
Abstract
Purpose
This study aims to investigate the clinical and molecular differences between diffuse large B-cell lymphoma (DLBCL) patients with MYD88L265P and MYD88other.
Methods
DLBCL patients with MYD88 variations were collected from the Cancer Hospital, Chinese Academy of Medical Sciences & Peking Union Medical College (CHCAMS), and Suzhou Municipal Hospital from February 6th, 2007 to May 20th, 2022. Clinicopathological parameters and treatment outcomes between MYD88L265P and MYD88other were investigated.
Results
A total of 132 patients with MYD88 variations from a cohort of 475 DLBCL patients were included, among which, 78 were MYD88L265P, while 54 were MYD88other. MYD88L265P was more common in non-GCB subtype than MYD88other (83% vs. 60%, P = 0.004). Besides, MYD88L265P was significantly related to higher proportion of testicle/ central nervous system involvement (31% vs. 6%, P < 0.001), PIM1 mutation (71% vs. 39%, P < 0.001), and PIM1 hypermutation (28% vs. 11%, P = 0.018), compared with MYD88other. Compared with MYD88L265P, MYD88other were more likely to have higher percentage of advanced stage (60% vs. 42%, P = 0.044), extranodal site ≥ 2 (45% vs. 28%, P = 0.044), elevated LDH (55% vs. 35%, P = 0.033), positive CD10 expression (36% vs. 16%, P = 0.009), BCL-6 translocation (20% vs. 8%, P = 0.033), and NOTCH pathway gene alteration (24% vs. 13%, P = 0.040). In non-GCB DLBCL subtype, patients with MYD88other were significantly associated with worse progression free survival (PFS) than those with MYD88L265P when treated initially with R-CHOP/R-CHOP-like regimen (P = 0.010).
Conclusion
The findings of this study indicate that DLBCL patients with MYD88L265P and MYD88other are likely to be two subgroups with different clinical and molecular characteristics. The survival of patients with MYD88other is not superior than those with MYD88L265P, even poorer when focusing on the non-GCB subtype.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Diffuse large B-cell lymphoma (DLBCL) is a highly heterogeneous lymphoid malignancy in adults, representing the most common entity in non-Hodgkin lymphomas (Alaggio et al. 2022). Despite about 60% DLBCL patients can be cured via standard front-line rituximab plus cyclophosphamide, doxorubicin, vincristine, and prednisone (R-CHOP), most of those refractory and relapse patients will succumb to their disease (Flowers et al. 2010; Shi et al. 2022). With the development of large-scale high-throughput sequencing technologies, the underlying heterogeneity in DLBCL has been characterized at an unprecedented scale. Genomic aberration-based classification of DLBCL subtypes is becoming increasingly accepted. Several taxonomies such as the four subtypes (MCD, N1, EZB, BN2), five subtypes (Cluster 1–5) or (MYD88, BCL2, SOCS1/SGK1, TET2/SGK1, and NOTCH2), and seven subtypes (MCD, N1, A53, BN2, ST2, EZB-MYC+, EZB-MYC−) have been reported (Schmitz et al. 2018; Chapuy et al. 2018; Lacy et al. 2020; Wright et al. 2020). Genetic subtypes provide useful prognostic information and treatment reference for clinical oncologist. Of special note is MYD88 mutation is a pivotal genetic driver determining the genetic classification in all above mentioned taxonomies and is mostly deemed to be an unfavorable prognostic factor along with CD79B mutation.
