Le conflit psoas-prothèse totale de hanche [Conflict between psoas and total hip prosthesis]. Rev Rhum Mal Osteoartic 58(9):559–564
Trousdale RT, Cabanela ME, Berry DJ (1995) Anterior iliopsoas impingement after total hip arthroplasty. J Arthroplasty 10(4):546–549
Capogna BM, Shenoy K, Youm T, Stuchin SA (2017) Tendon disorders after total hip arthroplasty: evaluation and management. J Arthroplasty 32(10):3249–3255
Baumgarten KM, McKenzie MJ (2012) Iliopsoas tendon impingement after total hip arthroplasty with use of a large-diameter femoral head: a case report. JBJS Case Connect 2(2):e22
Dora C, Houweling M, Koch P, Sierra RJ (2007) Iliopsoas impingement after total hip replacement: the results of non-operative management, tenotomy or acetabular revision. J Bone Joint Surg Br 89(8):1031–1035
Lazennec JY, Laudet CG, Guérin-Surville H, Roy-Camille R, Saillant G (1997) Dynamic anatomy of the acetabulum: an experimental approach and surgical implications. Surg Radiol Anat 19(1):23–30
Park KK, Tsai TY, Dimitriou D, Kwon YM (2016) Three-dimensional in vivo difference between native acetabular version and acetabular component version influences iliopsoas impingement after total hip arthroplasty. Int Orthop 40(9):1807–1812
Jasani V, Richards P, Wynn-Jones C (2002) Pain related to the psoas muscle after total hip replacement. J Bone Joint Surg Br 84(7):991–993
Della Valle CJ, Rafii M, Jaffe WL (2001) Iliopsoas tendinitis after total hip arthroplasty. J Arthroplasty 16(7):923–926
Rezig R, Copercini M, Montet X, Martinoli C, Bianchi S (2004) Ultrasound diagnosis of anterior iliopsoas impingement in total hip replacement. Skeletal Radiol 33(2):112–116
Cyteval C, Sarrabère MP, Cottin A et al (2003) Iliopsoas impingement on the acetabular component: radiologic and computed tomography findings of a rare hip prosthesis complication in eight cases. J Comput Assist Tomogr 27(2):183–188
Potter HG, Foo LF, Nestor BJ (2005) What is the role of magnetic resonance imaging in the evaluation of total hip arthroplasty? HSS J 1(1):89–93
Nunley RM, Wilson JM, Gilula L, Clohisy JC, Barrack RL, Maloney WJ (2010) Iliopsoas bursa injections can be beneficial for pain after total hip arthroplasty. Clin Orthop Relat Res 468(2):519–526
Fish DE, Chang WS (2007) Treatment of iliopsoas tendinitis after a left total hip arthroplasty with botulinum toxin type A. Pain Physician 10(4):565–571
Buller LT, Menken LG, Hawkins EJ et al (2021) Iliopsoas impingement after direct anterior approach total hip arthroplasty: epidemiology, risk factors, and treatment options. J Arthroplasty 36(5):1772–1778
Ilizaliturri VM Jr, Villalobos FE Jr, Chaidez PA, Valero FS, Aguilera JM (2005) Internal snapping hip syndrome: treatment by endoscopic release of the iliopsoas tendon. Arthroscopy 21(11):1375–1380
Williams M, Ashworth M (2019) An operative technique for psoas impingement following total hip arthroplasty: a case series of day case, extra articular, arthroscopic psoas tenotomy. Arch Orthop Trauma Surg 139(2):211–216
Wettstein M, Jung J, Dienst M (2006) Arthroscopic psoas tenotomy. Arthroscopy 22(8):907.e1-907.e9074
Liberati A, Altman DG, Tetzlaff J et al (2009) The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol 62(10):e1–e34
Burns PB, Rohrich RJ, Chung KC (2011) The levels of evidence and their role in evidence-based medicine. Plast Reconstr Surg 128(1):305–310
Ramponi L, Yasui Y, Murawski CD et al (2017) Lesion size is a predictor of clinical outcomes after bone marrow stimulation for osteochondral lesions of the talus: a systematic review. Am J Sports Med 45(7):1698–1705
Sideri S, Papageorgiou SN, Eliades T (2018) Registration in the international prospective register of systematic reviews (PROSPERO) of systematic review protocols was associated with increased review quality. J Clin Epidemiol 100:103–110
Nikou S, Lindman I, Sigurdsson A et al (2023) Arthroscopic iliopsoas tenotomy after total hip arthroplasty: safe method for the right patient. J Exp Orthop 10(1):3
Tassinari E, Castagnini F, Mariotti F et al (2021) Arthroscopic tendon release for iliopsoas impingement after primary total hip arthroplasty: a retrospective, consecutive series. Hip Int 31(1):125–132
Di Benedetto P, Niccoli G, Magnanelli S et al (2019) Arthroscopic treatment of iliopsoas impingement syndrome after hip arthroplasty. Acta Biomed 90(1-S):104–109
