
Abstract
The intricate interplay of exposure and speed leave motorcyclists vulnerable, leading to high mortality rates. During the collision, the driver and the passenger are usually projected away from the motorcycle, with variable trajectories or final positions. Injuries resulting from the crash can exhibit distinct and specific characteristics depending on the circumstances of the occurrence.
The aim of this study is to provide a systematic review of the literature on injuries sustained by motorcyclists involved in road accidents describing and analyzing elements that are useful for forensic assessment.
The literature search was performed using PubMed, Scopus and Web of Science from January 1970 to June 2023. Eligible studies have investigated issues of interest to forensic medicine about during traffic accidents involving motorcycle. A total of 142 studies met the inclusion criteria and were classified and analyzed based on the anatomical regions of the body affected (head, neck, thoraco-abdominal, pelvis, and limb injuries). Moreover, also the strategies for preventing lesions and assessing injuries in the reconstruction of motorcycle accidents were examined and discussed.
This review highlights that, beyond injuries commonly associated with motorcycle accidents, such as head injuries, there are also unique lesions linked to the specific dynamics of accidents. These include factors like the seating position of the passenger or impact with the helmet or motorbike components. The forensic assessment of injury distribution could serve as support in reconstructing the sequence of events leading to the crash and defining the cause of death in trauma fatalities.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Road crashes highly contribute to morbidity and mortality in developed and developing nations alike. Despite motorcycles account for a small fraction of the overall circulating vehicles, they are exaggeratedly involved in road collisions, thereby carrying significant forensic and medical implications [1, 2]. The intricate interplay of exposure and speed leave motorcyclists vulnerable resulting in high mortality rates. While enclosed passenger vehicles can dissipate a notable amount of energy in a collision, somehow providing driver protection against direct impact forces, motorcyclists have less protections and are easily injured [3,4,5]. In traffic accidents involving motorcycles, it is essential not only to determine the cause of death but also to provide a detailed description of all injuries. This information is crucial for accurately reconstructing the sequence of events [6]. Forensic pathologists can offer some insights for collision accident responsibility by studying the injury patterns and the location of the motorcycle victim’s body [7], with implications in the criminal, civil, and insurance fields. During the collision, the driver and the passenger are usually projected away from the motorcycle, resulting in variable trajectories and final positions of difficult interpretation [8]. Therefore, the reconstruction of motorcycle traffic accidents is still a challenging task [9, 10].
Injuries resulting from a traffic accident involving motorcyclists can show distinct and specific characteristics depending on the manner of occurrence. These findings can be integrated with other available information in the investigation, including circumstantial and engineering data, to assist in the reconstruction of the dynamics of the traffic accident.
A systematic review of studies reporting injuries observed in motorcyclists involved in traffic accidents was conducted to describe and analyze elements pertinent to forensic assessment. This includes features of reported injuries, their role in causing death, and their relevance in reconstructing the dynamics of the accidents.
Materials and methods
An electronic search was performed in 3 databases: PubMed, Scopus and Web of Science. Keywords related to the study aim and included in the search string were: (motorcycle OR motorbike) AND (traffic accident OR road traffic OR motor vehicle OR crash) AND (injury OR wound OR prevention). The Preferred Reporting Items for Systematic reviews and Meta-analyses (PRISMA) guidelines were used [11].
The English language and time interval of publication, from January 1970 to June 2023, were applied as filters. All studies (original article, case report, retrospective and prospective case series) that investigate the characteristics of injuries produced during traffic accidents involving motorcycles were included. A lot of peer-reviewed papers concerning injuries and safety measures can also be found in conference proceedings (i.e. STAPP and IRCOBI). However, for the purpose of the present review, peer-reviewed papers from conferences and proceedings were not included.
The following studies were included: (a) forensic studies involving the autopsy of victims; (b) clinical studies conducted in both living and deceased subjects within clinical settings, providing information on the distribution and injury mechanisms of injuries; (c) and traffic engineering and public health studies that analyzed strategies and technologies for injury prevention in motorcycle-related road traffic accidents.
Titles, abstracts, and full texts were screened for inclusion criteria and examined. References of the selected articles were further screened, and related papers were included as a source of additional data. The following details were collected: first authors’ names, article titles, journal names, publication years, article types (prospective studies, retrospective studies, case reports, or original articles), the number of cases, whether the autopsy had been performed and injury localization and trauma mechanisms.
Results
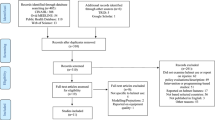
The results of the literature search are summarized in Fig. 1. One hundred and forty-two studies met the inclusion criteria and were included in the review. The results of the systematic review are summarized in Table 1.

PRISMA flowchart of the present review
One-hundred-eighteen papers fulfilled the inclusion criteria a) and b), as they presented findings from autopsy and clinical studies. Among these, 78 (66%) were retrospective studies, 33 (28%) were case reports, and 7 (6%) were prospective studies. The forensic studies, where autopsies were conducted were 63. The clinical studies conducted primarily on both living and deceased patients excluding autopsies were 55 and included the largest number of cases. Head injuries were the most extensively analyzed, appearing in the largest number of studies (89/118), followed by lesions to neck (73/118), chest and abdomen (chest 56/118; abdomen 44/118), pelvis (26/118), and limbs (55/118). The description and features of the lesions were extracted from each article and thoroughly discussed.
Twenty-four studies fulfilled the inclusion criteria (c), as they focus on injury prevention strategies and technologies. Among these, 10 (41%) were retrospective studies, 7 (29.5%) experimental studies, and 7 (29.5%) were reviews.
Discussion
In traffic accidents involving motorcycles, injuries can occur in various regions of the body through different mechanisms. Given their severity, these injuries can lead to the victim’s fatality or, if not fatal, can offer valuable insights into the dynamics of the accident. The first five paragraphs discuss the characteristics of the injuries, based on a literature review, categorised by the body regions affected (head, neck, thorax-abdomen, pelvis and limbs). The sixth paragraph discusses the evaluation of injury prevention tests and technologies. Given the broad timespan of the literature review (1970–2023), each paragraph shows the chronological arrangement of cited sources corresponding to the respective topics under discussion. The final section examines elements critical to forensic assessment, including the role of injuries in causing fatalities and their importance in reconstructing accident dynamics.
Head injuries
Head and facial injuries are the most frequent injuries observed in motorcycle accidents, with brain damage being the leading cause of death among motorcyclists [5, 34, 71, 131]. These injuries can result from various mechanisms. One major cause is the impact of victims’ head with other vehicles, fixed obstacles, or the ground when they are forcefully thrown after a collision due to the high inertia involved [71]. Additionally, brain injuries are often caused by deceleration forces, as the brain is not fixed, allowing it to relative movement within the skull. This can lead to various deceleration effects, such as multifocal vascular ruptures, cerebral concussion, or diffuse axonal damage [146]. Furthermore, injuries to the brainstem and pontomedullary region can result from significant movements like hyperextension, antero-flexion, and torsion of the head, caused by either direct contact trauma or acceleration-deceleration forces [147,148,149].
The most common head traumas observed in motorcycle accidents are concussions, followed by brain contusions or haemorrhages, facial and skull fractures [40, 143]. Wearing helmets prevents them: full-face helmets specifically reduce the incidence of brain contusions more effectively than the open-face type. However, the prevalence of skull fracture, subdural hematoma, and subarachnoid haemorrhage does not differ significantly between the two kinds of helmets [42]. Nonetheless, full-face integral crash helmets can also cause skull base fractures, as a portion of the impacting force is transmitted to the skull base through the chinstrap, involving the mandibular rami and condyles [15]. Moreover, heavier helmets are more likely to result in partial or complete ring fractures of the base of the skull when subjected to axial loading [25].
Brain injuries can also be linked to facial bone fractures. Studies have shown that fractures of the upper part of the face, such as the zygomatic and orbital bones, are more commonly associated with brain injuries than fractures of the lower part of the face, such as the mandibular bone [98, 150, 151].
Papers addressing skull fractures caused by direct impact have been distributed over the past 20 years [5, 34, 40, 42, 71, 98, 131]. Papers discussing severe ring fractures at the base of the skull associated with the use of full-face helmets originate from the 1990s [15, 25].
Neck injuries
The most prevalent neck injuries due to motorcycle accidents include hemorrhage in the carotid sheath, subluxation in the occipital-atlanto-axial complex, hemorrhage in the muscles and triangles of the anterior neck, and damages along the vertebral artery [39].
The cervical spine region is the most affected part in case of fatal crashes [34]. Specifically, when the head undergoes hyperextension during a crash, the forces are transmitted through the cervical spine, leading to tissue damage [98]. The effectiveness of helmets in preventing cervical spine injuries remains a topic of debate. Some studies suggest their usefulness [116, 127], but Hitosugi et al. reported that the prevalence of cervical fractures was slightly higher in individuals wearing full-face helmets compared to those wearing the open-face type [42].
Regarding other helmet-related injuries, the helmet buckle can also cause fractures in the neck cartilage, primarily affecting the thyroid cartilage. The energy from the trauma results in the displacement of the helmet, and its buckle subsequently exerts pressure on the surrounding tissues. If the helmet buckle is positioned over the larynx at the moment of impact, it can exert enough force to potentially fracture the laryngeal cartilages [117].
Concerning neck vascular injuries, internal carotid artery dissection, though rare, has a high mortality rate after motorcycle accidents [124]. This type of injury may occur due to hyperextension and rotation of the neck, reflecting traction on the internal carotid artery as it crosses the transverse processes of the second and third cervical vertebrae. Another possible mechanism is abrupt full flexion of the neck, which can directly compress the internal carotid artery between the angle of the mandible and the upper cervical vertebrae [152]. Additionally, the pressure applied by the helmet strap on the soft tissues of the neck could also contribute to vascular damage [120]. A traumatic injury to the vertebral artery may determine death, especially in low-speed accidents, where the person may not immediately complain of specific symptoms after the accident. Instead, they may start feeling unwell hours or even days later, typically experiencing neurological symptoms like nausea, vomiting, and eventually leading to coma and death. The traumatic dissection of the vertebral artery causes cerebral infarction, followed by edema and compression of the brainstem. The vertebral artery is particularly susceptible to longitudinal stretch, and it can be hurt during sudden neck movements involving hyperextension and/or rotation. Therefore, in cases of delayed symptom presentation, forensic examination should take into account the possibility of vertebral artery dissection as a potential cause of death [61, 153].
