
Abstract
Background
Over the past decade, the use of stent placement as a bridge to surgery (BTS) has emerged as an alternative to emergency surgery for patients with (OCRC). However, the optimal surgical approach remains indeterminate. This study seeks to evaluate the safety and feasibility of a combined treatment modality involving stent placement and laparoscopic surgery for OCRC presenting with malignant obstruction.
Methods
A comprehensive search of PubMed, Cochrane Library, EMBASE, Web of Science, and ClinicalTrials.gov was conducted until June 2023 to identify studies that compared laparoscopic to open surgery in patients with OCBC following stent insertion.
Results
The meta-analysis incorporated 12 cohort studies, encompassing 933 patients. There was no statistically significant difference in the 30-day mortality rates between the two groups (relative risk [RR], 1.09; 95% confidence interval [CI] 0.26 to 4.48; P = 0.95). Compared to the laparoscopic approach group, the open approach group had a higher rate of overall postoperative complications (POCs) (RR 0.52; 95% CI 0.37 to 0.72, P < 0.0001). There was no significant variance in lymph node (LN) dissection number between the groups (mean differences [MD], 1.64; 95% CI − 1.51 to 4.78; P = 0.31). Notably, laparoscopic surgery resulted in less intraoperative blood loss (MD, − 25.84 ml; 95% CI − 52.16 to 0.49; P = 0.05) and a longer operation time (MD, 20.99 mins; 95% CI 2.31 to 39.44; P = 0.03). The laparoscopic approach was associated with a shorter length of hospital stay (LOS) (MD − 3.29 days; 95% CI − 5.27 to 1.31; P = 0.001). Conversely, the open approach group had a higher rate of postoperative surgical site infection (SSI) (RR 0.47; 95% CI 0.23 to 0.96, P = 0.04). Although the number of included studies was insufficient to conduct a meta-analysis, several of them imply that laparoscopic surgery may yield more favorable outcomes in terms of the 3-year overall survival rate (OS), 3-year disease-free survival rate (DFS), 5-year OS, and 5-year DFS when compared to open surgery. It is worth noting that these differences lack statistical significance.
Conclusion
In patients with OCRC subjected to stent insertion, laparoscopic surgery arguably presents a modest superiority over open surgery by diminishing the overall postoperative risk and potentially reducing the LOS.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Colorectal cancer (CRC), the third most frequently diagnosed and deadly cancer globally, yields an estimated 1.85 million new cases annually [1, 2]. The primary objective is high-quality oncological resection [3]; however, an estimated 8% to 29% of CRC patients present with acute colorectal obstruction (ACO) [4]. Often, these patients are older and frail and their clinical condition deteriorated due to insufficient oral intake [5]. The management of this severe condition remains a contentious issue [6].
Historically, patients with OCRC have undergone emergency open surgery to restore luminal patency [7]. Emergency surgery for OCRC patients, while effective in relieving obstruction either curatively or palliatively with a permanent stoma, is associated with high mortality and morbidity rates [8, 9]. In the past decade, self-expanding metal stents (SEMS) have proven to be safe, easy, and effective as bridge to surgery (BTS) and palliative treatment for CRC, with an acceptable complication rate [10]. It allows for the conversion of an emergency surgery to an elective one, reduces stoma creation rate, overall postoperative complications, and enables the use of laparoscopic techniques by improving the surgical field [11]. The European Society of Gastrointestinal Endoscopy (ESGE) guideline [6] recommend stenting as a BTS in patients with potentially curable left-sided obstructing colon cancer (LSOCC). The American Gastroenterological Association (AGA) clinical practice [12] suggests inserting SEMS as a BTS for patients with proximal (or right-sided) malignant obstructions who are potential candidates for resection, thus facilitating elective rather than emergency surgery. A propensity score-matched analysis of oncological outcomes [13], as well as several meta-analyses [14, 15], has confirmed the feasibility, oncological safety, and benefits of SEMS implantation, which in certain cases can serve as a bridge to later elective surgery. Studies [16,17,18] have also demonstrated that a laparoscopic approach is feasible for patients with OCRC due to CRC following stent placement.
However, laparoscopic surgery presents unique challenges for OCRC patients, such as the introduction of trocars into a distended abdomen, potential intestinal injury, limited instrument mobility, and increased difficulty due to large, locally advanced tumors causing luminal obstruction. In contrast, laparotomy, while straightforward and versatile, is more traumatic and imposes a slower recovery post-operation. Comparative studies on the efficacy of laparoscopic surgery and laparotomy following stent placement are limited and a clear consensus on the surgical approach for OCRC patients post-SEMS implantation is lacking. Questions remain on the optimal time interval, technical difficulty, and other issues from stent implantation to determining the operation. Thus, this study aims to compare the safety and efficacy of elective laparoscopic surgery and open surgical approaches following stent insertion for OCRC patients.
Method
The development of the inclusion criteria adhered to the guidelines set forth by the Cochrane Collaboration [19] and the recommendations from the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) [20]. The methodology of the study is documented in a protocol, which is registered and accessible at http://www.crd.york.ac.uk/prospero/ (registration number: CRD42022301124).
Search strategy
A comprehensive literature search was conducted using PubMed, Cochrane Library, EMBASE, Web of Science, and ClinicalTrials.gov with the key terms ‘colorectal neoplasms,’ ‘intestinal obstruction,’ ‘stents,’ ‘laparoscopy,’ ‘minimal access surgical,’ and ‘elective surgery,’ without any restrictions on language or date. The search strategy is provided in Online Appendix 1. The initial search was performed in March 2022 and an email alert was set up in databases and journals to receive notifications for any new publications. However, no new relevant studies were identified, suggesting that the search period was from March 2022 to the end of February 2023. Each article was reviewed and analyzed by at least two members of the research team (KR.Z. and SX.F.) using an unblinded standardized approach for eligibility assessment. In cases where multiple publications reported findings for the same patients, the most recent or most comprehensive study was selected. Any conflicting studies were resolved through discussions among all the authors.
Literature inclusion
Inclusion criteria
Studies satisfying the subsequent criteria were deemed eligible for inclusion: (1) Patients who have undergone surgical intervention following stent insertion as a BTS for malignant obstruction induced by CRC; (2) The study compared the outcomes of stent insertion combined with laparoscopic surgery (experimental group) and stent insertion combined with laparotomy (control group); (3) The study reported a minimum of one outcome of interest; and (4) The study was a prospective study, retrospective study, or a Randomized Controlled Trial (RCT) published in either English or Chinese.
Exclusion criteria
Studies were excluded if they met the following criteria: (1) The administration of any adjuvant treatments, such as chemotherapy, between SEMS insertion and surgery; (2) Incomplete data; (3) Instances of repeat publications or studies with duplicate data, retaining only the highest quality representation; and (4) Studies that do not permit the execution of a meta-analysis.
Outcomes of interest and definitions
Primary outcomes included the following: (1) 30-day mortality rate; (2) overall postoperative complications (POCs) rates; (3) 3- and 5-year DFS rates; and (4) 3- and 5-year OS rates. The term ‘overall POCs’ encompasses any diagnosed adverse events associated with the surgery prior to hospital discharge.
