
Abstract
Background
A direct comparison of the cost–benefit analysis of retroperitoneoscopic adrenalectomy (RPA) versus the minimally invasive transperitoneal access (LTA) approach is currently lacking. We hypothesized that RPA is more cost effective than LTA; promising significant savings for the healthcare system in an era of ever more limited resources.
Methods
We performed a monocentric retrospective observational cohort study based on data from our Endocrine Surgery Registry. Patients who were operated upon between 2019 and 2022 were included. After pair-matching, both cohorts (RPA vs. LTA) were compared for perioperative variables and treatment costs (process cost calculation), revenue and profit.
Results
Two homogenous cohorts of 43 patients each (RPA vs. LTA) were identified following matching. Patient characteristics between the cohorts were comparable. In terms of both treatment-associated costs and profit, the RPA procedure was superior to LTA (costs: US$5789.99 for RPA vs. US$6617.75 for LTA, P = 0.043; profit: US$1235.59 for RPA vs. US$653.33 for LTA, P = 0.027). The duration of inpatient treatment and comorbidities significantly influenced the cost of treatment and the overall profit.
Conclusions
RPA appears not only to offer benefits over LTA in terms of perioperative morbidity and length of hospital stay, but also has a superior financial cost/benefit profile.
Graphical abstract

Similar content being viewed by others

Avoid common mistakes on your manuscript.
Health care costs have risen dramatically in recent decades and now account for a significant proportion of the global gross domestic product (GDP) (17% of the country’s GDP in the United States or Europe) [1]. In Germany, gross value added (GVA) in the core sector of the health care amounted to almost €441 billion in 2020, more than 13.1% of the country’s GDP [2]. With an annual growth rate of 3.3%, the health sector has grown significantly faster than GDP over the past decade [3] with surgical care accounting for almost one third of healthcare expenditure [4, 5]. As surgically treatable diseases are expected to account for two thirds of the global lost years by 2025 [6], efforts to investigate and control costs would be wise to focus on surgical care, particularly in the area of minimally invasive surgery, where highly specialized tools may potentially lead to higher costs than traditional open surgery.
However, economic studies attempting to ascertain the cost/benefit profile of surgical interventions face several challenges, including the absence of benchmarks (e.g. costs of care in the operating room, costs per time in the radiology) and a lack of consensus of what contributes to the overall costs [7]. This is further complicated by a lack of published literature on which cost estimation models are most suitable [4, 8,9,10,11,12,13,14,15]. While some of the operative and perioperative costs associated with retroperitoneoscopic adrenalectomy (RPA) and the minimally invasive transperitoneal access approach (LTA) have been reported [16], a comprehensive cost–benefit analysis directly comparing both procedures is lacking. Moreover, the published literature does not address revenue and profit.
Meta-analyses proved RPA to be associated with lower long-term complications, a shorter hospital stay and duration of surgery and less postoperative pain [16,17,18,19,20,21,22]. Therefore, the aim of our study was to test the hypothesis that RPA is less expensive and eventually leads to more profit than the standard minimally invasive method (LTA) employing a global, process-oriented assessment of costs, revenue and profit.
Patients and methods
Study design and patients
This was a retrospective monocentric observational cohort study. All patients included in this study underwent minimally invasive adrenalectomy without robotic assistance. Patient, procedure and follow-up data were prospectively collected and maintained in our Registry for Endocrine Surgery between 2012 and 2022 (Department of General, Visceral and Transplant Surgery). In order to ensure consistent data, only patients treated between 2019 and 2022 were investigated. Preoperative screening and assessment of patients was performed by a multidisciplinary team, consisting of endocrine surgeons, endocrinologists, internists and radiologists, all with experience in assessing patients before and after adrenal surgery. Our investigation has been reported in line with the CHEERS and STROCSS criteria (Supplementary Files 1, 2) [23, 24].
Patients and surgical technique
All patients were operated on by experienced and certified endocrine surgeons (DGAV Certification: Reference Center for Endocrine Surgery) [25]. The minimally invasive surgical techniques (LTA and RPA) which were adopted complied with guidelines of the American Association of Endocrine Surgeons (AAES) [26], the German Association of Endocrine Surgeons (CAEK) [27] and Society of the American Gastrointestinal and Endoscopic Surgeons (SAGES) [28]. These techniques have been described previously [29,30,31]. The choice of surgical technique was left to the patient, after having been informed of the surgical details of the technique and after having ensured that both techniques were applicable.
Methods
The comparability of the two groups (LTA vs. RPA) in terms of perioperative variables was tested after matching (see “Statistical analysis” section). Two aspects were taken into account to test our hypothesis: (1) the calculation of the costs incurred by both surgical techniques and (2) the calculation of the revenue/profit.
Perioperative patient characteristics
The evaluation of clinical, laboratory and imaging patient data was performed retrospectively using the above mentioned database. Operative time was measured from incision to skin closure. Postoperative complications were coded according to the Clavien–Dindo classification [32].
