
Abstract
Purpose
The association between idiopathic scoliosis (IS) and sports activities remains vague. We aimed to analyse their effect on full-time braced adolescents with IS.
Methods
We retrospectively recruited all the consecutive patients of a tertiary referral Institute of age ≥ 10 (adolescents), with a juvenile (JIS) or adolescent (AIS) IS diagnosis, Risser 0–2, TLSO brace prescription and self-reported adherence ≥ 20 h per day, and follow-up out-of-brace X-rays 18 months after brace prescription. We divided participants into two groups: SPORT (sport twice or more per week) and CONTROL (sport once per week or less). We calculated odds ratio (OR) to compare the outcome of subjects performing to those not performing sport. We ran a logistic regression with covariate adjustment to assess if sports frequency affected the outcomes.
Results
Out of 33,311 participants assessed for eligibility, 785 satisfied the inclusion criteria (693 females, age 12.7 ± 1.3 and 40 ± 11° Cobb). The SPORT group consisted of 290 participants and the CONTROL group of 495. The SPORT group showed higher odds of improvement (OR = 1.59, 95%CI = 1.17–2.16, p = 0.0018). The odds of improving increased with the frequency of sports activity (OR = 1.20, 95%CI 1.08–1.34).
Conclusion
This study shows that sports activities increase the odds of improvement at 18-month follow-up in adolescents with IS treated with a full-time brace. The odds of improvement increase with sports week frequency.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Scoliosis is a general term comprising a heterogeneous group of conditions consisting of changes in the shape and position of the spine, thorax and trunk [1]. By definition, idiopathic scoliosis (IS) is of unknown origin and is probably due to several causes [1]. The Scoliosis Research Society (SRS) suggests that the diagnosis is confirmed when the Cobb angle is 10° or higher and axial rotation can be recognised [2]. According to current evidence, adolescent idiopathic scoliosis (AIS) non-operative treatments include Physiotherapic Scoliosis Specific Exercises (PSSE) [3,4,5] and/or bracing [6, 7] according to curve severity and risk of progression [1].
Conservative treatment with rigid bracing and PSSE is recommended for curve angles above 20–25° Cobb in skeletally immature patients [1]. Bracing treatment involves using a brace (a corrective orthosis) for a specified time each day, usually until maturity [1]. Several studies verified the efficacy of brace treatment in preventing curve progression [6, 8].
In children and adolescents, there is a dose–response relation between physical activity, sedentary behaviour and health-related quality of life. Results suggest that the higher frequency of physical activity or the less sedentary time, the better the health-related quality of life [9]. The International Society on Scoliosis Orthopaedic and Rehabilitation Treatment (SOSORT) guidelines for the conservative treatment of scoliosis recommends continuing sports activities during brace treatment because of the physical and psychological benefits these activities provide [1]. However, there is an apparent discrepancy between the two: the brace immobilises the spine to prevent scoliosis progression, while sports activities require spine movements in all directions. For these reasons, all around the world, there are some physicians prescribing sport and others interdicting sport to braced adolescents. The primary aim of this study was to determine if sports activities can modify the therapy results of adolescents with IS wearing a full-time brace. The secondary aim was to verify if sports weekly frequency can increase or reduce the odds of improving in this population. [10–22]
Materials and methods
The study is a retrospective observational case–control study embedded in a prospective clinical data collection in a tertiary referral outpatient Institute in Italy specialised in spinal disorders. The local ethics committee approved the study, and all patients and their parents gave informed consent for research purposes. This study did not receive any external funding.
Participants
We considered all consecutive patients from 2003 up to 31 October 2018. Inclusion criteria were adolescents with IS (age ≥ ten years), diagnosis of JIS or AIS according to the criteria of the Society on Scoliosis Orthopaedic and Rehabilitation Treatment (SOSORT) [1], Risser stage between 0 and 2, thoraco-lumbosacral brace (TLSO) full-time prescription with a self-reported brace usage ≥ 20 h/day during the follow-up, frontal X-rays available at baseline and 18-month follow-up. We excluded patients with deformities associated with neurological or congenital pathologies.