Although rare, severe high-energy trauma can lead to the complete separation of neck tissues, even resulting in decapitation. The latter may be caused by different mechanisms, but it is often due to an impact against an immovable object [114]. Decapitation can also be attributed to the action of the lower edge of a full-face helmet during an incident. When a full-face helmet is worn during a traumatic event, the lower edge of the helmet can exert a significantly powerful force on the surrounding tissues, potentially leading to a complete cervical spine amputation [67, 88]. Additionally, instances of decapitation have been reported in the literature due to the interaction with motorcycle components. Ihama et al. reported a case in which a motorcyclist’s neck became entangled in a rotating motorcycle chain, resulting in complete decapitation [10].
All reported articles on neck injuries have been published within the last 20 years. Notably, certain articles focusing on helmet-related injuries [116, 127] and vertebral artery dissections [120, 124] encompass publications from the last 5 years.
Chest and abdomen injuries
Injuries to the thorax and abdominal regions pose a significant risk of death due to severe blood loss, asphyxiation caused by thorax compression, and vertebral spine fractures [5, 33, 63, 121]. Common lesions in these areas include lung contusion and liver laceration, often occurring simultaneously with rib fractures [34, 81]. Impact during falls, especially between the left side of the abdomen and the end of the motorcycle handlebars, can cause splenic and pancreatic damages [44].
In high-velocity trauma, injury to the aorta is a typical and highly fatal occurrence. The ascending aorta is the most common affected segment, followed by the arch, thoracic, and abdominal sections [140]. Traumatic events in the ascending aorta or arch should be considered in cases of cardiac tamponade, aortic valve regurgitation, and myocardial contusion [84]. According to Richens et al., the aorta is subjected to various mechanical forces in anatomically vulnerable sites. Sudden deceleration can cause a stretching effect, leading to laceration of the isthmus as the ascending aorta and aortic arch are more mobile than the fixed distal descending part. Additionally, the aorta may rupture due to a sudden increase in blood pressure and entrapment between the anterior chest wall and the vertebral column [154]. The primary physiopathological mechanism of aortic laceration can be difficult to ascertain because of the diversity and complexity of crash scenarios, particularly when victims have been exposed to multiple external forces [112].
In major traumas, the thoracic spinal column may fracture. These injuries exhibit an “all or nothing” phenomenon, irrespective of the cause of the trauma, and tend to be more severe compared to similar lesions in the cervical region [127]. The thoracic spinal column may extensively suffer the trauma, or it remains intact with no damage. This effect is caused by the restraining effect of the ribs and sternum on the thoracic spine, making it less mobile. Consequently, if a force is powerful enough to break through a segment, the adjacent mobile segments are unable to absorb the remaining force, leading to displacement and significant injury to the spinal cord. Moreover, the thoracic canal provides slightly less space per segment compared to the cervical spine, favouring even slight displacement more dangerous [155].
Complete trunk severance cases are rare and typically associated with accidents involving high impact speeds. Muggenthaler et al. [76] documented a case of complete trunk severance resulting from a collision with a road signpost.
The articles mentioned in this paragraph have all been published in the last 20 years. Specifically, the articles addressing injuries to the aorta [112, 140] and spine [127] are from the last 5 years.
Pelvis injuries
These are often attributed to contact with the motorcycle fuel tank during the collision [101]. These injuries can include fractures of the pelvic ring bones, damage to internal organs within the pelvic cavity, associated with pelvic haemorrhages of varying degrees, as well as lesions to the soft tissues of the lower abdomen, perineum, groin, or testicular area [9, 52].
Fuel tank injuries are typically experienced by the motorcycle driver, particularly in frontal collisions, when after impact, a sudden deceleration can propel the driver forward, colliding with the tank [71, 101, 156]. Interestingly, drivers who attempt to avoid a collision and topple over immediately before the impact are less likely to experience fuel tank injuries [52].
Even passengers can suffer groin injuries in accidents involving two riders on a motorcycle. In fact, passengers who are seated behind the driver often slide on the saddle, sometimes even onto the fuel tank, and then may hit the driver’s buttocks and back. However, the protection of the driver’s buttocks and back, can reduce the passengers’ risk of underbelly injuries [104].
The articles mentioned in this paragraph have all been published in the last 20 years. Specifically, some articles addressing fuel tank injuries [52, 101, 104] are from the last 5 years.
Limb injuries
Motorcycle riders are particularly susceptible to limb injuries due to their heightened exposure to direct impacts [5]. Non-fatal limb injuries are the most frequent, encompassing ligamentous lesions, fractures, and dislocations [34, 38, 93]. These lesions occur when limbs become entrapped between the motorcycle and the ground or impact with fixed road signs or poles [48, 59, 97].
Regarding the upper limbs, the most common limb injuries are fractures of the shoulder, forearm, and hand [59, 97], reflecting the motorcyclist’s position, with flexed elbows being farthest from the impact point [132].
Forearm and hand injuries have been associated with lower mortality rates, because upper extremities act like a “crumple zone” when crash at highway speeds, protecting the head and neck region from direct impact in head-first hit damages in frontal crashes [95]. The distal portion of the upper extremity absorbs the energy of the collision, potentially reducing severe proximal trauma to the head and neck [12].
Hand lesions are more common in motorcycle drivers than in passengers, because during a collision, the driver instinctively locks their elbows and firmly holds onto the handlebars, redistributing the resulting force into the palm and metacarpal base. Thumb carpometacarpal joint injuries are particularly common due to the thumb’s position onto the handlebar grip making it more vulnerable to trauma [5, 103].
Concerning the lower limbs, the tibia is the most common site, followed by the proximal femur, particularly in lateral impact, patella and foot [20, 34, 125]. The heel is particularly susceptible with calcaneus fractures, Achilles tendon ruptures, and defects. The motorcycle’s lack of spoke guards or poorly designed guards favours the entrapment of the pillion passenger’s heel between the spokes and the frames, resulting in crushing and grinding injuries from the continuously rotating wheels [30, 74].
The articles cited in this paragraph cover a wide range of time periods, from the 1970s to the 1990s [12, 26, 30] to the 2020s [125, 132]. This temporal variety is evident in articles discussing both upper and lower limb injuries.
Injury prevention strategies and technologies
The topic of injury prevention strategies and technologies has gained increasing interest in recent years. In fact, the articles mentioned in this paragraph have all been published since 2009, and a substantial number of them are very recent, with publication dates within the last five years [113, 115, 119, 122, 123, 128, 129, 133, 136, 137, 141, 145].
Injury prevention strategies and technologies for motorcyclists have focused on two main aspects. Firstly, helmets are used to primarily protect the head, an area highly correlated with increased mortality rates. Secondly, protective clothing and wearable devices are employed to shield the remaining parts of the body.
The mandatory use of motorcycle helmets for both drivers and adult passengers has become a global legal requirement, with few discrepancies in regulations across the world. However, variations persist, particularly regarding restrictions on transporting child passengers in Asia and Africa, despite the prevalence of motorcycle use in these continents [129, 157].
It is well known that motorcyclists wearing helmets tend to experience less frequent and severe episodes of head and facial injuries. Helmets have demonstrated effectiveness in mitigating and preventing traumatic brain injuries in motorcycle accidents, particularly during impacts with large energy-absorbing surfaces, for example when the head collides with the ground or the surface of a car body. However, the protective capacity of helmets is constrained when the materials they are made of surpass their tolerance thresholds, as in high-speed impacts or direct trauma with objects presenting limited surface areas, such as light poles, trees, or angular parts of the vehicle [131, 133, 139, 143].
Modern helmets are designed to have a rigid polycarbonate outer shell with a firmly placed energy-absorbing liner, while a soft expanded polystyrene or polyurethane foam padding forms the innermost layer.
Helmet damage can range from subtle blemishes to obvious defects, and their careful examination can provide valuable information about the accident dynamics and cranial injuries sustained by the motorcyclist. Conventional helmet damage assessment involves the manual removal of each layer, a process prone to oversight and additional damaging. To reduce these risks, the use of computed tomography scanning of the helmet has been suggested. This method allows precise delineation of damage within each layer, including breaks in the outer shell or compression in the inner layers. The radiological examination can also facilitate measurements of the thickness and density of the foam and can detect bloodstains, confirming that the helmet was worn by the motorcyclist at the time of impact [158].
While full-face helmets provide comprehensive protection, open-face and half-cover helmets, although less secure, are still in use [42, 145]. Recent studies suggest that full-face helmets offer better protection against head and face injuries, but may be less effective in preventing neck injuries and skull base fractures [136, 145]. Notably, motorcycle full-face helmet visors, while not designed for energy absorption, redirect mid-face impact forces to the upper and lower face, enhancing protection [145]. Despite the overall recommendation for full-face helmets due to their reduced mortality and injury probability, their usage is often limited due to discomfort, particularly in subtropical and tropical climates where most motorcyclists reside [141].
Despite the universally recognized head protection helmets offer, a debated issue remains concerning a potential increase in the risk of cervical spine injuries due to increased hyperflexion-hyperextension movements induced by the helmet’s lower edge [15, 117, 133]. Some studies suggest that helmet use reduces the risk of cervical spinal cord injuries during motorcycle crashes [116, 127]. However, Hitosugi et al. [42] reported a prevalence of cervical fractures wearing full-face helmets. The literature is inconclusive, suggesting that helmet use does not directly increase spinal injuries, but may be less effective in preventing severe cervical injuries compared to cranial injuries [94, 108]. Nevertheless, the present review indicates that fatal skull base ring fractures associated with the use of full-face helmets have been reported in articles dating back to the 1990s [15, 25]. This reinforces the notion that contemporary helmets are effective in preventing more severe spinal injuries. On this point, advancements in helmet technology have recently introduced airbag-equipped helmets, representing a novel class of protective headgear. These helmets, equipped with inflatable structures, have demonstrated a reduction in concentrated impact force to the lower- or mid-face region, resulting in decreased head rotation and brain strain. Contrary to conventional helmets, these devices only deploy when necessary, preserving the field of vision and ventilation during normal use [145].
