
Abstract
Background
Fibroblast growth factor 23 (FGF23) is a bone-derived hormone that plays a central role in chronic kidney disease-mineral bone disorder and is associated with CKD progression and cardiovascular morbidity. Factors related to CKD-associated anemia, including iron deficiency, can increase FGF23 production. This study aimed to assess whether anemia and/or iron deficiency are associated with increased circulating concentrations of FGF23 in the large, well-characterized Chronic Kidney Disease in Children (CKiD) study cohort.
Methods
Hemoglobin concentrations, iron parameters, C-terminal (total) FGF23, intact FGF23, and relevant covariables were measured in cross-sectional analysis of CKiD study subjects.
Results
In 493 pediatric patients with CKD (median [interquartile range] age 13 [9, 16] years), the median estimated glomerular filtration rate was 48 [35, 61] ml/min/1.73 m2, and 103 patients (21%) were anemic. Anemic subjects had higher total FGF23 concentrations than non-anemic subjects (204 [124, 390] vs. 109 [77, 168] RU/ml, p < 0.001). In multivariable linear regression modeling, anemia was independently associated with higher total FGF23, after adjustment for demographic, kidney-related, mineral metabolism, and inflammatory covariables (standardized β (95% confidence interval) 0.10 (0.04, 0.17), p = 0.002). In the subset of subjects with available iron parameters (n = 191), iron deficiency was not associated with significantly higher total FGF23 concentrations. In the subgroup that had measurements of both total and intact FGF23 (n = 185), in fully adjusted models, anemia was significantly associated with higher total FGF23 (standardized β (95% CI) 0.16 (0.04, 0.27), p = 0.008) but not intact FGF23 (standardized β (95% CI) 0.02 (−0.12, 0.15), p = 0.81).
Conclusions
In this cohort of pediatric patients with CKD, anemia was associated with increased total FGF23 levels but was not independently associated with elevated intact FGF23, suggesting possible effects on both FGF23 production and cleavage. Further studies are warranted to investigate non-mineral factors affecting FGF23 production and metabolism in CKD.
Graphical abstract

A higher resolution version of the Graphical abstract is available as Supplementary information
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Fibroblast growth factor 23 (FGF23) is an important hormone implicated in the pathogenesis of chronic kidney disease-mineral bone disorder (CKD-MBD). FGF23 is secreted predominantly by osteocytes to regulate phosphate and 1,25-dihydroxyvitamin D. In the early stages of CKD, bone [1] and circulating [2,3,4,5] FGF23 levels increase, and continue to rise as CKD progresses and glomerular filtration rate declines. Although increases in FGF23 help to maintain normophosphatemia until late in the course of CKD [2, 5], FGF23-induced suppression of 1,25-dihydroxyvitamin D contributes to secondary hyperparathyroidism.
Moreover, high levels of FGF23 have been associated with various adverse events in patients with CKD. In adult [6, 7] and pediatric [8] patients with CKD, higher circulating concentrations of FGF23 are associated with disease progression. Additionally, elevated FGF23 levels in CKD may contribute to cardiovascular morbidity. Pre-clinical in vitro and in vivo studies have demonstrated that FGF23 can directly induce cardiomyocyte hypertrophy [9]. In adult [9, 10] and pediatric [11] patients with CKD, higher circulating concentrations of FGF23 are associated with increased left ventricular mass. Lastly, in CKD, elevated FGF23 levels are associated with impaired neutrophil activation [12] and infection-related morbidity [13]. Potentially due to these multisystemic adverse effects, higher FGF23 levels in CKD are independently associated with increased overall mortality rates [7, 9, 10, 14].
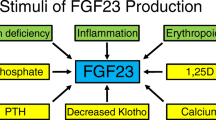
In the setting of CKD, various factors may contribute to increased FGF23 levels. Mineral metabolism factors, including phosphate and 1,25-dihydroxyvitamin D, are well-known stimuli of FGF23 production. Recently, however, novel, non-mineral stimuli of FGF23 production have been identified [15]. Specifically, anemia-related factors have been shown to increase FGF23 production, including iron deficiency [16,17,18,19], which is common in adult [20] and pediatric [21] CKD, and increased erythropoietin [22,23,24,25,26,27], levels of which increase in response to decreasing hemoglobin concentrations in mild–moderate CKD [28]. In the present study, we sought to evaluate how contributory anemia is to elevated FGF23 levels in a cohort of pediatric patients with CKD, hypothesizing that anemia is associated with increased circulating FGF23 concentrations.
Methods
Study design and participants
A retrospective, observational, cross-sectional study was performed which included 493 pediatric subjects from the multicenter Chronic Kidney Disease in Children (CKiD) Cohort Study. The CKiD study is an observational cohort study of children aged 6 months to 16 years with CKD. Enrollment began in January 2005. Complete details of the CKiD study design and methods have been published [29]. The CKiD study was approved by the institutional review board of each participating institution. Written informed consent and assent, when appropriate, was obtained from all parents/legal guardians of the enrolled study subjects.