Calculation of the revenue
The revenue calculation for each patient was performed retrospectively using the German Diagnosis Related Groups (gDRG) codes. These codes represent a classification system to match financial reimbursement according to each inpatient case. gDRG covers all operational costs incurred during the stay. The calculation of the revenue (R) was based for each patient on its relative treatment weight and the gDRG base rate, according to the formula [33]:
Deductions and supplements may apply for both groups (RPA vs. LTA). Two calculation methods were used: (1) the patient gDRG masks were grouped in the hospital information system (ISH med® system, SAP SE, Dietmar-Hopp-Allee 16, 69190 Walldorf, Germany) and calculated retrospectively; (2) as a control, a query was carried out in our accounting system. Both values were examined for plausibility and compared for each patient.
Calculation of the costs
A process cost calculation was used (health economic analysis plan). That calculation was structured in three stages: (1) process analysis, (2) identification of process variables (cost drivers) and (3) cost analysis [34, 35]. The process analysis was carried out on the basis of a personal survey of the cost center managers: (1) the nursing department, (2) the lead surgeon, (3) the lead anesthetist, (4) the radiologist, (5) a physiotherapist, (6) the head of the laboratory medicine department, (7) the lead pharmacist and (8) the commercial head of the surgical clinic. The process variables (cost drivers) (e.g. case numbers, number of patients, length of stay or duration of treatment [35]) were defined and evaluated (using InEK cost matrix [33]). Resource utilization was then used to calculate the process cost rates. The full cost recalculation could than been carried out. Adjustment were made for inflation. The individual costs were allocated directly to the patients on the basis of the documented consumption of medical goods (e.g. medicines, surgical instruments, surgery time). In the allocation of overhead costs, the case-related cost allocation was carried out via a process or reference calculation. The calculation rates were calculated on the basis of suitable reference quantities, such as the PPR minutes for the personnel costs of the nursing service for the normal ward.
Calculation of the profit
After revenue and cost analysis, a profit analysis was carried out. Profit was defined as the difference between revenue and costs. The profit was calculated for each individual case (patient), so that both positive and negative profit values could be calculated. The profit was calculated on a case-by-case basis, so that both positive and negative profit values were calculated. Subsequently, a statistical comparison between the two procedures (RPA vs. LTA) was performed.
Statistical analysis
Graphpad Prism 9 software, version 9. 3. 1 (350) (Graphpad Software, 2365 Northside Dr. Suite 560, San Diego, CA, 92108) was used for statistical analysis. Statistical advice was provided by the biostatistics department of our university surgical clinic.
Patient pair-matching
Pair matching was performed to be able to compare the cost, revenue and profit data among groups (RPA vs. LTA) and to minimize confounding bias. The surgical procedure used (RPA vs. LTA) was recorded as a dependent variable in the matching model and age (± 5 years), gender, body mass index BMI (± 5 kg/m2), presence of comorbidities (Charlson Comorbidity Index, CCI) (≤ 1 point) as independent covariates [36]. Tumors up to 4 cm in diameter were operated on in our series. Studies have shown that the laterality and size of adrenal tumors (for tumors < 6 cm) did not affect the duration of surgery or postoperative morbidity, either for LTA or RPA. Therefore, these two variables were not included as independent variables in our matching [37,38,39].
Analysis of endpoint variables
The normality of the distribution was investigated with the Kolmogorov Smirnov test. Normally distributed quantitative variables were described using the mean with standard deviation (SD), and not normally distributed quantitative variables using the median with interquartile range (IQR). Categorical variables were described in absolute numbers and percentages. Differences between groups were analyzed for quantitative normally distributed variables with a one-way ANOVA test, with a Mann–Whitney U test for quantitative non-normally distributed variables and with χ2 or Fischer’s Exact test for categorical variables. In order to investigate the significant influence parameters on the costs and revenue of both surgical procedures, a multiple logistic regression analysis was performed. Variables supposed to affect costs and profit entering multiple logistic regression were: sex (male vs. female), laterality (left vs. right), surgical technique (LTA vs. RPA), resection type (partial vs. total), tumor size (≤ 40 mm vs. > 40 mm), morbidity (yes vs. no), BMI (≤ 25 vs. > 25 kg/m2), hormonal activity (yes vs. no), prior abdominal surgery (yes vs. no), CCI (≤ 2 vs. > 2) and hospital stay (≤ 5 vs. > 5 days). Graphpad gives P values with three decimal places. P values < 0.05 were considered significant.
Results
Study flow chart
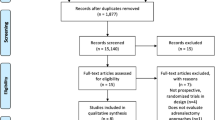
We identified a total of 174 patients who had undergone surgical treatment for a benign adrenal tumor between 2019 and 2022 in our center. 36 of these patients did open surgery and were therefore excluded from further analyses. Of the 138 remaining patients, 9 had to be withdrawn from the study due to lack of documented information on the endpoints. 7 patients were excluded as they did not complete the required 30 days of follow-up. A total of 122 patients (71 after LTA and 51 after RPA) were included in the final analysis. The flow chart summarizing patient selection is included in Fig. 1.

