
Abstract
Background
Inguinal hernia has a lifetime incidence of 27% in men and 3% in women. Surgery is the recommended treatment, but there is no consensus on the best method. Open repair is most popular, but there are concerns about the risk of chronic groin pain. Laparoscopic repair is increasingly accepted due to the lower risk of chronic pain, although its recurrence rate is still unclear. The aim of this overview is to compare the risk of recurrence and chronic groin pain in laparoscopic versus open repair for inguinal hernia.
Methods
We searched Ovid MEDLINE, EMBASE and the Cochrane Database of Systematic Reviews for systematic reviews and meta-analyses. Only reviews of randomised controlled trials (RCTs) in adults published in English were included. Conference proceedings and editorials were excluded. The quality of the systematic reviews was assessed using the AMSTAR 2 checklist. Two outcomes were considered: hernia recurrence and chronic pain.
Results
Twenty-one systematic reviews and meta-analyses were included. Laparoscopic repair was associated with a lower risk of chronic groin pain compared with open repair. In the four systematic reviews assessing any laparoscopic versus any open repairs, laparoscopic repair was associated with a statistically significant (range: 26–46%) reduction in the odds or risk of chronic pain. Most reviews showed no difference in recurrence rates between laparoscopic and open repairs, regardless of the types of repair considered or the types of hernia that were studied, but most reviews had wide confidence intervals and we cannot rule out clinically important effects favouring either type of repair.
Conclusion
Meta-analyses suggest that laparoscopic repairs have a lower incidence of chronic groin pain than open repair, but there is no evidence of differences in recurrence rates between laparoscopic and open repairs.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Inguinal hernia accounts for 75% of all abdominal wall hernias and has a lifetime incidence of 27% in males and 3% in women [1]. Several types of inguinal hernia have been identified and surgery to repair them, which began around the sixteenth century following the establishment of modern anatomy, has since evolved with a number of techniques currently available [2]. There has been ongoing debate about which form of repair offers the best patient outcomes and there is yet to be a unanimously agreed superior approach to the management of inguinal hernias.
Open inguinal hernia repair has long been the method of choice for most surgeons and is often recommended in contemporary literature as the optimal approach for primary unilateral inguinal hernia, which is a hernia occurring for the first time on one side of the groin, without any prior repair [3, 4]. Open repairs have mainly been classified as open mesh (e.g. Lichtenstein) or open non-mesh (e.g. Shouldice) repairs based on whether a synthetic material has been used to re-enforce the repaired posterior wall [5]. Tension-free mesh repair (Lichtenstein technique) is usually considered the repair method of choice among open repairs due to its easy reproducibility by non-specialist surgeons. However, there are concerns about the risk of chronic groin pain, although recurrence rates have been noticeably very low [6].
Trans-abdominal pre-peritoneal repair (TAPP) and the totally extra-peritoneal repair (TEP) are two of the main laparoscopic (keyhole) techniques used. Laparoscopic approaches have grown in popularity recently with some surgeons appreciative of its significantly lower incidence of long-term post-operatively pain, but there have been some concerns regarding a possible increased risk of recurrence after TEP repair [7]. This has been reported more frequently in primary, unilateral inguinal hernia compared with recurrent hernia. Despite this concern, TEP has nonetheless been adopted as the procedure of choice because of a lower risk of intra-abdominal injuries compared to TAPP repair as well as the comparably good outcomes especially when it is done by skilled surgeons [3, 4, 7,8,9,10].
Several systematic reviews and meta-analyses have compared laparoscopic and open repair techniques but there has not been any consensus on which technique offers better outcomes overall. This study aims to conduct an overview of existing systematic reviews, which is a relatively new methodology for summarising evidence. Compared with conducting a new systematic review, an overview takes considerably less time and resources and can help researchers synthesise evidence across interventions, especially where conflicting evidence has been reported from existing systematic reviews, with the aim of establishing a comprehensive overview on the current best evidence [11].
This overview of reviews aims at informing clinical practice by identifying, analysing and synthesising the numerous published systematic reviews assessing the comparative efficacy of open and laparoscopic repairs for inguinal hernia.