Predictor variable
The predictor variable was the presence vs. absence of anemia, as defined by hemoglobin concentration thresholds listed in the 2012 KDIGO guidelines for pediatric patients with CKD (Supplemental Table 1) [30], independent of erythropoiesis-stimulating agent (ESA) usage. Also, given that normal hemoglobin concentrations vary by age within the pediatric population, we used published normative data to calculate hemoglobin standard deviation scores (SDS) for age [31].
Outcome variables
The outcome variable of interest was plasma FGF23, as measured with the C-terminal (total) FGF23 ELISA kit (Immutopics) and obtained concurrently with hemoglobin concentrations. Due to non-normal data distribution, FGF23 concentrations were log-transformed prior to analysis. Also, given that normal concentrations of total FGF23 vary by age within the pediatric population, we used published normative data to calculate total FGF23 standard deviation scores (SDS) for age [32]. A subset of patients also had FGF23 measured with the intact FGF23 ELISA kit (Immutopics). Whereas the total FGF23 assay detects both full-length, intact FGF23 and C-terminal FGF23 proteolytic fragments, the intact FGF23 assay detects only the full-length form (Supplemental Fig. 1).
Covariables
Covariables were obtained concurrently with the predictor and outcome variables, and included demographic parameters (age, sex, race, ethnicity); kidney-related factors (CKD duration, glomerular vs. non-glomerular etiology of CKD, estimated glomerular filtration rate (eGFR, calculated using the CKiD under 25 (U25) GFR estimating equations [33])); C-reactive protein (CRP); ESA usage; iron supplementation; mineral metabolism parameters (serum calcium, phosphate, and parathyroid hormone (PTH); use of phosphate binder medications, use of native vitamin D (25D), and use of active vitamin D (1,25D)); and the presence vs. absence of iron deficiency. Given that normal concentrations of serum phosphate vary by age within the pediatric population, we used published normative data to calculate phosphate standard deviation scores (SDS) for age [34]. Measures of iron status, available in a subset of patients, included serum iron, total iron binding capacity (TIBC), transferrin saturation (TSAT), and ferritin. Consistent with the 2012 KDIGO guidelines for pediatric patients with CKD, iron deficiency was defined as TSAT ≤ 20% [30]. A concurrent serum ferritin concentration of ≤ 100 ng/ml or > 100 ng/ml defined absolute iron deficiency and “functional” iron deficiency, respectively.
Statistical analysis
A cross-sectional analysis was performed that included 493 subjects who had both hemoglobin and plasma total FGF23 measured concurrently. Descriptive statistics are expressed as numbers and percentages for categorical variables, and as medians and interquartile ranges (IQR) for continuous variables. Comparisons between groups were made using Chi-square tests (or Fisher exact tests, when appropriate) and Mann–Whitney U tests, for categorical and continuous variables, respectively. Univariable and multivariable linear regression analysis was used to evaluate associations between independent variables, including the presence vs. absence of anemia, and the dependent variable of log-transformed total FGF23. GraphPad Prism 10.0.1 was used for statistical analysis, with P-values < 0.05 considered statistically significant.
Results
Cohort characteristics
The cohort included 493 pediatric patients with CKD, with a median (IQR) age of 13 (9, 16) years and a median eGFR of 48 (35, 61) ml/min/1.73 m2 (Table 1). The median hemoglobin concentration was 13.1 (12.1, 14.1) g/dl, with a median hemoglobin SDS for age of −0.9 (−2.0, 0.1). The median C-terminal (total) FGF23 concentration was 118 (82, 204) RU/ml, with a median total FGF23 SDS for age of 1.6 (0.5, 3.6).
Study subjects with and without anemia
In this cohort, 103 participants (21%) were anemic. Compared to subjects without anemia, those with anemia had a lower median (IQR) eGFR (32 [21, 44] vs. 51 [40, 65] ml/min/1.73 m2, p < 0.001), a higher median phosphate SDS for age (−0.5 [−1.3, 0.7] vs. −0.8 [−1.5, −0.2], p < 0.001), a higher median total FGF23 concentration (204 [124, 390] vs. 109 [77, 168] RU/ml, p < 0.001), and a higher median total FGF23 SDS for age (3.5 [1.6, 6.6] vs. 1.3 [0.4, 2.8], p < 0.001) (Table 2). Across CKD stages and eGFR quartiles, anemic subjects generally had higher total FGF23 levels than non-anemic subjects, although statistical significance was not reached in all stages or quartiles (Supplemental Table 2).
Study subjects with and without ESA use
In this cohort, 53 participants (11%) were treated with ESAs. Compared to untreated subjects, those receiving ESAs had a lower median (IQR) eGFR (29 [20, 39] vs. 50 [38, 63] ml/min/1.73 m2, p < 0.001), a higher prevalence of anemia (51% vs. 17%, p < 0.001), a higher median total FGF23 concentration (254 [129, 459] vs. 113 [79, 184] RU/ml, p < 0.001), and a higher median total FGF23 SDS for age (4.3 [1.9, 7.2] vs. 1.4 [0.4, 3.4], p < 0.001) (Table 3).
