
Abstract
Background
The neovascular form of age-related macular degeneration (AMD) manifested with choroidal neovascularization (CNV) is one of the leading causes of rapid and irreversible visual loss. Recent reports suggest that bone marrow-derived stem/progenitor cells (SPCs) play a crucial role in the development and progression of the disease. The purpose of this study was to investigate whether or not undifferentiated non-haematopoietic stem cells, including those capable of differentiating into neural phenotypes, play a role in the pathological state of CNV formation.
Methods
Peripheral blood samples were collected from 46 patients diagnosed with CNV and from 46 controls. The CXCR4+Lin-CD45- stem cells were counted and analysed by flow cytometry. Using qRT-PCR and immunocytofluorescence, the expression of early neural and glial cell markers (β-III-tubulin, nestin, and glial fibrillary acidic protein) in the sorted cells was analysed, and correlated with plasma concentrations of stromal cell-derived factor 1 (SDF-1) (enzyme-linked immunosorbent assay), which is a pivotal chemokine that regulates the trafficking of SPCs.
Results
We found that the number of circulating CXCR4+Lin-CD45- cells did not differ in patients with active CNV as compared to the controls. However, we noticed significant intracellular overexpression of β-III-tubulin in the cells derived from AMD patients. Moreover, we observed significantly lower SDF-1 plasma levels in neovascular AMD patients compared to healthy individuals.
Conclusions
Our findings suggest that neural progenitor cells, together with low SDF-1 concentrations, may play a considerable role in the process of AMD progression. Further investigations aimed at the precise elucidation of these issues may help with the future development of effective prevention against, and the treatment of, this disease.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Age-related macular degeneration (AMD) is one of the leading causes of irreversible visual loss in people 65 years of age and older in the western world [1]. It represents a degenerative and progressive condition involving the retinal pigment epithelium (RPE), Bruch’s membrane and the choriocapillaries. The neovascular form of the disease is characterized by the invasion of new pathological vessels under the macula (choroidal neovascularization, CNV), and it is associated with a rapid and severe loss of vision [2]. Despite the fact that our understanding of molecular events presaging AMD has grown in the last decade, the pathogenesis of AMD is still not entirely clear [3].
Recent research strongly suggests that bone marrow-derived stem/progenitor cells may play an important role in the development and progression of the disease [4]. During the last decade, a growing body of evidence has suggested that bone marrow contains undifferentiated non-haematopoietic tissue-committed stem cells (TCSCs), which include cells capable of differentiating into neural phenotypes, for example neurons, astroglia and oligodendroglia. These stem/progenitor cells (SPCs) circulate in the peripheral blood, therefore maintaining a pool in distant tissues and playing a role in tissue regeneration. The trafficking of these cells is regulated by various chemokines and their receptors, including the pivotal stromal cell-derived factor 1 (SDF-1)-CXCR4 axis [5]. The secretion of SDF-1 increases during tissue damage, such as during ischaemia, toxic damage or total body irradiation, and the SDF-1 secreted during local tissue injury may play a role in chemoattracting the TCSCs necessary for organ/tissue renewal [6].
However, the precise subpopulation of cells that is the source of neural and glial TCSCs remains unidentified. A substantial level of diversity has been reported with regard to the identity of these cells. Most studies have indicated heterogeneous or poorly characterized populations of cells [7]. Although some of the cell candidates were defined according to their classification as non-haematopoietic stem cells, there are no standardized criteria with which to determine their phenotype. To date, it has been common to isolate and characterize non-HSCs stem cells by their lack of CD45 expression and their lineage antigens [8].
Up until now, no study has actually examined the concentrations of circulating TCSCs in the peripheral blood of AMD patients. In order to investigate whether or not SPCs play a role in the pathological state of CNV formation, we examined circulating CXCR4+Lin-CD45- cells from patients with exudative AMD and healthy controls, and analysed the expression of early neural and glial cell markers. Additionally, we correlated our findings with SDF-1 plasma levels and clinical data, including any accompanying vascular disorders. We found that the number of circulating CXCR4+Lin-CD45- cells did not differ in patients with active CNV. However, the cells derived from AMD patients significantly overexpressed β-III-tubulin. To the best of our knowledge, this is the first study on circulating non-haematopoietic TCSCs in individuals with AMD.
