
Abstract
Objectives
The aim of the study was to examine the associations between heavy physical workload among middle-aged and older workers and disability pension due to any diagnosis, as well as musculoskeletal, psychiatric, cardiovascular or respiratory diagnoses. The population-based design made it possible to examine dose–response and potential gender differences in the associations.
Methods
About 1.8 million men and women aged 44–63 years and registered as living in Sweden in 2005 were followed regarding disability pension during 2006–2016, until ages 55–65 years. Mean values of physical workload and job control, estimated through gender-specific job-exposure matrices (JEMs), were assigned to individuals through their occupational titles in 2005. Exposure values were ranked separately for women and men and divided into quintiles. Associations were analyzed with Cox proportional-hazards regression.
Results
The analyses showed robust, dose–response associations between physical workload and disability pension with a musculoskeletal diagnosis in both genders: the adjusted hazard ratio and 95% confidence interval for those with the heaviest exposure was 2.58 (2.37–2.81) in women and 3.34 (2.83–3.94) in men. Dose–response associations were also seen in relation to disability pension with a cardiovascular or a respiratory diagnosis, though the hazard ratios were smaller. Physical workload was not associated with disability pension with a psychiatric diagnosis after adjustment for job control.
Conclusion
This study of the entire Swedish population of middle-aged and older workers suggests that higher degrees of physical workload may increase the risk of disability pension overall, and specifically with musculoskeletal, cardiovascular or respiratory diagnosis, in both women and men.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Background
Because of impaired health, many working-aged people are eventually excluded from the labor market and receive their income through the welfare system. With today’s aging populations and political goals to keep older people in the workforce, this is considered increasingly problematic (Eurofound 2015). Occupational groups show large differences in rates of sickness absence and disability pension (Piha et al. 2013; Ropponen et al. 2013; Samuelsson et al. 2013; Stattin and Jarvholm 2005), which indicate that certain aspects of work may be difficult to reconcile with illness and reduced capacity.
Heavy physical workload, including heavy manual handling, awkward body postures, repetitive and circulatory demanding work, seems to decrease the possibility of continuing to work up until an older age. Several studies have shown that disability pension is much more frequent among workers with heavy physical workload than in those without (Emberland et al. 2017; Ervasti et al. 2019; Friis et al. 2008; Halonen et al. 2019; Jarvholm et al. 2014; Karkkainen et al. 2013; Karpansalo et al. 2002; Kjellberg et al. 2016; Labriola et al. 2009; Lahelma et al. 2012; Prakash et al. 2017; Ropponen et al. 2014; Sommer et al. 2016). Other studies have shown that long-term sickness absence, which usually precedes disability pension, is also more common (Andersen et al. 2016; Sommer et al. 2016; Sundstrup et al. 2018). Furthermore, when older manual workers are asked, they specifically highlight physical workload as an occupational barrier and reason for early retirement (Andersen et al. 2019).
The associations between heavy physical workload and disability pension with a musculoskeletal or psychiatric diagnosis–the most common diagnoses–have been the subject of most previous studies and, in these, a clear increase in risk of disability pension with a musculoskeletal diagnosis has been shown (Ervasti et al. 2019; Karkkainen et al. 2013; Karpansalo et al. 2002; Kjellberg et al. 2016; Lahelma et al. 2012; Ropponen et al. 2014). Less frequent disability pensions, such as disability pensions with a cardiovascular (CVD) or a respiratory diagnosis, have not been possible to examine reliably in relation to physical workload (Karpansalo et al. 2002). However, these are diagnoses that likely impair performance in a job with heavy physical workload and, in this way, increase risk of early exit from the labor market through disability pension.
Previous studies have been limited by size and sometimes to certain occupations or labor-market sectors. Therefore, these studies have not been able to examine whether the rate of disability pension increases across the full range of physical workload. Few studies have been able to investigate this separately for female and male workers, although it is of interest as women and men are often relatively segregated in different sectors and occupational groups in the labor market. It is also of interest to investigate this association while simultaneously taking psychosocial working conditions into account. For example, heavy physical work is often co-occurring with small opportunities for workers to influence when and how tasks are to be performed (low job control), which has been linked to increased risk of labor-market exit through disability pension (Knardahl et al. 2017).
The purpose of this study is to contribute to an enhanced understanding of the association between heavy physical workload and early exit from the labor market through disability pension among aging workers. To achieve this aim, we studied the entire Swedish population of middle-aged and older working men and women. Hypothesized dose–response associations with all-cause and cause-specific disability pension were examined using a job-exposure matrix (JEM) for classification of physical workload, and also job control, across the full range of the workers’ occupations.