MYD88 encodes an adapter protein that functions as an essential signal transducer in the interleukin-1 and Toll-like receptor signaling pathways (Iwasaki and Medzhitov 2010; Ishii and Akira 2006). MYD88 Leu 265 Pro (L265P) mutation, occurred in about 30% of activated B-cell-like (ABC) DLBCL, is the most common non-synonymous and gain-of-function driver mutation. In contrast, this mutation is rare in GCB cases (Ngo et al. 2011; Dubois et al. 2017; Rovira et al. 2016a). Other recurrent non-L265P variants of MYD88 were also identified in DLBCL. However, their role in DLBCL lacks adequate attention due to the low prevalence. Several studies have indicated the difference between MYD88L265P and MYD88other but lacking of direct and detailed comparison in clinical and genetic features. Besides, the samples are limited, which might cause insufficient analysis and biased conclusions. Moreover, the survival of DLBCL patients with MYD88L265P and MYD88other varies in different studies, which is still a matter of debate (Chapuy et al. 2018; Dubois et al. 2017; Rovira et al. 2016; Xie et al. 2022).
Therefore, this study intends to investigate the clinical characteristics, genetic alteration, and survival of DLBCL patients between MYD88L265P and MYD88other variants through retrospective analysis of 132 patients with MYD88 variations in a cohort of 475 DLBCL patients from the Cancer Hospital, Chinese Academy of Medical Sciences & Peking Union Medical College (CHCAMS), and Suzhou Municipal Hospital, hoping to better detail the clinical and genetic background of DLBCL patients with MYD88L265P and MYD88other.
Materials and methods
Patient selection and data collection
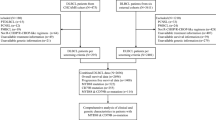
This study retrospectively collected 475 patients diagnosed with de novo DLBCL by two experienced pathologists at the CHCAMS and Suzhou Municipal Hospital from February 6th, 2007 to May 20th, 2022. A total of 132 patients with MYD88 variations were included for analysis. The inclusion criteria were as follows: (1) patients were histologically diagnosed with DLBCL based on the World Health Organization classification of Tumors of Hematopoietic and Lymphoid Tissue (2008) (Sabattini et al. 2010); (2) patients were confirmed MYD88 variation via next generation sequencing (NGS) technology as part of routine procedure; (3) patients who provided informed consent and adequate tissue for molecular and genetic detection. The exclusion criteria were those cases without adequate tissue for molecular and genetic detection or the information of MYD88 variation was unavailable. For survival analysis, we excluded patients with primary mediastinal large B-cell lymphoma, primary testicular DLBCL, and primary central nerves system lymphoma because of their particular biological behavior, clinical characteristics, treatment management, and prognosis. Only 85 patients who were received R-CHOP or R-CHOP-like regimens and with well-documented progression free survival (PFS) (from the date of initial diagnosis to the date of disease progression, relapse or death from any causes), overall survival (OS) (from the date of initial diagnosis to death from any causes), and survival status data were eventually included. The screening flowchart is displayed in Fig. 1. The study was approved by the Institutional Review Board of National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital, Chinese Academy of Medical Sciences & Peking Union Medical College (No. NCC2018JJJ-004) and was conducted in accordance with the ethical standards of the institutional committee and with the Declaration of Helsinki.

Flow chart of the study design
Patients baseline clinical characteristics, molecular and genetic alteration information, and follow-up data were collected, including gender, age, Ann Arbor stage, Eastern Cooperative Oncology Group (ECOG) performance status (PS), number of extranodal involvement sites, lactate dehydrogenase (LDH) level, International Prognostic Index (IPI) score, bulky disease, B symptoms, primary site, testicle/central nervous system (CNS) involvement, relapse, bone marrow/peripheral blood involvement, cell of origin (COO) type, first-line therapy, protein expression of CD5, CD10, CD20, BCL-2, BCL-6, c-MYC, MUM-1, Ki-67, and PD-L1, genetic alteration of CD79, TP53, BCL-2, BCL-6, c-MYC, PIM1, SGK1, cell cycle-related genes (CDKN2A, CCND3), NOTCH pathway-related genes (NOTCH1, NOTCH2, DTX1), JAK-STAT pathway-related genes (SOCS1, STAT3, STAT6), PI3K pathway-related genes (ITPKB, PTEN), immune-related genes (B2M, CIITA, CD58), epigenetics-related genes (KMT2D, KMT2C, CREBBP, EP300, TET2, EZH2, MEF2B), RAS pathway-related genes (GNA13, RHOA, RAS, BRAF). Any gene occurred alteration in the pathway will be defined as “pathway gene alteration”.