Treatments
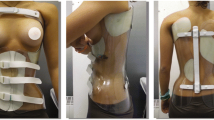
The braces included were TLSOs (Sforzesco or Sibilla-Cheneau) built according to SPoRT (Symmetric, Patient-oriented, Rigid, Three-dimensional, active) concept [23]. The SPoRT concept, due to its three-dimensional action of elongation pushing the spine in a down-up direction, is different from all the other corrective systems. The Sforzesco brace is a high rigidity brace constructed with high-density polyethylene, and the Sibilla-Cheneau brace is a rigid one made of polyethylene. The Sforzesco brace was prescribed to patients with more severe and structured curves.
At every consultation (every six months), full-time brace and PSSE were prescribed. We considered regular PSSE if performed ≥ 90 min a week. Finally, we prescribed participants regular sports activity, to help them psychologically and socially and develop better self-image [1].
Data sources/measurements
At each consultation, the treating physician collected all the data: weight, height, age, and angle of trunk rotation (ATR). Furthermore, participants self-reported how many hours a day they wore the brace if they practised regular physical activity, which sport, and how many times per week. All participants underwent a standing anteroposterior X-ray of the full spine at baseline, 6- and 18-month follow-ups The treating physician measured the X-rays using the Cobb method [1]. Table 1 shows all the data collected and their timing. The primary outcome was an improvement of ≥ 5° Cobb at the 18-month follow-up X-ray.
Data analysis
The sport variable
Patients self-reported if they had performed sports activity. If they did, they also reported which one, the weekly frequency, and the minutes per week. We considered only extra-curricular sport because in Italy all children perform 2 h a week of physical activity at school. Participants could perform sports activity wearing or not their brace, according to their preference and hours/day of brace wearing.
Since not all patients performed sports regularly, we divided the sports variable into two groups for the logistic regression analysis: SPORT group, if they practised regular sports twice or more per week during the entire follow-up period (18 months), and CONTROL group, if they practised sports activity only once or less per week, or not regularly with breaks of weeks or months.
Statistical analysis
The Wilcoxon rank-sum test and chi-square test were used to verify if there were differences between SPORT and CONTROL groups. The odds ratio (OR) was calculated to compare the outcome of three groups at 18-month follow-up. Binary logistic regression was used to verify the impact of the following covariates: JIS diagnosis, baseline age, Cobb degrees, Risser sign, and angle of trunk rotation (ATR). Logistic regression with covariate adjustment was run to assess if the frequency of the sport per week influenced the outcome measures. Stratification was applied to control covariates. The alpha level was set at 0.05 and CI at 95%. All statistical analyses were conducted using the Stata statistical package (version 14; Stata Corp).
Results
We included 785 patients (mean age 12.7 ± 1.3, 693 females) whose baseline characteristics are listed in Table 2. At each cross-sectional observation time, we had almost 50% of patients performing sport: 51.2% at six months, 53.5% at 12 months and 55.9% at 18 months, respectively. At the 18-month follow-up, SPORT group had 290 patients (36.9%) who never stopped sports activities from baseline to follow-up. We considered patients performing PSSE if they reported regular performance ≥ 90 min per week throughout the follow-up. At the baseline, we did not find significant differences between the groups in any variable considered (sex, age, Cobb degrees, Risser sign, ATR, JIS, PSSE). At the 18-month follow-up, subjects performing sport showed higher odds of improvement (OR = 1.59, 95%CI = 1.17–2.16, p = 0.0018).
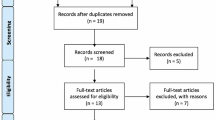
According to logistic regression, after adjusting for covariates, at the 18-month follow-up only ATR, sports activity, and sports frequency significantly increased the odds of improvement (p = 0.009, p = 0.009, p = 0.001, respectively). As baseline ATR increased, the odds of improvement decreased (OR = 0.95, 95%CI 0.91–0.98), and the odds of improvement increased with sports frequency (OR = 1.20, 95%CI 1.08–1.34) Fig. 1.

The flow chart of participants
Discussion
This is the first extensive prospective study to check the effect of sports activities on a large population of adolescents with IS, wearing a TLSO brace full time. The study shows that in this population, regular sports activity increases the odds of reducing scoliosis ≥ 5° Cobb at an 18-month follow-up and the odds of improvement increase with sports frequency. Clinical guidelines suggest performing sports activities when wearing a brace for psychological and social benefits [1]. According to current results, regular sports activity can also help scoliosis treatment within 18 months of observation.