In injury prevention, wearing a helmet is not only crucial but equally important is the correct method of wearing it. Proper helmet fixation and correct strap positioning are essential for effective prevention of head and neck injuries. Loose helmet straps can cause ejection or compromise anterior neck structures in high-impact crashes [136]. Moreover, helmeted individuals are significantly less likely to sustain shoulder fractures, suggesting a protective effect of helmets. A possible explanation is that energy transmission through the helmet and neck flexion during the impact may shield the proximal humerus and shoulder girdle [132].
The current regulation from January 2021 is ECE 22.06, which introduces new test procedures for the production and assessment of next-generation helmets. These include a rotational acceleration test to assess oblique impacts, linear impact tests for both high and low energy impacts, testing of retention systems and new assessments for helmet visors to measure impact resistance against small objects thrown at high speed. In addition, ECE 22.06 requires a test to assess helmet stability on the head. While the previous standard, ECE 22.05, simulated the risk of “roll-off”, where the helmet rotates forward and disengages from the rider’s head on impact, ECE 22.06 extends the assessment to the possibility of backward rotation, potentially exposing the rider’s forehead or neck after impact. This evaluation includes the open chin guard tear test, which ensures complete detachment of the chin guard to reduce the risk of neck injury. ECE regulations also assess the point of impact on the helmet during a crash. While ECE 22.05 identified six primary impact points (front, top, back, sides, and chin), ECE 22.06 extends the evaluation to include 12 additional intermediate impact points along the mid-lines [159].
Concerning protective clothing for motorcyclists, epidemiological observations highlight the vulnerability of light motorcycle drivers compared to heavy motorcycle users. Light motorcycle drivers, often not wearing protective clothing, are statistically more involved in road accidents, as these motorcycles are commonly used for work and transport [83]. Technical clothing such as jackets, pants, shoes, and gloves has shown effectiveness in preventing soft-tissue injuries, particularly open wounds, but has no significant impact on systemic injuries or fractures [75, 83].
The usage of protective clothing reduces the probability of upper (shoulder and elbow) and lower limb (buttock and thigh) skin injuries, while providing less effective protection for the chest, abdomen, back, and groin [91]. However, the use of motorcycle protective clothing in warm seasons may impair cognitive and psychophysical functions, potentially affecting riding performance and safety due to body overheating [82, 91].
Given the limitations of protective clothing, specific impact protection technologies have been developed for areas of the body where protection is limited, such as the back and abdomen [91]. Nevertheless, their adoption remains uncommon among on-road motorcyclists, and there are no laws governing the usage of such protective measures [139].
Protective clothing cannot entirely prevent limb fractures during falls, especially severe ones affecting the proximal femur in lateral impacts. Hard hip protectors, designed to cover the greater trochanter, effectively absorb and redirect impact energy away from vulnerable areas, preventing direct hip fractures [64]. Studies on limb injuries cover several decades, from the 1970s through the 1990s [12, 26, 30] to the 2020s [125, 132]. During this wide timeframe, to the best of our knowledge, no effective protective device suitable to prevent limb bone or soft tissue injuries was developed. Indeed, while current protective equipment is effective in preventing skin injuries, it still has significant limitations in preventing more severe damage [75, 83].
Back protectors, initially designed for racing sports, have shown effectiveness in reducing back cutaneous injuries but are limited in protecting against spinal injuries caused by bending and torsional forces [102, 128]. The integration of hard-shell or airbag technologies into back protectors may enhance their effectiveness in preventing serious spinal injuries [92].
Recent developments include rider-worn pelvic protection devices designed to reduce the risk of injury from contact with the motorcycle fuel tank during a crash. Simulation studies suggest potential benefits in the absorption and distribution of impact energy, but the understanding of pelvic biomechanics under anteroposterior loading is currently limited [137].
The effective prevention of trunk injuries remains a subject of ongoing study. The substantial number of recently published studies examining these injuries, particularly in relation to aorta laceration [112, 140], spinal fractures [127], and fuel tank injuries [52, 101, 104], underscores the persistent challenge posed by these injuries.
Injuries evaluation in the reconstruction of the crash dynamics
The evaluation of injuries for analyzing the dynamics of the accident is of forensic significance in criminal, civil, or insurance cases, since the results of medical examinations or autopsies enhance the information gathered from on-site inspections and circumstantial data. Fatal injuries typically result from direct impacts on the body during accidents involving other vehicles, the ground, or fixed obstacles. In many cases, multiple impacts usually involve an initial collision with objects, followed by a secondary impact with the ground. Furthermore, the subjects may sustain tertiary injuries due to being struck by vehicles or colliding with fixed obstacles such as road poles, walls, or barriers [81, 131].
In fatal cases from direct impacts the primary cause of death is a neurogenic shock due to a direct head impact [40, 71]. The site of cranial blunt trauma can be determined by combining autopsy findings, typically skull fractures and intracranial hemorrhages, with data collected from the accident scene. Therefore, it is crucial to establish whether the victim was wearing a helmet and, in such instances, to have the ability to examine it. Locating the break points on the surface of the helmet can provide crucial information regarding the precise point of impact.
It is also paramount to assess the helmet’s fit on the subject, by measuring the length of the buckle to assess its suitability for the subject’s facial and neck proportions, given that excessive helmet excursion during a crash can potentially led to laryngeal cartilage fracture which can be better identified by radiological studies such as computed tomography.
Direct trauma to the thorax and abdomen can result in internal thoracoabdominal organ lacerations, leading to fatal hemorrhagic shock. Such trauma can occur due to contact with the ground or components of the motorcycle, such as its handlebars [5, 33, 44, 63, 121]. At autopsy, if that kind of vehicle collision dynamics is suspected, bruising patterns that mimic the shape of handlebar components should externally be sought. During the examination of the body, consideration should be given to whether the victim was wearing protective motorcycle clothing. This factor can potentially mitigate skin injuries, particularly on the limbs, making them less apparent on external inspection.
Fatal injuries can be attributed also to the forces of acceleration and deceleration resulting from sudden, unrestricted body movements, which induce compressive, tensile, and shear strains of the tissue. Specifically, neck hyperextension can damage the brainstem and cervical region, presenting at autopsy as brain hemorrhages without cranial fractures, fractures of the cervical vertebrae, soft tissue hemorrhages, or carotid artery dissection. This vessel is particularly susceptible to hyperextension movements as the vascular wall can undergo stretching and tearing [34, 98, 124]. Even in cases of low-energy trauma where the subject deceases some days after the accident, suspicion should fall on vertebral artery dissection. This vessel is notably vulnerable to longitudinal stretching and can rupture even in mild hyperextension or neck rotation [61, 153]. A meticulous macroscopic and microscopic examination of the vertebral artery is mandatory when symptoms such as nausea and vomit were reported in clinical record.
In the thoracoabdominal region acceleration and deceleration forces can cause fatal injuries especially in high-energy trauma with the involvement of the aorta, that is highly susceptible to stretching and tearing, primarily in its more mobile segments, such as the isthmus and arch [140, 154], resulting in hemorrhagic shock without significant direct trauma indicators. A violent hyperextension of the thoracic spine can lead to severe vertebral fractures and spinal cord damage due to the limited mobility of this portion, which is firmly anchored to the ribs and sternum [127, 155].
In the forensic medical evaluation of a motorcycle accident, one of the most challenging and pertinent issues is distinguishing the driver from the passenger. In literature, it is reported that drivers are predominantly male, while passengers are female [139]. When analyzing motorcyclist fatalities by age, a notable spike is observed among subjects aged between 21 and 30 years. This trend can likely be attributed to a lack of riding experience and impulsive behavior among teens and younger adults [131]. Additionally, a higher prevalence of fatal crashes occurring at night and on weekends has been reported, with positive toxicology tests for alcohol and drugs for both drivers and passengers [139]. In most cases, it has been observed that drivers were wearing helmets at the time of the accident, whereas passengers more commonly did not wear helmets, thereby increasing the likelihood of sustaining severe traumatic brain injuries [143]. Nevertheless, these are general epidemiological data obtained from literature review, and cannot be used to discriminate between the passenger and the driver in individual cases.
The injuries sustained can provide some useful information. The ejection dynamics differ for drivers and passengers due to variations in their initial positions and postures.
The rider’s distinctive attitude is to hold the handlebars while driving, thus establishing a direct connection between himself and the motorcycle. In case of a collision, this connection can prevent the rider from being ejected from the motorcycle, thus increasing the risk of sustaining crushing or burning injuries as a result of impact with various parts of the motorcycle. Such incidents are more likely to occur in low energy collisions, as in high energy collisions the rider is typically thrown and ejected at a distance due to the significant inertial forces, preventing them from remaining anchored to the vehicle [71].
Conversely, pillion passengers have different options for support. They can either grasp the bar attached to the tail of the motorcycle or hold onto the driver’s haunches in front of them. However, due to their less stable position, pillion passengers are typically propelled higher into the air during the accident, resulting in a longer fall to the ground from a greater distance [71].
Some specific lesions may serve as distinguishing factors between the driver and the passenger involved. Passengers can suffer groin injuries, usually mild and caused by impact with the driver’s buttocks and back [104]. Furthermore, the passenger’s heel can become entrapped between the spokes and the rear wheel frame, resulting in crushing and grinding injuries [30, 74]. In drivers, lesions to the palm of the hand and the thumb carpometacarpal joints are more prevalent. This is because, during a collision, drivers tend to instinctively lock their elbows and grip the handlebars tightly [5, 71, 103]. Pelvic damage and fractures, called fuel tank injuries, tend to be associated with the driver’s impact against the fuel tank in frontal crashes where the sudden deceleration leads to the body sliding forward making contact with the fuel tank [71, 101, 156].
Nevertheless, the reconstruction remains a challenging task due to the intrinsic complexity of accident dynamics. This procedure entails a multidisciplinary approach, as demonstrated in many specific cases, mostly for the identification of the manner of death, consisting in conducting interviews with individuals directly involved in or witnessing the incident, performing mechanical and engineering examinations (i.e., a kinematic analysis) and procuring documented visual evidence of the occurrence [160, 161]. In cases involving motorcycle accidents, recorded images of the event can be sourced from various means, including surveillance cameras, helmet-mounted cameras worn by riders, and dashboard-mounted cameras in the vehicles participating in the accident.