Materials and methods
Characteristics and selection of the study groups
Participants were recruited from the outpatient population of the Department of Ophthalmology of Pomeranian Medical University in Szczecin, Poland. All of the enrolled subjects underwent a complete ophthalmic examination, i.e., visual acuity and intraocular pressure measurements and dilated fundus examination using slit-lamp biomicroscopy. Forty-six subjects with a clinical diagnosis of exudative AMD, with newly diagnosed CNV characterized by serous or haemorrhagic retinal pigment epithelium detachment, subretinal neovascular membrane, subretinal haemorrhage, or fibrous scar, were included in the study. The severity of AMD, based on the size and laterality of the lesions, was characterized by fluorescein angiography and by optical coherence tomography imaging. Patients who had previously been submitted for laser or intravitreal treatment were excluded from the study. In the case of different stages of the disease being diagnosed in each eye, the subject was categorized according to the severity of changes in the worse eye. Forty-six age- and sex-matched volunteers without AMD (defined as the absence of drusen, pigmentary abnormalities or neovascularization) were enrolled as the control group.
Data regarding medical history and smoking status were collected, with special attention being paid to arterial hypertension and pre-existing cardiovascular and cerebrovascular conditions.
Exclusion criteria included significant chronic systemic conditions, for example collagen or neoplastic disease, diabetes mellitus, renal failure, hepatic dysfunction and any evidence of retinal disease, with the exception of AMD (in AMD groups), i.e., glaucoma, intraocular inflammatory diseases, and recent (within 3 months) ocular surgery.
The study adhered to the tenets of the Declaration of Helsinki, and approval was obtained from the Local Research Ethics Committee. Moreover, each patient gave written informed consent for his or her involvement.
Sample collection
Venous blood samples (~7.5 ml) collected in EDTA tubes were centrifuged (2000 rpm, 4°C, 10 min) and the plasma was stored at −20°C to −80°C until assayed. The red blood cells were lysed using BD Pharm Lyse lysing buffer (BD Biosciencies, San Jose, CA, USA) for 15 min at room temperature to isolate peripheral blood nuclear cells (PBNCs).
Flow cytometry
Two million (2 × 106) PBNCs were stained with monoclonal antibodies for lineage markers (CD56, CD235a, CD3, CD66b, CD24, CD19, CD14, CD16, CD2) conjugated with fluorescein isothiocyanate (FITC), CD45 conjugated with phycoerythrin (PE), and CXCR4 conjugated with allophycocyanin (APC) (BD Biosciences, San Jose, CA, USA) (Fig. 2). In the control experiment the cells were stained with secondary isotypic antibodies: IgM, IgG1, IgG2a-FITC, IgG1-PE and IgG1-APC for the lineage antigens CD45 and CXCR4. The samples were incubated with antibodies at room temperature for 30 min, then washed and suspended in 1% formaldehyde. Flow analysis was performed on an LSR II instrument (BD Biosciences, San Jose, CA, USA). At least 105 events were acquired and analysed using Cell Quest software (BD Biosciences, San Jose, CA, USA). The number of cells in each population was expressed as a percentage of the total events.
Isolation and immunofluorescence of peripheral blood-derived SPCs
The population of CXCR4+Lin-CD45- cells was sorted by multiparameter, live sterile cell sorting (BD FACSAriaIIu Cell-Sorting System, BD Biosciences, San Jose, CA, USA). Cell staining for all of the antigens was performed as previously described. The sorted cells were permeabilized (0.1% Triton X-100, 10 min) and stained for β-III-tubulin (OriGene Technologies, Rockville, MD, USA), nestin (Novus Biologicals, Littleton, CO, USA) and glial fibrillary acidic protein (GFAP) (Santa Cruz Biotechnology, Santa Cruz, CA, USA) antigens with anti-human monoclonal antibodies for 1 h at room temperature followed by incubation with a secondary antibody conjugated to FITC (Sigma, St. Louis, MO, USA). The cells were subsequently fixed (3.7% paraformaldehyde) and the nuclei were stained with DAPI (Invitrogen, Paisley, UK). Isotype control antibody (APC-conjugated) staining was performed analogously to check if any unspecific antibody binding occured. For the same reason, the cells were stained solely with anti-rabbit secondary antibody (FITC-conjugated), omitting the primary antibody.The BD Biosciences Pathway 855 bioimager (BD Biosciences, Rockville, MD, USA) was used for fluorescence images.