Previous studies focused on various types of sports. They investigated the prevalence of scoliosis or trunk asymmetries in athletes performing specific sports such as swimming [11, 12], tennis [13, 14], ballet [15, 16], volleyball [17, 18], rhythmic [19] or artistic gymnastics [14, 20], wrestling [14], and soccer [14], and comparing them with data from normal controls. They found controversial relationships between specific sports and spine deformities or trunk asymmetries. Some studies found an association between swimming and trunk asymmetries [11, 12] but not Boldori and Bielec [21, 22]. MacMaster [23] found that subjects who never performed gymnastics had 5.1 times the odds of having AIS than those who participated in these activities. Conversely, Hellstrom [14] and Trexler [20] found a higher prevalence of scoliosis in gymnasts. Most of these studies have a cross-sectional design that does not allow drawing a cause-effect relationship. Furthermore, no study included patients with IS wearing a brace full time to determine the effect of sports activities on therapy.
Our study confirms that it is possible to undergo bracing treatment and continue practising sport. At all follow-ups, we had cross-sectionally almost 50% of our sample regularly practising sports activity. This result is consistent with a study that showed that bracing does not change sports habits of AIS patients wearing a TLSO brace 18–23 h a day: 51.3% of patients performed sports at baseline and 49.9% at the 6-month follow-up [24]. In our study, considering the entire 18-month follow-up, patients performing sports reduced to 36.9%. Nevertheless, this percentage includes only patients regularly performing sports during the whole period.
In most studies investigating the prevalence of scoliosis or trunk asymmetries in competitive athletes or professional dancers, subjects engaged in high-intensity training presented more frequently trunk asymmetries and scoliosis than controls [11, 12, 14, 15, 19, 20]. Athletes performing low-intensity sports activity showed the opposite trend [13, 21, 22]. These data contrast our study’s results of full-time braced adolescents showing an increase in the odds of improvement with the rise of sports frequency. The case–control design within a prospective database versus cross-sectional data can explain the difference and favours our observation.
Combining bracing with PSSE has decreased spinal deformities and improved quality of life compared to bracing alone [8, 25,26,27]. In our study, 52% of the population had been regularly performing PSSE throughout the follow-up period. However, we found no statistically significant differences in the percentage of patients regularly performing PSSE between SPORT and CONTROL groups.
The significant variability of sports did not allow us to reach conclusions on the various types of sports. When we tried to divide the patients, there were too many variables. Some patients started with one sport for the first six months and then changed; others played more sports simultaneously. Some practised sports activities up to 7 times a week but not agonistic because they played 3–4 different sports. All this variability did not allow us to reach conclusions on the matter. Still, it would be interesting to try to analyse them in the future with other studies on larger populations.
One of the main limitations of the current study is that the physicians interviewed patients only about the type of sport they played and the weekly frequency. Still, they did not ask the number of hours dedicated to sport at each session. Activity strength such as duration and intensity was not reported, and these factors might impact more than times per week and should be explored in future studies. Another limit is that the study relies entirely on the patients’ reports during the visit. Some of them may have answered to obtain doctor approval. However, the patients knew that the therapy priorities were adherence to brace wear and PSSE, not sports activities. Per our experience, patients feel free to declare if they perform physical activities or not.
Lastly, doctors measured X-rays not blindly to patients’ participation in sports activities. Nevertheless, they were blind to the study due to the case–control retrospective design. Moreover, doctors prescribe sports activity to the patients because it could help them prevent trunk muscle impairment, reduce trunk stiffness, improve lung function, and help them maintain their social life. Until now, sports activity could not be expected to enhance treatment results. Consequently, the allocation to SPORT or CONTROL group should probably not have influenced Cobb degrees measurement.
The merits of the present study include the prospective data collection of all consecutive patients corresponding to the inclusion criteria, the large sample size, and the focus on a specific population (patients wearing a full-time TLSO brace) with meaningful clinical outcome criteria. All this provides good reliability and generalisability of results, decreasing the risk for type I error (increasing the power of the study). Our study can serve in planning future interventional trials with a prospective design that could reduce our observed variability. Moreover, future studies could look at the sagittal plane too. We could not do so because of the absence of lateral X-rays in most patients and the observational retrospective design.