Study subjects with and without iron deficiency
A subset of the cohort (n = 191) had iron parameters measured (Table 4). In this subset, 67 participants (35%) were iron deficient, as defined by a TSAT ≤ 20%. Almost all of the iron deficient subjects (91%) had absolute iron deficiency, as defined by TSAT ≤ 20% and serum ferritin ≤ 100 ng/ml. Compared to subjects without iron deficiency, those with iron deficiency had a lower median (IQR) hemoglobin SDS for age (−1.4 [−2.4, −0.5] vs. −0.7 [−1.8, 0.4], p = 0.009), although the prevalence of anemia was similar in the two groups (27% vs. 20%, p = 0.36). Total FGF23 concentrations (134 [91, 207] vs. 126 [88, 196], p = 0.55) and total FGF23 SDS for age (2.1 [0.7, 3.9] vs. 1.9 [0.7, 3.7], p = 0.62) did not differ between the iron deficient and sufficient groups. Across CKD stages and eGFR quartiles, iron deficiency was not associated with higher total FGF23 in any stage or quartile (Supplemental Table 3).
Relationship between anemia and total FGF23
Multiple linear regression modeling was performed to evaluate the association between anemia and total FGF23. In models adjusted for demographic parameters, kidney-related factors, inflammation, ESA use, and mineral metabolism parameters, anemia was significantly associated with higher total FGF23 values (standardized β (95% confidence interval (CI)) 0.10 (0.04, 0.17), p = 0.002, n = 459 in the fully adjusted model; Table 5, Supplemental Table 4). In the subset of subjects with available iron parameters, upon further adjustment for iron deficiency, the association between anemia and total FGF23 was attenuated (standardized β (95% CI) 0.10 (−0.02, 0.21), p = 0.09, n = 177 in the fully adjusted model; Supplemental Table 5).
Relationship between anemia and intact FGF23
A subset of the cohort (n = 185) had plasma intact FGF23 measured, with a median concentration of 65 (44, 113) pg/ml (Table 1). Anemic subjects had a higher median intact FGF23 concentration (74 [54, 176] vs. 64 [42, 111] pg/ml, p = 0.012) (Table 2). However, in multiple linear regression modeling, anemia was not independently associated with intact FGF23 (Supplemental Table 6).
Comparison of effects on total and intact FGF23
In the 185 study participants with both total and intact FGF23 measurements, in unadjusted analyses, the magnitude of the association between anemia and total FGF23 was more pronounced than the magnitude of the association between anemia and intact FGF23 (Supplemental Table 7). In adjusted analyses, anemia remained significantly associated with total FGF23, but not intact FGF23.
Discussion
In adult [2,3,4] and pediatric [5] CKD, levels of FGF23 are greatly increased, which contribute to CKD-MBD pathogenesis and have been associated with multisystemic co-morbidity and mortality [6,7,8,9,10,11,12,13,14]. Several mineral and non-mineral factors stimulate FGF23 production. Interestingly, anemia-related factors, including iron deficiency [16,17,18,19] and erythropoietin [22,23,24,25,26,27], have been shown to increase FGF23 production. In the present study, we evaluated associations between anemia and FGF23 in a large cohort of pediatric patients with CKD, hypothesizing that anemia is associated with increased circulating FGF23 concentrations.
In the cohort evaluated, the median baseline eGFR was 48 ml/min/1.73 m2, consistent with CKD stage 3a. Overall, 21% of study participants were anemic, similar to what was observed in the National Health and Nutrition Examination Survey (NHANES) of adults with CKD stage 3 [35, 36]. The median (IQR) C-terminal (total) FGF23 concentration was 118 (82, 204) RU/ml, which is similar to what was observed in the large adult Chronic Renal Insufficiency Cohort (CRIC) study in subjects with eGFR 40–49 ml/min/1.73 m2 (135 [94,188] RU/ml), measured with the same C-terminal (total) FGF23 assay [2]. In our cohort, 43% had a total FGF23 SDS for age > 2.0 (> 2 standard deviations above the mean value for age). A similar interpretation of intact FGF23 concentrations in our cohort is not possible, given a lack of assay-specific reference values for healthy children [37].
In cross-sectional analysis, we observed that study subjects with anemia had higher circulating concentrations of total FGF23. This association remained significant after adjustment for demographic parameters, CKD-specific factors, inflammation, ESA use, iron supplementation, and mineral metabolism parameters, suggesting a robust association between anemia and higher total FGF23 values. In the subset of subjects with available iron parameters, upon further adjustment for the presence vs. absence of iron deficiency, the association between anemia and total FGF23 was attenuated. This observation could suggest that iron deficiency, which is associated with both anemia and elevated total FGF23 concentrations in patients with CKD [38, 39], confounded the association between anemia and increased total FGF23. However, in the subgroup of our cohort with iron parameters, those with iron deficiency did not have a higher prevalence of anemia or higher total FGF23 concentrations, arguing against a high degree of confounding. Alternatively, the loss of statistical significance with the addition of iron deficiency to the model was likely contributed to by the large decrease in sample size, as only a relatively small subset of the cohort (39%) had iron parameters available.