Immunohistochemical staining and scoring
Formalin-fixed paraffin-embedded (FFPE) tissues were obtained from included patients. The protein expression of CD5, CD10, CD20, BCL-2, BCL-6, c-MYC, MUM-1, and Ki-67 were evaluated by immunohistochemistry (IHC) using associated antibodies (Fuzhou 100 Maixin Biotech, Fuzhou, China). The Programmed death-ligand 1 (PD-L1) expression was detected using the 22C3 anti-PD-L1 rabbit monoclonal antibody (Beijing Hightrust Diagnostic Company Limited, Beijing, China). The COO classification was confirmed according to the Hans algorithm (Hans et al. 2004). The expression of BCL-2 ≥ 60%, BCL-6 ≥ 30%, and c-MYC ≥ 40% of tumor cells was regarded as positive, respectively as previously reported (Zhang et al. 2018; Johnson et al. 2012).
Detection of chromosome translocation
Interphase fluorescence in situ hybridization (FISH) was performed on three-micrometer-thick FFPE tumor tissues using Vysis LSI CMYC/BCL2/BCL6 Dual Color Break Apart Rearrangement Probe (Abbott Molecular, Abbott Park, IL, USA) according to the manufacturer’s instructions. Assessment of FISH signals was performed using Zeiss Axio Imager M2 epifluorescence microscope (Carl Zeiss, Oberkochen, Germany). Fifty tumor cells were counted, and the percentage of tumor cells with split-signal over 15% indicated the translocation of c-MYC, BCL-2, or BCL-6.
Next-generation sequencing
Genomic DNA was extracted from the collected FFPE DLBCL tissues using the QIAamp DNA FFPE tissue kit (Qiagen, Hilden, Germany). DNA concentration was quantified using Qubit dsDNA HS Assay Kit (Invitrogen, Carlsbad, CA, USA). DNA fragmentation was conducted using Covaris S2 Ultrasonicator (Covaris, Woburn, MA, USA). Fragments of 200–250 bp were selected by AMPure beads (Agencourt AMPure XP kit; Beckman Coulter, Brea, CA, USA). End repair, phosphorylation, adaptor ligation, hybridization with capture-probe baits, hybrid selection with magnetic beads, and polymerase chain-reaction amplification were subsequently processed. Two capture panels were adopted, one consisted of 112 commonly altered genes in lymphoma and hematologic malignancies, the other covering 413 frequently mutated genes in DLBCL. There were 101 overlapping genes between the two panels. Capture-based targeted sequencing was performed on a Next Seq500 Sequencer (Illumina, Hayward, CA, USA) with pair-end reads at Geneplus-Beijing (Beijing, China) or Burning Rock Biotech (Guangzhou, China). Detailed sequencing procedure was performed as our previous study described (Qin et al. 2020, 2021; Jiang et al. 2020a, b).
Statistical analysis
Chi-squared test or Fisher’s exact test when appropriated was adopted for the comparisons between categorical variables. Kaplan–Meier survival curve and log-rank test were performed for comparing the PFS and OS. P-value below 0.05 was considered statistically significant. All statistics were achieved via R software, version 4.21 (https://www.r-project.org/).