Study flowchart. LTA lateral transperitoneal adrenalectomy, RPA retroperitoneoscopic adrenalectomy
Patient matching
122 patients were entered into our matching algorithm to form two comparable cohorts. Based on the covariates age, sex, BMI and CCI, our matching was able to produce two homogenous cohorts with 43 patients in each (Fig. 1). All of the following data are based on these two patient cohorts.
Patient characteristics, intra- and postoperative outcome variables
After matching for age, sex, BMI and CCI there were no significant differences between the group in terms of histology, tumor laterality and rates of conversion to open surgery (Table 1). However, RPA patients tended to have more severe pre-existing disease than LTA patients (higher ASA score). These differences were not statistically significant (P = 0.353 and P = 0.555, respectively).
The analysis of the intra- and postoperative course (Table 1) showed that both cohorts (LTA vs. RPA) were comparable with regard to these variables (P > 0.05), excepted for the average duration of the procedure (67 min for LTA vs. 37 min for RPA P < 0.0001) and hospital stay (6.1 vs. 4.9 days, P = 0.040). An evaluation of postoperative mortality between the groups revealed no significant differences. However, there was a significant difference in overall morbidity (27.9% for RPA vs. 53.5%, for LTA, P = 0.016) in line with the published literature [40].
Revenue calculation
Also slightly higher in the LTA group, the mean revenues were comparable in both cohorts (P = 0.487). The mean revenue for LTA patients was US$7244.61 ± 472.58, whereas the RPA group presented a mean revenue of US$7204.42 ± 436.40.
Cost calculation
The analysis in terms of total hospital treatment costs (mean ± SD; median (IQR) values, respectively) showed that the LTA procedure [US$6617.75 ± 2198.78; US$5512 (4915–9007)] was significantly more expensive than the RPA technique [US$5789.99 ± 1615.92; US$5006 (4409–7535)] (P = 0.043).
Leading cost centers were similar for both procedures. With a decreasing share of the total costs, there are: (1) nursing normal ward (15.78% of the total costs vs. 14.38% for RPA and LTA), (2) infrastructure normal ward (12.60% vs. 12.32%), (3) medical needs operating theater (7.77% vs. 10.84%), (4) physicians operating theater (7.07% vs. 7.38%). Table 2 compares the leading cost centers for both procedures. This analysis showed significant differences for the following cost centers (mean value in US$): (1) medical needs operating room (US$828.6 vs. 589.8 for LTA and RPA, P = 0.013), (2) infrastructure operating room (US$257.0 vs. 208.2, P = 0.025). The comparative analysis of the leading cost centers indicated that the leading share of costs is spent on medical services (22.15% vs. 22.15% for RPA and LTA), followed by infrastructure costs (20.45% vs. 20.51%), nursing services (18.87% vs. 17.61%), medical-technical services (10.95% vs. 10.29%) and medical needs (8.00% vs. 10.86%). The costs of the leading providers represented 89.53% vs. 90.04% of the total costs for the RPA and LTA procedure, respectively.
Profit calculation
The median profit (IQR) for the LTA procedure was US$789.50 (− 509 to 1618) and US$1296 (359 to 2426) for the RPA procedure. This difference was statistically significant (P = 0.027).
Factors influencing the cost of treatment and the profit of both surgical procedures
The relationship between clinical variables (age, gender, complication, etc.) and the risk of costs > US$7500 was investigated with univariable and multivariable logistic regression. The choice of this cut-off was based on the results of the revenue analysis related to the two LTA and RPA techniques in our series. The value of US$7500 represents the cost limit at which the cost of treatment exceeds income and thus leads to a negative profit. Results are summarized in Table 3. Surgical approach (LTA vs. RPA), the existence of morbidity, patients comorbidity (CCI) and hospital stay were significant risk factors associated with costs > US$7500 in the univariate analysis. Only morbidity and hospital stay were shown to be significant independent risk factors in the multivariable analysis (P < 0.0001 and P = 0.0436 respectively).
Factors influencing the profit of both surgical procedures
Similar to the cost analysis, an analysis of the influencing factors for financial loss was carried out by means of uni- and multivariable logistic regression (Table 4). The existence of morbidity, patients comorbidity (CCI) and hospital stay were significant risk factors associated with financial loss in the univariate analysis. Only morbidity and hospital stay were shown to be significant independent risk factors in the multivariable analysis (P < 0.0001 and P = 0.021, respectively).
Discussion
Analyzing our matched cohorts of patients with various adrenal pathologies, RPA conferred superior costs/profit profile compared to LTA. This superiority of RPA may be associated with a lower risk of perioperative complications, a reduced use of postoperative drugs and reduced hospital stay.