Materials and methods
Study design and protocol
An overview of systematic reviews was conducted according to the recommendations of the Cochrane Handbook of Systematic Reviews of Interventions to gain understanding of the currently available evidence for the efficacy of inguinal hernia repairs from existing systematic reviews in the literature [11]. The method of the overview was pre-specified in a research protocol based on the PRISMA reporting guidelines [12].
Types of reviews
This overview included systematic reviews (including meta-analyses and network meta-analyses (NMA)) of randomised controlled trials (RCTs) published in English. Systematic reviews that included a mixture of randomised and non-randomised evidence were included if they reported RCT data separately. Conference proceedings, protocols and editorials were excluded.
Types of participants
Males and females aged 16 years or above.
Types of interventions
Laparoscopic surgery was compared with open surgery for the repair of inguinal hernias. When possible, we also included studies assessing TAPP and/or TEP repairs separately. Similarly, we included studies assessing all open repairs as well as open mesh and non-mesh repairs separately.
Outcomes
Hernia recurrence and incidence of chronic groin pain.
Literature search
We searched Ovid MEDLINE, EMBASE and CDSR (Cochrane Database of Systematic Reviews) to identify systematic reviews and meta-analyses published up to 8 May 2020. There were no restrictions on date or language of publication. An initial search strategy was generated for Ovid MEDLINE and adapted to other databases. The search focused on free-text and MeSH terms for ‘inguinal hernia surgery’, ‘open repair techniques’, ‘laparoscopic repair techniques’ and ‘systematic reviews and meta-analysis’. Additionally, we checked the reference lists of retrieved reviews for additional eligible reviews.
Screening and study selection
Two researchers (NH, AA) searched for and selected reviews based on criteria pre-specified in the research protocol. Initially, the researchers screened the titles and abstracts identified by the search strategy independently. Disagreements were resolved by discussion or arbitration by other authors. Selected studies were retrieved in full and assessed for inclusion by one author (NH).
Data collection
A data extraction form was developed and piloted to record relevant data from the identified systematic reviews. Recorded data included administrative data, bibliographic information, descriptive characteristics of reviews including inclusion/exclusion criteria, information on the type of hernia and definitions of the outcomes. Data on hernia recurrence and chronic pain were extracted by one researcher (NH) in the form of effect sizes and their 95% confidence intervals (or credible intervals for NMA).
Quality assessment of included reviews
The quality of included reviews was assessed using the AMSTAR 2 checklist, a 16-item tool that has been developed to appraise the methodological quality of overviews of systematic reviews [13]. AMSTAR 2 classifies overall confidence in the results of each review as ‘high’, ‘moderate’, ‘low’ or ‘critically low’ based on ratings for selected items identified as the critical domains. The items considered critical domains for the purpose of this overview included ‘duplicate study selection by review authors’ (item 5), ‘adequate description of included studies in the review’ (item 8), ‘use of appropriate method for meta-analysis’ (item 11) and either of ‘use of a satisfactory risk of bias (ROB) assessment for included studies in the review’ (item 9) or ‘assessment of the impact of ROB in interpretation of results’ (item 13).
Data synthesis
Quantitative outcome data were summarised in tables showing effect sizes and 95% confidence/credible intervals for hernia recurrence and chronic groin pain, bearing in mind that results of the reviews may include overlapping studies. Where no results from meta-analysis were available, the reported conclusions were included in the tables. A narrative synthesis was then carried out.
Results
Literature search
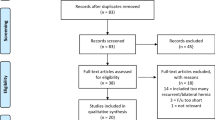
The initial search retrieved 175 systematic reviews with an additional four reviews identified from the reference lists of the included reviews. During abstract screening, sixty-two duplicate reviews were excluded, and a further 66 reviews failed to meet the pre-specified inclusion criteria. After full-text screening of the remaining 51 articles, 21 reviews met the inclusion criteria (Fig. 1).