Results
Clinical and genetic characteristics of DLBCL patients with MYD88 variations
A total of 132 patients with MYD88 variations from a cohort of 475 DLBCL patients were included in this study. The variation rate of MYD88 is 28% (132/475). Among the patients with MYD88 variation, 59% (78/132) occurred MYD88L265P, while 41% (54/132) were MYD88other. Among patients with MYD88other, the p.S219C (14/54), p.L273P (10/54), and p.S243N (6/54) were the top three frequently occurred mutations (Fig. 2). Ninety-six percent (127/132) of the MYD88 variations were missense mutation. In addition to MYD88 variations, plenty of associated genes occurred genetic alterations in over ten percent of cases including PIM1 (53%), CD79B (36%), KMT2D (33%), TP53 (20%), BCL2 (19%), PRDM1 (17%), IRF4 (14%), CREBBP (13%), BCL6 (12%), BM2 (11%), TET2 (11%), EP300 (11%), and DTX1 (11%) (Fig. 3). The median age of the included patients was 62 years old. Patients diagnosed at limited stage (66/132) and advanced stage (63/132) were comparable, while the number of patients with IPI < 3 was almost twice than those patients with IPI ≥ 3. Most of patients were classified into non-GCB subtype (96/132). Twenty percent (27/132) of patients suffered testicle or CNS involvement. Seventy-four percent (98/132) of patients received R-CHOP or R-CHOP-like regimen. During the follow-up, forty-six percent (61/132) of the cases occurred disease relapse, while twenty-two percent (29/132) of the patients occurred death (Table 1).

Distribution of MYD88 variants

Genetic alterations in DLBCL. A Overview of the genetic alteration profile between MYD88L265P and MYD88other. B Distribution of the top frequently mutated genes between MYD88L265P and MYD88other
Clinicopathological characteristics and genetic alterations in different MYD88 variants
Detailed patient clinicopathological characteristics and genetic alterations, as well as their associations with different MYD88 variation type were displayed in Table 1 and Supplementary file 1. We found that COO subtype, Ann Arbor stage, extranodal site, LDH, testicle/CNS involvement, CD10 expression, BCL-6 translocation, NOTCH pathway gene alteration, PIM1 mutation, and PIM1 hypermutation showed statistically significant distribution between MYD88L265P and MYD88other variants (Figs. 4 and 5). Specifically, MYD88L265P was more common seen in non-GCB subtype than MYD88other (83% vs. 60%, P = 0.004, Fig. 4A). Meanwhile, MYD88L265P was significantly related to higher proportion of testicle/CNS involvement (31% vs. 6%, P < 0.001, Fig. 4B), PIM1 mutation (71% vs. 39%, P < 0.001, Fig. 4C), and PIM1 hypermutation (28% vs. 11%, P = 0.018, Fig. 4D), compared with MYD88other. Instead, MYD88other were more likely to have higher percentage of advanced stage (60% vs. 42%, P = 0.044, Fig. 5A), extranodal site ≥ 2 (45% vs. 28%, P = 0.044, Fig. 5B), elevated LDH (55% vs. 35%, P = 0.033, Fig. 5C), positive CD10 expression (36% vs. 16%, P = 0.009, Fig. 5D), BCL-6 translocation (20% vs. 8%, P = 0.033, Fig. 5E), and NOTCH pathway gene alteration (24% vs. 13%, P = 0.040, Fig. 5F), compared with MYD88L265P.

Significantly higher proportion of variables in MYD88L265P than MYD88other. A COO subtype; B Testicle/CNS involvement; C PIM1 mutation; D PIM1 hypermutation

Significantly higher proportion of variables in MYD88other than MYD88L265P. A Ann Arbor stage; B extranodal site; C LDH; D CD10 expression; E BCL-6 translocation; F NOTCH pathway gene alteration
Treatment outcome between different MYD88 variants patients
A total of 85 patients were included for survival analysis, among which, 42 patients occurred MYD88L265P, while 43 patients occurred MYD88other. The median follow-up was 15.4 months (range: 0.5–118 months). A total of 21 patients eventually occurred death. No statistically significance was observed in PFS and OS between MYD88L265Pand MYD88other (Fig. 6).