Methods
Study population, setting, and design
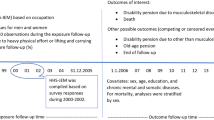
The study is based on the recently established Swedish Work, Illness, and labor-market Participation (SWIP) cohort, which includes all individuals 16–64 years of age and registered as living in Sweden in 2005, i.e. 5.4 million. We used a sub-population consisting of the 946,523 women and 888,032 men born during the years 1942–1961 and with occupational code available for the baseline year of the study, 2005. This corresponds to 76.9% of the almost 2.4 million individuals in total within the selected age range, which includes non-workers such as those already on early retirement at baseline. Follow-up regarding date and diagnosis of disability pension was made prospectively for the years 2006–2016. At baseline, the individuals in the study were aged 44–63 years; younger individuals were excluded, because, among them, disability pensions are less likely to be caused by work-environment factors.
Data collection and variables
Data on occupations, classified on a four-digit level according to SSYK96 (Sweden’s classification of occupations based on ISCO-88), were obtained from Statistics Sweden’s ‘LISA’ register (‘Longitudinal integrated database for health insurance and labour market studies’) (Ludvigsson et al. 2019). The register starts in the year 1990 and contains information on every individual in Sweden aged 16–64, but occupational data are only available from 2005. The data on occupations were linked to the cohort and used for classification of work-environmental exposure using job-exposure matrices (see below for description of variables). Further data, used for multivariable analyses (age, gender, education, marital status, history of unemployment, and registered sickness absence), were obtained either from the LISA register, the Total Population Register at Statistics Sweden (Ludvigsson et al. 2016), or the Swedish Social Insurance Agency’s MIDAS register (‘Micro Data for Analysis of the Social Insurance System’, see forsakringskassan.se 2020a). An overview of the utilization of register data in the study is shown in Table S1.
Physical workload (exposure)
The study participants' degree of overall occupational physical workload was classified using a recently developed job-exposure matrix (JEM) for physical workload applicable to up to 355 occupations in Sweden. This JEM is based on data from the Swedish Work Environment Surveys 1997–2013, which in turn derives from eight questions regarding physical loads that involve heavy lifting, uncomfortable working postures, repetitive work and physically demanding work (Badarin et al. 2021). A gender-specific index mean value for the overall physical exposure, based on the eight questions, was obtained from the matrix and linked to individuals through yearly data on their occupations in 2005. Quintiles of physical workload were created based on the gender-specific mean values.
Disability pension (outcome)
In Sweden, disability pension (from the year 2003 termed ‘sjukersättning’, i.e. sickness compensation) is a compensation for those between ages 30 and 64 who will probably never be able to work full time due to illness, injury or disability (forsakringskassan.se 2020b). There must be a proven reduction in work ability by at least one fourth “in all jobs on the labour market”, including jobs that are arranged for persons with disabilities, such as employment with salary grants. Depending on how much the work ability is reduced, full, three-quarter, one-half or one-quarter disability pension may be paid. The Social Insurance Agency can initiate the process itself, but disability pension is otherwise applied for. Due to a policy change in 2006, the proportion of applications granted has been sharply reduced and is currently based on a thorough examination of the degree of work disability (Kadefors et al. 2019). If disability pension is granted, it can cover up to about 65% of lost income (in those with previous employment).
Data on disability pension (e.g. granting date, grade, and ICD diagnosis) were obtained from the above-mentioned database MiDAS. Virtually, all reimbursements related to disability pension are registered in this database. In the present study, disability pension diagnoses (according to ICD, 10th version) were as follows: musculoskeletal diagnoses, codes M00-M99; psychiatric diagnoses, codes F00-M99; circulatory system diagnoses, codes I00-I99; and respiratory diagnoses, codes J00-J99. All first-time disability pensions were included in the study, i.e., both full and partial.
Covariates
Level of education, marital status, and history of unemployment are considered as indicators of underlying employability problems and were obtained from the above-mentioned LISA register (Ludvigsson et al. 2019). Level of education was classified based on number of years of education: ≤ 9, 10–11, 12, and ≥ 13 years, which largely corresponds to compulsory school, vocational (high) school, upper secondary school, and university-level degree. Marital status was coded as married (or registered partner), unmarried/single, divorced, widow(er). History of unemployment was calculated from the total number of days with benefits during 5 years before the baseline, i.e. 2000–2004, and was divided into (1) no unemployment days, (2) 365 or fewer days of unemployment, and (3) more than 365 days of unemployment.
Job control was classified with a recently developed JEM on decision authority at work (using the same source of survey data as for the physical JEM). Four questions from the survey were used for the classification and measured respondents’ continuous/daily possibilities/opportunity to (1) decide when tasks should be done, (2) control the work pace, (3) take short breaks for talking, and (4) participate in and decide on the organization of own work (Almroth et al. 2021). Like the physical workload variable, a gender-specific index mean value for job control was obtained and linked to study participants through their occupational data. As for physical workload, quintiles of job control were created based on the gender-specific mean values.