PRISMA flow diagram
Study details
Details of the study characteristics are summarised in Table 1. The included reviews were published between 1999 and 2020. The most recent search date for an included review was February 2019. The number of RCTs per review varied from 4 to 58, while the number of participants ranged from 404 to 17,510. The age of the participants ranged from 16 to 100 years. All the reviews included participants of both genders. Five reviews [8, 21, 27, 29, 32] analysed only data on hernia recurrence and did not report chronic pain while the remaining 16 reviews [10, 14,15,16,17,18,19,20, 22,23,24,25,26, 28, 30, 31] reported data on both outcomes. Five reviews [15, 16, 19, 23, 25] compared outcomes in primary inguinal hernias only, and five reviews [20, 21, 24, 27, 28] examined recurrent inguinal hernias alone, while the remaining 11 reviews [8, 10, 14, 17, 18, 22, 26, 29,30,31,32] either considered both types of hernia or did not specify the type. One Cochrane review was identified which collected individual participant data (IPD) from the trialists which enabled reporting of separate subgroups for primary and recurrent hernias [10]. One NMA was also identified [15].
Methodological quality of included reviews
Two reviews [15, 16] were scored as high quality (both published in 2019) (Table 2). Nine studies were judged to be of moderate quality [10, 14, 17,18,19,20,21, 23, 28]. Among the six older studies (before 2010), only the Cochrane review [10] was found to be of moderate quality and there were three reviews [29, 31, 32] of critically low quality.
Hernia recurrence
Table 3 presents the results for hernia recurrence, first for laparoscopic versus open overall and then for specific combinations of repairs. Results for primary and recurrent hernias are provided in separate columns where available, although usually the first of these columns represents a mixture of primary and recurrent hernias or a situation where it was unclear which types were included. Overall, most reviews showed no evidence of differences in recurrence rates between laparoscopic and open repairs, regardless of the type of hernia studied. However, most of the reviews had wide confidence intervals (CIs), so we cannot rule out clinically important effects favouring either laparoscopic or open repair.
Six reviews [10, 15, 16, 19, 23, 25] presented data for primary inguinal hernias alone and most reported no statistically significant differences between laparoscopic and open repairs. One review [25] showed lower recurrence for the open group versus both laparoscopic [RR 2.06 (1.26, 3.37)] and TEP groups [RR 3.72 (1.66, 8.35)]. However, this review included fewer studies compared with earlier published reviews. Similarly, six reviews [10, 20, 21, 24, 27, 28] presented results specifically for recurrent hernias and none reported statistically significant differences between laparoscopic and open groups.
Seven reviews [8, 17, 26, 29,30,31,32] did not report the specific hernia types they considered and were assumed to have included both primary and recurrent hernias (Table 3). These reviews generally reported considerable uncertainty in the magnitude and direction of their effects. Two [17, 26] of these reviews reported findings in favour of open repair techniques and one [26] showed a doubling of the odds of recurrence after laparoscopic repair [OR 2.17 (1.58, 2.98)]. However, it considered only six studies, significantly fewer than those included in earlier published reviews.
When comparing specific types of laparoscopic repair, most reviews comparing TAPP with open repair showed no statistically significant results. One study which used individual participant data (IPD) [10] found a lower risk of recurrence for TAPP versus open non-mesh repair, but this finding was not replicated in a more recent review [18].
When comparing TEP versus open repair, results of the meta-analyses varied considerably and most had wide confidence intervals. Three reviews [17, 22, 25] found evidence of fewer recurrences for open repairs compared with TEP.
Chronic pain
Definitions of chronic pain varied and ranged from one month to one year after the procedure. Five reviews [15, 16, 19, 23, 25] reporting this outcome studied primary inguinal hernias alone and another five [20, 21, 24, 27, 28] looked at only recurrent inguinal hernias (Table 4).
Most reviews of primary (or mixed primary/recurrent) hernias consistently suggested laparoscopic repairs to have a lower risk of chronic groin pain compared to open repairs, regardless of whether TAPP/TEP or open mesh/non-mesh was used, and although effect sizes varied, many reviews showed odds ratios around 0.5, indicating a 50% reduction in the odds of having chronic pain for laparoscopic repair compared to open repair (Table 4). In particular, in the four systematic reviews assessing any laparoscopic versus any open repairs, laparoscopic repair was associated with a statistically significant (range: 26% to 46%) reduction in the odds or risk of chronic pain. When considering the reviews of recurrent hernias alone, most studies did not show statistically significant results, but results were based on small number of trials [10, 20, 24, 28].