Prognostic significance of MYD88L265P and MYD88other in the whole DLBCL patients. A Progress-free survival. B Overall survival
We further investigated the survival between MYD88L265P and MYD88other variants in GCB and non-GCB subtype. In non-GCB subtype, 33 patients occurred MYD88L265P, while 26 patients were MYD88other. Compared with MYD88L265P, patients with MYD88other had worse PFS (median PFS: 9.77 months vs. 24.73 months, HR = 2.32, P = 0.010) (Fig. 7C). Regarding OS, patients with MYD88other also showed a trend to suffer worse outcome than those with MYD88L265P (median OS: 39.5 months vs. not reached, HR = 2.46, P = 0.090) (Fig. 7D). However, no statistical significance was observed for PFS or OS between MYD88L265P and MYD88other in GCB subtype (Fig. 7A, B).

Prognostic significance of MYD88L265P and MYD88other in DLBCL subtypes. A Progress-free survival in GCB-DLBCL. B Overall survival in GCB-DLBCL. C Progress-free survival in non-GCB-DLBCL. D Overall survival in non-GCB-DLBCL
Discussion
MYD88 mutation is a widely accepted pivotal oncogenic driver in B-cell lymphomas, among which, the hotspot MYD88L265P is mostly studied. In this study, the mutation frequency of MYD88L265P is 59%, which is slightly lower than Dubois et al. reported as 64%. For MYD88other, Dubois et al. identified the frequent variants were p.S243A, p.S219C, p.V217P, and p.M232T, while our results showed that p.S219C, p.L273P, and p.S243N were the top three frequent variants (Dubois et al. 2017). This reflects great complexity and heterogeneity of MYD88other variants in different cohorts of DLBCL. We found that MYD88L265P was more common in non-GCB DLBCL compared with MYD88other (83% vs. 60%, P = 0.004), which is consistent with previous reports (Ngo et al. 2011; Rovira et al. 2016a). As we know, the ABC DLBCL is characterized with chronic B-cell receptor signaling and activation of NF-κB (Davis et al. 2010, 2001; Havranek et al. 2017; Compagno et al. 2009). MYD88L265P has been identified as non-synonymous and gain-of-function driver mutation, which can promote cell survival via assembling IRAK1 and IRAK4 contained protein complex, leading to IRAK4 kinase activity, IRAK1 phosphorylation, NF-κB signalling, and JAK kinase activation of STAT3 in ABC DLBCL (Ngo et al. 2011). This might help explain why MYD88L265P is more frequent in non-GCB DLBCL. Nevertheless, in patients with MYD88other, non-GCB DLBCL still accounts for 60%, which might indicate the biological effect of some MYD88other variants and MYD88L265P is similar to some extent. A previous study also indicated their similarities. In Ngo’s study, most of MYD88other reside in MYD88 Toll/IL-1 receptor (TIR) domain, which is the same domain as MYD88L265P resides. As regards the ability to activate NF-κB, MYD88wild−type presents modest activity, MYD88L265P has strong activity, as does MYD88M232T and MYD88S243N, while MYD88S222R and MYD88T294P exert intermediate effect. Their results suggested MYD88other can contribute to the constitutive NF-κB activation in ABC DLBCL as with MYD88L265P (Ngo et al. 2011). Given that, patients with MYD88other should be also brought to attention in clinical. Intriguingly, there were 17% and 40% of GCB DLBCL patients with MYD88L265P and MYD88other, respectively. Albeit GCB DLBCL is not typically characterized by constitutive NF-κB activation. However, classic and alterative NF-κB pathway can be activated in both ABC and GCB DLBCL. About 60% ABC DLBCL and 30% GCB DLBCL present nuclear localization of NFKB1/p50 (classical pathway) and NFKB2/p52 (alternative pathway) (Compagno et al. 2009). Besides, mutations of BCR/PI3K signaling intermediates (RHOA, GNA13, and SGK1) and NF-kB modifiers (CARD11, NFKBIE, and NFKBIA) were also found to be enriched in cluster 4 subtype of DLBCL, which is primary GCB DLBCL (Chapuy et al. 2018). Whether those GCB DLBCL with MYD88 alteration will be involved in NF-κB pathway remains to be explored in future study.