Data analysis
Among the 1.834,555 individuals, a minor proportion lacked information on level of education (816) and history of unemployment (221). Individuals with a disability pension before the start of the follow-up were excluded from the analyses.
To characterize the women and men with different degrees of physical workload, we calculated the distribution of covariates across the quintiles of physical workload. We also estimated the crude associations between covariates and all-cause disability pension.
To answer the question of whether and how heavy physical work may increase the rate of disability pension, we used Cox proportional-hazards regression, which estimates hazard ratios (HR). Person-time was calculated from January 1, 2006 up to the date of emigration, early (non-disability) pension, death, disability pension or the end of follow-up on December 31, 2016. Associations with disability pension due to any diagnosis or a musculoskeletal, psychiatric, cardiovascular or respiratory diagnosis were analyzed in crude and covariate-adjusted regression models (i, ii), and separately for women and men; the covariates were (i) level of education, marital status, and history of unemployment and (ii) plus job control. To investigate potential over-adjustment, we also carried out analyses stratified by education level and job control, respectively (both dichotomised).
Granting of disability pension is in most cases preceded by a longer period of sickness absence, and due to this structural relation, sickness absence before baseline was not included as a confounding variable. However, as a sensitivity analysis, we reran our analyses on a population excluding individuals with sickness absence registered at the Swedish Social Insurance Agency between 2001 and 2005.
We also checked whether the above-mentioned reduction in granted disability pensions, which was fully implemented by the year 2010, may have impacted on the associations. In this sensitivity analysis, physical workload was related to disability pensions (any) occurring in 2006–2009 and 2010–2016, respectively.
For calculation of HR attenuations (%) in multivariable-adjusted models, the following formula was used: (crudeHR-adj.HR)/(crudeHR-1)*100. In a previous study (Kjellberg et al. 2016), we found large changes in estimates after adjusting for confounding variables.
Results
A characterization of the women and men with different degrees of occupational physical workload is seen in Table 1. In both genders, low levels of education and days of unemployment before the baseline year are clearly more common among those with higher degrees of physical workload. Marital status, however, differs most in men; those with more physical workload are more often unmarried or divorced at baseline. Lastly, among both women and men, having low job control is much likelier in jobs with higher degrees of physical workload than in jobs with low physical workload.
During the follow-up period, 71,057 (7.5%) women and 41,051 (4.6%) men were granted disability pension. In both genders, lower levels of education and more unemployment are associated with increased hazard of disability pension (Table 2). Furthermore, divorced and widowed women and men as well as unmarried men have an increased hazard of disability pension, compared to married individuals. Additionally, it is seen that low job control is associated with increased hazard of disability pension.
The crude regression models for the women (Table 3, upper part) show that higher physical workload is clearly associated with increased hazard of disability pension (any diagnosis). Furthermore, it is seen that disability pension with a musculoskeletal diagnosis, as expected, increases most in relation to degree of physical workload (HR = 4.38 for those in the category with highest exposure). Hazard of disability pension with a psychiatric diagnosis increases comparatively little while increases in hazard of disability pension with a cardiovascular, and especially a respiratory diagnosis, are clearly seen.
In the models adjusting for differences in education level and unemployment history up to baseline (first adjusted model), it is seen that the hazard ratios for disability pension, all-cause and cause-specific, are attenuated, with the exception of disability pension with a psychiatric diagnosis. A calculation shows that approximately 50–60% of the associations between higher physical workload and disability pension with a musculoskeletal, cardiovascular or respiratory diagnosis remains, and approximately 70% of the association with all-cause disability pension. In the regression models additionally adjusting for differences in job control (second adjusted model), the hazard ratios are further attenuated: the increase in hazard of disability pension with a psychiatric diagnosis disappears; the increase in hazard of disability pension with a cardiovascular diagnosis is reduced by more than half; the increase in hazard of disability pension with a respiratory diagnosis almost by half–as is the increase in hazard of any disability pension. However, the increase in hazard of disability pension with a musculoskeletal diagnosis remains with 80% after this adjustment.
The regression models for the men (Table 4) show roughly the same pattern as for the women: after adjustment for education level and unemployment history up to baseline, the hazard ratios for disability pension with a musculoskeletal diagnosis are highest (crude HR = 8.17 and adjusted HR 5.02 for the category with heaviest workload); the hazard ratios for disability pension with a psychiatric diagnosis are lowest, and the hazard ratios for disability pension with a cardiovascular or a respiratory diagnosis or all-cause disability pension are in between. The attenuation of the hazard ratios was approximately 40–60%, with the exception of < 30% for psychiatric diagnosis. After further adjustment for differences in job control, this pattern remains, but with further attenuated hazard ratios (−50% for all-cause disability pension, −35% for disability pension with a musculoskeletal diagnosis, −100% for disability pension with a psychiatric diagnosis, and −40 to −50% for disability pension with a cardiovascular or respiratory diagnosis). The association with disability pension with a psychiatric diagnosis among men is eliminated after adjustment (−100%), in the same way that was seen among women.