In conclusion, this study shows that regular sports activity performance increases the odds of improvement at 18-month follow-up in adolescents with IS treated with a full-time brace. The odds of improvement increase with the increase in sport’s frequency. According to the present results, regular sports activity can be recommended by physicians, thus confirming the recommendation of the clinical guidelines on conservative scoliosis treatment [1]. Future studies with different designs should check individual sports and the combined effect of PSSEs and sports activities.
Availability of data and material
data are available at https://zenodo.org/record/5896952#.Ye57kP7MI2w.
References
Negrini S, Donzelli S, Aulisa AG et al (2018) 2016 SOSORT guidelines: orthopaedic and rehabilitation treatment of idiopathic scoliosis during growth. Scoliosis Spinal Disord. https://doi.org/10.1186/s13013-017-0145-8
Negrini S, Aulisa AG, Aulisa L et al (2012) 2011 SOSORT guidelines: Orthopaedic and Rehabilitation treatment of idiopathic scoliosis during growth. Scoliosis 7:3. https://doi.org/10.1186/1748-7161-7-3
Monticone M, Ambrosini E, Cazzaniga D et al (2014) Active self-correction and task-oriented exercises reduce spinal deformity and improve quality of life in subjects with mild adolescent idiopathic scoliosis. Results of a randomised controlled trial. Eur Spine J 23:1204–1214. https://doi.org/10.1007/s00586-014-3241-y
Romano M, Minozzi S, Zaina F et al (2013) Exercises for adolescent idiopathic scoliosis: a Cochrane systematic review. Spine 38:E883-893. https://doi.org/10.1097/BRS.0b013e31829459f8
Negrini S, Donzelli S, Negrini A et al (2018) Specific exercises reduce the need for bracing in adolescents with idiopathic scoliosis: a practical clinical trial. Ann Phys Rehabil Med. https://doi.org/10.1016/j.rehab.2018.07.010
Weinstein SL, Dolan LA, Wright JG, Dobbs MB (2013) Effects of Bracing in Adolescents with Idiopathic Scoliosis. N Engl J Med 369:1512–1521. https://doi.org/10.1056/NEJMoa1307337
Negrini S, Minozzi S, Bettany-Saltikov J, et al (2015) Braces for idiopathic scoliosis in adolescents. Cochrane Database Syst Rev 6:CD006850. https://doi.org/10.1002/14651858.CD006850.pub3
Negrini S, Donzelli S, Lusini M et al (2014) The effectiveness of combined bracing and exercise in adolescent idiopathic scoliosis based on SRS and SOSORT criteria: a prospective study. BMC Musculoskelet Disord 15:263. https://doi.org/10.1186/1471-2474-15-263
Wu XY, Han LH, Zhang JH et al (2017) The influence of physical activity, sedentary behavior on health-related quality of life among the general population of children and adolescents: A systematic review. PLoS ONE 12:e0187668. https://doi.org/10.1371/journal.pone.0187668
Negrini S, Hresko TM, O’Brien JP et al (2015) Recommendations for research studies on treatment of idiopathic scoliosis: Consensus 2014 between SOSORT and SRS non-operative management committee. Scoliosis 10:8. https://doi.org/10.1186/s13013-014-0025-4
Kenanidis EI, Potoupnis ME, Papavasiliou KA et al (2010) Adolescent idiopathic scoliosis in athletes: is there a connection? Phys Sportsmed 38:165–170. https://doi.org/10.3810/psm.2010.06.1795
Watanabe K, Michikawa T, Yonezawa I et al (2017) Physical Activities and Lifestyle Factors Related to Adolescent Idiopathic Scoliosis. J Bone Joint Surg Am 99:284–294. https://doi.org/10.2106/JBJS.16.00459
Warren MP, Brooks-Gunn J, Hamilton LH et al (1986) Scoliosis and fractures in young ballet dancers. Relation to delayed menarche and secondary amenorrhea. N Engl J Med 314:1348–1353. https://doi.org/10.1056/NEJM198605223142104
Longworth B, Fary R, Hopper D (2014) Prevalence and predictors of adolescent idiopathic scoliosis in adolescent ballet dancers. Arch Phys Med Rehabil 95:1725–1730. https://doi.org/10.1016/j.apmr.2014.02.027