Several studies have examined the economic costs associated with adrenal surgery. For example, surgical treatment of Conn syndrome results in a saving of $31,132 for the healthcare system over the lifetime of the patient when compared to conservative medical treatment [41, 42]. Moreover, laparoscopic surgery significantly reduces hospital costs further (17.9% reduction in total hospital costs) when compared to the costs resulting from open surgery [43]. While the laparoscopic technique is associated with an 18.1% increase in intraoperative costs this is offset by the postoperative costs which are 63.4% lower [44]. The use of surgeons with extensive experience in adrenal surgery results in an additional reduction in overall costs [45,46,47].
Much less is known about the economic impact of RTA versus LTA surgery, with the published data to date being sparse and often seemingly contradictory [48, 49]. Moreover, many studies have limited their analysis to direct surgical costs and have exclusively focussed on data from the US health care system [50]. In fact, there are no data directly comparing costs, revenues and possible profit associated with these two surgical approaches. Given the significant differences between the costs, funding and reimbursement in the US healthcare system versus European healthcare models, it is difficult to extrapolate and draw firm conclusions from the existing data.
Therefore, we sought to perform a comprehensive cost–benefit analysis directly comparing LTA and RTA in patients who underwent adrenalectomy using a matched-case study design.
Both cohorts (n = 43) were similar in terms of demographic and clinical parameters. Although the revenue for LTA tended to be slightly higher (US$7244 vs. v US$7204) than for the RPA, this difference was not statistically significant (P = 0.487). This total revenue difference between LTA and RPA can be explained by the supplements and deductions specific to gDRG system. It should be noted that baseline revenue calculation was based on the German DRG system, which makes no difference between RPA and LTA in terms of the type of procedure, both procedures being coded as minimally invasive adrenalectomy.
In terms of overall costs, LTA is more expensive than RPA (US$6618 vs. US$5790 and US$5512 vs. US$5006 for mean and median values respectively). This difference is statistically significant (P = 0.043). The costs were generated by the same factors in both procedures, namely (in order of decreasing share) (1) the nursing costs on a general surgical ward, (2) the ward infrastructure, (3) medical expenses in the operating room and (4) physician-associated cost. The detailed analysis of cost centers revealed that the general surgical ward was responsible for most of the costs, followed by the operating room and the anesthestics (induction and recovery rooms). These are similar in any surgical department and were consistent between both groups (RPA vs. LTA). Medical needs in the OR and OR infrastructure differed significantly in both groups. The cost center “infrastructure operating room” consists in part of the costs associated with the use of the operating room and the instruments available on that facilites. As the operating time is statistically longer in LTA than in the RPA group, this explains why the cost center “infrastructure operating room” is higher in the LTA than in the RPA group. The leading cost bearers (with decreasing total share) were (1) physicians, (2) infrastructure, (3) nursing. Previous studies have shown that personnel costs, in the context of surgical treatments, account for the majority of the expenditure [51, 52]. This remains the case for minimally invasive adrenal procedure. We hypothesize that the benefits of RPA over LTA in terms of duration of surgery, postoperative morbidity, and reduced postoperative drug use (benefits found both in our series and in the international literature) account for the cost difference between the two techniques.
However, our analysis revealed that both techniques differed significantly in terms of profit. The median profit and the mean profit were statistically significantly different between both cohorts (P = 0.027). RPA led to a significantly higher profit than LTA (US$1235 vs. US$653 and US$1296 vs. US$789 respectively for mean and median profit). This finding is new and contradicts current studies [48,49,50], which in most cases failed to show any difference between these procedures. It should be noted here that most of the studies were purely cost-related, and predominantly restricted their analyses to operational costs. A full economic costing, taking into all of the key stakeholders and factors into account has been lacking.
The multivariate logistic regression analysis showed that the factors influencing treatment costs and profit (Tables 3, 4; Fig. 2) were the duration of hospitalization (P = 0.0436 and P = 0.021 respectively) and postoperative morbidity (P < 0.0001). No other significant factors were identified in this analysis. This result is consistent with the published literature [53,54,55]. Although surgical technique was not identified as significant factor in the multivariate analysis, it should be kept in mind that RPA was associated with significantly less overall morbidity and a shorter period of hospitalization. Thus, it is at least conceivable that the procedure itself may significantly impact upon costs and profit in larger randomized cohorts.

Multidimensional cost-analysis (US$) according to hospital stay, comorbidity and procedure. Length of hospital stay is represented in (x) coordinate (abscissa), costs are represented in (y) coordinate (ordinate). Each bubble corresponds to a patient and the size of the bubble is directly proportional to the CCI value of that patient (comorbidity). Yellow bubble: RPA retroperitoneoscopic adrenalectomy; violet bubble: LTA lateral transperitoneal adrenalectomy (Color figure online)
The large number of postoperative complications registered in our series is due to the method of accounting for morbidity. Any deviation from the optimal postoperative trajectory was coded as morbidity. Thus, a simple anomaly in the biological results was interpreted as such. In addition, we considered all events, as one patient may have several postoperative complications. This explains why the total number is large compared to other series dealing with minimally invasive surgery of the adrenal gland.