Additional analyses showed that associations within strata of level of education and job control (low and high), respectively, did not differ from the non-stratified associations (results on all-cause disability pension in Tables S2, S3). Furthermore, excluding individuals with registered sickness-absence periods during a few years prior to baseline [160,653 (17.0%) women and 134,129 (15.1%) men] resulted in estimates similar to those seen in the main analysis (results on all-cause disability pension in Table S4). Also, associations with disability pensions occurring in 2006–2009 and 2010–2016, respectively, were similar (results on all-cause disability pension in Table S5).
Discussion
Our analyses showed associations between occupational physical workload and disability pension with musculoskeletal, cardiovascular, and respiratory diagnoses. The association with disability pension with a musculoskeletal diagnosis followed a dose–response pattern and was the strongest of the associations. Associations remained in multivariable-adjusted models, including job control as a covariate. At the same time, we observed that adjusted estimates of the associations were often substantially attenuated as compared with unadjusted estimates. When differences in job control were adjusted for, no association between physical workload and disability pension with a psychiatric diagnosis remained.
Comparison with previous studies
The association between heavy physical workload and disability pension with a musculoskeletal diagnosis has also been demonstrated in previous studies. A few of these studies had the opportunity to compare several different work-environmental factors and found that the risk estimates for physical workload appeared to be particularly high (Karkkainen et al. 2013; Lahelma et al. 2012). Most of the previous studies have been conducted in Finland and all have used a cohort design with several years or sometimes decades of follow-up data on disability pension. Study populations have varied: middle-aged men in Kuopio (Karpansalo et al. 2002), women and men in Helsinki (Ervasti et al. 2019; Lahelma et al. 2012), and Finish twins born in the first half of the twentieth century (Karkkainen et al. 2013). The sets of variables used for confounding control have also differed.
The largest gender-specific study on disability pension with musculoskeletal diagnoses before the present one is Swedish and was done on cohort data from just under 12,000 workers who were followed over a number of years in middle age with regard to disability pension and diagnosis (Kjellberg et al. 2016). For both women and men, the analyses showed a gradual increase in the risk of disability pension with a musculoskeletal diagnosis in relation to higher long-term physical workload. In multivariable models of the associations, childhood socio-economic position, late childhood cognitive ability, level of education, and degree of control at work were used for confounding control.
Associations between heavy physical workload and disability pension with diagnoses other than musculoskeletal have only been investigated in a small number of studies. One of these studies showed an association between heavy physical workload and increased risk of disability pension with a cardiovascular diagnosis (Karpansalo et al. 2002), although with a statistically uncertain risk estimate after multivariable adjustment. Thus, the present study goes further than previous studies by showing that disability pension with a cardiovascular or a respiratory diagnosis increases with higher degrees of physical workload in multivariable-adjusted models, among both women and men. We have not found any other studies that examined physical workload in relation to disability pension with a cardiovascular diagnosis. However, some studies have investigated disability pension with such a diagnosis in relation to psychosocial work-environmental factors, job strain (Mantyniemi et al. 2012) and effort–reward imbalance (Juvani et al. 2014) but did not show any robust associations.
In several of the studies referred to above, both crude and multivariable-adjusted estimates were reported, and we note that attenuation after adjustments was often large. In Karpansalo et al. (2002), the association between heavy physical workload and disability pension with a musculoskeletal diagnosis was greatly attenuated after adjustments for education level, BMI, alcohol consumption, smoking, maximum oxygen uptake and disease diagnoses at baseline and, in Lahelma et al. (2012), adjustment for occupational social class also had a considerable attenuating effect. In Kjellberg et al. (2016), the estimated hazard ratios were significantly smaller in models that adjusted for differences in late childhood cognitive ability, subsequent level of education, and job control, including disability pension with a musculoskeletal diagnosis. Similar effects were shown in the respective studies by Kärkkäinen et al. (2013) and Ropponen et al. (2014) of older twins, which could also adjust for differences in BMI, education, socio-economic position, marital status, and shift work. The present study adds to this by showing that the statistical association between higher physical workload and disability pension is further attenuated or even eliminated (for disability pension with a psychiatric diagnosis) when low job control is added to other covariates.
Interpretation of the results
A decision at the Swedish Social Insurance Agency to grant disability pension is based on an assessment of full or partial long-term reduction of the individual's work ability (forsakringskassan.se 2020b). In turn, work ability is a function of both health and capacity of the individual and of the requirements and conditions in the individual's work, for example the degree of physical workload.