Bonano JC, Pierre K, Jamero C, Segovia NA, Huddleston JI, Safran MR (2023) Endoscopic iliopsoas lengthening for treatment of recalcitrant iliopsoas tendinitis after total hip arthroplasty. J Hip Preserv Surg 10(2):63–68
Amellal O, Lamraski K, Penasse M (2020) Endoscopic iliopsoas tenotomy following total hip replacement: Retrospective study of 19 cases. J Arthros Joint Surg 7(3):131–136
Viamont-Guerra MR, Ramos-Pascual S, Saffarini M, Bonin N (2021) Endoscopic tenotomy for iliopsoas tendinopathy following total hip arthroplasty can relieve pain regardless of acetabular cup overhang or anteversion. Arthroscopy 37(9):2820–2829
Guicherd W, Bonin N, Gicquel T et al (2017) Endoscopic or arthroscopic iliopsoas tenotomy for iliopsoas impingement following total hip replacement. A prospective multicenter 64-case series. Orthop Traumatol Surg Res 103(8S):S207–S214
Finsterwald M, Mancino F, Waters G et al (2024) Endoscopic tendon release for iliopsoas impingement after total hip arthroplasty-excellent clinical outcomes and low failure rates at short-term follow-up. Arthroscopy 40(3):790–798
Valenzuela J, O’Donnell JM (2021) Endoscopic treatment of iliopsoas impingement after total hip arthroplasty: a minimum 2-year follow-up and comparison of tenotomy performed at the acetabular rim versus lesser trochanter. J Hip Preserv Surg 8(1):83–89
Bell CD, Wagner MB, Wang L et al (2019) Evaluation of endoscopic iliopsoas tenotomy for treatment of iliopsoas impingement after total hip arthroplasty. J Arthroplasty 34(7):1498–1501
Moreta J, Cuéllar A, Aguirre U, Casado-Verdugo ÓL, Sánchez A, Cuéllar R (2021) Outside-in arthroscopic psoas release for anterior iliopsoas impingement after primary total hip arthroplasty. Hip Int 31(5):649–655
Zimmerer A, Hauschild M, Nietschke R (2022) Results after arthroscopic treatment of iliopsoas impingement after total hip arthroplasty. Arch Orthop Trauma Surg 142(2):189–195
Gédouin JE, Huten D (2012) Technique and results of endoscopic tenotomy in iliopsoas muscle tendinopathy secondary to total hip replacement: a series of 10 cases. Orthop Traumatol Surg Res 98(4 Suppl):S19–S25
Filanti M, Carubbi C, Del Piccolo N, Rani N, Mazzotta A, Dallari D (2016) The role of arthroscopy in the treatment of groin pain after total hip arthroplasty: our experience. Hip Int 26(Suppl 1):28–33
Brandenburg JB, Kapron AL, Wylie JD, Wilkinson BG, Maak TG, Gonzalez CD, Aoki SK (2016) The Functional and Structural Outcomes of Arthroscopic Iliopsoas Release. Am J Sports Med 44(5):1286–1291
Contreras MEK, Dani WS, Endges WK, De Araujo LCT, Berral FJ (2010) Arthroscopic treatment of the snapping iliopsoas tendon through the central compartment of the hip. J Bone Joint Surg Br 92-B(6):777–780
Anderson SA, Keene JS (2008) Results of arthroscopic iliopsoas tendon release in competitive and recreational athletes. Am J Sports Med 36(12):2363–2371
Márquez Arabia WH, Gómez-Hoyos J, Llano Serna JF et al (2013) Regrowth of the psoas tendon after arthroscopic tenotomy: a magnetic resonance imaging study. Arthroscopy 29(8):1308–1313
Funding
Open access funding provided by Università degli Studi di Palermo within the CRUI-CARE Agreement. There is no funding source.
Author information
Authors and Affiliations
Contributions
RGV, AE, and AD have contributed substantially to conception and design, data acquisition, analysis, and interpretation. They have been involved in drafting the manuscript and revising it critically for important intellectual content, given final approval of the version to be published. They agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved, SDV and MG have contributed substantially to the data analysis, interpretation, and manuscript drafting. FB and AM has made substantial contributions to the concept and design of the manuscript and revising it critically for important intellectual content.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Giai Via, R., Giachino, M., Elzeiny, A. et al. Arthroscopic and endoscopic techniques for iliopsoas release in THA are safe and effective: a systematic review of the literature. Eur J Orthop Surg Traumatol (2024). https://doi.org/10.1007/s00590-024-04042-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s00590-024-04042-1