In this small subset of our cohort, iron deficiency was not associated with higher total FGF23 concentrations; however, in larger adult CKD cohorts [38, 39], this association has been observed. In adults with CKD, multivariable linear regression modeling has shown independent, inverse associations between both serum ferritin and total FGF23 levels, and between hemoglobin and total FGF23 levels [27], suggesting that both iron status and hemoglobin concentration may affect FGF23 in CKD.
Additionally, other erythropoiesis-related factors may also affect FGF23 production in CKD. Exogenous erythropoietin administration can increase total FGF23 concentrations in patients with CKD [40], so it is possible that ESA use may have at least partially mediated the association we observed between anemia and elevated total FGF23 concentrations. In our cohort, study subjects with anemia had a higher prevalence of ESA use, and ESA use was associated with higher concentrations of total FGF23. However, in adjusted models, anemia was not significantly associated with ESA use (data not shown), ESA use was not significantly associated with FGF23, and the inclusion vs. exclusion of ESA use as an independent variable did not reduce the effect of anemia on FGF23, suggesting relatively little mediating effect of ESA use.
In our multiple linear regression modeling, we presented standardized coefficients, allowing for comparison of the relative effects of different independent variables on the dependent variable (log-transformed total FGF23). In our fully adjusted model, the magnitude of the effect of anemia on total FGF23 was similar to that of eGFR, and was greater than that of phosphate SDS for age, serum PTH, and active vitamin D use. In this model, the variance inflation factors (VIF) for the mineral metabolism variables were low, suggesting little collinearity among these independent variables that could affect the coefficients. Therefore, our modeling suggests that, in this CKD cohort, anemia may be as contributory to total FGF23 concentrations as kidney function and mineral metabolism parameters.
A subset of study participants (38%) had both total and intact FGF23 measurements available. In adjusted analyses, anemia was not associated with intact FGF23. Given that differences in sample size may have contributed to the differential observations for intact FGF23 (subset) vs. total FGF23 (full cohort), we performed analyses limited to this subgroup, in which both intact and total FGF23 were measured. In this group, in adjusted analyses, anemia was associated with total FGF23, but not intact FGF23.
Associations with total FGF23 but not intact FGF23 suggest effects on FGF23 cleavage. Translated FGF23 protein can be cleaved intracellularly, resulting in secretion into the circulation of predominantly intact FGF23, predominantly C-terminal and N-terminal FGF23 fragments, or a combination of intact and fragmented FGF23 [41]. Factors that increase FGF23 transcription or translation without affecting post-translational cleavage would be expected to increase circulating concentrations of both total and intact FGF23. Conversely, factors that increase FGF23 transcription or translation while concurrently increasing post-translational cleavage would be expected to increase circulating concentrations of total FGF23 to a greater degree than circulating concentrations of intact FGF23, reflecting the presence of increased FGF23 fragments. Factors that have been reported to concurrently increase FGF23 transcription and post-translational cleavage, resulting in the disproportionate cellular secretion of FGF23 fragments, include iron deficiency [16,17,18,19], erythropoietin [22,23,24,25,26,27], and inflammation [18].
Therefore, our observation of an association between anemia and total FGF23 but not anemia and intact FGF23 suggests the effects of a factor associated with anemia that couples increased FGF23 transcription/translation with increased proteolytic cleavage. All three aforementioned factors—iron deficiency [20], increased serum erythropoietin concentrations [28], and inflammation [42]—are associated with anemia in CKD and have similar effects on FGF23 production and metabolism. Therefore, these factors may have contributed to the observed results from our multiple linear regression modeling evaluating associations between anemia and FGF23 moieties in this subgroup. However, in our final model, which included adjustments for ESA use and C-reactive protein, anemia remained associated with total FGF23 but not intact FGF23, suggesting that neither of these factors markedly confounded our observations. As the subsets of subjects with available iron parameters and intact FGF23 measurements were almost completely mutually exclusive, we could not directly evaluate the effects of iron deficiency on relationships between anemia and FGF23 moieties in patients with both total and intact FGF23 measurements. However, in the iron parameter subset, iron deficiency was not associated with higher total FGF23 concentrations, suggesting likely little confounding effect in our cohort. Additionally, other as yet unidentified factors may mediate the inverse association between anemia and total FGF23. In a cohort of adult patients with CKD of similar size to our cohort and with a similar mean eGFR, in multivariable analysis, hemoglobin was inversely associated with total FGF23, independent of iron status (serum ferritin), serum erythropoietin, and inflammation (serum C-reactive protein), as well as eGFR and serum phosphate [27].