One likely explanation for the association between heavy physical workload and disability pension with a musculoskeletal diagnosis is that high biomechanical loading affects the musculoskeletal system negatively and decreases physical capacity. There is extensive evidence to support this explanation (da Costa and Vieira 2010; Punnett and Wegman 2004). Furthermore, the association with disability pension with a cardiovascular diagnosis may possibly be explained by overload and deleterious effects of prolonged and intense heavy physical work on the cardiovascular system, possibly involving exertion-related elevation of heart rate and blood pressure, and inflammatory processes manifested in arteriosclerosis (Petersen et al. 2012). However, there is a limited number of studies investigating the associations between heavy physical workload and cardiovascular diseases, and the results are inconsistent (Li et al. 2013; Petersen et al. 2012).
Another explanation may be that heavy manual occupations provide less opportunity for adaptations for older workers with physical illness and reduced physical capacity, which should have a bearing on disability pensions with both musculoskeletal, cardiovascular, and respiratory diagnoses. Furthermore, low decision latitude is a risk factor for disability pension even with musculoskeletal diagnoses (Lahelma et al. 2012). Conversely, occupations without physical strain are often non-manual occupations which allow more flexibility for the workers in terms of how and when tasks are to be performed (Johansson and Lundberg 2009). A hindering effect in physically strenuous jobs could give rise to the more general association with poor self-rated health (Burr et al. 2017), long-term sick leave (Andersen et al. 2016; Sommer et al. 2016; Sundstrup et al. 2018), all-cause disability pension (Emberland et al. 2017; Friis et al. 2008; Halonen et al. 2019; Jarvholm et al. 2014; Karpansalo et al. 2002; Labriola et al. 2009; Lahelma et al. 2012; Sommer et al. 2016) and, consequently, loss of work–life expectancy (Schram et al. 2020) demonstrated in previous studies. However, low education and a history of unemployment also seem to contribute to the explanation. We (Falkstedt et al. 2014; Kjellberg et al. 2016) and others (Schram et al. 2019) have shown in previous studies that the large amount of disability pension cases and loss of work–life expectancy among workers with physically heavy occupations may partly be explained by circumstances that relate to this group's weaker position in the labor market. It has also recently been shown on data from 26 European countries that the gap in work participation between workers with and without chronic diseases is substantially larger and increasing over time for workers with short education as compare to higher educational levels (Schram et al. 2019). To some extent, this could be related to limited opportunities for skills development and broadening of competence within manual occupations. Many years in a job that primarily involves routine task execution could lead to employment problems when health or physical capacity decline.
The lack of association with disability pension with a psychiatric diagnosis, after multivariable adjustment, indicates that physical workload does not create significant obstacles to work in the event of mental illness. The slightly higher prevalence of psychiatric disability pensions among women and men with physically heavy occupations seems instead to be explained by the co-occurrence of low job control in these occupations. There are some previous studies (see Knardahl et al. 2017) indicating that the probability of disability pension with a psychiatric diagnosis is increased at lower degrees of control at work.
Strengths and limitations
One of the main strengths of the present study is the much larger size of the study population compared to all other previous studies focusing on a similar research question. This size allowed uniquely clear analyses of associations for disability pension with a cardiovascular or respiratory diagnosis, in women and men separately. The size and comprehensiveness also enabled analyses of the full range of exposure to physical workload in the labor market and, thus, hypothetical dose–response relations. Another strength is the use of JEMs for ranking of individuals within the study population in terms of physical workload and job control. The use of JEMs reduces differential misclassification and spurious risk estimates, which may arise from the use of self-reported data on physical workload and psychosocial factors at work (Fredlund et al. 2000). Initial differences in capacity and health do not affect the differences in physical and psychosocial workloads attributed by JEMs, as can be the case in self-reported data. An additional strength is the ability to account for the co-occurrence of physical workload and low job control.
Of course, using JEMs also has a downside. Through the construction of JEMs, differences in exposure between individuals within different occupations are eliminated, which can result in non-differential misclassification and downward bias of risk estimates. In addition, we know from previous research that questionnaire data on ergonomic factors, on which the JEMs are based, do not have the same precision as measurement and observation data (Teschke et al. 2009), but are the reasonable alternative for larger study populations. However, both recent (Madsen et al. 2018) and older studies (Bosma et al. 1997; Theorell et al. 1998) on physical workload or job-strain factors have found comparable results when using job-exposure matrices and self-reported exposures side by side. Furthermore, the JEMs in our study are indices that consist of mean value calculations based on multiple questionnaire items, which is a commonly used method in the field. An alternative is statistical modeling for the construction of JEMs, which Madsen et al. used recently and that possibly reduces misclassification to some extent. Finally, like these authors, we emphasize that analytical results based on JEM data refer to the occupational level and thus cannot be directly extrapolated to individuals.