Secondary outcomes included lymph node (LN) dissection and a range of perioperative outcomes, such as operation duration, intraoperative blood loss, length of hospital stay (LOS), time to first flatus, and any postprocedural adverse events prior to hospital discharge, including postoperative ileus (POI), surgical site infection (SSI), anastomotic leakage (AL), postoperative pulmonary infection, and postoperative wound dehiscence.
Data extraction
Two researchers, KR.Z. and SX.F., independently reviewed the articles. Any disagreements regarding the inclusion of certain studies were resolved through discussions involving all authors. The first step involved identifying and excluding any duplicate articles. Subsequently, these two researchers analyzed the titles and abstracts of the articles, eliminating those that were irrelevant. The full texts of the remaining articles were then scrutinized for potential inclusion. KR.Z. conducted the data extraction, which was later reviewed and confirmed by SX.F. Any discrepancies were resolved through discussion among all authors. Where available, the reviewers independently gathered four types of data. The first type included basic information about the studies, such as titles, authors, publication year, and country of origin. The second type involved baseline characteristics, including study design, tumor location, sample size, patient age and sex, American Society of Anesthesiologists (ASA) classification, time from SEMS insertion to surgery, and median follow-up period. The third type of data related to outcomes of interest, encompassing perioperative outcomes, histopathological outcomes, and postoperative complications. The fourth type included key elements for assessing bias risk.
Quality evaluation
Two reviewers, KR.Z. and FQ.Z., independently assessed the risk of bias in individual studies using the Newcastle–Ottawa Quality Assessment Scale (NOS) [21]. The NOS evaluation is based on three specific domains: selection, comparability, and outcome, with scores ranging from zero to nine. In our study, scores equal to or greater than seven were deemed high quality, while scores lower than seven were considered low quality. RCTs were evaluated according to the Cochrane Collaboration guidelines [19] to identify potential bias. These potential biases included random sequence generation, allocation concealment, blinding of outcome assessment, blinding of participants, selective reporting, assessment of incomplete data outcome, and other potential sources of bias.
Statistical analysis
Data analysis was conducted using RevMan software (Cochrane Review Manager, Version 5.4.1) and STATA version 16.0 (StataCorp LP, College Station, TX). Relative risks (RR) and 95% confidence intervals (CIs) for dichotomous variables were estimated via the Mantel–Haenszel method. For continuous outcome data, mean differences (MDs) and 95% CIs were calculated using inverse variance weighting. In cases where means or standard deviations (SDs) were not provided, estimations were made from the reported medians, ranges, and sample size as outlined by Hozo et al. [22]. Forest plots were then generated using RevMan, with a P value of less than 0.05 on 2-tailed testing indicating a statistically significant difference. If both the exposure and control groups in a study had a value of zero, STATA was utilized to generate a forest plot. A 0.5 continuity correction transformation was implemented to account for zero events. To assess heterogeneity, the Q test based on the χ2 statistics and I2 statistics were used. Significant between-study heterogeneity was determined when P < 0.1 and I2 > 50% among the studies. Anticipating between-study heterogeneity, the pooled estimates were analyzed using the random-effects model and the Der Simonian and Laird method based on the moment estimator. Subgroup analysis, meta-regression, and sensitivity analysis were employed to analyze significant heterogeneity, or it was merely stated. Sensitivity analysis was executed by sequentially eliminating individual studies. Publication bias was initially assessed by visually inspecting for the presence of funnel plot asymmetry, and the Egger test was used to evaluate the presence of asymmetry, with P < 0.05 deemed significant.
Results
Study selection
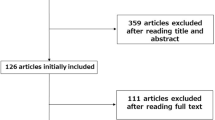
Figure 1 illustrates the detailed procedures of the systematic literature selection. Initially, a total of 2179 articles were identified via a systematic review of the literature. After eliminating 305 duplicate papers from the initial search, the number was reduced to 1874. Of these, 1857 studies were excluded after examining titles and abstracts due to non-compliance with the inclusion criteria. Notably, four consensus conference studies and one clinical trial [23] were among the excluded. The clinical trial’s patient data did not meet the inclusion criteria. A thorough review of the full text of the remaining 17 potentially suitable studies led to the inclusion of 12 cohort studies [16, 24,25,26,27,28,29,30,31,32,33,34] in the quantitative analysis. Of these, 11 were retrospective studies, while one was a prospective study [34].

Flowchart of study selection.
Characteristics of included studies
The studies under consideration encompassed a total of 933 patients who underwent either laparoscopic or open surgical procedures. Of these, 463 patients were part of the laparoscopic group, while the open group consisted of 470 patients. A radical effect was achieved in the types of surgeries reported in four studies [26, 28, 31, 33]. Another set of four studies [24, 25, 32, 34] incorporated both radical and non-radical surgeries. However, the surgical types, whether curative or otherwise, were not specified in the remaining four studies [16, 27, 29, 30]. A total of 14 outcome indexes were compared, which included 30-day mortality, overall POCs, 3-year or 5-year DFS rates, 3-year or 5-year OS rates, LN dissection, operation time, intraoperative blood loss, LOS, POI, SSI, AL, postoperative pulmonary infection, postoperative wound dehiscence, and time to first flatus. The primary characteristics of the included studies are detailed in Table 1.
Risk of bias of the studies
The quality of the cohort studies was evaluated based on the NOS scores, which are detailed in Table 2. Quality assessments conducted on all the papers yielded scores ranging from 5 to 8. Nine studies [16, 26,27,28,29, 31,32,33,34] were deemed high quality (with a quality score of 7 or above), while the remaining three studies [24, 25, 30] were classified as low quality (with a quality score below 7).
Primary outcomes
This meta-analysis examined the 30-day mortality rates (Fig. 2) and overall POCs rates (Fig. 3), along with 3-year and 5-year DFS and OS rates as the primary outcomes.

Frost plot for 30-day mortality rates. LAP laparoscopic approach; OPEN open approach

Frost plot for overall POCs rates. POCs postoperative complications; LAP laparoscopic approach; OPEN open approach
Six studies [26, 27, 29,30,31, 34] evaluated the 30-day mortality rates, revealing no significant differences (RR 95% CI 1.09; 0.26 to 4.48; P = 0.95), with no observed between-study heterogeneity (I2 = 0, P = 0.91). The rates of overall POCs were reported in nine studies [16, 25,26,27,28, 30, 31, 33, 34]. In comparison to the laparoscopic group, the open approach group exhibited a higher rate of overall POCs (RR 0.52; 95% CI 0.37 to 0.72, P < 0.0001), with no apparent between-study heterogeneity (I2 = 0, P = 0.51).
The study by reference [26] underscores a 5-year DFS rate of 61.5% within the laparoscopic group, in contrast to 55.8% in the open surgery cohort. However, these findings lack statistical significance (HR 0.982, 95% CI 0.522 to 1.847; P = 0.995). Despite the absence of statistical significance, the same study [26] reports a higher 5-year OS rate of 71.7% for the laparoscopic group, compared to the 67.1% rate in the open surgery group (HR 1.028, 95% CI 0.491 to 2.15; P = 0.942). Another study [32] documented both 5-year DFS and OS rates. Despite the laparoscopic approach group exhibiting higher 5-year DFS rates and 5-year OS rates, no significant differences were observed in either the 5-year DFS or OS rates when comparing the laparoscopic approach group with the open approach group (5-year DFS rates were 68.9% vs. 57.1%, P = 0.233; 5-year OS rates were 81.65% vs. 71.0%, P = 0.206).