The goal of our study was to evaluate how anemia and anemia-related factors affect FGF23 levels; however, a bi-directional relationship may exist in which FGF23 also affects erythropoiesis. Pre-clinical studies have demonstrated that administration of exogenous intact FGF23 protein decreases kidney erythropoietin mRNA expression [26], serum erythropoietin concentrations [43], and erythropoietic parameters [43], whereas administration of an FGF23 blocking peptide increases serum erythropoietin concentrations and some erythropoietic parameters [44], suggesting that FGF23 negatively regulates erythropoiesis. Consistent with these pre-clinical studies, in a large cohort of adult patients with CKD (the Chronic Renal Insufficiency Cohort), increased baseline concentrations of total FGF23 were independently associated with both prevalent and incident anemia [45]. Therefore, whereas iron deficiency, increased erythropoietin, and anemia may contribute to higher FGF23 levels (with total FGF23 increased more so than intact FGF23), elevated FGF23, in turn, may contribute to decreased erythropoietin and impaired erythropoiesis.
Other cohort studies of pediatric patients with CKD have evaluated associations between hemoglobin concentrations and FGF23 levels [46,47,48]. One cross-sectional study observed that hemoglobin was inversely associated with total FGF23, but was not associated with intact FGF23 [46], similar to our findings. Another study also found that hemoglobin was inversely associated with total FGF23 [47], while a third study observed that hemoglobin was inversely associated with intact FGF23 [48]. However, all three of these cohorts were relatively small (53–62 patients), limiting the number of covariables for which the results could be adjusted; the former two studies included patients with kidney transplants or on dialysis, respectively; and the latter two studies used different FGF23 assays than those used in the present study.
Our study has strengths and limitations. To our knowledge, it is the largest study to date to evaluate associations among anemia, iron parameters, and FGF23 in a pediatric CKD cohort. In our multiple linear regression modeling, we were able to adjust for a large number of potentially confounding covariables. Additionally, our study benefits from the concurrent measurements of total and intact FGF23 concentrations, at least in a subset of study subjects, allowing for insight into possible effects on FGF23 cleavage. Study limitations include incomplete data for all subjects, such that iron parameters and intact FGF23 concentrations were only available in subsets of the entire cohort. Also, CRP may not be a very sensitive marker for inflammation. Lastly, our study is cross-sectional in nature and thus does not provide longitudinal insight as to whether anemia is associated with changes in FGF23 over time.
In summary, our study evaluated associations among anemia, iron parameters, and FGF23 in a large cohort of pediatric patients with CKD, demonstrating independent associations between anemia and higher total FGF23, but not intact FGF23, suggesting possible effects on both FGF23 production and cleavage. Our study highlights important associations between the anemia of CKD and CKD-MBD, and suggests that further studies are warranted to investigate how non-mineral factors influence FGF23 production and metabolism in CKD, and how the treatment of anemia in CKD may affect FGF23 and FGF23-related outcomes.
References
Pereira RC, Juppner H, Azucena-Serrano CE, Yadin O, Salusky IB, Wesseling-Perry K (2009) Patterns of FGF-23, DMP1, and MEPE expression in patients with chronic kidney disease. Bone 45:1161–1168
Isakova T, Wahl P, Vargas GS, Gutierrez OM, Scialla J, Xie H, Appleby D, Nessel L, Bellovich K, Chen J, Hamm L, Gadegbeku C, Horwitz E, Townsend RR, Anderson CA, Lash JP, Hsu CY, Leonard MB, Wolf M (2011) Fibroblast growth factor 23 is elevated before parathyroid hormone and phosphate in chronic kidney disease. Kidney Int 79:1370–1378
Larsson T, Nisbeth U, Ljunggren O, Juppner H, Jonsson KB (2003) Circulating concentration of FGF-23 increases as renal function declines in patients with chronic kidney disease, but does not change in response to variation in phosphate intake in healthy volunteers. Kidney Int 64:2272–2279