We did not have access to data that could measure differences in lifestyle-related risk factors, such as tobacco smoking, physical inactivity, and obesity, and we cannot rule out the possibility of residual confounding. However, the studies that have had access to such information about the study participants have obtained approximately the same results as we did in this study, that is, remaining although attenuated associations. Furthermore, the adjustment for differences in age, education level, marital status, and history of unemployment before baseline should reduce potential confounding from lifestyle-related risk factors in the present study. As in other countries, low levels of education are known to be associated with several such factors (Falkstedt et al. 2016).
The multivariable models also did not include health status at baseline as a covariate. We chose not to adjust for registered sickness absence at baseline, as disability pension among workers is almost always preceded by long-term sickness absence, but the sensitivity analysis excluding individuals with sickness-absence periods in the years up to the baseline of the study gave results similar to those reported in the tables.
In conclusion, this study of the entire Swedish working population aged 44–63 years at baseline and followed for up to 11 years (censored at age 65) showed that, among both women and men, a higher degree of occupational physical workload is associated with a higher rate of disability pension with a musculoskeletal, cardiovascular or respiratory diagnosis. These associations, shown in multivariable-adjusted models, may reflect mechanisms reducing the chances of continued labor-force participation among older workers. An increased rate of disability pension with a psychiatric diagnosis was explained by confounding variables, including low job control.
References
Almroth M, Hemmingsson T, Sorberg Wallin A, Kjellberg K, Burstrom B, Falkstedt D (2021) Psychosocial working conditions and the risk of diagnosed depression: a Swedish register-based study. Psychol Med. https://doi.org/10.1017/S003329172100060X
Andersen LL, Fallentin N, Thorsen SV, Holtermann A (2016) Physical workload and risk of long-term sickness absence in the general working population and among blue-collar workers: prospective cohort study with register follow-up. Occup Environ Med 73:246–253. https://doi.org/10.1136/oemed-2015-103314
Andersen LL, Jensen PH, Sundstrup E (2019) Barriers and opportunities for prolonging working life across different occupational groups: the SeniorWorkingLife study. Eur J Public Health. https://doi.org/10.1093/eurpub/ckz146
Badarin K, Hemmingsson T, Hillert L, Kjellberg K (2021) Physical workload and increased frequency of musculoskeletal pain: a cohort study of employed men and women with baseline occasional pain. Occup Environ Med. https://doi.org/10.1136/oemed-2020-107094
Bosma H, Marmot MG, Hemingway H, Nicholson AC, Brunner E, Stansfeld SA (1997) Low job control and risk of coronary heart disease in Whitehall II (prospective cohort) study. BMJ 314:558–565. https://doi.org/10.1136/bmj.314.7080.558
Burr H, Pohrt A, Rugulies R, Holtermann A, Hasselhorn HM (2017) Does age modify the association between physical work demands and deterioration of self-rated general health? Scand J Work Environ Health 43:241–249. https://doi.org/10.5271/sjweh.3625
da Costa BR, Vieira ER (2010) Risk factors for work-related musculoskeletal disorders: a systematic review of recent longitudinal studies. Am J Ind Med 53:285–323. https://doi.org/10.1002/ajim.20750
Emberland JS, Nielsen MB, Knardahl S (2017) Psychological, social, and mechanical work exposures and disability retirement: a prospective registry study. BMC Public Health 17:56. https://doi.org/10.1186/s12889-016-3921-0
Ervasti J, Pietilainen O, Rahkonen O, Lahelma E, Kouvonen A, Lallukka T, Manty M (2019) Long-term exposure to heavy physical work, disability pension due to musculoskeletal disorders and all-cause mortality: 20-year follow-up-introducing Helsinki Health Study job exposure matrix. Int Arch Occup Environ Health 92:337–345. https://doi.org/10.1007/s00420-018-1393-5
Eurofound (2015) Sustainable work over the life course: concept paper. Publications Office of the European Union, Luxembourg, Luxembourg
Falkstedt D, Backhans M, Lundin A, Allebeck P, Hemmingsson T (2014) Do working conditions explain the increased risks of disability pension among men and women with low education? A follow-up of Swedish cohorts. Scand J Work Environ Health 40:483–492. https://doi.org/10.5271/sjweh.3441
Falkstedt D, Moller J, Zeebari Z, Engstrom K (2016) Prevalence, co-occurrence, and clustering of health-risk behaviors among people with different socio-economic trajectories: a population-based study. Prev Med 93:64–69. https://doi.org/10.1016/j.ypmed.2016.09.017