A critical analysis of findings collected at accident scenes, including skid marks and the resting positions of vehicles, combined with the forensic evaluation of injuries in the light of developments in safety devices, addresses medical-legal responses based on scientific evidence.
Conclusion
This review highlights that, in addition to injuries commonly associated with motorcycle accidents, such as head injuries, there are also unique lesions linked to the seating position of the passenger and the specific nature of the trauma. Given the considerable variability in real-life accident scenarios and the frequent lack of comprehensive crash details, the forensic assessment of injury distribution could be a support to aid in reconstructing the dynamics of traffic accidents and to define cause of death in the crash fatalities.
Limits
While the PRISMA guidelines are widely accepted standards for conducting systematic reviews in various fields, the application of these guidelines in the present forensic pathology article presented specific challenges. In particular, the data of interest consisted primarily of qualitative information, involving descriptions of injuries and interpretations of accident dynamics, rather than numerical measurements or quantifiable data points. As a result, qualitative data inherently exhibited high variability, which made it challenging to standardise or homogenise in order to draw coherent and general conclusions within the field of forensic pathology.
Data availability
Not applicable.
References
Anh NT, Hung LS, Xuan NT, Lap PD, Tuan DT, Kien VD (2021) Skull Fracture Patterns and Morphologies Among Fatal Motorcycle Traffic Accident Victims in Vietnam. Am J Forensic Med Pathol. 42(1):30–35. https://doi.org/10.1097/PAF.0000000000000627. PMID: 33074839
Takeda A, Hitosugi M, Furukawa S (2017) Cases of Motorcyclists Dying of Trauma or Disease. Am J Forensic Med Pathol. 38(3):222–225. https://doi.org/10.1097/PAF.0000000000000331. PMID: 28682804
Grange JT, Corbett SW, Cotton A (2004) Street bikes versus dirt bikes: a comparison of injuries among motorcyclists presenting to a regional trauma center. J Trauma. 57(3):591-4. https://doi.org/10.1097/01.ta.0000144065.56090.2a. PMID: 15454807
Emiogun EF, Sanni DA, Soyemi SS, Faduyile FA, Obafunwa JO (2022) Trends in motorcycle accident mortality in Lagos: consequences of government policy changes. Med Sci Law 62(4):269–274 Epub 2022 Feb 21. https://doi.org/10.1177/00258024221082341. PMID: 35188802
Zhao H, Huang W, Yang GY, Chen R, Liu SX, Yu YM, Yin ZY, Wang ZG (2012) Analysis of 86 fatal motorcycle frontal crashes in Chongqing, China. Chin J Traumatol 15(3):170–174 PMID: 22663913
Moskała A, Woźniak K, Kluza P, Romaszko K, Lopatin O (2016) The importance of post-mortem computed tomography (PMCT) in confrontation with conventional forensic autopsy of victims of motorcycle accidents. Leg Med (Tokyo) 18:25–30 Epub 2015 Nov 23. PMID: 26832372
Guo L, Jin XL, Zhang XY, Shen J, Chen YJ, Chen JG (2008) Study of injuries combining computer simulation in motorcycle-car collision accidents. Forensic Sci Int 177(2–3):90–96. https://doi.org/10.1016/j.forsciint.2007.10.011. Epub 2008 Feb 21. PMID: 18093772
Muggenthaler H, Bismann D, Autsch A, Hubig M, Subramaniam JS, Mall G, Wittschieber D (2023) Stabbed by motorcycle? Reconstruction of an unusual traffic accident. Int J Legal Med 137(2):601–607. https://doi.org/10.1007/s00414-022-02941-8. Epub 2022 Dec 22. PMID: 36547700; PMCID: PMC9902312.]
Tattoli L, Moretti M, Di Vella G (2022) Fuel tank injury in a fatal motorcycle accident. Forensic Sci Med Pathol 18(3):256–259. https://doi.org/10.1007/s12024-021-00445-2. Epub 2022 Jan 20. PMID: 35048266
Ihama Y, Miyazaki T, Fuke C, Niki H, Maehira T (2008) Complete decapitation of a motorcycle driver due to a roadblock chain. Int J Legal Med 122(6):511–515. https://doi.org/10.1007/s00414-008-0284-9. Epub 2008 Sep 16. PMID: 18795312
Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group (2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Ann Intern Med 151(4):264–269. W64. https://doi.org/10.7326/0003-4819-151-4-200908180-00135. Epub 2009 Jul 20. PMID: 19622511
Zettas JP, Zettas P, Thanasophon B (1979) Injury patterns in motorcycle accidents. J Trauma 19:833–836
Krantz KP (1985) Head and neck injuries to motorcycle and moped riders–with special regard to the effect of protective helmets. Injury. 16(4):253-8. https://doi.org/10.1016/s0020-1383(85)80014-0. PMID: 3967913
Hoekstra HJ, Kingma LM (1985) Bilateral first rib fractures induced by integral crash helmets. J Trauma. 25(6):566-7. https://doi.org/10.1097/00005373-198506000-00020. PMID: 4009761
Cooter RD, David DJ, McLean AJ, Simpson DA (1988) Helmet-induced skull base fracture in a motorcyclist. Lancet 1:84–85. https://doi.org/10.1016/S0140-6736(88)90285-1
Shiono H, Akane A, Matsubara K, Tanabe K, Takahashi S (1990) Identification of the driver in two-rider motorcycle accidents. Inguinal contusion-laceration as an indication of the driver. Am J Forensic Med Pathol. 11(3):190-2. https://doi.org/10.1097/00000433-199009000-00002. PMID: 2220701
Shankar BS, Ramzy AI, Soderstrom CA, Dischinger PC, Clark CC (1992) Helmet use, patterns of injury, medical outcome, and costs among motorcycle drivers in Maryland. Accid Anal Prev. 24(4):385 – 96. https://doi.org/10.1016/0001-4575(92)90051-j. PMID: 1605821
Braddock, Braddock M, Schwartz R, Lapidus G, Banco L et al (1992) L. Jacobs A population-based study of motorcycle injury and costs Ann. Emerg. Med., 21 (1992), pp. 273–278
Muelleman, Muelleman RL, Mlinek EJ et al (1992) P.E. Collicott Motorcycle crash injuries and costs: effect of a reenacted comprehensive helmet use law Ann. Emerg. Med., 21 (1992), pp. 266–272
Peek C, Braver ER, Shen H, Kraus JF (1994) Lower extremity injuries from motorcycle crashes: a common cause of preventable injury. J Trauma. 37(3):358 – 64. https://doi.org/10.1097/00005373-199409000-00004. PMID: 8083893
Sharma GK, Sarangi MP, Tyagi AK (1995) Decapitation death. Med Sci Law. 35(1):85 – 6. https://doi.org/10.1177/002580249503500117. PMID: 7877481
McLean AJ (1995) Brain injury without head impact? J Neurotrauma. 12(4):621-5. https://doi.org/10.1089/neu.1995.12.621. PMID: 8683613
Johnson RM, McCarthy MC, Miller SF, Peoples JB (1995) Craniofacial trauma in injured motorcyclists: the impact of helmet usage. J Trauma. 38(6):876-8. https://doi.org/10.1097/00005373-199506000-00008. PMID: 7602627
Tracy TF Jr, Silen ML, Graham MA (1996) Delayed rupture of the abdominal aorta in a child after a suspected handlebar injury. J Trauma. 40(1):119 – 20. https://doi.org/10.1097/00005373-199601000-00022. PMID: 8576973
Konrad CJ, Fieber TS, Schuepfer GK, Gerber HR (1996) Are fractures of the base of the skull influenced by the mass of the protective helmet? A retrospective study in fatally injured motorcyclists. J Trauma. 41(5):854-8. https://doi.org/10.1097/00005373-199611000-00016. PMID: 8913216
Peek-Asa C, Kraus JF (1996) Injuries sustained by motorcycle riders in the approaching turn crash configuration. Accid Anal Prev. 28(5):561-9. https://doi.org/10.1016/0001-4575(96)00022-x. PMID: 8899037
Wick M, Müller EJ, Ekkernkamp A, Muhr G (1998) The motorcyclist: easy rider or easy victim? An analysis of motorcycle accidents in Germany. Am J Emerg Med. 16(3):320-3. https://doi.org/10.1016/s0735-6757(98)90113-9. PMID: 9596444
Hitosugi M, Takatsu A, Shigeta A (1999) Injuries of motorcyclists and bicyclists examined at autopsy. Am J Forensic Med Pathol. 20(3):251-5. https://doi.org/10.1097/00000433-199909000-00007. PMID: 10507793
Wyatt JP, O’Donnell J, Beard D, Busuttil A (1999) Injury analyses of fatal motorcycle collisions in south-east Scotland. Forensic Sci Int. 104(2–3):127 – 32. https://doi.org/10.1016/s0379-0738(99)00104-8. PMID: 10581718
Waikakul S, Vanadurongwan V, Wongtrakul S (1999) Revascularization of subtotal amputation at the ankle in children following motorcycle-spoke injury. Injury. 30(1):51 – 6. https://doi.org/10.1016/s0020-1383(98)00214-9. PMID: 10396456
Richter M, Otte D, Lehmann U, Chinn B, Schuller E, Doyle D, Sturrock K, Krettek C (2001) Head injury mechanisms in helmet-protected motorcyclists: prospective multicenter study. J Trauma. 51(5):949 – 58. https://doi.org/10.1097/00005373-200111000-00021. PMID: 11706346