Tanchev PI, Dzherov AD, Parushev AD, et al (2000) Scoliosis in rhythmic gymnasts. Spine (Phila Pa 1976) 25:1367–1372. https://doi.org/10.1097/00007632-200006010-00008
Becker TJ (1986) Scoliosis in swimmers. Clin Sports Med 5:149–158
Zaina F, Donzelli S, Lusini M et al (2015) Swimming and spinal deformities: a cross-sectional study. J Pediatr 166:163–167. https://doi.org/10.1016/j.jpeds.2014.09.024
Hellström M, Jacobsson B, Swärd L, Peterson L (1990) Radiologic abnormalities of the thoraco-lumbar spine in athletes. Acta Radiol 31:127–132
Negrini S, Minozzi S, Bettany-Saltikov J, et al (2015) Braces for idiopathic scoliosis in adolescents. Cochrane Database Syst Rev CD006850. https://doi.org/10.1002/14651858.CD006850.pub3
Negrini S, Donzelli S, Negrini F et al (2012) Bracing does not change the sport habits of patients. Stud Health Technol Inform 176:437–440
Rivett L, Rothberg A, Stewart A, Berkowitz R (2009) The relationship between quality of life and compliance to a brace protocol in adolescents with idiopathic scoliosis: a comparative study. BMC Musculoskelet Disord 10:5. https://doi.org/10.1186/1471-2474-10-5
Romano M, Minozzi S, Zaina F, et al (2013) Exercises for adolescent idiopathic scoliosis: a Cochrane systematic review. Spine (Phila Pa 1976) 38:E883–893. https://doi.org/10.1097/BRS.0b013e31829459f8
Negrini S, Marchini G, Tessadri F (2011) Brace technology thematic series - The Sforzesco and Sibilla braces, and the SPoRT (Symmetric, Patient oriented, Rigid, Three-dimensional, active) concept. Scoliosis 6:8. https://doi.org/10.1186/1748-7161-6-8
Atanasio S, Zaina F, Negrini S (2008) The Sforzesco brace and SPoRT concept: a brace to replace cast in worst curves. Disabil Rehabil Assist Technol 3:154–160. https://doi.org/10.1080/17483100801905843
Tobias JH, Fairbank J, Harding I et al (2019) Association between physical activity and scoliosis: a prospective cohort study. Int J Epidemiol 48:1152–1160. https://doi.org/10.1093/ije/dyy268
Romano M, Negrini A, Parzini S et al (2015) SEAS (Scientific Exercises Approach to Scoliosis): a modern and effective evidence based approach to physiotherapic specific scoliosis exercises. Scoliosis 10:3. https://doi.org/10.1186/s13013-014-0027-2
Negrini S, Donzelli S, Negrini A et al (2019) Specific exercises reduce the need for bracing in adolescents with idiopathic scoliosis: A practical clinical trial. Ann Phys Rehabil Med 62:69–76. https://doi.org/10.1016/j.rehab.2018.07.010
Acknowledgements
This study was supported and funded by the Italian Ministry of Health - Ricerca Corrente 2022. We thank Alberto Negrini and the ISICO software team for the conception, development, and maintenance of the program for data collection and extraction.
Funding
Open access funding provided by Università degli Studi di Milano within the CRUI-CARE Agreement. The authors did not receive support from any organisation for the submitted work.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
SN, AN, and RM own stock from ISICO, and the other authors have no relevant financial or non-financial interests to disclose.
Consent to participate
All parents provided written consent to an anonymous retrospective analysis of their children’s clinical data.
Ethics approval
The local Ethics Committee provided consent to the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Negrini, A., Poggio, M., Donzelli, S. et al. Sport improved medium-term results in a prospective cohort of 785 adolescents with idiopathic scoliosis braced full time. SOSORT 2018 award winner. Eur Spine J 31, 2994–2999 (2022). https://doi.org/10.1007/s00586-022-07370-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-022-07370-0