Discussion
There was no clear evidence of a difference in recurrence rates between laparoscopic and open repairs for inguinal hernia in the systematic reviews and meta-analyses identified, although clinically important effects could not be ruled out due to the wide CIs reported. However, laparoscopic techniques were generally found to have less chronic groin pain compared to open repairs, regardless of the specific open or laparoscopic repair considered, or the hernia type (primary or recurrent hernia) that was studied. Overall, conclusions remained similar when examining either primary or recurrent inguinal hernias alone.
Reviews assessing recurrence rates showed heterogeneity in the magnitude and direction of effects. Most reviews which looked at primary hernias, recurrent hernias and both types of hernias together were rated high to moderate quality, suggesting high confidence in their findings. Other reviews which did not report the specific hernia types also had uncertain results with four reviews [8, 17, 26, 30] of moderate to low quality showing statistically significant results in favour of open repair techniques, but the generally low overall quality of these reviews remains a concern. These findings are similar to those published in a recent clinical guideline [33] in which experienced hernia surgeons and researchers across the world made recommendations based on comparable recurrence rates between laparoscopic and open repairs. The guideline emphasised that the recurrence rates remain comparable especially where the surgeries were conducted by highly skilled surgeons.
For chronic groin pain, we found that laparoscopic repairs were consistently associated with lower pain compared with open repairs regardless of the type of open or laparoscopic repair or the types of hernia studied. This is despite the noticeable difference in the definitions of chronic groin pain across the reviews we included. A recent review [18] reported both early and late chronic groin pain with distinct definitions, but the findings are similar and consistent with those of other reviews in this overview. Two reviews [20, 24] were also noted to have included exactly the same studies and participants in a number of comparisons of hernia types, although their findings are consistent with similar reviews.
In recurrent hernias, there are concerns about the risk of chronic pain, which is determined mainly by the chosen approach to repair. The HerniaSurge group guidelines [33] noted that repair of a recurrent hernia is always challenging compared with a primary hernia, and they emphasised that re-entry through a scar tissue increases risk of nerve and blood vessel entrapment/damage and potentially increases the risk of chronic groin pain and testicular atrophy. Therefore, the guideline recommends that if the prior repair is an open repair, then a laparoscopic approach is strongly favoured due to reduced risk of damage to structures.
The systematic reviews varied considerably in quality, included patients and outcome definitions. Attempts have been made to minimise the differences between reviews by categorising the review findings by hernia type and specific repair techniques to enable more meaningful interpretation of findings during the narrative synthesis. Because of the limitations of this narrative approach, a more robust synthesis, for example, a series of pairwise and network meta-analyses at different levels would be needed to provide comprehensive answers to research questions in this area including the type of mesh and the effect on different subgroups of patients.
This overview has a number of strengths including the pre-specification of methods in a protocol, which guided the conduct of the overview as recommended by the preferred reporting items for systematic reviews and meta-analysis (PRISMA) guidelines [12]. Study identification and selection were carried out by two researchers to enhance the integrity of the study selection process. Only systematic reviews and meta-analyses of RCTs were included in the overview to avoid the intrinsic bias of observational studies. Limitations of the overview include difficulty in retrieving some articles, exclusion of reviews published in languages other than English, restriction of outcome analysis to hernia recurrence and chronic groin pain, single data extraction and quality assessment and the exclusion of conference proceedings.
In conclusion, although the overview has found no clear evidence of differences in recurrence rates between laparoscopic and open repairs, laparoscopic techniques have generally been shown to have less postoperative long-term pain compared with open repairs.