Tajima’s investigation [32] revealed a 3-year OS rate of 66.4% for the laparoscopic approach group, slightly lower than the 67.5% rate observed in the open approach group, although the difference lacked statistical significance (P = 0.56). In the same study [35], a 3-year DFS rate of 82.2% was observed for the laparoscopic group, in contrast to 62.5% for the open group. Despite the laparoscopic group exhibiting a higher 3-year DFS rate, no statistical significance was found between the two groups (P = 0.11). Another investigation [16] disclosed no significant disparities between the laparoscopic and open approach groups in terms of 3-year DFS rates (71% vs. 70%, P = 0.731) or 3-year OS rates (83% vs. 70%, P = 0.915).
Secondary outcomes
The secondary outcomes investigated comprised LN dissection (Fig. 4), operation time (Fig. 5), intraoperative blood loss (Fig. 6), LOS (Fig. 7), POI (Fig. 8), SSI (Fig. 9), and AL (Fig. 10).

Frost plot for LN dissection. LAP laparoscopic approach; OPEN open approach

Frost plot for operation time. LAP laparoscopic approach; OPEN open approach

Frost plot for intraoperative blood loss. LAP laparoscopic approach; OPEN open approach

Frost plot for LOS. LOS: length of hospital stay. LAP laparoscopic approach; OPEN open approach

Frost plot for POI. LAP laparoscopic approach; OPEN open approach; POI postoperative ileus

Frost plot for postoperative SSI. SSI surgical site infection; LAP laparoscopic approach; OPEN open approach

Frost plot for AL. AL anastomotic leakage, LAP laparoscopic approach; OPEN open approach
Seven studies [24,25,26, 29, 31,32,33] reported on LN dissection, demonstrating a moderate level of heterogeneity (I2 = 50%, P = 0.06). The MD was 1.64 (95% CI − 1.51 to 4.78; P = 0.31), suggesting no significant difference between the groups in terms of LN dissection number. A sensitivity analysis, conducted by sequentially eliminating individual studies, confirmed the stability of the meta-analysis result, with no significant change observed pre- and post-elimination.
Operation time was documented in ten studies [16, 24,25,26, 28,29,30,31,32,33]. Despite a high degree of heterogeneity (I2 = 90% and P < 0.0001), a significant difference was noted between the laparoscopic approach and the open group (MD = 20.99 mins, 95% CI 2.31 to 39.44; P = 0.03). A funnel plot inspection showed no evidence of asymmetry, corroborated by an Egger test for funnel plot asymmetry resulting in a P-value of 0.4956, thus indicating no potential publication bias.
Intraoperative blood loss was reported in nine studies [16, 24, 25, 28,29,30,31,32,33] revealing a significant difference in favor of the laparoscopic approach (MD = − 25.84 ml, 95% CI − 52.16 to 0.49; P = 0.05), with considerable heterogeneity (I2 = 73% and P = 0.0002).
The six studies [25, 26, 29,30,31, 33] reported on LOS, exhibiting a high degree of heterogeneity (I2 = 89%, P < 0.00001). The overall effect test revealed a MD of -3.29 days, which was statistically significant (95% CI − 5.27 to 1.31; P = 0.001).
POI was assessed in nine studies [24,25,26, 28, 30,31,32,33], and no statistically significant risk difference between the two groups was found (RR 0.92; 95% CI 0.48 to 1.74; P = 0.8), in the absence of between-study heterogeneity (I2 = 0, P = 0.58).
SSI was reported in eight studies [16, 24, 26, 28, 30,31,32,33]. Compared to the laparoscopic approach, the open approach was associated with a higher rate of SSI (RR 0.47; 95% CI 0.23 to 0.96, P = 0.04), with no between-study heterogeneity (I2 = 0, P = 0.78).
AL was evaluated in seven studies [24, 26, 28, 30,31,32], with no between-study heterogeneity (I2 = 0, P = 0.99). The overall effect test showed an RR of 0.82 (95% CI 0.37 to 1.84; P = 0.64).
The analysis of additional primary outcomes, such as postoperative pulmonary infection, postoperative wound dehiscence, and time to first flatus, was hindered by insufficient data for inferential analysis. Postoperative pulmonary infection was reported in six studies [24, 26,27,28, 31, 33]; however, inconsistencies in the definitions of this outcome across the studies were noted. Specifically, one study [26] defined it as a pulmonary complication, another [27] as pleural effusion, while the remaining four studies [24, 28, 31, 33] classified it as pulmonary infection. To mitigate bias, an analysis of these outcomes was not conducted. Furthermore, postoperative wound dehiscence was documented in only three studies [16, 26, 28], and time to first flatus was reported in four studies [16, 28, 31, 33]. The limited number of studies addressing these outcomes precluded further analysis.
Subgroup and sensitivity analyses
Meta-regression analysis was conducted to explore factors that potentially influence heterogeneity, including the types of surgeries, tumor sites, and NOS scores. The findings indicated that the types of surgeries significantly contributed to the heterogeneity of operation time (P < 0.001). Subsequently, subgroup analysis was performed to further investigate significant heterogeneity based on the types of surgeries, and sensitivity analysis was conducted using the one-by-one exclusion method.
The study analyzed the operation time, intraoperative bleeding, and LOS based on the type of surgery performed (radical or not). Detailed information can be found in Table 3. The results showed that among patients undergoing radical surgery, there was no significant difference in the operation time between the two groups. This finding deviated from the overall results, and there was a lower heterogeneity between studies (I2 = 0). Although there was no significant difference in intraoperative blood loss between the two groups, there was substantial heterogeneity (I2 = 89%). Regarding LOS, the laparoscopic approach group exhibited a shorter hospital stay than the open approach group in the radical surgery subgroup. However, there was also significant heterogeneity among the studies (I2 = 89%).
Sensitivity analysis of the one-by-one exclusion method was conducted to examine the impact of greater heterogeneity in the population and radical subgroups on the results. Our findings reveal that excluding Kim [29] and Mat [24] did not significantly alter the overall heterogeneity of operation time. However, the overall results differed significantly (MD = 18.92, 95% CI − 2.18 to 40.02; P = 0.08), (MD = 18.69, 95% CI − 0.41 to 37.79; P = 0.06). Thus, it can be suggested that the overall results are not reliable, but the results of the radical subgroup remain stable.
Based on a meticulous analysis of the total and specific subgroups of intraoperative blood loss, our findings indicate that there is considerable heterogeneity and variability in the results, with only a small number of studies remaining unaffected. This leads us to conclude that the reliability of both the overall and specific subgroup results of intraoperative blood loss is questionable.
Furthermore, in order to conduct a sensitive analysis, we excluded the results of LOS for both the overall and specific subgroups individually. It is worth noting that none of these exclusions had a significant impact on the results, suggesting their stability.
Discussion
Upon review of the literature [36], the use of a stent as BTS is designed to decompress the large bowel in acutely ill patients, thereby providing time for patient stabilization, diagnostic staging, bowel cleansing, and the transition from an emergency to an elective surgical intervention. The attenuation of intestinal edema, enhancement of the patient’s nutritional status, and bolstered immunity collectively facilitate the subsequent employment of minimally invasive surgical techniques once the intestinal obstruction is alleviated. Currently, there is a dearth of published randomized trials evaluating the surgical modalities for CRC resection in an emergency context. Furthermore, comprehensive meta-analytical reviews of SEMS placement remain absent. To our knowledge, this meta-analysis represents the inaugural effort to elucidate the correlation between surgical approaches and clinical outcomes, aiming to draw significant conclusions through meta-analytical methods.