forsakringskassan.se (2020a) MiDAS. The Swedish Social Insurance Agency. https://www.forsakringskassan.se/. Accessed Nov 12 2020
forsakringskassan.se (2020b) Sickness compensation. The Swedish Social Insurance Agency. https://www.forsakringskassan.se/. Accessed Nov 12 2020
Fredlund P, Hallqvist J, Diderichsen F (2000). Psykosocial yrkesexponeringsmatris: En uppdatering av ett klassifikationssystem för yrkesrelaterade psykosociala exponeringar [Psychosocial job exposure matrix: An update of a classification system for work-related psychosocial exposures]. In Arbete och Hälsa (Report No. 11). Stockholm: Arbetslivsinstitutet
Friis K, Ekholm O, Hundrup YA (2008) The relationship between lifestyle, working environment, socio-demographic factors and expulsion from the labour market due to disability pension among nurses. Scand J Caring Sci 22:241–248. https://doi.org/10.1111/j.1471-6712.2007.00521.x
Halonen JI et al (2019) Physical working conditions and subsequent disability retirement due to any cause, mental disorders and musculoskeletal diseases: does the risk vary by common mental disorders? Soc Psychiatry Psychiatr Epidemiol. https://doi.org/10.1007/s00127-019-01823-6
Jarvholm B, Stattin M, Robroek SJW, Janlert U, Karlsson B, Burdorf A (2014) Heavy work and disability pension: a long term follow-up of Swedish construction workers. Scand J Work Environ Health 40:335–342. https://doi.org/10.5271/sjweh.3413
Johansson G, Lundberg I (2009) Components of the illness flexibility model as explanations of socioeconomic differences in sickness absence. Int J Health Serv 39:123–138. https://doi.org/10.2190/HS.39.1.f
Juvani A, Oksanen T, Salo P, Virtanen M, Kivimaki M, Pentti J, Vahtera J (2014) Effort-reward imbalance as a risk factor for disability pension: the Finnish Public Sector Study. Scand J Work Environ Health 40:266–277. https://doi.org/10.5271/sjweh.3402
Kadefors R, Nilsson K, Ostergren PO, Rylander L, Albin M (2019) Social inequality in working life expectancy in Sweden. Z Gerontol Geriatr 52:52–61. https://doi.org/10.1007/s00391-018-01474-3
Karkkainen S et al (2013) Disability pension due to musculoskeletal diagnoses: importance of work-related factors in a prospective cohort study of Finnish twins. Scand J Work Env Health 39:343–350. https://doi.org/10.5271/sjweh.3345
Karpansalo M, Manninen P, Lakka TA, Kauhanen J, Rauramaa R, Salonen JT (2002) Physical workload and risk of early retirement: prospective population-based study among middle-aged men. J Occup Environ Med 44:930–939. https://doi.org/10.1097/00043764-200210000-00012
Kjellberg K, Lundin A, Falkstedt D, Allebeck P, Hemmingsson T (2016) Long-term physical workload in middle age and disability pension in men and women: a follow-up study of Swedish cohorts. Int Arch Occup Env Hea 89:1239–1250. https://doi.org/10.1007/s00420-016-1156-0
Knardahl S, Johannessen HA, Sterud T, Harma M, Rugulies R, Seitsamo J, Borg V (2017) The contribution from psychological, social, and organizational work factors to risk of disability retirement: a systematic review with meta-analyses. BMC Public Health 17:176. https://doi.org/10.1186/s12889-017-4059-4
Labriola M, Feveile H, Christensen KB, Stroyer J, Lund T (2009) The impact of ergonomic work environment exposures on the risk of disability pension: prospective results from DWECS/DREAM. Ergonomics 52:1419–1422. https://doi.org/10.1080/00140130903067771
Lahelma E et al (2012) Working conditions as risk factors for disability retirement: a longitudinal register linkage study. BMC Public Health 12:Artn 309. https://doi.org/10.1186/1471-2458-12-309
Li J, Loerbroks A, Angerer P (2013) Physical activity and risk of cardiovascular disease: what does the new epidemiological evidence show? Curr Opin Cardiol 28:575–583. https://doi.org/10.1097/HCO.0b013e328364289c
Ludvigsson JF et al (2016) Registers of the Swedish total population and their use in medical research. Eur J Epidemiol 31:125–136. https://doi.org/10.1007/s10654-016-0117-y
Ludvigsson JF, Svedberg P, Olen O, Bruze G, Neovius M (2019) The longitudinal integrated database for health insurance and labour market studies (LISA) and its use in medical research. Eur J Epidemiol 34:423–437. https://doi.org/10.1007/s10654-019-00511-8
Madsen IEH et al (2018) Physical work demands and psychosocial working conditions as predictors of musculoskeletal pain: a cohort study comparing self-reported and job exposure matrix measurements. Occup Environ Med 75:752–758. https://doi.org/10.1136/oemed-2018-105151
Mantyniemi A et al (2012) Job strain and the risk of disability pension due to musculoskeletal disorders, depression or coronary heart disease: a prospective cohort study of 69 842 employees. Occup Environ Med 69:574–581. https://doi.org/10.1136/oemed-2011-100411