The genomic background hidden behind MYD88 is extremely complicated. We found that patients with MYD88 variation also frequently occurred PIM1, CD79B, KMT2D, TP53, BCL2, PRDM1, IRF4, CREBBP, BCL6, BM2, TET2, EP300, and DTX1 alterations. This is partly in accordance with previously reported results (Dubois et al. 2017; Shen et al. 2020). We found that the CD10 expression, NOTCH pathway gene alteration, and BCL-6 translocation were more common in MYD88other than MYD88L265P. On the contrary, the PIM1 mutation and PIM1 hypermutation were more common in MYD88L265P than MYD88other. These provided some clues implying why MYD88other is more likely related to GCB subtype. For example, CD10 and BCL6 are markers of germinal center B cell. DLBCL patients with CD10 + , or CD10-/BCL6 + /MUM1- was classified into GCB subtype according to COO algorism (Alizadeh et al. 2000). Besides, according to several large-scale genetics-based classification of DLBCL subtype articles, PIM1 mutation was less frequent in GCB DLBCL (Schmitz et al. 2018; Chapuy et al. 2018; Lacy et al. 2020; Wright et al. 2020; Reddy et al. 2017). However, the BCL6 translocation, NOTCH1 mutation, and NOTCH2 mutation were all reported to be more common in non-GCB subgroup, which still remains confusing on their preference in MYD88other (Schmitz et al. 2018). Given above, the intricate genomic variation underlies MYD88 variation type and their relationship with COO subtype requires persistent investigation.
No significant difference in PFS and OS between MYD88L265P and MYD88other was observed in the whole DLBCL group. However, when focusing on the non-GCB type, the PFS of patients with MYD88other was significantly shorter than those with MYD88L265P. Several studies have investigated the survival of DLBCL patients between MYD88L265P and MYD88other variants. In Dubois’s study, he performed a survival analysis on 26 ABC DLBCL patients with MYD88L265P and 9 ABC DLBCL patients with MYD88other, who all received R-CHOP therapy. No statistical significance was found in OS and PFS (Dubois et al. 2017). Another study also investigated the PFS and OS between 39 patients with MYD88L265P and 8 patients with MYD88other. Their results suggested that the OS and PFS of patients with MYD88L265P showed a trend to be inferior than that of patients with MYD88other, but didn’t achieve statistically significant (Rovira et al. 2016). The samples in the two above studies are limited, which might lead to insufficient statistical efficacy and bias results. Compared with the above two studies, larger samples including 42 patients with MYD88L265P and 43 patients with MYD88other were performed for survival analysis in this study. MYD88other was indicated as an unfavorable factor in DLBCL patients especially in non-GCB subgroup. Why patients with MYD88other showed not superior survival than those with MYD88L265P remains to be discussed. We did find that patients with MYD88other presented higher percentage of advanced stage, extranodal site ≥ 2, and elevated LDH than those with MYD88L265P, which may provide some hints. Nevertheless, the genetic alteration and corresponding biological function difference between MYD88L265P and MYD88other may be the predominant factors influencing survival, which needs further study.
Altogether, this study highlights the clinical and genomic heterogeneity hidden behind the MYD88L265P and MYD88other variants. Furthermore, prognostic differences were revealed, most notably highlighting the survival of patients with MYD88other is not superior than those with MYD88L265P, even poorer when focusing on the non-GCB subtype. Finally, this study added the importance of MYD88 variants status to the current knowledge and provided reference for the individualized targeted therapy and management of DLBCL patients.
Data availability
The data supporting the conclusions of this study can be obtained upon a reasonable request from the corresponding author.