References
Kingsnorth A, LeBlanc K (2003) Hernias: inguinal and incisional. Lancet 362: 1561–1571. https://www.ncbi.nlm.nih.gov/pubmed/14615114
Sachs M, Damm M, Encke A (1997) Historical evolution of inguinal hernia repair. World J Surg 21:218–223. https://doi.org/10.1007/s002689900220.pdf
Bloor K, Freemantle N, Khadjesari Z et al (2003) Impact of NICE guidance on laparoscopic surgery for inguinal hernias: analysis of interrupted time series. BMJ 326:578
de Lange DH, Kreeft M, van Ramshorst GH et al (2010) Inguinal hernia surgery in The Netherlands: are patients treated according to the guidelines? Hernia 14:143–148
Eklund AS, Montgomery AK, Rasmussen IC et al (2009) Low recurrence rate after laparoscopic (TEP) and open (Lichtenstein) inguinal hernia repair: a randomized, multicenter trial with 5-year follow-up. Ann Surg 249:33–38
EU Hernia Trialists Collaboration (2000) Laparoscopic compared with open methods of groin hernia repair: systematic review of randomised controlled trials. Br J Surg 37:860–867. https://www.ncbi.nlm.nih.gov/pubmed/10931019
Neumayer L et al (2004) Open versus laparoscopic mesh repair of inguinal hernia. N Engl J Med 350: 1819–1827. https://www.ncbi.nlm.nih.gov/pubmed/15107485
Memon MA, Cooper NJ, Memon B et al (2003) Meta-analysis of randomized clinical trials comparing open and laparoscopic inguinal hernia repair. Br J Surg 90:1479–1492
Bittner R, Sauerland S, Schmedt CG (2005) Comparison of endoscopic techniques vs Shouldice and other open nonmesh techniques for inguinal hernia repair: a meta-analysis of randomized controlled trials. Surg Endosc 19:605–615
McCormack K, Scohtt NW, Go PM et al (2003) Laparoscopic techniques versus open techniques for inguinal hernia repair. Cochrane Database Syst Rev 1:CD001785
Pollock M, Fernandes RM, Becker LA, Pieper D, Hartling L (2018) Chapter V: overviews of reviews. Draft version (8 October 2018) for inclusion. In: Higgins JPT, Thomas J, Chandler J, Cumpston MS, Li T, Page MJ, Welch V (eds) Cochrane handbook for systematic reviews of interventions. Cochrane, London
Larissa S (2015) Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: elaboration and explanation. BMJ 349:g7647. https://doi.org/10.1136/bmj.g7647[Accessed25May2019]
Shea BJ et al (2007) Development of AMSTAR: a measurement tool to assess the methodological quality of systematic reviews. BMC Med Res Methodol. https://doi.org/10.1186/1471-2288-7-10
Lyu Y, Cheng Y, Wang B, Du W, Xu Y (2020) Comparison of endoscopic surgery and Lichtenstein repair for treatment of inguinal hernias: a network meta-analysis. Medicine 99(6):e19134
Aiolfi A et al (2019) Primary inguinal hernia: systematic review and Bayesian network meta-analysis comparing open, laparoscopic transabdominal preperitoneal, totally extraperitoneal, and robotic preperitoneal repair. Hernia 23:473–484. https://doi.org/10.1007/s10029-019-01964-2
Bullen NL, Massey LH, Antoniou SA, Smart NJ, Fortelny RJ (2019) Open versus laparoscopic mesh repair of primary unilateral uncomplicated inguinal hernia: a systematic review with meta-analysis and trial sequential analysis. Hernia 23:461–472. https://doi.org/10.1007/s10029-019-01989-7
Gavriilidis P, Davies RJ, Wheeler J, de’Angelis N, Di Saverio S (2019) Total extraperitoneal endoscopic hernioplasty (TEP) versus Lichtenstein hernioplasty: a systematic review by updated traditional and cumulative meta-analysis of randomised-controlled trials. Hernia 23:1093–1103. https://doi.org/10.1007/s10029-019-02049-w
Patterson TJ, Beck J, Currie PJ, Spence RAJ, Spence G (2019) Meta-analysis of patient-reported outcomes after laparoscopic versus open inguinal hernia repair. Br J Surg BJS 106:824–836. https://doi.org/10.1002/bjs.11139
Scheuermann U, Niebisch S, Lyros O, Jansen-Winkeln B, Gockel I (2017) Transabdominal preperitoneal (TAPP) versus Lichtenstein operation for primary inguinal hernia repair—a systematic review and meta-analysis of randomized controlled trials. BMC Surg 17:55. https://doi.org/10.1186/s12893-017-0253-7