Real-time reverse transcriptase-polymerase chain reaction (qRT-PCR)
Total mRNA was isolated from PBNCs (2 × 106) using an RNeasy Mini Kit (Qiagen GmbH, Hilden, Germany). The RNA was reverse-transcribed with Moloney murine leukaemia virus reverse transcriptase and oligo dt primers (Fermentas International Inc., Burlington, Canada). Quantitative assessment of the mRNA levels for early neural and glial cell markers was performed by real-time RT-PCR on a Bio-Rad CFX96 Real-Time PCR Detection System (Bio-Rad Inc., Philadelphia, PA, USA). A 25-μl reaction mixture contained 12.5 μl of iQ SYBER Green Supermix reagent, 10 ng of cDNA template, and one of each of the primer pairs: 5′-ACA CCT GTG CCA GCC TTT CTT-3′ (forward) and 5′-TGA ACA CTC TAG ACC CAC CG-3′ (reverse) primers for nestin; 5′-GTG GGC AGG TGG GAG CTT GA-3′ (forward) and 5′-CTG GGG CGG CCT GGT ATG AC-3′ (reverse) primers for GFAP; 5′-CGA GTC GCC CAC GTA GTT G-3′ (forward) and 5′-TTC TGG GAA GTC ATC AGT GAT-3′ (reverse) primers for β-III-tubulin and 5’-AAT GCG GCA TCT TCA AAC CT-3’ (forward) and 5’-TGA CTT TGT CAC AGC CCA AGA TA-3’ (reverse) primers for beta-2 microglobulin (BMG), designed using Primer Express software (Applied Biosystems, Foster City, CA, USA). The real-time cycling conditions were: 1 cycle at 95°C for 10 min, followed by 40 cycles at 95°C for 15 s, 60°C for 1 min, and 72°C for 15 s. Relative quantification of mRNA expression was performed using the comparative Ct method. The relative quantization value of the target, normalized to an endogenous control BMG (housekeeping) gene and relative to a calibrator, was expressed as 2ΔCt, where ΔCt = [Ct of the endogenous control gene (BMG)] - [Ct of the target gene].
ELISA
Plasma concentrations of stromal derived factor-1 alpha (SDF-1α) were measured using commercially available enzyme-linked immunosorbent assay (ELISA) Quantikine kits (R&D Systems, Minneapolis, MN, USA) according to the manufacturer’s protocol. Calibration was performed with recombinant human SDF-1α in the concentration range 156 to 10,000 pg/ml. Absorbance was read at 450 nm using an ELX 808IU automated Microplate Reader (Bio-Tek Instruments Inc). The results were analysed using a quadratic or 4PL algorithm curve fit. The limit of detection was 18 pg/ml. Intra-assay precision (CV%) was 3.4–3.9%, while inter-assay precision was 8.2–13.4%.
Statistics
Quantitative variables were compared between groups with the Mann–Whitney test. Fisher’s exact test was used for nominal variables. Correlations between quantitative variables were measured with Spearman’s rank correlation coefficient. Multivariate analyses were performed using General Linear Model (GLM); variables with non-normal distributions (Shapiro–Wilk test) were transformed logarithmically for this analysis. Results with p < 0.05 were considered statistically significant.
Results
Characteristics of study subjects
The characteristics of the patients and controls are summarized in Table 1. The AMD and control groups were matched for age, gender, and selected well-known AMD risk factors, including hypertension, history of ischaemic heart disease and stroke. The rate of past smokers was slightly higher in the AMD group than in the control group (p = 0.054). However, no difference was found between current smokers in the AMD and control groups. Moreover, in the AMD group, a positive association between patient age and lesion diameter, as well as patient age and bilateral CNV, was noted. This means that patients who manifested bilateral CNV and a larger diameter of the macular lesion were significantly older compared to those with unilateral changes (median: 79 vs 72 years; p = 0.020) and to those with a smaller CNV area (median: 76 vs 69 years; p = 0.014), respectively.
Enumeration of CXCR4+Lin-CD45- cells in peripheral blood of AMD patients and controls
Next, we focused on evaluating the number of CXCR4+Lin-CD45- cells in the peripheral blood (Fig. 1). We did not observe any significant difference in the number of cells analysed between AMD and control groups (median: 0.0059% and 0.0071%, respectively, p = 0.51) The results obtained suggest that age-related macular degeneration is not an independent factor triggering the mobilization of SPCs from the bone marrow.

Strategy for analysing CXCR4+Lin–CD45- stem/progenitor cells based on their size and antigen profile. a Cell distribution based on the FSC (forward scatter) and SSC (side scatter) parameters that describe their size and granularity, respectively. b Analysis of cells according to their lineage markers and CXCR4 expression. The cells enclosed in the P2 region were further analysed based on their CD45 antigen expression (c). d Presentation of the percentages of CXCR4+Lin–CD45-stem cells circulating in the peripheral blood of AMD patients and the control group. The values are expressed as percentages of the total peripheral blood nuclear cells. Q1–Q3 — upper and lower quartiles
Interestingly, in the control group, we noted a strong negative correlation between patient age and the number of cells analysed in peripheral blood (Rs = −0.38, p = 0.0096). This implies that a noticeably larger amount of SPCs was observed in younger individuals. The results obtained corroborate the previous observations, indicating that younger individuals display a higher regenerative potential. Moreover, in the AMD group, a greater number of CXCR4+Lin-CD45- cells was observed in males (median: 0.0097% vs 0.0044%, p = 0.019).