Gutierrez O, Isakova T, Rhee E, Shah A, Holmes J, Collerone G, Juppner H, Wolf M (2005) Fibroblast growth factor-23 mitigates hyperphosphatemia but accentuates calcitriol deficiency in chronic kidney disease. J Am Soc Nephrol 16:2205–2215
Portale AA, Wolf M, Juppner H, Messinger S, Kumar J, Wesseling-Perry K, Schwartz GJ, Furth SL, Warady BA, Salusky IB (2014) Disordered FGF23 and mineral metabolism in children with CKD. Clin J Am Soc Nephrol 9:344–353
Fliser D, Kollerits B, Neyer U, Ankerst DP, Lhotta K, Lingenhel A, Ritz E, Kronenberg F, Group MS, Kuen E, Konig P, Kraatz G, Mann JF, Muller GA, Kohler H, Riegler P (2007) Fibroblast growth factor 23 (FGF23) predicts progression of chronic kidney disease: the Mild to Moderate Kidney Disease (MMKD) Study. J Am Soc Nephrol 18:2600–2608
Isakova T, Xie H, Yang W, Xie D, Anderson AH, Scialla J, Wahl P, Gutierrez OM, Steigerwalt S, He J, Schwartz S, Lo J, Ojo A, Sondheimer J, Hsu CY, Lash J, Leonard M, Kusek JW, Feldman HI, Wolf M, Chronic Renal Insufficiency Cohort Study Group (2011) Fibroblast growth factor 23 and risks of mortality and end-stage renal disease in patients with chronic kidney disease. JAMA 305:2432–2439
Portale AA, Wolf MS, Messinger S, Perwad F, Juppner H, Warady BA, Furth SL, Salusky IB (2016) Fibroblast Growth Factor 23 and Risk of CKD Progression in Children. Clin J Am Soc Nephrol 11:1989–1998
Faul C, Amaral AP, Oskouei B, Hu MC, Sloan A, Isakova T, Gutierrez OM, Aguillon-Prada R, Lincoln J, Hare JM, Mundel P, Morales A, Scialla J, Fischer M, Soliman EZ, Chen J, Go AS, Rosas SE, Nessel L, Townsend RR, Feldman HI, St John Sutton M, Ojo A, Gadegbeku C, Di Marco GS, Reuter S, Kentrup D, Tiemann K, Brand M, Hill JA, Moe OW, Kuro OM, Kusek JW, Keane MG, Wolf M (2011) FGF23 induces left ventricular hypertrophy. J Clin Invest 121:4393–4408
Gutierrez OM, Januzzi JL, Isakova T, Laliberte K, Smith K, Collerone G, Sarwar A, Hoffmann U, Coglianese E, Christenson R, Wang TJ, deFilippi C, Wolf M (2009) Fibroblast growth factor 23 and left ventricular hypertrophy in chronic kidney disease. Circulation 119:2545–2552
Mitsnefes MM, Betoko A, Schneider MF, Salusky IB, Wolf MS, Juppner H, Warady BA, Furth SL, Portale AA (2018) FGF23 and Left Ventricular Hypertrophy in Children with CKD. Clin J Am Soc Nephrol 13:45–52
Rossaint J, Oehmichen J, Van Aken H, Reuter S, Pavenstadt HJ, Meersch M, Unruh M, Zarbock A (2016) FGF23 signaling impairs neutrophil recruitment and host defense during CKD. J Clin Invest 126:962–974
Chonchol M, Greene T, Zhang Y, Hoofnagle AN, Cheung AK (2016) Low vitamin d and high fibroblast growth factor 23 serum levels associate with infectious and cardiac deaths in the HEMO study. J Am Soc Nephrol 27:227–237
Gutierrez OM, Mannstadt M, Isakova T, Rauh-Hain JA, Tamez H, Shah A, Smith K, Lee H, Thadhani R, Juppner H, Wolf M (2008) Fibroblast growth factor 23 and mortality among patients undergoing hemodialysis. N Engl J Med 359:584–592
Hanudel MR, Laster M, Salusky IB (2018) Non-renal-Related Mechanisms of FGF23 Pathophysiology. Curr Osteoporos Rep 16:724–729
Farrow EG, Yu X, Summers LJ, Davis SI, Fleet JC, Allen MR, Robling AG, Stayrook KR, Jideonwo V, Magers MJ, Garringer HJ, Vidal R, Chan RJ, Goodwin CB, Hui SL, Peacock M, White KE (2011) Iron deficiency drives an autosomal dominant hypophosphatemic rickets (ADHR) phenotype in fibroblast growth factor-23 (Fgf23) knock-in mice. Proc Natl Acad Sci U S A 108:E1146-1155
Clinkenbeard EL, Farrow EG, Summers LJ, Cass TA, Roberts JL, Bayt CA, Lahm T, Albrecht M, Allen MR, Peacock M, White KE (2014) Neonatal iron deficiency causes abnormal phosphate metabolism by elevating FGF23 in normal and ADHR mice. J Bone Miner Res 29:361–369
David V, Martin A, Isakova T, Spaulding C, Qi L, Ramirez V, Zumbrennen-Bullough KB, Sun CC, Lin HY, Babitt JL, Wolf M (2016) Inflammation and functional iron deficiency regulate fibroblast growth factor 23 production. Kidney Int 89:135–146
Hanudel MR, Chua K, Rappaport M, Gabayan V, Valore E, Goltzman D, Ganz T, Nemeth E, Salusky IB (2016) Effects of dietary iron intake and chronic kidney disease on fibroblast growth factor 23 metabolism in wild-type and hepcidin knockout mice. Am J Physiol Renal Physiol 311:F1369–F1377