In our series, the calculation of revenue and profit is based on the gDRG system. In 2011, German hospital financing was changed to the gDRG, which is based on the US-DRG system. There, Robert B. Fetter of Yale University had already proposed in 1967 that the financing of hospital costs should be based on prospectively determined and disease-specific case financing. In the USA, this system was used since the early 1980s. Subsequently, it was implemented in Australia. The diagnosis-related group systems in Europe (EuroDRG project) brings together 12 countries: Austria, England, Estonia, Finland, France, Germany, Ireland, the Netherlands, Poland, Portugal, Spain and Sweden.
This study has a number of limitations. Our investigation may be subject to inherent biases based on its pair-matching and monocentric nature. Selection bias may have resulted in patients with more complex comorbidities being over- or underrepresented in one particular group. Another limitation of the study is that our database does not offer data on the expertise of individual surgeons for both techniques.
In conclusion, RPA conferred superior cost/profit profile associated with a lower risk of perioperative complications and hospital stay compared to LTA in a matched cohort of patients with various adrenal pathologies.
Data availability
Data are available on request.
References
Bradley EH, Sipsma H, Taylor LA (2017) American health care paradox-high spending on health care and poor health. QJM 110:61–65
Bundesamt S (2022) D-statis. Gesundheitsausgaben
Energie BfrWu (2021) Gesundheitswirtschaft Fakten & Zahlen 2020. Ergebnisse der Gesundheitswirtschaftlichen Gesamtrechnung, Zentraler Bestellservice für Publikationen der Bundesregierung
Macario A (2010) What does one minute of operating room time cost? J Clin Anesth 22:233–236
Munoz E, Munoz W 3rd, Wise L (2010) National and surgical health care expenditures, 2005–2025. Ann Surg 251:195–200
Lozano R, Naghavi M, Foreman K, Lim S, Shibuya K, Aboyans V, Abraham J, Adair T, Aggarwal R, Ahn SY, Alvarado M, Anderson HR, Anderson LM, Andrews KG, Atkinson C, Baddour LM, Barker-Collo S, Bartels DH, Bell ML, Benjamin EJ, Bennett D, Bhalla K, Bikbov B, Bin Abdulhak A, Birbeck G, Blyth F, Bolliger I, Boufous S, Bucello C, Burch M, Burney P, Carapetis J, Chen H, Chou D, Chugh SS, Coffeng LE, Colan SD, Colquhoun S, Colson KE, Condon J, Connor MD, Cooper LT, Corriere M, Cortinovis M, de Vaccaro KC, Couser W, Cowie BC, Criqui MH, Cross M, Dabhadkar KC, Dahodwala N, De Leo D, Degenhardt L, Delossantos A, Denenberg J, Des Jarlais DC, Dharmaratne SD, Dorsey ER, Driscoll T, Duber H, Ebel B, Erwin PJ, Espindola P, Ezzati M, Feigin V, Flaxman AD, Forouzanfar MH, Fowkes FG, Franklin R, Fransen M, Freeman MK, Gabriel SE, Gakidou E, Gaspari F, Gillum RF, Gonzalez-Medina D, Halasa YA, Haring D, Harrison JE, Havmoeller R, Hay RJ, Hoen B, Hotez PJ, Hoy D, Jacobsen KH, James SL, Jasrasaria R, Jayaraman S, Johns N, Karthikeyan G, Kassebaum N, Keren A, Khoo JP, Knowlton LM, Kobusingye O, Koranteng A, Krishnamurthi R, Lipnick M, Lipshultz SE, Ohno SL, Mabweijano J, MacIntyre MF, Mallinger L, March L, Marks GB, Marks R, Matsumori A, Matzopoulos R, Mayosi BM, McAnulty JH, McDermott MM, McGrath J, Mensah GA, Merriman TR, Michaud C, Miller M, Miller TR, Mock C, Mocumbi AO, Mokdad AA, Moran A, Mulholland K, Nair MN, Naldi L, Narayan KM, Nasseri K, Norman P, O’Donnell M, Omer SB, Ortblad K, Osborne R, Ozgediz D, Pahari B, Pandian JD, Rivero AP, Padilla RP, Perez-Ruiz F, Perico N, Phillips D, Pierce K, Pope CA 3rd, Porrini E, Pourmalek F, Raju M, Ranganathan D, Rehm JT, Rein DB, Remuzzi G, Rivara FP, Roberts T, De Leon FR, Rosenfeld LC, Rushton L, Sacco RL, Salomon JA, Sampson U, Sanman E, Schwebel DC, Segui-Gomez M, Shepard DS, Singh D, Singleton J, Sliwa K, Smith E, Steer A, Taylor JA, Thomas B, Tleyjeh IM, Towbin JA, Truelsen T, Undurraga EA, Venketasubramanian N, Vijayakumar L, Vos T, Wagner GR, Wang M, Wang W, Watt K, Weinstock MA, Weintraub R, Wilkinson JD, Woolf AD, Wulf S, Yeh PH, Yip P, Zabetian A, Zheng ZJ, Lopez AD, Murray CJ, AlMazroa MA, Memish ZA (2012) Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 380:2095–2128