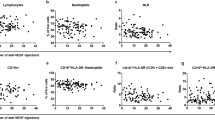
Since there are available data suggesting that AMD is associated with underlying systemic vascular disease [9], we assessed the impact of the abovementioned coincidence on SPC mobilisation into peripheral blood. We noted that those patients with concurrent vascular diseases had a significant reduction in CXCR4+Lin–CD45- cells. In patients with AMD and concomitant ischaemic heart disease, or history of stroke, a lower percentage of SPCs analysed in peripheral blood was found than in those without accompanying vascular disorders (Table 2). A similar tendency was observed in the control group. Furthermore, a decrease in the numbers of CXCR4+Lin–CD45- cells was observed in hypertensive individuals in the control group. The number of SPCs analysed in blood seemed to be unaffected either by the size and laterality of the disease or by the smoking status of the patients.
The expression of neuroprogenitor and glial cell markers in SPCs
In order to obtain detailed characteristics of peripheral blood SPCs, we analysed them for the presence of early neural and glial cell markers. Accordingly, the CXCR4+Lin–CD45- cell population sorted from among the PB cells was labelled with antibodies directed against nestin, GFAP and β-III-tubulin. Figure 2 shows the results of the microscope analysis of the isolated cell populations. A clearly evident expression of the three antigens analysed in the cytoplasm of CXCR4+Lin–CD45- corroborate the presence of early neural progenitors in the peripheral blood of AMD patients.

Identification of CXCR4+Lin–CD45- TCSCs derived from the peripheral blood of AMD patients. The individual images depict the expression of CXCR4 and β-III-tubulin (a), GFAP (b) and nestin (c) antigens in isolated CXCR4+Lin–CD45-cells. The nuclei were visualized via DAPI staining. A pseudocolour was assigned to each stain as follows: anti-CXCR4 – red, anti-nestin, β-III-tubulin and GFAP – green, nuclei – blue. The control images (the upper boxed insets) confirm no unspecific binding of antibodies. The scale bar shows 5 μm. Representative data are shown
Next, we performed a quantitative analysis of the expression of the abovementioned markers in PB cells by qRT-PCR (Table 3). The expression of β-III-tubulin was significantly higher in the AMD group compared to healthy volunteers (p = 0.0074). The difference remained significant in the multivariate analysis performed in the General Linear Model after adjustment for age, gender, smoking status, presence of ischaemic heart disease and hypertension (ß = +0.29; p = 0.029). However, no differences were observed in the expression of nestin or GFAP between the AMD and control groups. This may indicate that the advanced stage of the disease (i.e., neovascular AMD) is accompanied by the mobilization of more differentiated neural progenitors with high β-III-tubulin expression.
Subsequent correlation analysis of the neuroprogenitor and glial cell markers showed positive correlations between the expressions of these antigens. In both of the groups investigated, a positive correlation was observed between the mRNA expression of GFAP and β-III-tubulin (Rs = +0.33, p = 0.033 in the control group, and Rs = +0.65, p < 0.001 in AMD patients), as well as between nestin and β-III-tubulin (Rs = +0.35; p = 0.048 in the control group, and Rs = +0.56; p = 0.016 in the AMD group). Moreover, such a relationship was also revealed between the expression of GFAP and nestin in the AMD group (Rs = +0.70; p < 0.001). Therefore, this may indicate that the genes/proteins analysed are basically present in a relatively homogeneous cell population (Table 4).
Subsequently, we assessed the effect of underlying vascular diseases on the expression of nestin, GFAP, and β-III-tubulin in PB cells. In the AMD patients, we observed a higher expression of GFAP in subgroups with ischaemic heart disease or a history of stroke compared to those without these concomitant diseases (medians: 27.6 vs 9.8; p = 0.0013). Likewise, the expression of β-III-tubulin was also found to be higher in these patients, although the difference was at borderline significance (medians: 0.152 for atherosclerotic individuals vs 0.093 for non-atherosclerotic individuals; p = 0.066). Furthermore, in the control group the expression of GFAP proved to be noticeably higher in atherosclerotic individuals (medians: 27.3 vs 10.3; p = 0.020). Analogous associations were revealed regarding hypertension. In the control group, the expression of GFAP was higher in hypertensive individuals (medians: 14.6 vs 4.1; p = 0.051). Similarly, in the AMD group, a higher expression of nestin was observed in patients with hypertension, although the difference had borderline significance (medians: 14.53 vs 4.42; p = 0.064). Expression of the neuroprogenitor and glial cell markers analysed was unaffected by size or laterality of CNV, as well as by the smoking status of the patients.