Pisanu A, Podda M, Saba A, Porceddu G, Uccheddu A (2015) Meta-analysis and review of prospective randomized trials comparing laparoscopic and Lichtenstein techniques in recurrent inguinal hernia repair. Hernia 19:355–366. https://doi.org/10.1007/s10029-014-1281-1
Li J, Ji Z, Li Y (2014) Comparison of laparoscopic versus open procedure in the treatment of recurrent inguinal hernia: a meta-analysis of the results. Am J Surg 207:602–612. https://doi.org/10.1016/j.amjsurg.2013.05.008
Zheng B, Wang N, Qiao Q, Wu T, Lu J, He X (2014) Meta-analysis of randomized controlled trials comparing Lichtenstein and totally extraperitoneal laparoscopic hernioplasty in treatment of inguinal hernias. J Surg Res 192:409–420. https://doi.org/10.1016/j.jss.2014.05.082
Koning GG, Wetterslev J, van Laarhoven CJHM, Keus F (2013) The totally extraperitoneal method versus Lichtenstein’s technique for inguinal hernia repair: a systematic review with meta-analyses and trial sequential analyses of randomized clinical trials. PLoS ONE 8(1):e52599. https://doi.org/10.1371/journal.pone.0052599
Yang J, Tong DN, Yao J, Chen W (2013) Laparoscopic or Lichtenstein repair for recurrent inguinal hernia: a meta-analysis of randomized controlled trials. ANZ J Surg. https://doi.org/10.1111/ans.12010
O’Reilly EA, Burke JP, O’Connell PR (2012) A meta-analysis of surgical morbidity and recurrence after laparoscopic and open repair of primary unilateral inguinal hernia. Ann Surg 255:846–853. https://doi.org/10.1097/SLA.0b013e31824e96cf
Aly O, Green A, Joy M, Wong CH, Al-Kandari A, Cheng S, Malik M (2011) Is laparoscopic inguinal hernia repair more effective than open repair? J College Phys Surg Pakistan 5:291–296
Dedemadi G, Sgourakis G, Radtke A, Dounavis A, Gockel I, Fouzas I et al (2010) Laparoscopic versus open mesh repair for recurrent inguinal hernia: a meta-analysis of outcomes. Am J Sur 200:2. https://doi.org/10.1016/j.amjsurg.2009.12.009
Karthikesalingam A, Markar A, Holt PJE, Praseedom RK (2010) Meta-analysis of randomized controlled trials comparing laparoscopic with open mesh repair of recurrent inguinal hernia. Br J Surg 97:4–11. https://doi.org/10.1002/bjs.6902
Kuhry E, van Veen RN, Langeveld HR, Steyerberg EW, Jeekel J, Bonjer HJ (2007) Open or endoscopic total extraperitoneal inguinal hernia repair? A systematic review. Surg Endosc 21:161–166. https://doi.org/10.1007/s00464-006-0167-4
Schmedt CG, Sauerland S, Bittner R (2005) Comparison of endoscopic procedures vs Lichtenstein and other open mesh techniques for inguinal hernia repair. Surg Endosc 19:188–199. https://doi.org/10.1007/s00464-004-9126-0
Schmedt CG, Leibl BJ, Bittner R (2002) Endoscopic inguinal hernia repair in comparison with shouldice and lichtenstein repair. Dig Surg 19:511–517. https://doi.org/10.1159/000067607
Chung RS, Rowland DY (1999) Meta-analyses of randomized controlled trials of laparoscopic vs conventional inguinal hernia repairs. Surg Endosc 13:689–694
HerniaSurge Group (2018) International guidelines for groin hernia management. Hernia 22(1):1–165. https://doi.org/10.1007/s10029-017-1668-x
Funding
No specific funding was received for this work.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
Nafi’u Haladu, Adegoke Alabi, Miriam Brazzelli, Mari Imamura, Irfan Ahmed and George Ramsay have no conflict of interest or other financial ties to disclose. Neil Scott is an author of one of the included systematic reviews [10] but has no other conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Haladu, N., Alabi, A., Brazzelli, M. et al. Open versus laparoscopic repair of inguinal hernia: an overview of systematic reviews of randomised controlled trials. Surg Endosc 36, 4685–4700 (2022). https://doi.org/10.1007/s00464-022-09161-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-022-09161-6