Childers CP, Maggard-Gibbons M (2018) Understanding costs of care in the operating room. JAMA Surg 153:e176233
Abbott T, White SM, Pandit JJ (2011) Factors affecting the profitability of surgical procedures under ‘Payment by Results.’ Anaesthesia 66:283–292
Brown JK, Campbell BT, Drongowski RA, Alderman AK, Geiger JD, Teitelbaum DH, Quinn J, Coran AG, Hirschl RB (2009) A prospective, randomized comparison of skin adhesive and subcuticular suture for closure of pediatric hernia incisions: cost and cosmetic considerations. J Pediatr Surg 44:1418–1422
Cross KJ, Teo EH, Wong SL, Lambe JS, Rohde CH, Grant RT, Ascherman JA (2009) The absorbable dermal staple device: a faster, more cost-effective method for incisional closure. Plast Reconstr Surg 124:156–162
Potter BJ, Ann Thompson C (2019) Cost of operating room time for endovascular transcatheter aortic valve replacement. J Med Econ 22:1022–1024
Raft J, Millet F, Meistelman C (2015) Example of cost calculations for an operating room and a post-anaesthesia care unit. Anaesth Crit Care Pain Med 34:211–215
Siddharth V, Kumar S, Vij A, Gupta SK (2015) Cost analysis of operation theatre services at an apex tertiary care trauma centre of India. Indian J Surg 77:530–535
Ting NT, Moric MM, Della Valle CJ, Levine BR (2012) Use of knotless suture for closure of total hip and knee arthroplasties: a prospective, randomized clinical trial. J Arthroplasty 27:1783–1788
Volpin A, Khan O, Haddad FS (2016) Theater cost is pound16/minute so what are you doing just standing there? J Arthroplasty 31:22–26
Constantinides VA, Christakis I, Touska P, Palazzo FF (2012) Systematic review and meta-analysis of retroperitoneoscopic versus laparoscopic adrenalectomy. Br J Surg 99:1639–1648
Nigri G, Rosman AS, Petrucciani N, Fancellu A, Pisano M, Zorcolo L, Ramacciato G, Melis M (2013) Meta-analysis of trials comparing laparoscopic transperitoneal and retroperitoneal adrenalectomy. Surgery 153:111–119
Heger P, Probst P, Huttner FJ, Goossen K, Proctor T, Muller-Stich BP, Strobel O, Buchler MW, Diener MK (2017) Evaluation of open and minimally invasive adrenalectomy: a systematic review and network meta-analysis. World J Surg 41:2746–2757
Arezzo A, Bullano A, Cochetti G, Cirocchi R, Randolph J, Mearini E, Evangelista A, Ciccone G, Bonjer HJ, Morino M (2018) Transperitoneal versus retroperitoneal laparoscopic adrenalectomy for adrenal tumours in adults. Cochrane Database Syst Rev 12:CD011668
Jiang YL, Qian LJ, Li Z, Wang KE, Zhou XL, Zhou J, Ye CH (2020) Comparison of the retroperitoneal versus transperitoneal laparoscopic adrenalectomy perioperative outcomes and safety for pheochromocytoma: a meta-analysis. BMC Surg 20:12
Gavriilidis P, Camenzuli C, Paspala A, Di Marco AN, Palazzo FF (2021) Posterior retroperitoneoscopic versus laparoscopic transperitoneal adrenalectomy: a systematic review by an updated meta-analysis. World J Surg 45:168–179
Meng C, Du C, Peng L, Li J, Li J, Li Y, Wu J (2021) Comparison of posterior retroperitoneoscopic adrenalectomy versus lateral transperitoneal laparoscopic adrenalectomy for adrenal tumors: a systematic review and meta-analysis. Front Oncol 11:667985
Mathew G, Agha R, Albrecht J, Goel P, Mukherjee I, Pai P, D’Cruz AK, Nixon IJ, Roberto K, Enam SA, Basu S, Muensterer OJ, Giordano S, Pagano D, Machado-Aranda D, Bradley PJ, Bashashati M, Thoma A, Afifi RY, Johnston M, Challacombe B, Ngu JC, Chalkoo M, Raveendran K, Hoffman JR, Kirshtein B, Lau WY, Thorat MA, Miguel D, Beamish AJ, Roy G, Healy D, Ather HM, Raja SG, Mei Z, Manning TG, Kasivisvanathan V, Rivas JG, Coppola R, Ekser B, Karanth VL, Kadioglu H, Valmasoni M, Noureldin A, Group S (2021) STROCSS 2021: strengthening the reporting of cohort, cross-sectional and case-control studies in surgery. Int J Surg 96:106165
Husereau D, Drummond M, Augustovski F, de Bekker-Grob E, Briggs AH, Carswell C, Caulley L, Chaiyakunapruk N, Greenberg D, Loder E, Mauskopf J, Mullins CD, Petrou S, Pwu RF, Staniszewska S, Force CIGRPT (2022) Consolidated Health Economic Evaluation Reporting Standards 2022 (CHEERS 2022) statement: updated reporting guidance for health economic evaluations. Value Health 25:3–9