Fishbane S, Pollack S, Feldman HI, Joffe MM (2009) Iron indices in chronic kidney disease in the National Health and Nutritional Examination Survey 1988–2004. Clin J Am Soc Nephrol 4:57–61
Baracco R, Saadeh S, Valentini R, Kapur G, Jain A, Mattoo TK (2011) Iron deficiency in children with early chronic kidney disease. Pediatr Nephrol 26:2077–2208
Clinkenbeard EL, Hanudel MR, Stayrook KR, Appaiah HN, Farrow EG, Cass TA, Summers LJ, Ip CS, Hum JM, Thomas JC, Ivan M, Richine BM, Chan RJ, Clemens TL, Schipani E, Sabbagh Y, Xu L, Srour EF, Alvarez MB, Kacena MA, Salusky IB, Ganz T, Nemeth E, White KE (2017) Erythropoietin stimulates murine and human fibroblast growth factor-23, revealing novel roles for bone and bone marrow. Haematologica 102:e427–e430
Rabadi S, Udo I, Leaf DE, Waikar SS, Christov M (2018) Acute blood loss stimulates fibroblast growth factor 23 production. Am J Physiol Renal Physiol 314:F132–F139
Flamme I, Ellinghaus P, Urrego D, Kruger T (2017) FGF23 expression in rodents is directly induced via erythropoietin after inhibition of hypoxia inducible factor proline hydroxylase. PLoS One 12:e0186979
Toro L, Barrientos V, Leon P, Rojas M, Gonzalez M, Gonzalez-Ibanez A, Illanes S, Sugikawa K, Abarzua N, Bascunan C, Arcos K, Fuentealba C, Tong AM, Elorza AA, Pinto ME, Alzamora R, Romero C, Michea L (2018) Erythropoietin induces bone marrow and plasma fibroblast growth factor 23 during acute kidney injury. Kidney Int 93:1131–1141
Daryadel A, Bettoni C, Haider T, Imenez Silva PH, Schnitzbauer U, Pastor-Arroyo EM, Wenger RH, Gassmann M, Wagner CA (2018) Erythropoietin stimulates fibroblast growth factor 23 (FGF23) in mice and men. Pflugers Arch 470:1569–1582
Hanudel MR, Eisenga MF, Rappaport M, Chua K, Qiao B, Jung G, Gabayan V, Gales B, Ramos G, de Jong MA, van Zanden JJ, de Borst MH, Bakker SJL, Nemeth E, Salusky IB, Gaillard C, Ganz T (2019) Effects of erythropoietin on fibroblast growth factor 23 in mice and humans. Nephrol Dial Transplant 34:2057–2065
Artunc F, Risler T (2007) Serum erythropoietin concentrations and responses to anaemia in patients with or without chronic kidney disease. Nephrol Dial Transplant 22:2900–2908
Furth SL, Cole SR, Moxey-Mims M, Kaskel F, Mak R, Schwartz G, Wong C, Munoz A, Warady BA (2006) Design and methods of the chronic kidney disease in children (CKiD) prospective cohort study. Clin J Am Soc Nephrol 1:1006–1015
Kidney Disease: Improving Global Outcomes (KDIGO) Anemia Work Group (2012) KDIGO clinical practice guideline for anemia in chronic kidney disease. Kidney Int Suppl 2:279–335
Janus J, Moerschel SK (2010) Evaluation of anemia in children. Am Fam Physician 81:1462–1471
Fischer DC, Mischek A, Wolf S, Rahn A, Salweski B, Kundt G, Haffner D (2012) Paediatric reference values for the C-terminal fragment of fibroblast-growth factor-23, sclerostin, bone-specific alkaline phosphatase and isoform 5b of tartrate-resistant acid phosphatase. Ann Clin Biochem 49:546–553
Pierce CB, Munoz A, Ng DK, Warady BA, Furth SL, Schwartz GJ (2021) Age- and sex-dependent clinical equations to estimate glomerular filtration rates in children and young adults with chronic kidney disease. Kidney Int 99:948–956
Ardeshirpour L, Cole DE, Carpenter TO (2007) Evaluation of bone and mineral disorders. Pediatr Endocrinol Rev 5(Suppl 1):584–598
Stauffer ME, Fan T (2014) Prevalence of anemia in chronic kidney disease in the United States. PLoS One 9:e84943
Kovesdy CP, Davis JR, Duling I, Little DJ (2023) Prevalence of anaemia in adults with chronic kidney disease in a representative sample of the United States population: analysis of the 1999–2018 National Health and Nutrition Examination Survey. Clin Kidney J 16:303–311
Heijboer AC, Cavalier E (2023) The measurement and interpretation of fibroblast growth factor 23 (FGF23) concentrations. Calcif Tissue Int 112:258–270
Eisenga MF, van Londen M, Leaf DE, Nolte IM, Navis G, Bakker SJL, de Borst MH, Gaillard C (2017) C-terminal fibroblast growth factor 23, iron deficiency, and mortality in renal transplant recipients. J Am Soc Nephrol 28:3639–3646
Mehta RC, Cho ME, Cai X, Lee J, Chen J, He J, Flack J, Shafi T, Saraf SL, David V, Feldman HI, Isakova T, Wolf M, CRIC Study Investigators (2021) Iron status, fibroblast growth factor 23 and cardiovascular and kidney outcomes in chronic kidney disease. Kidney Int 100:1292–1302