Furthermore, in our study, in order to characterize the cells more accurately, we evaluated the association between the number of circulating non-HSCs and the expression of the markers analysed at the mRNA level. Remarkably, we noticed a negative correlation between the number of CXCR4+Lin–CD45- cells in peripheral blood and the intracellular expression of all of the markers analysed in AMD patients (Rs = −0.54; p = 0.0083 for GFAP; Rs = −0.61; p = 0.0043 for β-III-tubulin; Rs = −0.67; p = 0.0013 for nestin). This may suggest that the impairment of CXCR4+Lin–CD45- cell mobilization to the peripheral blood is accompanied by their relative enrichment in neural and glial cell progenitors.
Plasma SDF-1 levels in AMD patients and controls
The SDF-1 plasma level was found to be evidently lower in patients with AMD compared to the control group (p = 0.0031) (Fig. .3). Multivariate analysis of patients and controls, adjusted for age, gender and smoking status (past or present), as well as the presence of ischaemic heart disease and hypertension, revealed that AMD was an independent factor associated with lower SDF-1 plasma concentrations (ß = −0.32; p = 0.0012). Moreover, in the control group (but not the AMD group), we found that the plasma SDF-1 level was higher in subjects with hypertension (median 2860 vs 2032 pg/ml, p = 0.0004) and individuals with ischaemic heart disease or a history of stroke (median: 3162 vs 2122 pg/ml, p = 0.0005) than in control participants with no history of these diseases. Additionally, in control individuals, a strong negative correlation was observed between the number of CXCR4+Lin–CD45- cells and the SDF-1 plasma level (Rs = −0.52, p = 0.0003). Similarly, we noted a negative correlation between SDF-1 concentration and the intracellular expression of β-III-tubulin in AMD patients (Rs = −0.44, p = 0.039). The negative correlation between SDF-1 concentration and the intracellular expression of nestin in controls had borderline significance (Rs = −0.30; p = 0.10).

Plasma concentrations of SDF-1 in AMD patients and in the control group. The values are expressed in pg/ml. Q1–Q3 — upper and lower quartiles
Discussion
Age-related macular degeneration is caused by a series of metabolic and histological changes in the retina and underlying tissues, which culminate in progressive retinal atrophy and, in the most severe form, neovascularisation. Abnormal blood vessel growth begins in the vascular choroid, which gradually invades the outer retina, and the accompanying leak of blood and fluid secondarily damage the photoreceptor cells [2].
Attempts at retinal self-regeneration in the course of AMD could be considered possible based on reports indicating the role of bone-marrow-derived SPCs in this process [10]. Bone marrow is considered to be the richest reservoir of versatile stem/progenitor cells, maintaining constant haematopoiesis and supporting the homeostasis of other tissues. Accumulating evidence indicates that in addition to haematopoietic stem cells, different types of non-haematopoietic TCSCs reside in the BM and possess the potential to differentiate into a variety of mature cells, including those with neural and retinal characteristics [11–13]. Apart from cellular differentiation into the target tissue type, the beneficial effect of SPCs can be achieved via other ways, e.g., antiapoptotic signalling or paracrine cross-talk. Furthermore, as reported recently, SPCs are able to modulate local inflammatory processes [14].
Since early non-HSCs may actually represent diverse cell populations and cannot be purely defined based on their phenotype, we focused on the cells expressing CXCR4 (a receptor for SDF-1 alpha-chemokine) that are lineage-negative as well as CD45-negative (non-haematopoietic). The phenotype of the analysed CXCR4+Lin–CD45- cells corresponds to some extent to very small embryonic-like SCs (VSEL-SCs) that express pluripotent SC markers, as recently described in human umbilical cord and peripheral blood, with a contribution by our research team [15]. The phenotype of VSEL-SCs is characterized by the expression of surface CXCR4, CD133, and/or CD34 antigens, as well as by nuclear embryonic Oct-4 and Nanog markers. In addition, VSEL-SCs are also lineage- and CD45-negative [16]. Hence, the population of CXCR4+Lin–CD45- cells that was analysed contained a “cocktail” of diverse early SPCs enriched with neural progenitors.