DGAV DGAV Referenzzentren Endokrine Chirurgie
Yip L, Duh QY, Wachtel H, Jimenez C, Sturgeon C, Lee C, Velazquez-Fernandez D, Berber E, Hammer GD, Bancos I, Lee JA, Marko J, Morris-Wiseman LF, Hughes MS, Livhits MJ, Han MA, Smith PW, Wilhelm S, Asa SL, Fahey TJ 3rd, McKenzie TJ, Strong VE, Perrier ND (2022) American association of endocrine surgeons guidelines for adrenalectomy: executive summary. JAMA Surg 157:870–877
Lorenz K, Langer P, Niederle B, Alesina P, Holzer K, Nies C, Musholt T, Goretzki PE, Rayes N, Quinkler M, Waldmann J, Simon D, Trupka A, Ladurner R, Hallfeldt K, Zielke A, Saeger D, Poppel T, Kukuk G, Hotker A, Schabram P, Schopf S, Dotzenrath C, Riss P, Steinmuller T, Kopp I, Vorlander C, Walz MK, Bartsch DK (2019) Surgical therapy of adrenal tumors: guidelines from the German Association of Endocrine Surgeons (CAEK). Langenbecks Arch Surg 404:385–401
Stefanidis D, Goldfarb M, Kercher KW, Hope WW, Richardson W, Fanelli RD (2013) SAGES guidelines for minimally invasive treatment of adrenal pathology. Surg Endosc 27:3960–3980
Billmann F (2017) Retroperitoneoskopische Adrenalektomie. In: Keck T, Germer C (eds) Minimalinvasive Viszeralchirurgie. Springer, Berlin, pp 173–186
Walz MK, Alesina PF, Wenger FA, Deligiannis A, Szuczik E, Petersenn S, Ommer A, Groeben H, Peitgen K, Janssen OE, Philipp T, Neumann HP, Schmid KW, Mann K (2006) Posterior retroperitoneoscopic adrenalectomy—results of 560 procedures in 520 patients. Surgery 140:943–948 (discussion 948–950)
Walz MK (2012) Minimally invasive adrenal gland surgery. Transperitoneal or retroperitoneal approach? Chirurg 83:536–545
Dindo D, Demartines N, Clavien PA (2004) Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg 240:205–213
InEK (2016) Kalkulation von Behandlungskosten. Handbuch zur Anwendung in Krankenhäusern, 4.0 edn. Deutsche Krankenhaus Verlagsgesellschaft, Düsseldorf
Cokins G, Căpuşneanu S (2010) Cost drivers. Evolution and benefits. Theor Appl Econ 17:7–16
Erlangen-Nürnberg F (2020) LS Gesundheitsmanagement, Klinikum Nürnberg, Text 52, Krankenhausmanagement und Prozesskostenrechnung. MHBA, pp 52/13–52/27
Charlson ME, Pompei P, Ales KL, MacKenzie CR (1987) A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis 40:373–383
Bittner JG, Gershuni VM, Matthews BD, Moley JF, Brunt LM (2013) Risk factors affecting operative approach, conversion, and morbidity for adrenalectomy: a single-institution series of 402 patients. Surg Endosc 27:2342–2350
Lan BY, Taskin HE, Aksoy E, Birsen O, Dural C, Mitchell J, Siperstein A, Berber E (2015) Factors affecting the surgical approach and timing of bilateral adrenalectomy. Surg Endosc 29:1741–1745
Giron F, Rey Chaves CE, Rodriguez L, Rueda-Esteban RJ, Nunez-Rocha RE, Toledo S, Conde D, Hernandez JD, Vanegas M, Nassar R (2022) Postoperative outcomes of minimally invasive adrenalectomy: do body mass index and tumor size matter? A single-center experience. BMC Surg 22:280
Billmann F, Billeter A, Thomusch O, Keck T, El Shishtawi S, Langan EA, Strobel O, Muller-Stich BP (2021) Minimally invasive partial versus total adrenalectomy for unilateral primary hyperaldosteronism—a retrospective, multicenter matched-pair analysis using the new international consensus on outcome measures. Surgery 169:1361–1370
Reimel B, Zanocco K, Russo MJ, Zarnegar R, Clark OH, Allendorf JD, Chabot JA, Duh QY, Lee JA, Sturgeon C (2010) The management of aldosterone-producing adrenal adenomas—does adrenalectomy increase costs? Surgery 148:1178–1185 (discussion 1185)
Sywak M, Pasieka JL (2002) Long-term follow-up and cost benefit of adrenalectomy in patients with primary hyperaldosteronism. Br J Surg 89:1587–1593
Schell SR, Talamini MA, Udelsman R (1999) Laparoscopic adrenalectomy for nonmalignant disease: improved safety, morbidity, and cost-effectiveness. Surg Endosc 13:30–34
Hobart MG, Gill IS, Schweizer D, Bravo EL (1999) Financial analysis of needlescopic versus open adrenalectomy. J Urol 162:1264–1267
Anderson KL Jr, Thomas SM, Adam MA, Pontius LN, Stang MT, Scheri RP, Roman SA, Sosa JA (2018) Each procedure matters: threshold for surgeon volume to minimize complications and decrease cost associated with adrenalectomy. Surgery 163:157–164