Hitosugi M, Fukui K, Takatsu A (2001) Incomplete decapitation of a motorcyclist from hyperextension by inertia: a case report. Med Sci Law. 41(2):174-7. https://doi.org/10.1177/002580240104100217. PMID: 11368401
Kraus JF, Peek-Asa C, Cryer HG (2002) Incidence, severity, and patterns of intrathroacic and intra-abdominal injuries in motrocycle crashes. J Trauma 52(3):548–553
Ankarath S, Giannoudis PV, Barlow I, Bellamy MC, Matthews SJ, Smith RM (2002) Injury patterns associated with mortality following motorcycle crashes. Injury. 33(6):473-7. https://doi.org/10.1016/s0020-1383(02)00048-7. PMID: 12098541
Wladis A, Boström L, Nilsson B (2002) Injuries in 8927 patients admitted after motor-cycle crashes in Sweden 1987–1994 inclusive. Eur J Surg. 168(3):187 – 92. https://doi.org/10.1080/110241502320127810. PMID: 12182245
Lateef F (2002) Riding motorcycles: is it a lower limb hazard? Singapore Med J. 43(11):566-9. PMID: 12680525
Watanabe-Suzuki K, Suzuki O, Nozawa H, Ishii A (2002) An Yes case of a stunt man who jumped into seawater riding a motorcycle: a case report. Med Sci Law. 42(4):355-7. https://doi.org/10.1177/002580240204200413. PMID: 12487523
Colburn NT, Meyer RD (2003) Sports injury or trauma? Injuries of the competition off-road motorcyclist. Injury. 34(3):207 – 14. https://doi.org/10.1016/s0020-1383(02)00039-6. PMID: 12623252
Kasantikul V, Ouellet JV, Smith TA (2003) Head and neck injuries in fatal motorcycle collisions as determined by detailed Yes. Traffic Inj Prev. 4(3):255 – 62. https://doi.org/10.1080/15389580309878. PMID: 14522650
Kraus JF, Rice TM, Peek-Asa C, McArthur DL (2003) Facial trauma and the risk of intracranial injury in motorcycle riders. Ann Emerg Med. 41(1):18–26. https://doi.org/10.1067/mem.2003.1. PMID: 12514678
Vega RS, Adams VI (2004) Suffocation in motor vehicle crashes. Am J Forensic Med Pathol. 25(2):101-7. https://doi.org/10.1097/01.paf.0000114136.84700.f5. PMID: 15166758
Hitosugi M, Shigeta A, Takatsu A, Yokoyama T, Tokudome S (2004) Analysis of fatal injuries to motorcyclists by helmet type. Am J Forensic Med Pathol. 25(2):125-8. https://doi.org/10.1097/01.paf.0000127397.67081.f5. PMID: 15166762
Jeffers RF, Tan HB, Nicolopoulos C, Kamath R, Giannoudis PV (2004) Prevalence and patterns of foot injuries following motorcycle trauma. J Orthop Trauma. 18(2):87–91. https://doi.org/10.1097/00005131-200402000-00005. PMID: 14743027
Guerrero MA, Lin PH, Bush RL, Lumsden AB (2005) Splenic and pancreatic infarction due to motorcycle handlebar injury. J Trauma. 58(6):1304. https://doi.org/10.1097/01.ta.0000169427.28625.97. PMID: 15995489
Oliva A, Vernooy K, Cooter R, David DJ, Pascali V (2005) Helmet-induced neck degloving in a motorcyclist. J Trauma. 58(2):370-1. https://doi.org/10.1097/01.ta.0000152601.83858.72. PMID: 15706202
Ihama Y, Miyazaki T, Ageda S, Arao T, Fuke C (2006) An Yes case of heart rupture from a scooter accident with 3 riders. Am J Forensic Med Pathol. 27(1):87 – 9. https://doi.org/10.1097/01.paf.0000202808.85644.09. PMID: 16501358
Bohmer JH, Proust AF (2006) Adult bicycle handlebar injury. Am J Emerg Med. 24(5):624-5. https://doi.org/10.1016/j.ajem.2005.12.022. PMID: 16938607
Solagberu BA, Ofoegbu CK, Nasir AA, Ogundipe OK, Adekanye AO, Abdur-Rahman LO (2006) Motorcycle injuries in a developing country and the vulnerability of riders, passengers, and pedestrians. Inj Prev 12(4):266–268. https://doi.org/10.1136/ip.2005.011221. PMID: 16887951; PMCID: PMC2586788
Zargar M, Khaji A, Karbakhsh M Pattern of motorcycle-related injuries in Tehran, 1999 to 2000: a study in 6 nos. East Mediterr Health J 2006 Jan-Mar 12(1–2):81–87. PMID: 17037224.
Agnihotri AK, Joshi HS (2006) Pattern of road traffic injuries: one year No-based study in Western Nepal. Int J Inj Contr Saf Promot. 13(2):128 – 30. https://doi.org/10.1080/17457300500310236. PMID: 16707352
Suri MP, Naik NR, Raibagkar SC, Mehta DR (2007) Heel flap injuries in spoke wheel accidents. Injury. 38(5):619 – 24. https://doi.org/10.1016/j.injury.2007.01.004. PMID: 17472796
Ihama Y, Fuke C, Miyazaki T (2007) A two-rider motorcycle accident involving injuries around groin area in both the driver and the passenger. Leg Med (Tokyo). 9(5):274-7. https://doi.org/10.1016/j.legalmed.2007.03.003. Epub 2007 Jun 11. PMID: 17562381
Munkholm J, Thomsen AH, Lynnerup N (2007) Cyklister draebt af højresvingende lastbiler–retspatologiske fund [Fatal bicycle accidents involving right turning heavy goods vehicles–forensic pathological findings]. Ugeskr Laeger 169(3):232–235 Danish. PMID: 17234101
Doichinov ID, Spasov SS, Dobrev TS, Doichinova JA (2007) Complete decapitation of a motorcyclist in a road accident. A case report. Folia Med (Plovdiv) 49(3–4):80–83 PMID: 18504940
Kuo LC, Lin HL, Chen CW, Lee WC (2008) Traumatic hyoid bone fracture in patient wearing a helmet: a case report. Am J Emerg Med. 26(2):251.e1-2. https://doi.org/10.1016/j.ajem.2007.04.015. PMID: 18272129
Robertson J, Garrett P (2008) Paediatric motorbike injuries: do children riding motorbikes get the same injuries as those riding bicycles? ANZ J Surg. 78(7):593-6. https://doi.org/10.1111/j.1445-2197.2008.04580.x. PMID: 18593417
Alicioğlu B, Yalniz E, Eşkin D, Yilmaz B Motosiklet kazalarina bağli yaralanmalar [Injuries associated with motorcycle accidents]. Acta Orthop Traumatol Turc. 2008 Mar-Apr;42(2):106 – 11. Turkish. PMID: 18552531
Bener A, Rahman YS, Mitra B (2009) Incidence and severity of head and neck injuries in victims of road traffic crashes: in an economically developed country. Int Emerg Nurs 17(1):52–59. https://doi.org/10.1016/j.ienj.2008.07.007. Epub 2008 Sep 12. PMID: 19135016
Kosola S, Salminen P, Laine T (2009) Heading for a fall - moped and scooter accidents from 2002 to 2007. Scand J Surg. 98(3):175-9. https://doi.org/10.1177/145749690909800309. PMID: 19919924
Mohammadi G (2009) Road traffic fatalities among pedestrians, bicyclists and motor vehicle occupants in Sirjan, Kerman, Iran. Chin J Traumatol. 12(4):200-2. PMID: 19635211
Yeh HF, Seak CJ, Chiu TF, Chang YC (2009) Traumatic vertebral artery dissection and Wallenberg syndrome after a motorcycle collision. Am J Emerg Med. 27(1):131.e1-131.e3. https://doi.org/10.1016/j.ajem.2008.04.025. PMID: 19041559
Murphy J, Nyland J, Lantry J, Roberts C (2009) Motorcyclist biker couples: a descriptive analysis of orthopaedic and non-orthopaedic injuries. Injury 40(11):1195–1199. https://doi.org/10.1016/j.injury.2009.03.015. Epub 2009 Jun 13. PMID: 19524908
Fitzharris M, Dandona R, Kumar GA, Dandona L (2009) Crash characteristics and patterns of injury among Noized motorised two-wheeled vehicle users in urban India. BMC Public Health 9:11. https://doi.org/10.1186/1471-2458-9-11. PMID: 19134225; PMCID: PMC2630936
Kannus P, Parkkari J, Robinovitch S (2010) The European Standard testing method for motorcyclists’ protective clothing (EN 1621-1) is unsuitable for hip protectors. Injury 41(4):430–431 author reply 431. https://doi.org/10.1016/j.injury.2009.08.010
Talving P, Teixeira PG, Barmparas G, Dubose J, Preston C, Inaba K, Demetriades D (2010) Motorcycle-related injuries: effect of age on type and severity of injuries and mortality. J Trauma 68(2):441–446. https://doi.org/10.1097/TA.0b013e3181cbf303
Chalya PL, Mabula JB, Ngayomela IH, Kanumba ES, Chandika AB, Giiti G, Mawala B, Balumuka DD (2010) Motorcycle injuries as an emerging public health problem in Mwanza City, north-western Tanzania. Tanzan J Health Res 12(4):214–221 PMID: 24409627
Zoja R, Gentile G, Giovanetti GF, Palazzo E (2011) Death by complete decapitation of motorcyclist wearing full face helmet: case report. Forensic Sci Int 207(1–3). https://doi.org/10.1016/j.forsciint.2010.12.010. Epub 2011 Jan 26. PMID: 21269787 e48-50
Ogunlusi JD, Nathaniel C (2011) Motorcycle trauma in a St Lucian No. West Indian Med J 60(5):557–561 PMID: 22519233
Amin NH, Jakoi A, Katsman A, Harding SP, Tom JA, Cerynik DL (2011) Incidence of orthopedic surgery intervention in a level I urban trauma center with motorcycle trauma. J Trauma. 71(4):948 – 51. https://doi.org/10.1097/TA.0b013e31821e601d. PMID: 21768896
Brandimarti F, Giacomini I, Fraternale B, Giorgetti R, Tagliabracci A (2011) Massive lesions owing to motorcyclist impact against guardrail posts: analysis of two cases and safety considerations. J Forensic Sci 56(2):544–546. https://doi.org/10.1111/j.1556-4029.2010.01649.x. Epub 2011 Jan 6. PMID: 21210807