In this study, we performed a quantitative and qualitative characterization of circulating CXCR4+Lin–CD45- cells in patients with the neovascular form of AMD. We found no significant differences between the concentrations of the cells analysed in the AMD and healthy control groups, which indicates that the analysed cell population did not undergo a noticeable mobilization into PB during the course of AMD. Several studies have shown atherosclerotic diseases to be a risk factor preceding AMD [17]. Moreover, there is a great body of evidence that AMD occurs mutually with vascular disorders or may independently predict stroke or coronary heart disease [18, 19]. Interestingly, the circulating CXCR4+Lin–CD45- cell concentration significantly decreased in hypertensive patients and in individuals with a history of cardiovascular disease or stroke. The diminished CXCR4+Lin–CD45- cell numbers in these patients might well have resulted from a gradual collapse of the supply of this cell population during the course of chronic vascular impairment. In support of this notion, reduced levels of circulating CXCR4-positive cells have previously been reported in diabetes and cardiovascular disease, as well as in cardiac transplant recipients [20–22]. In addition, recently published reports indicated that the number of circulating SPCs steadily decreases with the increasing age of individuals [23]. Our findings correspond with the abovementioned observations, as we revealed a strong negative correlation between PB CXCR4+Lin–CD45- cell concentrations and the patient’s age within the healthy control group. However, the possibility that the reduced concentrations of these analysed cells in individuals with concomitant hypertension and/or atherosclerosis could be attributed to the recruitment of these cells from the PB and reattachment to the site of injury (i.e., the ischaemic tissue) cannot be excluded. Also, it is possible that CXCR4+Lin–CD45- cell depletion in the PB may have resulted from their excessive utilization in the ongoing repair of continuously damaged tissues. This is an attractive hypothesis that considers the possibility that CXCR4-positive cells may attach locally or be recruited distally to the sites of injury. Interestingly, the general reduction of CXCR4+Lin–CD45- cells detected in patients with concomitant hypertension and atherosclerosis in our study was accompanied by an enhanced GFAP, β-III-tubulin, and nestin mRNA expression in these cells. Thus, it may be considered that disorders of a chronic nature, especially those of a systemic nature, induce a relatively specific regenerative response via the release of TCSCs from bone marrow or other tissue niches into the PB. Hence, it is possible that circulating CXCR4+Lin–CD45- cells may exhibit a beneficial role in the reparative process.
Furthermore, this study demonstrated for the first time the higher expression of β-III-tubulin in the PB cells of patients with the exudative form of AMD. This may suggest that circulating cells have a potential ability to regenerate injured retinal tissue. Moreover, the negative correlation between PB CXCR4+Lin–CD45- cell concentrations and the intracellular expression of neuroprogenitor and glial cell markers observed in patients with neovascular AMD may indicate pathophysiological relationships between the analysed parameters. The possibility that a relatively small pool of circulating CXCR4+Lin–CD45- cells, under conditions of their poor mobilization into the PB, comprise a comparatively large percentage of neural and glial progenitor cells cannot be excluded. However, the exact proportions of neural and glial TCSCs cells within the population of CXCR4+Lin–CD45- cells remain to be determined.
The mechanism by which SPCs home into the damaged retina is not fully understood either. Many reports have indicated that stem-cell migration and tissue-specific homing are regulated by chemokines/growth factors and their receptors [24]. Among the chemokines involved in these processes, SDF-1 plays a unique and very important biological role by regulating the trafficking of SPCs expressing the chemokine receptor CXCR4 [25].
In our study, we found a significantly lower SDF-1 plasma level in exudative AMD patients than in the healthy controls. Furthermore, our findings revealed a negative correlation between the SDF-1 plasma level and the number of CXCR4+Lin–CD45- cells in healthy controls, as well as a similar relationship between SDF-1 concentration and the expression of β-III-tubulin in PB cells in AMD patients. These results collectively indicate a possible pathophysiological linkage between the distribution of bone-marrow-derived neural progenitors in tissues and systemic SDF-1 levels. It should be noted that the current findings are in accordance with our earlier observations, where we showed that SDF-1 concentration was significantly lower in the group of AMD patients than in the healthy controls [26].
However, it was not clarified whether the SDF-1 plasma level reflects the actual concentration of the chemokine within the injured retina or not. Therefore, the possibility that a low SDF-1 plasma level makes the attraction of bone-marrow-derived neural progenitors into the damaged retina ineffective cannot be excluded, since they stay in circulation at a higher concentration. In light of the above, a recent report by Bhutto et al. focused on the immunolocalisation of SDF-1 and its receptor in human retina. The most prominent localisation of SDF–1 was detected in RPE cells and the inner photoreceptor matrix, while CXCR4 expression was mostly identified in circulating cells within the lumen of blood vessels. More interestingly, SDF-1 immunoreactivity was significantly reduced in advanced stages of AMD when compared to normal aged choroidal stroma and RPE [27]. Since these findings are consistent with our observations, we suggest a disturbed local synthesis of the chemokine under conditions of chronic vascular impairment. Our suggestion could be additionally supported by reports showing that SDF-1 levels are elevated in acute ischaemia but decreased in chronically ischaemic tissue [28]. However, it cannot be excluded that other factors may also play an important role in recruiting circulating SPCs to sites of retinal injury [6]. Therefore, complete elucidation of all the mechanisms involved in mutual cellular and humoral interactions during the course of AMD requires further studies.