Petersen CB, Eriksen L, Tolstrup JS, Sogaard K, Gronbaek M, Holtermann A (2012) Occupational heavy lifting and risk of ischemic heart disease and all-cause mortality. BMC Public Health 12:1070. https://doi.org/10.1186/1471-2458-12-1070
Piha K, Laaksonen M, Martikainen P, Rahkonen O, Lahelma E (2013) Socio-economic and occupational determinants of work injury absence. Eur J Pub Health 23:693–698. https://doi.org/10.1093/eurpub/cks162
Prakash KC et al (2017) Work-related biomechanical exposure and job strain in midlife separately and jointly predict disability after 28 years: a Finnish longitudinal study. Scand J Work Environ Health 43:405–414. https://doi.org/10.5271/sjweh.3656
Punnett L, Wegman DH (2004) Work-related musculoskeletal disorders: the epidemiologic evidence and the debate. J Electromyogr Kines 14:13–23. https://doi.org/10.1016/j.jelekin.2003.09.015
Ropponen A, Samuelsson A, Alexanderson K, Svedberg P (2013) Register-based data of psychosocial working conditions and occupational groups as predictors of disability pension due to musculoskeletal diagnoses: a prospective cohort study of 24,543 Swedish twins. BMC Musculoskelet Disord 14:268. https://doi.org/10.1186/1471-2474-14-268
Ropponen A, Svedberg P, Koskenvuo M, Silventoinen K, Kaprio J (2014) Physical work load and psychological stress of daily activities as predictors of disability pension due to musculoskeletal disorders. Scand J Public Health 42:370–376. https://doi.org/10.1177/1403494814525005
Samuelsson A, Ropponen A, Alexanderson K, Svedberg P (2013) Psychosocial working conditions, occupational groups, and risk of disability pension due to mental diagnoses: a cohort study of 43 000 Swedish twins. Scand J Work Env Health 39:351–360. https://doi.org/10.5271/sjweh.3338
Schram JLD, Schuring M, Oude Hengel KM, Burdorf A (2019) Health-related educational inequalities in paid employment across 26 European countries in 2005–2014: repeated cross-sectional study. BMJ Open 9:e024823. https://doi.org/10.1136/bmjopen-2018-024823
Schram JL, Solovieva S, Leinonen T, Viikari-Juntura E, Burdorf A, Robroek SJ (2020) The influence of occupational class and physical workload on working life expectancy among older employees. Scand J Work Environ Health. https://doi.org/10.5271/sjweh.3919
Sommer TG, Svendsen SW, Frost P (2016) Sickness absence and permanent work disability in relation to upper- and lower-body pain and occupational mechanical and psychosocial exposures. Scand J Work Environ Health 42:481–489. https://doi.org/10.5271/sjweh.3600
Stattin M, Jarvholm B (2005) Occupation, work environment, and disability pension: a prospective study of construction workers. Scand J Public Health 33:84–90. https://doi.org/10.1080/14034940410019208
Sundstrup E et al (2018) Retrospectively assessed physical work environment during working life and risk of sickness absence and labour market exit among older workers. Occup Environ Med 75:114–123. https://doi.org/10.1136/oemed-2016-104279
Teschke K, Trask C, Johnson P, Chow Y, Village J, Koehoorn M (2009) Measuring posture for epidemiology: Comparing inclinometry, observations and self-reports. Ergonomics 52:1067–1078. https://doi.org/10.1080/00140130902912811
Theorell T et al (1998) Decision latitude, job strain, and myocardial infarction: a study of working men in Stockholm. Am J Public Health 88:382–388. https://doi.org/10.2105/Ajph.88.3.382
Acknowledgements
The study was funded by the Swedish Council for Working Life and Social Research (Project No 2016-07185).
Funding
Open access funding provided by Karolinska Institute.
Author information
Authors and Affiliations
Contributions
Falkstedt, Kjellberg and Hemmingsson conceived the study and designed the analyses together with Andersson. Falkstedt analyzed the data and wrote the paper. All authors contributed to the interpretations of the results and to the manuscript writing.
Corresponding author
Ethics declarations
Conflict of interest
The authors have no relevant financial or non-financial interests to disclose.
Ethical approval
The Regional Ethics Review Board in Stockholm, Sweden, has approved the research (protocol no. 2017/1224-31 and no. 2018/1675-32). Due to the character of the data base and Statistics Sweden’s anonymization of all data, the Review Board waived the normal requirement for written consent.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Falkstedt, D., Hemmingsson, T., Albin, M. et al. Disability pensions related to heavy physical workload: a cohort study of middle-aged and older workers in Sweden. Int Arch Occup Environ Health 94, 1851–1861 (2021). https://doi.org/10.1007/s00420-021-01697-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00420-021-01697-9