Zhao H, Chen R, Deng G, Yin Z, Yang G, Liu S, Chen H, Wang Z (2011) Comparison of injuries sustained by drivers and pillion passengers in fatal head-on motorcycle collision accidents. Forensic Sci Int 207(1–3):188–192. https://doi.org/10.1016/j.forsciint.2010.10.003. Epub 2010 Oct 28. PMID: 21030167
Ječmenica DS, Alempijević DM, Pavlekić S, Aleksandrić BV (2011) Traumatic testicular displacement in motorcycle drivers. J Forensic Sci 56(2):541–543. https://doi.org/10.1111/j.1556-4029.2010.01682.x. Epub 2011 Feb 9. PMID: 21306375
Nwadiaro HC, Ekwe KK, Akpayak IC, Shitta H (2011) Apr-Jun;14(2):186-9 Motorcycle injuries in North-Central Nigeria. Niger J Clin Pract. https://doi.org/10.4103/1119-3077.84012. PMID: 21860137
Zhu YL, Li J, Ma WQ, Mei LB, Xu YQ (2011) Motorcycle spoke injuries of the heel. Injury. 42(4):356 – 61. https://doi.org/10.1016/j.injury.2010.08.029. PMID: 20863491
de Rome L, Ivers R, Fitzharris M, Du W, Haworth N, Heritier S, Richardson D (2011) Motorcycle protective clothing: protection from injury or just the weather? Accid Anal Prev 43(6):1893–1900. https://doi.org/10.1016/j.aap.2011.04.027. Epub 2011 May 28. PMID: 21819816
Muggenthaler H, Drobnik S, Hubig M, Reiners J, Mall G (2012) Complete trunk severance of a motorcyclist by a traffic sign post at a comparably low collision speed. Forensic Sci Int 223(1–3). https://doi.org/10.1016/j.forsciint.2012.09.004. Epub 2012 Sep 28. PMID: 23022766 e35-7
Živković V, Nikolić S, Strajina V, Babić D, Djonić D, Djurić M (2012) Pontomedullary lacerations in unhelmeted motorcyclists and bicyclists: a retrospective Yes study. Am J Forensic Med Pathol. 33(4):349 – 53. https://doi.org/10.1097/PAF.0b013e318221be3c. PMID: 21659838
Heydari ST, Maharlouei N, Foroutan A, Sarikhani Y, Ghaffarpasand F, Hedjazi A, Zarenezhad M, Moafian G, Aghabeigi MR, Peymani P, Ahmadi SM, Dehghankhalili M, Joulaei H, Lankarani KB (2012) Fatal motorcycle accidents in Fars Province, Iran: a community-based survey. Chin J Traumatol 15(4):222–227 PMID: 22863339
Júnior SM, Santos SE, Kluppel LE, Asprino L, Moreira RW, de Moraes M (2012) A comparison of motorcycle and bicycle accidents in oral and maxillofacial trauma. J Oral Maxillofac Surg 70(3):577–583. https://doi.org/10.1016/j.joms.2011.03.035. Epub 2011 Jun 12. PMID: 21665346
Carrasco CE, Godinho M, Berti de Azevedo Barros M, Rizoli S, Fraga GP (2012) Fatal motorcycle crashes: a serious public health problem in Brazil. World J Emerg Surg 7(Suppl 1):S5. https://doi.org/10.1186/1749-7922-7-S1-S5. Epub 2012 Aug 22. PMID: 23531421; PMCID: PMC3424925
Bambach MR, Grzebieta RH, McIntosh AS (2012) Injury typology of fatal motorcycle collisions with roadside barriers in Australia and New Zealand. Accid Anal Prev 49:253–260. https://doi.org/10.1016/j.aap.2011.06.016. Epub 2011 Jul 20. PMID: 23036403
Zwolińska M (2013) Thermal subjective sensations of motorcyclists. Accid Anal Prev. 50:1211-20. https://doi.org/10.1016/j.aap.2012.09.021. Epub 2012 Oct 3. PMID: 23040666
Erdogan MO, Sogut O, Colak S, Ayhan H, Afacan MA, Satilmis D (2013) Roles of motorcycle type and protective clothing in motorcycle crash injuries. Emerg Med Int 2013:760205. https://doi.org/10.1155/2013/760205. Epub 2013 Nov 17. PMID: 24349787; PMCID: PMC3855950
Mosquera VX, Marini M, Muñiz J, Gulias D, Asorey-Veiga V, Adrio-Nazar B, Herrera JM, Pradas-Montilla G, Cuenca JJ (2013) Blunt traumatic aortic injuries of the ascending aorta and aortic arch: a clinical multicentre study. Injury. 44(9):1191-7. https://doi.org/10.1016/j.injury.2012.12.011. Epub 2013 Jan 4. PMID: 23294894
Hassan FH, Jajja Q (2013) An yes-based study of death due to road traffic accidents in metropolis of Karachi. J Pak Med Assoc 63(2):156–160 PMID: 23894886
Pircher R, Grosse Perdekamp M, Lutz-Bonengel S, Pollak S, Thierauf A (2013) Primarily unrecognized thoracoabdominal impalement in a motorcyclist. Forensic Sci Int 226(1–3):e37-41. https://doi.org/10.1016/j.forsciint.2013.01.026. Epub 2013 Feb 13. PMID: 23415162
Mohammadi G (2013) Road traffic crash injuries and fatalities in the city of Kerman, Iran. Int J Inj Contr Saf Promot 20(2):184–191. https://doi.org/10.1080/17457300.2012.686039. Epub 2012 May 14. PMID: 22583531
Gioia S, Suadoni F, Carlini L, Lancia M, Bacci M (2013) An unusual case of incomplete decapitation of a motorcyclist with herniation of thoracic organs through a helmet-related neck wound. Am J Forensic Med Pathol. 34(4):325-7. https://doi.org/10.1097/PAF.0000000000000060. PMID: 24189629
Meredith L, Brown J, Ivers R, De Rome L (2014) Distribution and type of crash damage to motorcyclists’ clothing: validation of the zone approach in the European Standard for motorcycle protective clothing, EN13595. Traffic Inj Prev. 15(5):501-7. https://doi.org/10.1080/15389588.2013.838672. PMID: 24678573
Edirisinghe PA, Kitulwatte ID, Senarathne UD (2014) Injuries in the vulnerable road user fatalities; a study from Sri Lanka. J Forensic Leg Med 27:9–12. https://doi.org/10.1016/j.jflm.2014.07.002. Epub 2014 Jul 25. PMID: 25287792
de Rome L, Meredith L, Ivers R, Brown J (2014) Validation of the principles of injury risk zones for motorcycle protective clothing. J Safety Res. 50:83 – 7. https://doi.org/10.1016/j.jsr.2014.04.003. Epub 2014 May 9. PMID: 25142364
Giustini M, Cedri S, Tallon M, Roazzi P, Formisano R, Pitidis A (2014) Use of back protector device on motorcycles and mopeds in Italy. Int J Epidemiol. 43(6):1921-8. https://doi.org/10.1093/ije/dyu209. PMID: 25342252
Elachi IC, Okunola BB, Yongu WT, Onyemaechi NO, Odatuwa-Omagbemi OD, Ahachi CN, Mue DD (2014) Motorcycle-related injuries at a university teaching no in north central Nigeria. Niger Med J 55(6):452–455
Hooten KG, Murad GJ (2014) Helmet use and cervical spine injury: a review of motorcycle, moped, and bicycle accidents at a level 1 trauma center. J Neurotrauma. 31(15):1329-33. https://doi.org/10.1089/neu.2013.3253. Epub 2014 Jun 3. PMID: 24661125
Paryavi E, Gilotra MN, Johnson AJ, Pensy RA, Eglseder WA, Abzug JM (2015) Upper extremity injuries in motorcyclists: Implications for mortality and need for rehabilitation services. J Trauma Acute Care Surg. 78(5):1021-5. https://doi.org/10.1097/TA.0000000000000565. PMID: 25909425
Lam C, Lin MR, Chu SF, Tsai SH, Bai CH, Chiu WT (2015) The effect of various types of motorcycle helmets on cervical spine injury in head injury patients: a multicenter study in Taiwan. Biomed Res Int 2015:487985. https://doi.org/10.1155/2015/487985. Epub 2015 Feb 1. PMID: 25705663; PMCID: PMC4330949
Kong LB, Lekawa M, Navarro RA, McGrath J, Cohen M, Margulies DR, Hiatt JR (1996) Pedestrian-motor vehicle trauma: an analysis of injury profiles by age. J Am Coll Surg 182(1):17–23 PMID: 8542084
Bambach MR, Mattos GA (2015) Head and spine injuries sustained by motorcyclists in head-leading collisions with fixed roadside objects. Traffic Inj Prev 16(2):168–176. https://doi.org/10.1080/15389588.2014.921289. Epub 2014 Oct 15. PMID: 24827754
Aikyo Y, Kobayashi Y, Akashi T, Ishiwatari M (2015) Feasibility study of airbag concept applicable to motorcycles without sufficient reaction structure. Traffic Inj Prev. 16 Suppl 1:S148-52. https://doi.org/10.1080/15389588.2015.1016156. PMID: 26027968
Chichom-Mefire A, Atashili J, Tsiagadigui JG, Fon-Awah C, Ngowe-Ngowe M (2015) A prospective pilot cohort analysis of crash characteristics and pattern of injuries in riders and pillion passengers involved in motorcycle crashes in an urban area in Cameroon: lessons for prevention. BMC Public Health 15:915. https://doi.org/10.1186/s12889-015-2290-4. PMID: 26384779; PMCID: PMC4575460
Meredith L, Baldock M, Fitzharris M, Duflou J, Dal Nevo R, Griffiths M, Brown J (2016) Motorcycle fuel tanks and pelvic fractures: a motorcycle fuel tank syndrome. Traffic Inj Prev 17(6):644–649 Epub 2016 Feb 18. PMID: 26891030
Ekmejian R, Sarrami P, Naylor JM, Harris IA (2016) A systematic review on the effectiveness of back protectors for motorcyclists. Scand J Trauma Resusc Emerg Med 24(1):115. https://doi.org/10.1186/s13049-016-0307-3. PMID: 27716409; PMCID: PMC5050611
Alexander C, Abzug JM, Johnson AJ, Pensy RA, Eglseder WA, Paryavi E (2016) Motorcyclist’s thumb: carpometacarpal injuries of the thumb sustained in motorcycle crashes. J Hand Surg Eur Vol 41(7):707–709. https://doi.org/10.1177/1753193415620186. Epub 2015 Dec 6. PMID: 26642850