Eisenga MF, Emans ME, van der Putten K, Cramer MJ, Diepenbroek A, Velthuis BK, Doevendans PA, Verhaar MC, Joles JA, Bakker SJL, Nolte IM, Braam B, Gaillard C (2019) Epoetin beta and c-terminal fibroblast growth factor 23 in patients with chronic heart failure and chronic kidney disease. J Am Heart Assoc 8:e011130
Komaba H, Fukagawa M (2012) The role of FGF23 in CKD–with or without Klotho. Nat Rev Nephrol 8:484–490
Babitt JL, Lin HY (2012) Mechanisms of anemia in CKD. J Am Soc Nephrol 23:1631–1634
Coe LM, Madathil SV, Casu C, Lanske B, Rivella S, Sitara D (2014) FGF-23 is a negative regulator of prenatal and postnatal erythropoiesis. J Biol Chem 289:9795–9810
Agoro R, Montagna A, Goetz R, Aligbe O, Singh G, Coe LM, Mohammadi M, Rivella S, Sitara D (2018) Inhibition of fibroblast growth factor 23 (FGF23) signaling rescues renal anemia. FASEB J 32:3752–3764
Mehta R, Cai X, Hodakowski A, Lee J, Leonard M, Ricardo A, Chen J, Hamm L, Sondheimer J, Dobre M, David V, Yang W, Go A, Kusek JW, Feldman H, Wolf M, Isakova T, CRIC Study Investigators (2017) Fibroblast growth factor 23 and anemia in the chronic renal insufficiency cohort study. Clin J Am Soc Nephrol 12:1795–1803
Limm-Chan B, Wesseling-Perry K, Pearl MH, Jung G, Tsai-Chambers E, Weng PL, Hanudel MR (2021) Associations among erythropoietic, iron-related, and FGF23 parameters in pediatric kidney transplant recipients. Pediatr Nephrol 36:3241–3249
Karava V, Dotis J, Kondou A, Christoforidis A, Taparkou A, Farmaki E, Economou M, Printza N (2023) Fibroblast growth-factor 23 and vitamin D are associated with iron deficiency and anemia in children with chronic kidney disease. Pediatr Nephrol 38:2771–2779
Yamamura-Miyazaki N, Michigami T, Ozono K, Yamamoto K, Hasuike Y (2022) Factors associated with 1-year changes in serum fibroblast growth factor 23 levels in pediatric patients with chronic kidney disease. Clin Exp Nephrol 26:1014–1021
Acknowledgements
Data in this manuscript were collected by the Chronic Kidney Disease in children prospective cohort study (CKiD) with clinical coordinating centers (Principal Investigators) at Children’s Mercy Hospital and the University of Missouri – Kansas City (Bradley Warady, MD) and Children’s Hospital of Philadelphia (Susan Furth, MD, PhD), Central Biochemistry Laboratory (George Schwartz, MD) at the University of Rochester Medical Center, and data coordinating center (Alvaro Muñoz, PhD and Derek Ng, PhD) at the Johns Hopkins Bloomberg School of Public Health. Data from the Chronic Kidney Disease in Children Cohort Study [(V7)/https://doi.org/10.58020/dzq8-ct80] reported here are available for request at the NIDDK Central Repository (NIDDK-CR) website, Resources for Research (R4R), https://repository.niddk.nih.gov/.
The CKiD Study is supported by grants from the National Institute of Diabetes and Digestive and Kidney Diseases, with additional funding from the Eunice Kennedy Shriver National Institute of Child Health and Human Development, and the National Heart, Lung, and Blood Institute (U01-DK066143, U01-DK066174, U24-DK082194, U24-DK066116). The CKiD website is located at https://statepi.jhsph.edu/ckid, and a list of CKiD collaborators can be found at https://statepi.jhsph.edu/ckid/site-investigators/.
This work was presented as an oral abstract at the 2021 American Society of Nephrology Annual Meeting, and as a poster abstract at the 2022 Pediatric Academic Societies Annual Meeting.
Funding
The work in this manuscript has been performed with the support of the National Institute of Diabetes, Digestive, and Kidney Disease of the National Institute of Health research grants T32-DK104687 (ET) and K23-DK123378 (MLL).
Author information
Authors and Affiliations
Contributions
SLL and BAW are the CKiD Principal Investigators. ET, AMK, and MRH analyzed the data. ET drafted the initial manuscript; MLL, IBS, and MRH provided edits; ET and MRH drafted the revised manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflicts of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Thomas, E., Klomhaus, A.M., Laster, M.L. et al. Associations between anemia and FGF23 in the CKiD study. Pediatr Nephrol 39, 837–847 (2024). https://doi.org/10.1007/s00467-023-06160-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00467-023-06160-0