References
Alaggio R, Amador C, Anagnostopoulos I et al (2022) The 5th edition of the World Health Organization classification of haematolymphoid tumours: lymphoid neoplasms. Leukemia 36(7):1720–1748. https://doi.org/10.1038/s41375-022-01620-2
Alizadeh AA, Eisen MB, Davis RE et al (2000) Distinct types of diffuse large B-cell lymphoma identified by gene expression profiling. Nature 403(6769):503–511. https://doi.org/10.1038/35000501
Chapuy B, Stewart C, Dunford AJ et al (2018) Molecular subtypes of diffuse large B cell lymphoma are associated with distinct pathogenic mechanisms and outcomes. Nat Med 24(5):679–690. https://doi.org/10.1038/s41591-018-0016-8
Compagno M, Lim WK, Grunn A et al (2009) Mutations of multiple genes cause deregulation of NF-kappaB in diffuse large B-cell lymphoma. Nature 459(7247):717–721. https://doi.org/10.1038/nature07968
Davis RE, Brown KD, Siebenlist U, Staudt LM (2001) Constitutive nuclear factor kappaB activity is required for survival of activated B cell-like diffuse large B cell lymphoma cells. J Exp Med 194(12):1861–1874. https://doi.org/10.1084/jem.194.12.1861
Davis RE, Ngo VN, Lenz G et al (2010) Chronic active B-cell-receptor signalling in diffuse large B-cell lymphoma. Nature 463(7277):88–92. https://doi.org/10.1038/nature08638
Dubois S, Viailly PJ, Bohers E et al (2017a) Biological and clinical relevance of associated genomic alterations in MYD88 L265P and non-L265P-mutated diffuse large B-Cell lymphoma: analysis of 361 cases. Clin Cancer Res 23(9):2232–2244. https://doi.org/10.1158/1078-0432.CCR-16-1922
Flowers CR, Sinha R, Vose JM (2010) Improving outcomes for patients with diffuse large B-cell lymphoma. CA Cancer J Clin 60(6):393–408. https://doi.org/10.3322/caac.20087
Hans CP, Weisenburger DD, Greiner TC et al (2004) Confirmation of the molecular classification of diffuse large B-cell lymphoma by immunohistochemistry using a tissue microarray. Blood 103(1):275–282. https://doi.org/10.1182/blood-2003-05-1545
Havranek O, Xu J, Kohrer S et al (2017) Tonic B-cell receptor signaling in diffuse large B-cell lymphoma. Blood 130(8):995–1006. https://doi.org/10.1182/blood-2016-10-747303
Ishii KJ, Akira S (2006) Innate immune recognition of, and regulation by. DNA. Trends Immunol. 27(11):525–532. https://doi.org/10.1016/j.it.2006.09.002
Iwasaki A, Medzhitov R (2010) Regulation of adaptive immunity by the innate immune system. Science 327(5963):291–295. https://doi.org/10.1126/science.1183021
Jiang S, Qin Y, Jiang H et al (2020a) Molecular profiling of Chinese R-CHOP treated DLBCL patients: Identifying a high-risk subgroup. Int J Cancer 147(9):2611–2620. https://doi.org/10.1002/ijc.33049
Jiang S, Qin Y, Gui L et al (2020b) Genomic alterations and MYD88(MUT) variant mapping in patients with diffuse large B-cell lymphoma and response to ibrutinib. Target Oncol 15(2):221–230. https://doi.org/10.1007/s11523-020-00710-4
Johnson NA, Slack GW, Savage KJ et al (2012) Concurrent expression of MYC and BCL2 in diffuse large B-cell lymphoma treated with rituximab plus cyclophosphamide, doxorubicin, vincristine, and prednisone. J Clin Oncol 30(28):3452–3459. https://doi.org/10.1200/JCO.2011.41.0985
Lacy SE, Barrans SL, Beer PA et al (2020) Targeted sequencing in DLBCL, molecular subtypes, and outcomes: a Haematological Malignancy Research Network report. Blood 135(20):1759–1771. https://doi.org/10.1182/blood.2019003535
Ngo VN, Young RM, Schmitz R et al (2011) Oncogenically active MYD88 mutations in human lymphoma. Nature 470(7332):115–119. https://doi.org/10.1038/nature09671