Taken together, the results presented here support the hypothesis of a genuine role of TCSCs in the maintenance of retinal tissue homeostasis. However, the process of differentiation of circulating TCSCs into mature cells at the place of injury, as well as the regulatory mechanisms involved in this process, was not entirely clarified. Further studies are needed for a precise elucidation of these issues. We conclude that neural progenitor cells, together with a low SDF-1 concentration, may play a considerable role in process of AMD development. Our findings extend current knowledge on the pathophysiological circulation of SPCs in the course of AMD, and they may have implications for the future development of effective preventive measures against this disease.
References
Augood CA, Vingerling JR, de Jong PT, Chakravarthy U, Seland J, Soubrane G, Tomazzoli L, Topouzis F, Bentham G, Rahu M, Vioque J, Young IS, Fletcher AE (2006) Prevalence of age-related maculopathy in older Europeans: the European Eye Study. Arch Ophthalmol 124:529–535
Wang W, Dean DC, Kaplan HJ (2010) Age-related macular degeneration. Discov Med 9:13–15
Gehrs KM, Anderson DH, Johnson LV, Hageman GS (2006) Age-related macular degeneration—emerging pathogenetic and therapeutic concepts. Ann Med 38:450–471
Yodoi Y, Sasahara M, Kameda T, Yoshimura N, Otani A (2007) Circulating hematopoietic stem cells in patients with neovascular age-related macular degeneration. Invest Ophthalmol Vis Sci 48:5464–72
Kucia M, Ratajczak J, Reca R, Janowska-Wieczorek A, Ratajczak MZ (2004) Tissue-specific muscle, neural and liver stem/progenitor cells reside in the bone marrow, respond to an SDF-1 gradient and are mobilized into peripheral blood during stress and tissue injury. Blood Cells Mol Dis 32:52–57
Kucia M, Wojakowski W, Reca R, Machalinski B, Gozdzik J, Majka M, Baran J, Ratajczak J, Ratajczak MZ (2006) The migration of bone marrow-derived non-hematopoietic tissue-committed stem cells is regulated in an SDF-1-, HGF-, and LIF-dependent manner. Arch Immunol Ther Exp (Warsz) 54:121–135
Bajetto A, Bonavia R, Barbero S, Piccioli P, Costa A, Florio T, Schettini G (1999) Glial and neuronal cells express functional chemokine receptor CXCR4 and its natural ligand stromal cell-derived factor 1. J Neurochem 73:2348–2357
Kucia M, Ratajczak J, Ratajczak MZ (2005) Bone marrow as a source of circulating CXCR4+ tissue-committed stem cells. Biol Cell 97:133–146
Connell PP, Keane PA, O’Neill EC, Altaie RW, Loane E, Neelam K, Nolan JM, Beatty S (2009) Risk factors for age-related maculopathy. J Ophthalmol 360764:1–39
Caballero S, Sengupta N, Crafoord S, Lund R, Kruse FE, Young M, Grant MB (2004) The many possible roles of stem cells in age-related macular degeneration. Graefes Arch Clin Exp Ophthalmol 242:85–90
Kicic A, Shen WY, Wilson AS, Constable IJ, Robertson T, Rakoczy PE (2003) Differentiation of marrow stromal cells into photoreceptors in the rat eye. J Neurosci 23:7742–7749
Tomita M, Adachi Y, Yamada H, Takahashi K, Kiuchi K, Oyaizu H, Ikebukuro K, Kaneda H, Matsumura M, Ikehara S (2002) Bone marrow-derived stem cells can differentiate into retinal cells in injured rat retina. Stem Cells 20:279–283
Shi Q, Rafii S, Wu MH, Wijelath ES, Yu C, Ishida A, Fujita Y, Kothari S, Mohle R, Sauvage LR, Moore MA, Storb RF, Hammond WP (1998) Evidence for circulating bone marrow-derived endothelial cells. Blood 92:362–367
Siqueira RC, Voltarelli JC, Messias AM, Jorge R (2010) Possible mechanisms of retinal function recovery with the use of cell therapy with bone marrow-derived stem cells. Arq Bras Oftalmol 73:474–479
Kucia M, Halasa M, Wysoczynski M, Baskiewics-Masiuk M, Moldenhawer S, Zuba-Surma E, Czajka R, Wojakowski W, Machalinski B, Ratajczak MZ (2007) Morphological and molecular characterization of novel population of CXCR4(+) SSEA-4(+) Oct-4(+) very small embryonic-like cells purified from human cord blood - preliminary report. Leukemia 21:297–303