Palazzo F, Dickinson A, Phillips B, Sahdev A, Bliss R, Rasheed A, Krukowski Z, Newell-Price J (2016) Adrenal surgery in England: better outcomes in high-volume practices. Clin Endocrinol (Oxford) 85:17–20
Park HS, Roman SA, Sosa JA (2009) Outcomes from 3144 adrenalectomies in the United States: which matters more, surgeon volume or specialty? Arch Surg 144:1060–1067
Barczynski M, Konturek A, Nowak W (2014) Randomized clinical trial of posterior retroperitoneoscopic adrenalectomy versus lateral transperitoneal laparoscopic adrenalectomy with a 5-year follow-up. Ann Surg 260:740–747 (discussion 747–748)
Kiriakopoulos A, Economopoulos KP, Poulios E, Linos D (2011) Impact of posterior retroperitoneoscopic adrenalectomy in a tertiary care center: a paradigm shift. Surg Endosc 25:3584–3589
Farres H, Felsher J, Brodsky J, Siperstein A, Gill I, Brody F (2004) Laparoscopic adrenalectomy: a cost analysis of three approaches. J Laparoendosc Adv Surg Tech A 14:23–26
Wu SY, Terrell J, Park A, Perrier N (2020) Understanding thyroidectomy cost variations among national cancer institute-designated cancer centers. World J Surg 44:385–392
Rajan SS, Akeroyd JM, Ahmed ST, Ramsey DJ, Ballantyne CM, Petersen LA, Virani SS (2021) Health care costs associated with primary care physicians versus nurse practitioners and physician assistants. J Am Assoc Nurse Pract 33:967–974
Al-Thani H, Al-Thani N, Al-Sulaiti M, Tabeb A, Asim M, El-Menyar A (2022) A descriptive comparative analysis of the surgical management of adrenal tumors: the open, robotic, and laparoscopic approaches. Front Surg 9:848565
Samreen S, Fluck M, Hunsinger M, Wild J, Shabahang M, Blansfield JA (2019) Laparoscopic versus robotic adrenalectomy: a review of the national inpatient sample. J Robot Surg 13:69–75
Al-Qurayshi Z, Robins R, Buell J, Kandil E (2016) Surgeon volume impact on outcomes and cost of adrenal surgeries. Eur J Surg Oncol 42:1483–1490
Acknowledgements
We thank Mr. Bönsert for making available the economic data of the patients included in this series.
Funding
Open Access funding enabled and organized by Projekt DEAL. No funding.
Author information
Authors and Affiliations
Contributions
AF: Formal analysis, investigation, methodology, writing-original draft, writing-review and editing. OS: Formal analysis, investigation, methodology, writing-original draft. AH: Methodology, project administration, writing-original draft. EAL: Methodology, writing-original draft, writing-review and editing. AN: Methodology, writing-original draft, writing-review and editing. MWB: Conceptualization, formal analysis, validation, writing-original draft. FB: Conceptualization, formal analysis, investigation, methodology, project administration, resources, supervision, validation, visualization, writing-original draft, writing-review and editing.
Corresponding author
Ethics declarations
Disclosures
A. Fischer, O Schöffski, A. Nießen, M.W. Büchler, E. A. Langan and F. Billmann have no conflicts of interest or financial ties to disclose.
Ethical approval
This research was approved by the local ethical committee (Ethikkommission der medizinischen Fakultät Heidelberg, S-656/2022) related to the surgical department of the university Hospital Heidelberg and was registered in the German Clinical Trials Register (DRKS00030186; available at: https://drks.de/search/de/trial/DRKS00030186) and the International Clinical Trials Registry Platform (available at: https://trialsearch.who.int).
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This study will be presented to the 31st International EAES Congress, 20–23 June 2023 in Roma, Italy.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Fischer, A., Schöffski, O., Nießen, A. et al. Retroperitoneoscopic adrenalectomy may be superior to laparoscopic transperitoneal adrenalectomy in terms of costs and profit: a retrospective pair-matched cohort analysis. Surg Endosc 37, 8104–8115 (2023). https://doi.org/10.1007/s00464-023-10395-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-023-10395-1