
Abstract
Background
Roux-en-Y gastric bypass excludes the biliary and pancreatic tree from traditional endoscopic evaluation and treatment. As the number of former bypass patients accrues, the need to assess and treat this subset of patients for biliary and pancreatic disease will increase. The authors describe their technique, indications, and outcomes for this group of patients.
Methods
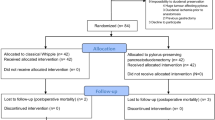
Data were collected by a retrospective chart review of the experience two surgeons had with laparoscopically assisted transgastric endoscopic retrograde cholangiopancreatography (ERCP) from July 2004 to October 2008 at a single institution. This review identified 22 cases. The operating surgeon performed the entire procedure. The indications were suspected sphincter of Oddi dysfunction in 18 patients and recurrent pancreatitis in four patients. Adhesions were lysed, and a purse-string suture was placed on the anterior portion of the stomach. A gastrotomy was made with monopolar electrocautery, and a 12 mm trocar was inserted. It was secured with a purse-string suture. A side-viewing duodenoscope was inserted through this port. An intestinal clamp was placed on the biliopancreatic limb. The intended interventions were sphincter of Oddi manometry, sphincterotomy, placement of a pancreatic duct stent, and injection of botulinum toxin if indicated.
Results
Laparoscopic access to the remnant stomach was sufficient for ERCP in 21 cases. One patient required conversion to an open procedure. A total of 12 patients had undergone prior open upper abdominal surgery. One retroperitoneal perforation was noted, with precut sphincterotomy and cannulation of the minor duodenal papilla and no clinical repercussions. Manometry was performed for 18 patients. The pancreatic duct cannulation rate for manometry was 89%, and the rate of bile duct cannulation for manometry was 94%. The manometry studies for 12 patients yielded abnormal results. Eight patients had transient improvement, and three patients had long-term improvement or resolution of symptoms after the index procedure. With additional treatment, two of the transient responders had long-term resolution of symptoms.
Conclusions
The findings demonstrate that gastric bypass patients with biliary pain can be successfully evaluated endoscopically by laparoscopic transgastric ERCP for sphincter of Oddi dysfunction. The rate for technical success and complications does not appear to be significantly greater than for standard ERCP. A few helpful techniques were noted during this experience. Comparison of efficacy with that of a prior study was limited.



Similar content being viewed by others


References
Lo SK (2008) ERCP in surgically altered anatomy. In: Baron TH, Kozarek R, Carr-Locke D (eds) ERCP. Saunders-Elsevier, Philadelphia, pp 237–258
Martinez J, Guerrero L, Byers P, Lopez P, Scagnelli T, Azuaje R, Dunkin B (2006) Endoscopic retrograde choalngiopancreatography and gastroduodenoscopy after Roux-en-Y gastric bypass. Surg Endosc 20:1548–1550
Patel JA, Patel NA, Shinde T, Uchal M, Dhawan M, Kulkarni A, Colella J (2008) Endoscopic retrograde cholaniopancreatography after laparoscopic Roux-en-Y gastric bypass: a case series and review of the literature. Am Surg 74:689–694
Corazziari E, Shaffer EA, Hogan W, Sherman S, Toouli J (1999) Functional disorders of the biliary tract and pancreas. Gut 45(Suppl2):45–54
Hogan W, Sherman S, Pasricha P, Carr-Locke DL (1997) Sphincter of Oddi manometry. Gastrointest Endosc 50:637–641
Roberts K, Panait L, Duffy AJ, Jamidar PA, Bell RL (2008) Laparoscopic-assisted transgastric endoscopy: current indications and future implications. JSLS 12:30–36
Mönkemüller K, Bellutti M, Neumann H, Malfertheiner P (2008) Therapeutic ERCP with the double-balloon enteroscope in patients with Roux-en-Y anastamosis. Gastrointest Endosc 67:992–995
Emmett DS, Mallat D (2007) Double-balloon ERCP in patients who have undergone Roux-en-Y surgery: a case series. Gastrointest Endosc 66:1038–1041
Sato H, Yamamoto H, Tamada K, Kita H, Wada S, Sunada K, Tano S, Hayashi Y, Sato Y, Yano T, Hanatuka K, Ajibe H, Hachimori H, Takamatsu T, Ito K, Shinozaki S, Iwamoto M, Miyata T, Kuno A, Tomiyama T, Ido K, Sugano K (2005) Application of double-balloon endoscopy for afferent limb lesions of Roux-en-Y surgical anastamoses. Gastrointest Endosc 61:AB238
Fogel EL, Sherman S (2006) Sphincter of Oddi dysfunction. In: Cotton P, Leung J (eds) Advanced digestive endoscopy: ERCP. Blackwell, Malden, MA, pp 165–198
Wehrmann T, Wiemer K, Lembcke B, Caspary WF, Juno M (1996) Do patients with sphincter of Oddi dysfunction benefit from endoscopic sphincterotomy? A 5 year prospective trial. Eur J Gastroenterol Hepatol 8:245–249
Choudhry U, Ruffolo T, Jamidar P, Hawes R, Lehman G (1993) Sphincter of Oddi dysfunction in patients with intact gallbladder: therapeutic response to endoscopic sphincterotomy. Gastrointest Endosc 39:492–495
Botoman VA, Kozarek RA, Novell LA, Patterson DJ, Ball TJ, Wechter DG, Neal LA (1994) Long-term outcome after endoscopic sphincterotomy in patients with biliary colic and suspected sphincter of Oddi dysfunction. Gastrointest Endosc 40:165–170
Bozkurt T, Orth KH, Butsch B, Lux G (1996) Long-term clinical outcome of postcholecystectomy patients with biliary-type pain results of manometry, noninvasive techniques, and endoscopic sphincterotomy. Eur J Gastroenterol Hepatol 8:245–249
Sherman S, Lehman GA, Jamidar P, Hawes RH, Silverman W, Madura J (1994) Efficacy of endoscopic sphincterotomy and surgical sphincterotomy for sphincter of Oddi dysfunction (SOD): randomized controlled study. Gastrointest Endosc 40:A125
Disclosures
Peter M. Bertin, Kirpal Singh, and Maurice E. Arregui have no conflicts of interest or financial ties to disclose.
Author information
Authors and Affiliations
Corresponding author
Additional information
Presented at the SAGES 2009 Annual Meeting, April 22--24, 2009, Phoenix, AZ.
Rights and permissions
About this article
Cite this article
Bertin, P.M., Singh, K. & Arregui, M.E. Laparoscopic transgastric endoscopic retrograde cholangiopancreatography (ERCP) after gastric bypass: case series and a description of technique. Surg Endosc 25, 2592–2596 (2011). https://doi.org/10.1007/s00464-011-1593-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-011-1593-5