For primary outcomes, this meta-analysis demonstrated that laparoscopic surgery significantly reduced the rates of overall POCs (RR 0.52; 95% CI 0.37 to 0.72, P < 0.0001). Additionally, there was no significant difference in 30-day mortality when comparing the open surgery group to the laparoscopic group (RR 1.09; 95% CI 0.26 to 4.48; P = 0.95). Hence, laparoscopic surgery post-stent insertion for OCRC patients is deemed safe and viable.
Concerning secondary outcomes, which encompassed perioperative metrics, postprocedural adverse events, and LN dissection, the laparoscopic group showed a reduction in LOS (MD − 3.29; 95% CI − 5.27 to 1.31; P = 0.001), intraoperative blood loss (MD − 25.84, 95% CI − 52.16 to 0.49; P = 0.05), and postoperative SSI (RR 0.47; 95% CI 0.23 to 0.96, P = 0.04) compared to the open surgery group. No significant differences were noted in LN dissection, POI, or AL between the two groups. Open surgery, however, required less operative time than the laparoscopic approach (MD 20.99, 95% CI 2.31 to 39.44; P = 0.03). High heterogeneity in the results for operative time, intraoperative blood loss, and LOS prompted a meta-regression, which identified the type of surgery as the source of this heterogeneity. Consequently, we conducted a subgroup analysis based on this finding for two primary reasons: (1) such analysis significantly reduces heterogeneity and (2) the established approach for curative surgery in colon cancer involves Colectomy with en bloc removal of regional lymph nodes [37]. The resection should encompass a segment of the colon, extending at least 5 cm on either side of the tumor, with the excision of a minimum of 12 lymph nodes [38]. Guided by established protocol [39], TME is a fundamental element of radical rectal cancer surgery. From a clinical perspective, radical surgery is a standardized procedure with considerable practical importance.
Upon stratifying the outcome of operation time and intraoperative blood loss according to surgical type, we found that despite overall results being statistically significant, no significant differences were observed in the radical subgroup. Researchers [40] suggest that the proficiency gain curve for self-taught senior surgeons performing laparoscopic colorectal surgery lies between 100 and 150 procedures. This learning curve might account for why the outcomes of operation time and intraoperative blood loss for the laparoscopic approach were not superior to those of the open approach in the radical subgroup. Other potential factors could include the improved general condition of patients following SEMS implantation, which may not align with the conditions of routine elective patients due to factors, such as intestinal edema and nutritional status, thereby complicating the actual laparoscopic operation. Regrettably, the included studies neither quantified the degree of remission nor conducted a systematic comparison with conventional elective patients. More convincing results might be obtained if future studies grade the degree of obstruction and establish corresponding subgroups for analysis. It is noteworthy that our studies' statistical results related to intraoperative blood loss are highly heterogeneous and the sensitivity analysis results are unreliable. The primary reasons include (1) a lack of standard descriptions for calculating intraoperative blood loss in the studies and (2) the presence of numerous confounding factors during calculation, such as varying amounts of abdominal lavage and intraoperative fluid loss among patients. As such, we recommend treating the result of intraoperative bleeding with caution.
Resection of rectal cancer is technically more challenging than colon cancer resection [41]. A study [42] highlighted that laparoscopic procedures, which often employ long, straight instruments, inherently face limitations during the surgical excision of rectal cancers situated deep within the pelvis. These limitations include a restricted range of motion, diminished dexterity, and uncontrolled traction by assistants. Another study [1] noted similar challenges with laparoscopic surgery for rectal tumors, specifically due to limited pelvic exposure and the inherent limitations of instrumentation in obese patients or male patients with a narrow pelvis. Regrettably, our subgroup analysis could not isolate obstructions caused by rectal cancers due to the paucity of studies focusing solely on obstructive rectal cancer.
Clinical practice guidelines from the AGA [12] stated that despite growing evidence supporting the use of SEMS in left-sided malignant obstructions, concerns remain regarding their application for right-sided or proximal colon tumors due to the technical complexities associated with SEMS insertion in these areas. Most studies have focused on LSOCC and rectal cancers [6], whereas few have reported on right-sided malignant obstructions. Emergency resection is generally considered safe for acute obstructing right-sided colon cancer. The findings of a recent meta-analysis [43] reveal that BTS for right-sided malignant large bowel obstruction (MLBO) yields more favorable short-term outcomes compared to left-sided MLBO. This implies that BTS leads to a decrease in postoperative complications and mortality for right-sided MLBO when compared to emergency resection. While current evidence supports the feasibility of BTS for right-sided obstructive colon cancer, limited studies assessing its safety and effectiveness impede the establishment of definitive conclusions. Unfortunately, our subgroup analysis was also unable to conduct a focused analysis on obstructions caused by right colon cancer due to the absence of independent studies.
Our findings indicate that the laparoscopic group did not exhibit superiority over the open group concerning POI, AL, and LN dissection. Abdominal surgery has been shown to activate muscularis macrophages and inflame the intestinal muscle layer, resulting in compromised contraction and motility [44, 45].. The extent of tissue damage is influenced by the degree of intestinal manipulation and the duration of surgery, thereby affecting the severity of POI. In mice, laparoscopic surgery did not induce intestinal inflammation and POI as compared to standard intestinal manipulation [46, 47]. Open surgery, in contrast to minimally invasive surgery (MIS), has been shown to substantially increase the likelihood of POI, with OR ranging from 1.97 to 6.37 [48]. However, our research yielded a divergent result, indicating no statistically significant difference between the two groups.
Incomplete resolution of bowel wall edema is posited to contribute to the incidence of AL. AL continues to pose a significant risk to patients, particularly at high-risk sites, such as colorectal areas [49]. Limitations of minimal access intracorporeal anastomosis include the absence of direct tactile sensation, insufficient exposure, and a suboptimal cutting angle of the endo-linear stapler [50]. Recent meta-analyses [1, 51] comparing techniques for rectal cancer resection found no significant difference in anastomotic leak between the laparoscopic and open approaches. Conversely, a meta-analysis by Qu et al. [52] suggested that laparoscopy may be associated with a lower risk of AL than open surgery. Our research concurred with the former, finding no statistical difference between the two groups. One potential explanation is that laparoscopic surgery inflicts less tissue trauma and is correlated with more favorable immunological outcomes and a reduced inflammatory response, potentially enhancing anastomotic healing and decreasing leakage rates. However, laparoscopic surgeries, particularly in rectal cancers with a narrow pelvis, may tend to employ multiple staplers.
In open surgery, anastomotic tension can be readily evaluated before anastomosis, often leading to additional proximal resection beyond the oncological safety margin. Conversely, in laparoscopic surgery, the extent of proximal resection is constrained by the requirement for tension-free anastomosis when planning an anastomosis. Despite the potential challenges posed by the use of in-line instrumentation in the pelvis during laparoscopic surgery, the benefits of enhanced access and visualization in the mid to lower rectum should not be overlooked [53]. Several meta-analyses have compared techniques for rectal cancer resection and found no significant difference in the number of nodes retrieved between laparoscopic and open methods [1, 54]. An RCT [55] on stage II/III colon cancer reported no significant differences in the number of dissected LN between open surgery and laparoscopic surgery groups. Another study [51] showed fewer dissected LN in the laparoscopic group for advanced low rectal cancer compared to the open group. However, our results found no significant difference between the two groups.