Paczkowska E, Kucia M, Koziarska D, Halasa M, Safranow K, Masiuk M, Karbicka A, Nowik M, Nowacki P, Ratajczak MZ, Machalinski B (2009) Clinical evidence that very small embryonic-like stem cells are mobilized into peripheral blood in patients after stroke. Stroke 40:1237–1244
Tan JS, Mitchell P, Smith W, Wang JJ (2007) Cardiovascular risk factors and the long-term incidence of age-related macular degeneration: the Blue Mountains Eye Study. Ophthalmology 114(6):1143–1150
Tan JS, Wang JJ, Liew G, Rochtchina E, Mitchell P (2008) Age-related macular degeneration and mortality from cardiovascular disease or stroke. Br J Ophthalmol 92:509–512
Duan Y, Mo J, Klein R, Scott IU, Lin HM, Caulfield J, Patel M, Liao D (2007) Age-related macular degeneration is associated with incident myocardial infarction among elderly Americans. Ophthalmology 114:732–737
Egan CG, Caporali F, Capecchi PL, Lazzerini PE, Pasini FL, Sorrentino V (2011) Levels of circulating CXCR4-positive cells are decreased and negatively correlated with risk factors in cardiac transplant recipients. Heart Vessels 26(3):258–266
Egan CG, Caporali F, Huqi AF, Zito MC, Focardi M, Mondillo S, Pierli C, Marzilli M, Sorrentino V (2009) Reduced levels of putative endothelial progenitor and CXCR4+ cells in coronary artery disease: kinetics following percutaneous coronary intervention and association with clinical characteristics. Thromb Haemost 101:1138–1146
Egan CG, Lavery R, Caporali F, Fondelli C, Laghi-Pasini F, Dotta F, Sorrentino V (2008) Generalised reduction of putative endothelial progenitors and CXCR4-positive peripheral blood cells in type 2 diabetes. Diabetologia 51:1296–1305
Stolzing A, Scutt A (2006) Age-related impairment of mesenchymal progenitor cell function. Aging Cell 5:213–224
Lapidot T, Petit I (2002) Current understanding of stem cell mobilization: The roles of chemokines, proteolytic enzymes, adhesion molecules, cytokines, and stromal cells. Exp Hematol 30:973–981
Kucia M, Jankowski K, Reca R, Wysoczynski M, Bandura L, Allendorf DJ, Zhang J, Ratajczak J, Ratajczak MZ (2004) CXCR4-SDF-1 signalling, locomotion, chemotaxis and adhesion. J Mol Histol 35:233–245
Machalinska A, Safranow K, Dziedziejko V, Mozolewska-Piotrowska K, Paczkowska E, Klos P, Pius E, Grymula K, Wiszniewska B, Karczewicz D, Machalinski B (2011) Different populations of circulating endothelial cells in patients with age-related macular degeneration: a novel insight into pathogenesis. Invest Ophthalmol Vis Sci 52:93–100
Bhutto IA, McLeod DS, Merges C, Hasegawa T, Lutty GA (2006) Localisation of SDF-1 and its receptor CXCR4 in retina and choroid of aged human eyes and in eyes with age related macular degeneration. Br J Ophthalmol 90:906–910
van Weel V, Seghers L, de Vries MR, Kuiper EJ, Schlingemann RO, Bajema IM, Lindeman JH, Delis-van Diemen PM, van Hinsbergh VW, van Bockel JH, Quax PH (2007) Expression of vascular endothelial growth factor, stromal cell-derived factor-1, and CXCR4 in human limb muscle with acute and chronic ischemia. Arterioscler Thromb Vasc Biol 27:1426–1432
Acknowledgments
This work was supported by the Polish Ministry of Science and Higher Education (grant number: N N402 172137 to AM).
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Author information
Authors and Affiliations
Corresponding authors
Rights and permissions
Open Access This is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License (https://creativecommons.org/licenses/by-nc/2.0), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
About this article
Cite this article
Machalińska, A., Kłos, P., Safranow, K. et al. Neural stem/progenitor cells circulating in peripheral blood of patients with neovascular form of AMD: a novel view on pathophysiology. Graefes Arch Clin Exp Ophthalmol 249, 1785–1794 (2011). https://doi.org/10.1007/s00417-011-1767-9
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00417-011-1767-9