
Abstract
Purpose
Electroshock wave lithotripsy (ESWL) is a painful procedure performed with sedoanalgesia in paediatric patients. The propofol–ketamine combination may be the preferable anaesthesia for this procedure, and propofol–ketamine consumption may be decreased with the administration of intravenous (IV) paracetamol. In this study we investigated the effect of IV paracetamol administration on propofol–ketamine consumption, recovery time and frequency of adverse events in paediatric patients undergoing ESWL.
Methods
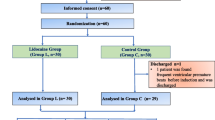
Sixty children, ranging in age from 1 to 10 years and with American Society of Anesthesiologists Physical Status 1–2, were included in this prospective, randomized, double-blinded study. Thirty minutes prior to the procedure children randomly assigned to Group I received IV 15 mg/kg paracetamol, and those randomly assigned to Group II received 1.5 mL/kg IV saline infusion 30 min. The propofol–ketamine combination was prepared by mixing 25 mg propofol and 25 mg ketamine in a total 10 mL solution in the same syringe. After the administration of 0.1 mg/kg midazolam and 10 μg/kg atropine to both groups and during the procedure, the propofol–ketamine combination was administered at 0.5 mg/kg doses to achieve a Wisconsin sedation score of 1 or 2. Oxygen saturation and heart rate were recorded at 5-min intervals. Propofol–ketamine consumption, recovery times and adverse events were also recorded.
Results
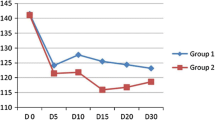
Demographic data were similar between groups. Propofol–ketamine consumption (Group I, 25.2 ± 17.7 mg; Group II, 35.4 ± 20.1 mg; p = 0.04) and recovery times (Group I, 19.4 ± 7.9 min; Group II, 29.6 ± 11.4 min; p < 0.0001) were significantly different between groups. Saturation, heart rate and adverse events were similar in both groups.
Conclusion
Our data suggest that the administration of IV paracetamol decreases propofol–ketamine consumption for adequate sedation during ESWL procedures in paediatric patients and shortens recovery time.


Similar content being viewed by others
References
Koruk S, Mizrak A, Gul R, Kilic E, Yendi F, Oner U. Dexmedetomidine–ketamine and midazolam–ketamine combinations for sedation in pediatric patients undergoing extracorporeal shock wave lithotripsy: a randomized prospective study. J Anesth. 2010;24:858–63.
Gozal D, Gozal Y. Pediatric sedation/anesthesia outside the operating room. Curr Opin Anaesthesiol. 2008;21(4):494–8.
Neuhäuser C, Wagner B, Heckmann M, Weigand MA, Zimmer KP. Analgesia and sedation for painful interventions in children and adolescents. Dtsch Arztebl Int. 2010;107(14):241–7
Davis PJ, Cook DR. Clinical pharmacokinetics of the newer intravenous anaesthetic agents. Clin Pharmacokinet. 1986;11(1):18–35.
Slavik VC, Zed PJ. Combination ketamine and propofol for procedural sedation and analgesia. Pharmacotherapy. 2007;27(11):1588–98.
Graham GG, Scott KF. Mechanism of action of paracetamol. Am J Ther. 2005;12(1):46–55.
Oscier CD, Milner QJW. Peri-operative use of paracetamol. Anaesthesia. 2009;64(1):65–72.
Lowrie L, Weiss AH, Lacombe C. The pediatric sedation unit: a mechanism for pediatric sedation. Pediatrics. 1998;102(3):E30.
Akin A, Esmaoglu A, Tosun Z, Gulcu N, Aydogan H, Boyaci A. Comparison of propofol with propofol–ketamine combination in pediatric patients undergoing auditory brainstem response testing. Int J Pediatr Otorhinolaryngol. 2005;69(11):1541–5.
Tosun Z, Esmaoglu A, Coruh A. Propofol–ketamine vs propofol–fentanyl combinations for deep sedation and analgesia in pediatric patients undergoing burn dressing changes. Paediatr Anaesth. 2008;18(1):43–7.
Badrinath S, Avramov MN, Shadrick M, Witt TR, Ivankovich AD. The use of a ketamine–propofol combination during monitored anesthesia care. Anesth Analg. 2000;90(4):858–62.
Çok OY, Eker HE, İzmirli H, Arıboğan A, Arslan G. Endoskopik Retrograd Kolanjiopankreatografide sedasyon: propofol ve ketamin karışım infüzyonunun aralıklı bolus uygulamaları ile karlaşılaştırılması. Anestezi Dergisi. 2009;17(1):49–54.
Coté CJ, Karl HW, Notterman DA, Weinberg JA, McCloskey C. Adverse sedation events in pediatrics: analysis of medications used for sedation. Pediatrics. 2000;106(4):633–44.
Willman EV, Andolfatto G. A prospective evaluation of “ketofol” (ketamine/propofol combination) for procedural sedation and analgesia in the emergency department. Ann Emerg Med. 2007;49(1):23–30.
Mortero RF, Clark LD, Tolan MM, Metz RJ, Tsueda K, Sheppard RA. The effects of small-dose ketamine on propofol sedation: respiration, postoperative mood, perception, cognition, and pain. Anesth Analg. 2001;92(6):1465–9.
Pickering G, Loriot MA, Libert F, Eschalier A, Beaune P, Dubray C. Analgesic effect of acetaminophen in humans: first evidence of a central serotonergic mechanism. Clin Pharmacol Ther. 2006;79(4):371–8.
Memis D, Inal MT, Kavalci G, Sezer A, Sut N. Intravenous paracetamol reduced the use of opioids, extubation time, and opioid-related adverse effects after major surgery in intensive care unit. J Crit Care. 2010;25(3):458–62.
Bannwarth B, Péhourcq F. Pharmacologic basis for using paracetamol: pharmacokinetic and pharmacodynamic issues. Drugs 2003;63(Spec No 2):5–13.
Kaygusuz K, Gokce G, Gursoy S, Ayan S, Mimaroglu C, Gultekin Y. A comparison of sedation with dexmedetomidine or propofol during shockwave lithotripsy: a randomized controlled trial. Anesth Analg. 2008;106(1):114–9 (table of contents).
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
About this article
Cite this article
Eker, H.E., Çok, O.Y., Ergenoğlu, P. et al. IV paracetamol effect on propofol–ketamine consumption in paediatric patients undergoing ESWL. J Anesth 26, 351–356 (2012). https://doi.org/10.1007/s00540-012-1335-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00540-012-1335-4