The optimal time interval between stent implantation and subsequent surgery for patients with OCRC remains undefined [56]. This variable, which is within our control, influences surgical strategy and impacts tumor prognosis. Some research [7, 57] suggests a higher risk of AL when the interval between SEMS placement and surgery is brief. An extremely short time interval (< 7 days) appears associated with POCs due to insufficient intestinal decompression and systemic recovery [58]. A longer gap between SEMS insertion and surgery allows patient condition stabilization, accurate disease staging, effective bowel decompression, and resolution of bowel obstruction symptoms, possibly leading to improved surgical outcomes in a BTS setting [59]. However, a longer duration of stent placement could theoretically cause silent and micro-perforations, leading to tumor cell dissemination through the bloodstream and poorer oncological outcomes [35]. One retrospective cohort study [60] suggested that longer intervals (> 14 days) between SEMS placement and surgery did not affect surgical difficulty but improved the rate of primary anastomosis and reduced the rate of stoma creation and postoperative complications. Ho et al. [61] reported an increased risk of surgery if the interval exceeded two weeks due to significant peritumor inflammation and fibrotic adhesions caused by the SEMS. Some studies [62, 63] have also found no correlation between varying time intervals and postoperative complications. A recent meta-analysis [43] reveals that an interval of 20 days or more between the placement of SEMS and surgery significantly lowers the occurrence of postoperative complications. An extensive national cohort study [64] of patients diagnosed with LSOCC indicates that achieving an optimal equilibrium between SEMS-related complications and patient recovery, under optimized surgical conditions, is likely attained by scheduling the resection approximately 2 weeks after successful SEMS placement. The ESGE guideline [6] recommends the use of uncovered SEMS in the curative setting and a two-week interval between colonic SEMS placement and resection. The guideline also notes the lack of high-quality literature to grade obstruction severity. The timing of surgery following colonic stenting must consider the balance between stent-related adverse events (reduced by a short interval) and surgical outcomes (improved by a longer delay). Accurate grading of obstruction before and after SEMS placement may guide the length of this interval. Exploring the specific bridging interval for obstructive malignant tumors at different sites of the large bowel (left side, right side, and rectum) may necessitate further investigation.
Chemotherapy reduces the risk of tumor ingrowth compared to SEMS use alone; however, it is also associated with long-term complications, like perforation and stent migration. The decision to combine neoadjuvant chemotherapy during the interval as a treatment is poorly studied [58]. A meta-analysis [65] indicated that neoadjuvant chemotherapy (NAC) was not associated with improved survival outcomes, despite its safety and feasibility in perioperative management. There is also a potential risk of emergency surgery during NAC, particularly in patients with tumor progression or adverse conditions due to chemotherapy. Further optimization of clinical staging is crucial to accurately identify patients who may benefit from neoadjuvant therapy and avoid overtreatment of low-risk patients.
This study acknowledges several limitations that warrant consideration: (1) Conducting RCTs for patients with OCRC is challenging. Consequently, the studies included in this article are either retrospective or prospective cohort studies. As a result of these research design constraints, there may be a high risk of selection, implementation, and measurement biases. Patients with complete obstruction may not attempt stent placement. Furthermore, during the pre-operative evaluation following stent implantation, if a patient is deemed at high surgical risk, the surgical plan may be modified to avoid elective surgery. Currently, there is no objective standard for determining the surgical approach, and the choice between open surgery and laparoscopic surgery is largely dependent on the surgeon's preference, potentially causing selection bias. Additionally, the varying quality of studies and insufficient sample sizes in some may undermine the credibility of the results; (2) there is heterogeneity in the population definition and some outcome indicators included in the study. The limited number of studies precludes further subgroup analysis based on factors, such as tumor location, specific operation mode, interval between stent insertion and operation, stent type, obstruction degree, and relief degree of obstruction post-stent implantation. These areas represent directions for future research; (3) the clinicians involved in the SEMS program differ. Stenting is performed by endoscopists, interventional radiologists, and colorectal surgeons. Owing to the lack of detailed information on endoscopic physician composition in most studies, meaningful comparisons between different clinician groups are unfeasible; (4) most of the studies included do not specify clear follow-up times or have short follow-up periods, limiting the evaluation of equivalent later indicators, and the long-term effects remain uncertain.
Conclusion
In summary, for patients diagnosed with OCRC, laparoscopic surgery marginally outperforms open surgery by diminishing postoperative risks and abbreviating hospital stays. However, to substantiate these findings, research of superior quality is imperative. Furthermore, it is essential to ascertain the ideal interval between stent implantation and surgery, as well as to refine the clinical staging of patients for a more precise evaluation of neoadjuvant therapy risks.
References
Simillis C, Lal N, Thoukididou SN, Kontovounisios C, Smith JJ, Hompes R, Adamina M, Tekkis PP (2019) Open versus laparoscopic versus robotic versus transanal mesorectal excision for rectal cancer: a systematic review and network meta-analysis. Ann Surg 270:59–68. https://doi.org/10.1097/sla.0000000000003227
Coker OO, Nakatsu G, Dai RZ, Wu WKK, Wong SH, Ng SC, Chan FKL, Sung JJY, Yu J (2019) Enteric fungal microbiota dysbiosis and ecological alterations in colorectal cancer. Gut 68:654–662. https://doi.org/10.1136/gutjnl-2018-317178