Liu S, Yin Z, Su S, Li K (2016) Underbelly injury based identification of the driver in a three-rider motorcycle accident. Leg Med (Tokyo). 18:20 – 4. https://doi.org/10.1016/j.legalmed.2015.11.006. Epub 2015 Nov 24. PMID: 26832371
Bedolla J, Santelli J, Sabra J, Cabanas JG, Ziebell C, Olvey S (2016) Elite Motorcycle Racing: Crash types and Injury patterns in the MotoGP Class. Am J Emerg Med 34(9):1872–1875. https://doi.org/10.1016/j.ajem.2016.07.005. Epub 2016 Jul 6. PMID: 27431735
Lastfogel J, Soleimani T, Flores R, Cohen A, Wooden WA, Munshi I, Tholpady SS (2016) Helmet Use and Injury Patterns in Motorcycle-Related Trauma. JAMA Surg. 151(1):88–90. https://doi.org/10.1001/jamasurg.2015.3225. PMID: 26501417
Erhardt T, Rice T, Troszak L, Zhu M (2016) Motorcycle helmet type and the risk of head injury and neck injury during motorcycle collisions in California. Accid Anal Prev. 86:23 – 8. https://doi.org/10.1016/j.aap.2015.10.004. Epub 2015 Oct 22. PMID: 26496484
Rice TM, Troszak L, Ouellet JV, Erhardt T, Smith GS, Tsai BW (2016) Motorcycle helmet use and the risk of head, neck, and fatal injury: revisiting the Hurt Study. Accid Anal Prev 91:200–207. https://doi.org/10.1016/j.aap.2016.03.002. Epub 2016 Mar 19. PMID: 26998593; PMCID: PMC5360190
Faduyile F, Emiogun F, Soyemi S, Oyewole O, Okeke U, Williams O (2017) Pattern of injuries in Fatal Motorcycle accidents seen in Lagos State University Teaching No: an yes-based study. Open Access Maced J Med Sci 5(2):112–116. https://doi.org/10.3889/oamjms.2017.025. PMID: 28507612; PMCID: PMC5420758
Bell C, Prickett TRA, Rutty GN (2017) PMCT images of a motorcycle helmet-associated fracture. Forensic Sci Med Pathol 13(4):511–514. https://doi.org/10.1007/s12024-017-9911-4. Epub 2017 Sep 5. PMID: 28871386; PMCID: PMC5688187
Albanese B, Gibson T, Whyte T, Meredith L, Savino G, de Rome L, Baldock M, Fitzharris M, Brown J (2017) Energy attenuation performance of impact protection worn by motorcyclists in real-world crashes. Traffic Inj Prev 18(sup1):S116–S121. https://doi.org/10.1080/15389588.2017.1311014. Epub 2017 Apr 6. PMID: 28383999
Pelletti G, Cecchetto G, Viero A, De Matteis M, Viel G, Montisci M (2017) Traumatic fatal aortic rupture in motorcycle drivers. Forensic Sci Int 281:121–126. https://doi.org/10.1016/j.forsciint.2017.10.038. Epub 2017 Nov 6. PMID: 29127893
Araujo M, Illanes E, Chapman E, Rodrigues E (2017) Effectiveness of interventions to prevent motorcycle injuries: systematic review of the literature. Int J Inj Contr Saf Promot. 24(3):406–422. https://doi.org/10.1080/17457300.2016.1224901. Epub 2016 Oct 3. PMID: 27690735
Osculati A, Visonà SD, Della Chiesa L, Navarra F, Calbi A, Andrello L (2017) Death due to decapitation in two motorcyclists: a description of a Unique Case and a brief review of the literature. J Forensic Sci 62(3):804–806. https://doi.org/10.1111/1556-4029.13346. Epub 2016 Dec 16. PMID: 27982427
Peng Y, Vaidya N, Finnie R, Reynolds J, Dumitru C, Njie G, Elder R, Ivers R, Sakashita C, Shults RA, Sleet DA, Compton RP (2017) Community Preventive Services Task Force. Universal Motorcycle Helmet laws to reduce injuries: a community guide systematic review. Am J Prev Med 52(6):820–832. https://doi.org/10.1016/j.amepre.2016.11.030. PMID: 28526357; PMCID: PMC6918948
Page PS, Wei Z, Brooks NP (2018) Motorcycle helmets and cervical spine injuries: a 5-year experience at a level 1 trauma center. J Neurosurg Spine 28(6):607–611. https://doi.org/10.3171/2017.7.SPINE17540. Epub 2018 Mar 6. PMID: 29506463
Ostby ET, Crawley BK (2018) Helmet Clasp Cracks Larynx? A Case Series and Literature Review. Ann Otol Rhinol Laryngol. 127(4):282–284. https://doi.org/10.1177/0003489418755405. Epub 2018 Jan 31. PMID: 29383952
Saunders RN, Dull MB, Witte AB, Regan JM, Davis AT, Koehler TJ, Gibson CJ, Iskander GA, Rodriguez CH, Cohle SD, Chapman AJ (2019) The danger zone: Injuries and conditions associated with immediately fatal motorcycle crashes in the state of Michigan. Am J Surg. 217(3):552–555. https://doi.org/10.1016/j.amjsurg.2018.10.007. Epub 2018 Oct 11. PMID: 30352664
Meredith L, Albanese B, Whyte T, Gibson T, Fitzharris M, Baldock M, Brown J (2019) Assessing the performance of motorcyclists’ impact protectors in simulated ATD knee and shoulder impacts. Traffic Inj Prev 20(2):169–173. https://doi.org/10.1080/15389588.2018.1540867. Epub 2019 Mar 19. PMID: 30888879
Gioia S, Franceschetto L, Lancia M, Bacci M, Suadoni F (2019) A Case of Bilateral Extracranial Internal Carotid Artery Dissection Due to the Helmet Strap After Motorcycle Crash. Am J Forensic Med Pathol. 40(2):153–155. https://doi.org/10.1097/PAF.0000000000000458. PMID: 30624242
Bakovic M, Mažuranić A, Petrovecki V, Mayer D (2019) Fatal motorcycle crashes in wide urban area of Zagreb, Croatia-A 10-year review. Traffic Inj Prev 20(6):655–660. https://doi.org/10.1080/15389588.2019.1622007. Epub 2019 Jun 25. PMID: 31237793
de Rome L (2019) Could wearing motorcycle protective clothing compromise rider safety in hot weather? Accid Anal Prev 128:240–247. https://doi.org/10.1016/j.aap.2019.04.011. Epub 2019 May 6. PMID: 31071655
Madej-Kiełbik L, Kośla K, Zielińska D, Chmal-Fudali E, Maciejewska M (2019) Effect of Accelerated Ageing on the Mechanical and Structural properties of the material system used in protectors. Polym (Basel) 11(8):1263. https://doi.org/10.3390/polym11081263. PMID: 31366100; PMCID: PMC6723406
Petetta C, Santovito D, Tattoli L, Melloni N, Bertoni M, Di Vella G (2020) Forensic and Clinical Issues in a Case of Motorcycle Blunt Trauma and Bilateral Carotid Artery Dissection. Ann Vasc Surg. 64:409.e11-409.e16. https://doi.org/10.1016/j.avsg.2019.10.049. Epub 2019 Oct 23. PMID: 31655108
Cheong HS, Tham KY, Chiu LQ (2021) Injury patterns in elderly cyclists and motorcyclists presenting to a tertiary trauma centre in Singapore. Singap Med J 62(9):482–485. https://doi.org/10.11622/smedj.2020038. Epub 2020 Mar 25. PMID: 32211913; PMCID: PMC9251234
Jia M, Li Z, Zhang J, Huang P, Wang J, Zou D, Tao L, Chen Y (2020) Finite element analysis to determine the cause of ring fractures in a motorcyclist’s head. Leg Med (Tokyo). 45:101697. https://doi.org/10.1016/j.legalmed.2020.101697. Epub ahead of print. PMID: 32305675
Medina O, Singla V, Liu C, Fukunaga D, Rolfe K (2020) Patterns of spinal cord injury in automobiles versus motorcycles and bicycles. Spinal Cord Ser Cases 6(1):75. https://doi.org/10.1038/s41394-020-00324-y. PMID: 32820149; PMCID: PMC7441156
Afquir S, Melot A, Ndiaye A, Hammad E, Martin JL, Arnoux PJ (2020) Descriptive analysis of the effect of back protector on the prevention of vertebral and thoracolumbar injuries in serious motorcycle accident. Accid Anal Prev 135:105331. https://doi.org/10.1016/j.aap.2019.105331. Epub 2019 Nov 18. PMID: 31751784
Lepard JR, Spagiari R, Corley J, Barthélemy EJ, Kim E, Patterson R, Venturini S, Still MEH, Lo YT, Rosseau G, Mekary RA, Park KB (2021) Differences in outcomes of mandatory motorcycle helmet legislation by country income level: a systematic review and meta-analysis. PLoS Med 18(9):e1003795. https://doi.org/10.1371/journal.pmed.1003795. PMID: 34534215; PMCID: PMC8486090
Kleinertz H, Ntalos D, Hennes F, Nüchtern JV, Frosch KH, Thiesen DM (2021) Accident mechanisms and Injury patterns in E-Scooter Users–A retrospective analysis and comparison with cyclists. Dtsch Arztebl Int 118(8):117–121. https://doi.org/10.3238/arztebl.m2021.0019. PMID: 33879309; PMCID: PMC8204371
Mohd Saman SA, Jothee S, Nor FM, Shafie MS (2021) The Pattern of Injuries Among Motorcyclists in Fatal Road Traffic Accidents: An Yes-Based Study. Am J Forensic Med Pathol. 42(2):141–146. https://doi.org/10.1097/PAF.0000000000000639. PMID: 33346978
Cravez E, Rankin KA, Ondeck N, Yaari L, Leslie M, Swigart C, Wiznia DH (2021) Motorcycle crashes and upper extremity trauma. SICOT J 7:8. https://doi.org/10.1051/sicotj/2021007. Epub 2021 Mar 8. PMID: 33683193; PMCID: PMC7938721
Barron S, Falank C, Ontengco J, Chung B, Carter DW (2021) Severity and patterns of injury in helmeted vs. non-helmeted motorcyclists in a rural state. J Saf Res 77:212–216. https://doi.org/10.1016/j.jsr.2021.03.004. Epub 2021 Mar 20. PMID: 34092311