Qin Y, Jiang S, Liu P et al (2020) Characteristics and Management of TP53-Mutated Diffuse Large B-Cell Lymphoma Patients. Cancer Manag Res 12:11515–11522. https://doi.org/10.2147/CMAR.S269624
Qin Y, Chen H, Liu P et al (2021) Prognostic value of BCL2 and TP53 genetic alterations for diffuse large B-cell lymphoma patients treated with R-CHOP. Cancer Biol Med. https://doi.org/10.20892/j.issn.2095-3941.2021.0193
Reddy A, Zhang J, Davis NS et al (2017) Genetic and functional drivers of diffuse large B cell lymphoma. Cell 171(2):481-494.e15. https://doi.org/10.1016/j.cell.2017.09.027
Rovira J, Karube K, Valera A et al (2016a) MYD88 l265p mutations, but no other variants, identify a subpopulation of DLBCL patients of activated B-cell origin, extranodal involvement, and poor outcome. Clin Cancer Res 22(11):2755–2764. https://doi.org/10.1158/1078-0432.CCR-15-1525
Sabattini E, Bacci F, Sagramoso C, Pileri SA (2010) WHO classification of tumours of haematopoietic and lymphoid tissues in 2008: an overview. Pathologica 102(3):83–87
Schmitz R, Wright GW, Huang DW et al (2018) Genetics and pathogenesis of diffuse large B-cell lymphoma. N Engl J Med 378(15):1396–1407. https://doi.org/10.1056/NEJMoa1801445
Shen R, Xu PP, Wang N et al (2020) Influence of oncogenic mutations and tumor microenvironment alterations on extranodal invasion in diffuse large B-cell lymphoma. Clin Transl Med 10(7):e221. https://doi.org/10.1002/ctm2.221
Shi Y, Chen H, Qin Y et al (2022) Clinical characteristics and treatment outcomes of Chinese diffuse large B-cell lymphoma patients in the era of rituximab (2005–2018). Cancer Pathogen Ther. https://doi.org/10.1016/j.cpt.2022.09.006
Wright GW, Huang DW, Phelan JD et al (2020) a probabilistic classification tool for genetic subtypes of diffuse large B cell lymphoma with therapeutic implications. Cancer Cell 37(4):551–56814. https://doi.org/10.1016/j.ccell.2020.03.015
Xie J, Shen X, Shi Q et al (2022) Clinical significance of MYD88 non-L265P mutations in diffuse large B-cell lymphoma. Hematol Oncol 40(5):885–893. https://doi.org/10.1002/hon.3073
Zhang Y, Wang H, Ren C et al (2018) Correlation between C-MYC, BCL-2, and BCL-6 protein expression and gene translocation as biomarkers in diagnosis and prognosis of diffuse large B-cell lymphoma. Front Pharmacol 9:1497. https://doi.org/10.3389/fphar.2018.01497
Acknowledgements
The authors would like to thank all the patients and their families.
Funding
This study was funded by China National Major Project for New Drug Innovation (2017ZX09304015) and Beijing National Science Foundation (H2018206591).
Author information
Authors and Affiliations
Contributions
YQ: Data curation, Writing-Original draft preparation and revising. TQ: Data curation, Writing-Original draft preparation and revising. ZCX: Data analysis and visualization, Writing-Original draft preparation. XRC: Data curation. PL: Data curation. JLY: Data curation. XHH: Data curation. LG: Data curation. SYZ: Data curation. HXJ: Data curation. CGZ: Data curation. SY: Data curation. LT: Data curation. YKS: Conceptualization, Methodology, Writing-Reviewing and Editing.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no potential conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Qin, Y., Qiu, T., Xie, Z. et al. MYD88L265P and MYD88other variants show different molecular characteristics and prognostic significance in diffuse large B-cell lymphoma. J Cancer Res Clin Oncol 149, 8483–8494 (2023). https://doi.org/10.1007/s00432-023-04714-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00432-023-04714-1