Veld JV, Amelung FJ, Borstlap WAA, Eise van Halsema E, Consten ECJ, Siersema PD, Ter Borg F, Silvester van der Zaag E, Fockens P, Bemelman WA, Elise van Hooft J, Tanis PJ (2019) Changes in management of left-sided obstructive colon cancer: National Practice and Guideline Implementation. J Natl Compr Cancer Netw 17:1512–1520. https://doi.org/10.6004/jnccn.2019.7326
Abelson JS, Yeo HL, Mao J, Milsom JW, Sedrakyan A (2017) Long-term postprocedural outcomes of palliative emergency stenting vs stoma in malignant large-bowel obstruction. JAMA Surg 152:429–435. https://doi.org/10.1001/jamasurg.2016.5043
Veld JV, Amelung FJ, Borstlap WAA, van Halsema EE, Consten ECJ, Siersema PD, Ter Borg F, van der Zaag ES, de Wilt JHW, Fockens P, Bemelman WA, van Hooft JE, Tanis PJ (2020) Comparison of decompressing stoma vs stent as a bridge to surgery for left-sided obstructive colon cancer. JAMA Surg 155:206–215. https://doi.org/10.1001/jamasurg.2019.5466
van Hooft JE, Veld JV, Arnold D, Beets-Tan RGH, Everett S, Götz M, van Halsema EE, Hill J, Manes G, Meisner S, Rodrigues-Pinto E, Sabbagh C, Vandervoort J, Tanis PJ, Vanbiervliet G, Arezzo A (2020) Self-expandable metal stents for obstructing colonic and extracolonic cancer: European Society of Gastrointestinal Endoscopy (ESGE) Guideline—Update 2020. Endoscopy 52:389–407. https://doi.org/10.1055/a-1140-3017
van Hooft JE, Bemelman WA, Oldenburg B, Marinelli AW, Lutke Holzik MF, Grubben MJ, Sprangers MA, Dijkgraaf MG, Fockens P (2011) Colonic stenting versus emergency surgery for acute left-sided malignant colonic obstruction: a multicentre randomised trial. Lancet Oncol 12:344–352. https://doi.org/10.1016/s1470-2045(11)70035-3
Papachrysos N, Shafazand M, Alkelin L, Kilincalp S, de Lange T (2023) Outcome of self-expandable metal stents placement for obstructive colorectal cancer: 7 years’ experience from a Swedish tertiary center. Surg Endosc 37:2653–2658. https://doi.org/10.1007/s00464-022-09761-2
Vallance AE, Keller DS, Hill J, Braun M, Kuryba A, van der Meulen J, Walker K, Chand M (2019) Role of emergency laparoscopic colectomy for colorectal cancer: a population-based study in England. Ann Surg 270:172–179. https://doi.org/10.1097/sla.0000000000002752
Puértolas S, Navallas D, Herrera A, López E, Millastre J, Ibarz E, Gabarre S, Puértolas JA, Gracia L (2017) A methodology for the customized design of colonic stents based on a parametric model. J Mech Behav Biomed Mater 71:250–261. https://doi.org/10.1016/j.jmbbm.2017.03.023
Lim T, Tham HY, Yaow CYL, Tan IJ, Chan DKH, Farouk R, Lee KC, Lieske B, Tan KK, Chong CS (2021) Early surgery after bridge-to-surgery stenting for malignant bowel obstruction is associated with better oncological outcomes. Surg Endosc 35:7120–7130. https://doi.org/10.1007/s00464-020-08232-w
Ahmed O, Lee JH, Thompson CC, Faulx A (2021) AGA clinical practice update on the optimal management of the malignant alimentary tract obstruction: expert review. Clin Gastroenterol Hepatol 19:1780–1788. https://doi.org/10.1016/j.cgh.2021.03.046
Amelung FJ, Borstlap WAA, Consten ECJ, Veld JV, van Halsema EE, Bemelman WA, Siersema PD, Ter Borg F, van Hooft JE, Tanis PJ (2019) Propensity score-matched analysis of oncological outcome between stent as bridge to surgery and emergency resection in patients with malignant left-sided colonic obstruction. Br J Surg 106:1075–1086. https://doi.org/10.1002/bjs.11172
Arezzo A, Passera R, Lo Secco G, Verra M, Bonino MA, Targarona E, Morino M (2017) Stent as bridge to surgery for left-sided malignant colonic obstruction reduces adverse events and stoma rate compared with emergency surgery: results of a systematic review and meta-analysis of randomized controlled trials. Gastrointest Endosc 86:416–426. https://doi.org/10.1016/j.gie.2017.03.1542
Atukorale YN, Church JL, Hoggan BL, Lambert RS, Gurgacz SL, Goodall S, Maddern GJ (2016) Self-expanding metallic stents for the management of emergency malignant large bowel obstruction: a systematic review. J Gastrointest Surg 20:455–462. https://doi.org/10.1007/s11605-015-2997-7
Zhou JM, Yao LQ, Xu JM, Xu MD, Zhou PH, Chen WF, Shi Q, Ren Z, Chen T, Zhong YS (2013) Self-expandable metallic stent placement plus laparoscopy for acute malignant colorectal obstruction. World J Gastroenterol 19:5513–5519. https://doi.org/10.3748/wjg.v19.i33.5513
Han JG, Wang ZJ, Zeng WG, Wang YB, Wei GH, Zhai ZW, Zhao BC, Yi BQ (2020) Efficacy and safety of self-expanding metallic stent placement followed by neoadjuvant chemotherapy and scheduled surgery for treatment of obstructing left-sided colonic cancer. BMC Cancer 20:57. https://doi.org/10.1186/s12885-020-6560-x
Hiyoshi Y, Mukai T, Nagasaki T, Yamaguchi T, Nagayama S, Akiyoshi T, Sasaki T, Saito S, Fukunaga Y (2021) Treatment outcome of laparoscopic surgery after self-expandable metallic stent insertion for obstructive colorectal cancer. Int J Clin Oncol 26:2029–2036. https://doi.org/10.1007/s10147-021-01990-0
Cumpston M, Li T, Page MJ, Chandler J, Welch VA, Higgins JP, Thomas J (2019) Updated guidance for trusted systematic reviews: a new edition of the Cochrane Handbook for Systematic Reviews of Interventions. Cochrane Database Syst Rev 2019(10):142. https://doi.org/10.1002/14651858.Ed000142
Page MJ, Moher D, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, Shamseer L, Tetzlaff JM, Akl EA, Brennan SE, Chou R, Glanville J, Grimshaw JM, Hróbjartsson A, Lalu MM, Li T, Loder EW, Mayo-Wilson E, McDonald S, McGuinness LA, Stewart LA, Thomas J, Tricco AC, Welch VA, Whiting P, McKenzie JE (2021) PRISMA 2020 explanation and elaboration: updated guidance and exemplars for reporting systematic reviews. BMJ (Clinical Research Ed) 372:n160. https://doi.org/10.1136/bmj.n160
Stang A (2010) Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol 25:603–605. https://doi.org/10.1007/s10654-010-9491-z
Hozo SP, Djulbegovic B, Hozo I (2005) Estimating the mean and variance from the median, range, and the size of a sample. BMC Med Res Methodol 5:13. https://doi.org/10.1186/1471-2288-5-13
Cheung HY, Chung CC, Tsang WW, Wong JC, Yau KK, Li MK (2009) Endolaparoscopic approach vs conventional open surgery in the treatment of obstructing left-sided colon cancer: a randomized controlled trial. Arch Surg (Chicago, Ill: 1960) 144:1127–1132. https://doi.org/10.1001/archsurg.2009.216
Hajime M, Tomohiko A, Takashi H, Hiroki M, Tohei Y, Hitomi I, Takashi G, Toru I, Susumu EJIS (2017) Elective surgery after endoscopic self-expandable metallic stent placement for patients with obstructive colon cancer: preoperative systemic evaluation and management. Int Surg 102:21–28
