
Abstract
Background
Laparoscopic sigmoidectomy is the preferred approach in the elective surgical management of diverticulitis. However, it is unclear if the benefits of laparoscopy persist when operative times are prolonged. We aimed to investigate if the recovery benefits associated with laparoscopy are retained when operative times are long.
Methods
A retrospective review of a prospectively maintained database of patients who underwent elective laparoscopic sigmoidectomy from 2010–2015 at a single academic tertiary institution was performed. Operative times among laparoscopic completed cases were divided into quartiles, and patient outcomes were compared between the groups.
Results
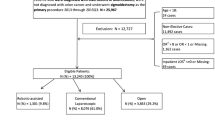
A total of 466 patients (median age: 58 ± 11.6 years, 58% females) underwent sigmoidectomy: 430 completed laparoscopically and 36 (7.7%) converted. Median operative time in laparoscopically completed cases was 188 min (IQR 154–230). There were no differences in morbidity (P = 0.52) or readmission rates (P = 0.22) among the quartiles. The 2nd and 4th operative time quartiles were associated with significantly longer length of stay (LOS) when compared to the fastest quartile (P = 0.003 and P = 0.002, respectively), but there was no increase in LOS as operative times progressed between the 2nd, 3rd, and 4th quartiles. LOS after conversion was longer but did not reach statistical significance when compared to laparoscopically completed operations in the longest quartile (5.0 vs 6.5 days, P = 0.075)
Conclusions
Our data do not support preemptive conversion of laparoscopic sigmoidectomy to avoid prolonged operative times. As long as progress is safely being made, surgeons are justified to continue pursuing laparoscopic completion.

Similar content being viewed by others

References
Bharucha AE, Parthasarathy G, Ditah I, Fletcher JG, Ewelukwa O, Pendlimari R, Yawn BP, Melton LJ, Schleck C, Zinsmeister AR (2015) Temporal trends in the incidence and natural history of diverticulitis: a population-based study. Am J Gastroenterol 110:1589–1596
Feingold D, Steele SR, Lee S, Kaiser A, Boushey R, Buie WD, Rafferty JF (2014) Practice parameters for the treatment of sigmoid diverticulitis. Dis Colon Rectum 57:284–294
Klarenbeek BR, Bergamaschi R, Veenhof AA, van der Peet DL, van den Broek WT, de Lange ES, Bemelman WA, Heres P, Lacy AM, Cuesta MA (2011) Laparoscopic versus open sigmoid resection for diverticular disease: follow-up assessment of the randomized control Sigma trial. Surg Endosc 25:1121–1126
Gervaz P, Inan I, Perneger T, Schiffer E, Morel P (2010) A prospective, randomized, single-blind comparison of laparoscopic versus open sigmoid colectomy for diverticulitis. Ann Surg 252:3–8
Klarenbeek BR, Coupé VM, van der Peet DL, Cuesta MA (2011) The cost effectiveness of elective laparoscopic sigmoid resection for symptomatic diverticular disease: financial outcome of the randomized control Sigma trial. Surg Endosc 25:776–783
Casillas S, Delaney CP, Senagore AJ, Brady K, Fazio VW (2004) Does conversion of a laparoscopic colectomy adversely affect patient outcome? Dis Colon Rectum 47:1680–1685
Bailey MB, Davenport DL, Vargas HD, Evers BM, McKenzie SP (2014) Longer operative time: deterioration of clinical outcomes of laparoscopic colectomy versus open colectomy. Dis Colon Rectum 57:616–622
Scheer A, Martel G, Moloo H, Sabri E, Poulin EC, Mamazza J, Boushey RP (2009) Laparoscopic colon surgery: does operative time matter? Dis Colon Rectum 52:1746–1752
Senagore AJ (2001) Laparoscopic techniques in intestinal surgery. Semin Laparosc Surg 8:183–188
Delaney CP, Fazio VW, Senagore AJ, Robinson B, Halverson AL, Remzi FH (2001) 'Fast track' postoperative management protocol for patients with high co-morbidity undergoing complex abdominal and pelvic colorectal surgery. Br J Surg 88:1533–1538
Zutshi M, Delaney CP, Senagore AJ, Mekhail N, Lewis B, Connor JT, Fazio VW (2005) Randomized controlled trial comparing the controlled rehabilitation with early ambulation and diet pathway versus the controlled rehabilitation with early ambulation and diet with preemptive epidural anesthesia/analgesia after laparotomy and intestinal resection. Am J Surg 189:268–272
Senagore AJ, Duepree HJ, Delaney CP, Brady KM, Fazio VW (2003) Results of a standardized technique and postoperative care plan for laparoscopic sigmoid colectomy: a 30-month experience. Dis Colon Rectum 46:503–509
Poles G, Stafford C, Francone T, Roberts PL, Ricciardi R (2018) What Is the Relationship between Operative Time and Adverse Events after Colon and Rectal Surgery? Am Surg 84:712–716
Jackson TD, Wannares JJ, Lancaster RT, Rattner DW, Hutter MM (2011) Does speed matter? The impact of operative time on outcome in laparoscopic surgery. Surg Endosc 25:2288–2295
Evans C, Lim J, Gatzen C, Huang A (2012) Factors influencing laparoscopic colorectal operative duration and its effect on clinical outcome. Surg Laparosc Endosc Percutan Tech 22:437–442
A S, G M, H M, E S, EC P, J M, RP B (2009). Laparoscopic colon surgery: does operative time matter? In: Editor ed.^eds. Book Laparoscopic colon surgery: does operative time matter? City: Dis Colon Rectum, 1746–52
Funding
Financial ties or grants to disclose.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
Drs. Williams, Stocchi, Aiello, Bhama, Kessler, Gorgun, Steele, Delaney, and Valente have no conflicts of interest or financial ties or grants to disclose .
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Williams, J., Stocchi, L., Aiello, A. et al. No need to watch the clock: persistence during laparoscopic sigmoidectomy for diverticular disease. Surg Endosc 35, 2823–2830 (2021). https://doi.org/10.1007/s00464-020-07717-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-020-07717-y