Gentile G, Tambuzzi S, Giovanetti G, Zoja R (2021) Sudden death due to cardiac contusion: forensic implications in a rare pediatric case. J Forensic Sci 66(5):1996–2001. https://doi.org/10.1111/1556-4029.14741. Epub 2021 May 7. PMID: 33960426; PMCID: PMC8453835
Martins RS, Saqib SU, Gillani M, Sania SRT, Junaid MU, Zafar H (2021) Patterns of traumatic injuries and outcomes to motorcyclists in a developing country: a cross-sectional study. Traffic Inj Prev 22(2):162–166. doi: https://doi.org/10.1080/15389588.2020.1856374. Epub 2021 Jan 26. PMID: 33497294
Tabary M, Ahmadi S, Amirzade-Iranaq MH, Shojaei M, Sohrabi Asl M, Ghodsi Z, Azarhomayoun A, Ansari-Moghaddam A, Atlasi R, Araghi F, Shafieian M, Heydari ST, Sharif-Alhoseini M, O’Reilly G, Rahimi-Movaghar V (2021) The effectiveness of different types of motorcycle helmets - a scoping review. Accid Anal Prev 154:106065. https://doi.org/10.1016/j.aap.2021.106065. Epub 2021 Mar 6. PMID: 33689958
Whyte T, Kent N, Cernicchi A, Brown J (2022) Mitigating fuel tank syndrome pelvic injuries - is there potential for rider worn protectors? Traffic Inj Prev 23(sup1):S50–S55. https://doi.org/10.1080/15389588.2022.2072834. Epub 2022 Jun 10. PMID: 35687036
Kent T, Miller J, Shreve C, Allenback G, Wentz B (2022) Comparison of injuries among motorcycle, moped and bicycle traffic accident victims. Traffic Inj Prev 23(1):34–39. https://doi.org/10.1080/15389588.2021.2004311. Epub 2021 Dec 22. PMID: 34936538
Lusetti A, Dagoli S, Banchini A, Gentile M, Lezzi P, Cecchi R (2022) Over 30-year retrospective analyses of moped-motorcycle fatal road accidents in the northern area of the Italian region of Emilia Romagna and review of the literature: aiming for further preventive measures in the future. Leg Med (Tokyo) 59:102139. https://doi.org/10.1016/j.legalmed.2022.102139. Epub 2022 Aug 22. PMID: 36055135
He WQ, Wu J, Cai ZB (2022) LX. Analysis of Thoracic Aorta Injury in 27 Road Traffic Accident Deaths. Fa Yi Xue Za Zhi. 38(4):486–489. English, Chinese. https://doi.org/10.12116/j.issn.1004-5619.2020.410502. PMID: 36426692
Urréchaga EM, Kodadek LM, Bugaev N, Bauman ZM, Shah KH, Abdel Aziz H, Beckman MA, Reynolds JM, Soe-Lin H, Crandall ML, Rattan R (2022) Full-face motorcycle helmets to reduce injury and death: a systematic review, meta-analysis, and practice management guideline from the Eastern Association for the surgery of Trauma. Am J Surg 224(5):1238–1246. https://doi.org/10.1016/j.amjsurg.2022.06.018. Epub 2022 Jul 7. PMID: 35821175
Rauer T, Aschwanden A, Rothrauff BB, Pape HC, Scherer J (2023) Fractures of the Lower Extremity after E-Bike, Bicycle, and Motorcycle accidents: a retrospective cohort study of 624 patients. Int J Environ Res Public Health 20(4):3162. https://doi.org/10.3390/ijerph20043162. PMID: 36833856; PMCID: PMC9959038
Liasidis P, Benjamin E, Jakob D, Lewis M, Demetriades D (2023) Injury patterns and outcomes in motorcycle passengers. Eur J Trauma Emerg Surg. Jun 27. https://doi.org/10.1007/s00068-023-02296-8. Epub ahead of print. PMID: 37367970
Kleinertz H, Volk A, Dalos D, Rutkowski R, Frosch KH, Thiesen DM (2023) Risk factors and injury patterns of e-scooter associated injuries in Germany. Sci Rep 13(1):706. https://doi.org/10.1038/s41598-022-25448-z. PMID: 36639664; PMCID: PMC9837749
Meng S, Ivarsson P, Lubbe N (2023) Evaluation of full-face, open-face, and airbag-equipped helmets for facial impact protection. Accid Anal Prev. 191:107181. https://doi.org/10.1016/j.aap.2023.107181. Epub 2023 Jul 5. PMID: 37418868
Viano DC, King AI, Melvin JW, Weber K (1989) Injury biomechanics research: an essential element in the prevention of trauma. J Biomech. 22(5):403 – 17. https://doi.org/10.1016/0021-9290(89)90201-7. PMID: 2674145
Kondo T, Saito K, Nishigami J (1995) Fatal injuries of the brain stem and/or upper cervical spinal cord in traffic accidents: nine yes cases. Sci Justice 35(3):197–201
Gunji H, Mizusawa I, Hiraiwa K (2002) The mechanism underlying the occurrence of traumatic brainstem lesions in victims of traffic accidents. Leg Med (Tokyo). 4(2):84 – 9. https://doi.org/10.1016/s1344-6223(02)00012-3. PMID: 12935674
Imamura T, Kojima T, Yashiki M, Namera A (2000) Traumatic avulsion fracture of the occipital condyles and clivus: a case report. Leg Med (Tokyo). 2(1):49–53. https://doi.org/10.1016/s1344-6223(00)80010-3. PMID: 12935467
Keenan HT, Brundage SI, Thompson DC, Maier RV, Rivara FP (1999) Does the face protect the brain? A case-control study of traumatic brain injury and facial fractures. Arch Surg. 134(1):14 – 7. https://doi.org/10.1001/archsurg.134.1.14. PMID: 9927123
Haug RH, Adams JM, Conforti PJ, Likavec MJ (1994) Cranial fractures associated with facial fractures: a review of mechanism, type, and severity of injury. J Oral Maxillofac Surg. 52(7):729 – 33. https://doi.org/10.1016/0278-2391(94)90488-x. PMID: 8006737
Lee WW, Jensen ER (2000) Bilateral internal carotid artery dissection due to trivial trauma. J Emerg Med. 19(1):35–41. https://doi.org/10.1016/s0736-4679(00)00190-6. PMID: 10863116
Johnson CP, How T, Scraggs M, West CR, Burns J (2000) A biomechanical study of the human vertebral artery with implications for fatal arterial injury. Forensic Sci Int. 109(3):169 – 82. https://doi.org/10.1016/s0379-0738(99)00198-x. PMID: 10725653
Richens D, Field M, Neale M, Oakley C (2002) The mechanism of injury in blunt traumatic rupture of the aorta. Eur J Cardiothorac Surg. 21(2):288 – 93. https://doi.org/10.1016/s1010-7940(01)01095-8. PMID: 11825737
Shah KN (2010) The diagnostic and clinical significance of café-au-lait macules. Pediatr Clin North Am. 57(5):1131-53. https://doi.org/10.1016/j.pcl.2010.07.002. PMID: 20888463
Petit L, Zaki T, Hsiang W, Leslie MP, Wiznia DH (2020) A review of common motorcycle collision mechanisms of injury. EFORT Open Rev 5(9):544–548. https://doi.org/10.1302/2058-5241.5.190090. PMID: 33072406; PMCID: PMC7528667
WHO. Motorcycle helmet laws, by occupant-Data by country (2020) https://apps.who.int/gho/data/view.main.51427
Cooter RD (1990) Computed tomography in the assessment of protective helmet deformation. J Trauma. 30(1):55–68. https://doi.org/10.1097/00005373-199001000-00009. PMID: 2296068
UNECE (2021) UN Regulation No. 22 - Rev.5–06 series. 2021. Agreement concerning the Adoption of Harmonized Technical United Nations Regulations for Wheeled Vehicles, Equipment and Parts which can be Fitted and/or be Used on Wheeled Vehicles and the Conditions for Reciprocal Recognition of Approvals Granted on the Basis of these United Nations Regulations. https://unece.org/transport/documents/2021/08/standards/un-regulation-no-22-rev5-06-series. Accessed 28 april 2024
Giovannini E, Giorgetti A, Pelletti G, Giusti A, Garagnani M, Pascali JP, Pelotti S, Fais P (2021) Importance of dashboard camera (dash cam) analysis in fatal vehicle-pedestrian crash reconstruction. Forensic Sci Med Pathol 17(3):379–387. https://doi.org/10.1007/s12024-021-00382-0. Epub 2021 May 19. PMID: 34013466; PMCID: PMC8413177
Santelli S, Berti L, Giovannini E, Pelletti G, Pelotti S, Fais P (2023) Homicide, suicide, or accident? Complex differential diagnosis. A case series. Leg Med (Tokyo). 66:102357. https://doi.org/10.1016/j.legalmed.2023.102357. Epub ahead of print. PMID: 37984052
Funding
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Open access funding provided by Alma Mater Studiorum - Università di Bologna within the CRUI-CARE Agreement.
Author information
Authors and Affiliations
Contributions
EG: conceptualization, writing-original draft; SS: methodology; data curation; GP: data curation, writing-review & editing; MPB: writing-original draft, methodology; EL: data curation; formal analysis; SP: writing-review & editing, supervision; PF: conceptualization, supervision.
Corresponding author
Ethics declarations
Ethical approval
No approval of an ethical committee is needed for this type of study.
Human Ethics and Consent to participate declarations
Not applicable.
Consent for publication
All authors have read and approved the final version of the manuscript.
Competing interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Giovannini, E., Santelli, S., Pelletti, G. et al. Motorcycle injuries: a systematic review for forensic evaluation. Int J Legal Med (2024). https://doi.org/10.1007/s00414-024-03250-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s00414-024-03250-y