Chung TS, Lim SB, Sohn DK, Hong CW, Han KS, Choi HS, Jeong SY (2008) Feasibility of single-stage laparoscopic resection after placement of a self-expandable metallic stent for obstructive left colorectal cancer. World J Surg 32:2275–2280. https://doi.org/10.1007/s00268-008-9695-5
Bae SU, Yang CS, Kim S, Lim DR, Jeong WK, Dong Kim D, Kim JH, Shin EJ, Lee YJ, Lee JY, Kim NK, Baek SK (2019) Long-term oncologic outcomes of laparoscopic versus open resection following stent insertion for obstructing colon cancer: a multi-center retrospective study. Surg Endosc 33:3937–3944. https://doi.org/10.1007/s00464-019-06680-7
Stipa F, Pigazzi A, Bascone B, Cimitan A, Villotti G, Burza A, Vitale A (2008) Management of obstructive colorectal cancer with endoscopic stenting followed by single-stage surgery: open or laparoscopic resection? Surg Endosc 22:1477–1481. https://doi.org/10.1007/s00464-007-9654-5
Yang SY, Park YY, Han YD, Cho MS, Hur H, Min BS, Lee KY, Kim NK (2019) Oncologic outcomes of self-expandable metallic stent as a bridge to surgery and safety and feasibility of minimally invasive surgery for acute malignant colonic obstruction. Ann Surg Oncol 26:2787–2796. https://doi.org/10.1245/s10434-019-07346-3
Kim MH, Kang SI, Lee J, Oh HK, Ahn S, Kim DW, Kang SB, Shin R, Heo SC, Youk EG, Park SC, Sohn DK, Oh JH, Kim MJ, Park JW, Ryoo SB, Jeong SY, Park KJ (2022) Oncologic safety of laparoscopic surgery after metallic stent insertion for obstructive left-sided colorectal cancer: a multicenter comparative study. Surg Endosc 36:385–395. https://doi.org/10.1007/s00464-021-08293-5
Enomoto T, Saida Y, Takabayashi K, Nagao S, Takeshita E, Watanabe R, Takahashi A, Nakamura Y, Asai K, Watanebe M, Nagao J, Kusachi S (2016) Open surgery versus laparoscopic surgery after stent insertion for obstructive colorectal cancer. Surg Today 46:1383–1386. https://doi.org/10.1007/s00595-016-1331-7
Li ZX, Wu XH, Wu HY, Chang WJ, Chang XJ, Yi T, Shi Q, Chen JW, Feng QY, Zhu DX, Wei Y, Zhong YS, Xu JM (2016) Self-expandable metallic stent as a bridge to elective surgery versus emergency surgery for acute malignant colorectal obstruction. Int J Colorectal Dis 31:561–570. https://doi.org/10.1007/s00384-015-2476-3
Tajima JY, Matsuhashi N, Takahashi T, Mizutani C, Iwata Y, Kiyama S, Kubota M, Ibuka T, Araki H, Shimizu M, Doi K, Yoshida K (2020) Short- and long-term outcomes after colonic self-expandable metal stent placement for malignant large-bowel obstruction as a bridge to surgery focus on the feasibility of the laparoscopic approach: a retrospective, single center study. World J Surg Oncol 18:265. https://doi.org/10.1186/s12957-020-02039-8
Lu Q, Lan Q, Chen L, Xu D, Li J, Lin S, Que C, Chen J (2017) Endoscopic metallic stent followed by elective laparoscopic surgery for malignant colorectal obstruction. Zhonghua wei chang wai ke za zhi = Chin J Gastrointest Surg 20:684–688
Law WL, Poon JT, Fan JK, Lo OS (2013) Colorectal resection after stent insertion for obstructing cancer: comparison between open and laparoscopic approaches. Surg Laparosc Endosc Percutaneous Tech 23:29–32. https://doi.org/10.1097/SLE.0b013e318275743b
Maruthachalam K, Lash GE, Shenton BK, Horgan AF (2007) Tumour cell dissemination following endoscopic stent insertion. Br J Surg 94:1151–1154. https://doi.org/10.1002/bjs.5790
Song LM, Baron TH (2011) Stenting for acute malignant colonic obstruction: a bridge to nowhere? Lancet Oncol 12:314–315. https://doi.org/10.1016/s1470-2045(11)70059-6
Benson AB, Venook AP, Al-Hawary MM, Arain MA, Chen YJ, Ciombor KK, Cohen S, Cooper HS, Deming D, Farkas L, Garrido-Laguna I, Grem JL, Gunn A, Hecht JR, Hoffe S, Hubbard J, Hunt S, Johung KL, Kirilcuk N, Krishnamurthi S, Messersmith WA, Meyerhardt J, Miller ED, Mulcahy MF, Nurkin S, Overman MJ, Parikh A, Patel H, Pedersen K, Saltz L, Schneider C, Shibata D, Skibber JM, Sofocleous CT, Stoffel EM, Stotsky-Himelfarb E, Willett CG, Gregory KM, Gurski LA (2021) Colon cancer, Version 2.2021, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Cancer Netw 19:329–359. https://doi.org/10.6004/jnccn.2021.0012
Le Voyer TE, Sigurdson ER, Hanlon AL, Mayer RJ, Macdonald JS, Catalano PJ, Haller DG (2003) Colon cancer survival is associated with increasing number of lymph nodes analyzed: a secondary survey of intergroup trial INT-0089. J Clin Oncol 21:2912–2919. https://doi.org/10.1200/jco.2003.05.062
Benson AB, Venook AP, Al-Hawary MM, Azad N, Chen YJ, Ciombor KK, Cohen S, Cooper HS, Deming D, Garrido-Laguna I, Grem JL, Gunn A, Hecht JR, Hoffe S, Hubbard J, Hunt S, Jeck W, Johung KL, Kirilcuk N, Krishnamurthi S, Maratt JK, Messersmith WA, Meyerhardt J, Miller ED, Mulcahy MF, Nurkin S, Overman MJ, Parikh A, Patel H, Pedersen K, Saltz L, Schneider C, Shibata D, Skibber JM, Sofocleous CT, Stotsky-Himelfarb E, Tavakkoli A, Willett CG, Gregory K, Gurski L (2022) Rectal cancer, version 2.2022, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Cancer Netw 20:1139–1167. https://doi.org/10.6004/jnccn.2022.0051
Mackenzie H, Miskovic D, Ni M, Parvaiz A, Acheson AG, Jenkins JT, Griffith J, Coleman MG, Hanna GB (2013) Clinical and educational proficiency gain of supervised laparoscopic colorectal surgical trainees. Surg Endosc 27:2704–2711. https://doi.org/10.1007/s00464-013-2806-x
Hui VW, Guillem JG (2014) Minimal access surgery for rectal cancer: an update. Nat Rev Gastroenterol Hepatol 11:158–165. https://doi.org/10.1038/nrgastro.2013.203
Stefanidis D, Wang F, Korndorffer JR Jr, Dunne JB, Scott DJ (2010) Robotic assistance improves intracorporeal suturing performance and safety in the operating room while decreasing operator workload. Surg Endosc 24:377–382. https://doi.org/10.1007/s00464-009-0578-0
Kanaka S, Matsuda A, Yamada T, Ohta R, Sonoda H, Shinji S, Takahashi G, Iwai T, Takeda K, Ueda K, Kuriyama S, Miyasaka T, Yoshida H (2022) Colonic stent as a bridge to surgery versus emergency resection for right-sided malignant large bowel obstruction: a meta-analysis. Surg Endosc 36:2760–2770. https://doi.org/10.1007/s00464-022-09071-7
Thomas H (2019) Prucalopride before surgery alleviates postoperative ileus. Nat Rev Gastroenterol Hepatol 16:76. https://doi.org/10.1038/s41575-019-0106-1
Pohl JM, Gutweiler S, Thiebes S, Volke JK, Klein-Hitpass L, Zwanziger D, Gunzer M, Jung S, Agace WW, Kurts C, Engel DR (2017) Irf4-dependent CD103 (+)CD11b (+) dendritic cells and the intestinal microbiome regulate monocyte and macrophage activation and intestinal peristalsis in postoperative ileus. Gut 66:2110–2120. https://doi.org/10.1136/gutjnl-2017-313856
Gomez-Pinilla PJ, Farro G, Di Giovangiulio M, Stakenborg N, Némethova A, de Vries A, Liston A, Feyerabend TB, Rodewald HR, Boeckxstaens GE, Matteoli G (2014) Mast cells play no role in the pathogenesis of postoperative ileus induced by intestinal manipulation. PLoS ONE 9:e85304. https://doi.org/10.1371/journal.pone.0085304
Gomez-Pinilla PJ, Binda MM, Lissens A, Di Giovangiulio M, van Bree SH, Nemethova A, Stakenborg N, Farro G, Bosmans G, Matteoli G, Deprest J, Boeckxstaens GE (2014) Absence of intestinal inflammation and postoperative ileus in a mouse model of laparoscopic surgery. Neurogastroenterol Motil 26:1238–1247. https://doi.org/10.1111/nmo.12376
Sommer NP, Schneider R, Wehner S, Kalff JC, Vilz TO (2021) State-of-the-art colorectal disease: postoperative ileus. Int J Colorectal Dis 36:2017–2025. https://doi.org/10.1007/s00384-021-03939-1
Jacobson RA, Williamson AJ, Wienholts K, Gaines S, Hyoju S, van Goor H, Zaborin A, Shogan BD, Zaborina O, Alverdy JC (2021) Prevention of anastomotic leak via local application of tranexamic acid to target bacterial-mediated plasminogen activation: a practical solution to a complex problem. Ann Surg 274:e1038–e1046. https://doi.org/10.1097/sla.0000000000003733
Penna M, Hompes R, Arnold S, Wynn G, Austin R, Warusavitarne J, Moran B, Hanna GB, Mortensen NJ, Tekkis PP (2019) Incidence and risk factors for anastomotic failure in 1594 patients treated by transanal total mesorectal excision: results from the International TaTME Registry. Ann Surg 269:700–711. https://doi.org/10.1097/sla.0000000000002653
Hida K, Okamura R, Sakai Y, Konishi T, Akagi T, Yamaguchi T, Akiyoshi T, Fukuda M, Yamamoto S, Yamamoto M, Nishigori T, Kawada K, Hasegawa S, Morita S, Watanabe M (2018) Open versus laparoscopic surgery for advanced low rectal cancer: a large, multicenter, propensity score matched cohort study in Japan. Ann Surg 268:318–324. https://doi.org/10.1097/sla.0000000000002329
Qu H, Liu Y, Bi DS (2015) Clinical risk factors for anastomotic leakage after laparoscopic anterior resection for rectal cancer: a systematic review and meta-analysis. Surg Endosc 29:3608–3617. https://doi.org/10.1007/s00464-015-4117-x
Sujatha-Bhaskar S, Jafari MD, Gahagan JV, Inaba CS, Koh CY, Mills SD, Carmichael JC, Stamos MJ, Pigazzi A (2017) Defining the role of minimally invasive proctectomy for locally advanced rectal adenocarcinoma. Ann Surg 266:574–581. https://doi.org/10.1097/sla.0000000000002357
Martínez-Pérez A, Carra MC, Brunetti F (2017) Pathologic outcomes of laparoscopic vs open mesorectal excision for rectal cancer: a systematic review and meta-analysis. JAMA Surg 152:e165665. https://doi.org/10.1001/jamasurg.2016.5665
Yamamoto S, Inomata M, Katayama H, Mizusawa J, Etoh T, Konishi F, Sugihara K, Watanabe M, Moriya Y, Kitano S (2014) Short-term surgical outcomes from a randomized controlled trial to evaluate laparoscopic and open D3 dissection for stage II/III colon cancer: Japan Clinical Oncology Group Study JCOG 0404. Ann Surg 260:23–30. https://doi.org/10.1097/sla.0000000000000499
Neo VSQ, Jain SR, Yeo JW, Ng CH, Gan TRX, Tan E, Chong CS (2021) Controversies of colonic stenting in obstructive left colorectal cancer: a critical analysis with meta-analysis and meta-regression. Int J Colorectal Dis 36:689–700. https://doi.org/10.1007/s00384-021-03834-9
Lee GJ, Kim HJ, Baek JH, Lee WS, Kwon KA (2013) Comparison of short-term outcomes after elective surgery following endoscopic stent insertion and emergency surgery for obstructive colorectal cancer. Int J Surg (London, England) 11:442–446. https://doi.org/10.1016/j.ijsu.2013.04.010
Ormando VM, Palma R, Fugazza A, Repici A (2019) Colonic stents for malignant bowel obstruction: current status and future prospects. Expert Rev Med Devices 16:1053–1061. https://doi.org/10.1080/17434440.2019.1697229
Lim TZ, Chan DKH, Tan KK (2018) Endoscopic stenting should be advocated in patients with stage IV colorectal cancer presenting with acute obstruction. J Gastrointest Oncol 9:785–790. https://doi.org/10.21037/jgo.2018.06.03
Chen S, Zhou S, Lin Y, Xue W, Huang Z, Yu J, Yu Z, Chen S (2022) Self-expandable metal stent as a bridge to surgery for left-sided acute malignant colorectal obstruction: optimal timing for elective surgery. Comput Math Methods Med 2022:6015729. https://doi.org/10.1155/2022/6015729
Ho KS, Quah HM, Lim JF, Tang CL, Eu KW (2012) Endoscopic stenting and elective surgery versus emergency surgery for left-sided malignant colonic obstruction: a prospective randomized trial. Int J Colorectal Dis 27:355–362. https://doi.org/10.1007/s00384-011-1331-4
Mu C, Chen L (2023) A retrospective evaluation of short-term results from colonic stenting as a bridge to elective surgery versus emergency surgery for malignant colonic obstruction. Sci Rep 13:1600. https://doi.org/10.1038/s41598-023-28685-y
Gianotti L, Tamini N, Nespoli L, Rota M, Bolzonaro E, Frego R, Redaelli A, Antolini L, Ardito A, Nespoli A, Dinelli M (2013) A prospective evaluation of short-term and long-term results from colonic stenting for palliation or as a bridge to elective operation versus immediate surgery for large-bowel obstruction. Surg Endosc 27:832–842. https://doi.org/10.1007/s00464-012-2520-0
Veld JV, Kumcu A, Amelung FJ, Borstlap WAA, Consten ECJ, Dekker JWT, van Westreenen HL, Siersema PD, Ter Borg F, Kusters M, Bemelman WA, de Wilt JHW, van Hooft JE, Tanis PJ (2021) Time interval between self-expandable metal stent placement or creation of a decompressing stoma and elective resection of left-sided obstructive colon cancer. Endoscopy 53:905–913. https://doi.org/10.1055/a-1308-1487
Liang Z, Li Z, Yang Q, Feng J, Xiang D, Lyu H, Mai G, Wang W (2022) The role of neoadjuvant chemotherapy in patients with locally advanced colon cancer: a systematic review and meta-analysis. Front Oncol 12:1024345. https://doi.org/10.3389/fonc.2022.1024345
Acknowledgements
Not applicable.
Funding
No funding was received.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
Mr. Kerui Zeng, Mr. Faqiang Zhang, Dr. Hua Yang, Mrs. Xiaoying Zha, and Shixu Fang have no conflicts of interest or financial ties to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Zeng, K., Zhang, F., Yang, H. et al. Laparoscopic versus open surgery in obstructive colorectal cancer patients following stents placement: a comprehensive meta-analysis of cohort studies. Surg Endosc 38, 1740–1757 (2024). https://doi.org/10.1007/s00464-024-10710-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-024-10710-4