
Abstract
Introduction
Extra-articular calcaneal fractures represent 25–40% of all calcaneal fractures and an even higher percentage of up to 60% is seen in children. A disproportionately small part of the literature on calcaneal fractures involves the extra-articular type. The aim of this study was to investigate the incidence of extra-articular calcaneal fractures in a Level 1 trauma centre, define the distribution of the various types of fractures and compare patient demographics between extra- and intra-articular calcaneal fractures. In addition the literature was reviewed for the most common types of extra-articular calcaneal fractures with regard to incidence, treatment and clinical outcome.
Methods
The radiological records between 2003 and 2005 were reviewed for intra- and extra-articular calcaneal fractures. Patient gender-distribution and age were compared. A literature search was conducted for the treatment of extra-articular calcaneal fractures.
Results
In this 3-year study period a total of 49 patients with 50 extra-articular calcaneal fractures and 91 patients with 101 intra-articular fractures were identified. The median age for the first group was 32.7 years, and for the second group 40.3 years; P = 0.04. Male predominance was significantly less pronounced for extra-articular (63%) compared with intra-articular fractures (79%; P = 0.04).
Conclusion
One-third of all calcaneal fractures are extra-articular. Significant differences exist between the intra- and extra-articular groups, in terms of lower age and male–female ratio. The literature study shows inconsistencies in treatment options, but most extra-articular fractures are well manageable conservatively.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The proportion of calcaneal fractures without involvement of the posterior subtalar joint in adults is reported to be approximately 25% [4, 12, 26]. In children this number is higher and ranges from 25 to 63%, with increased percentages at lower age [14, 41, 67]. A disproportionately small part of the literature on calcaneal fractures involves the extra-articular type [17]. Controversy exists in the treatment of calcaneal fractures in general, but to a lesser extent in the extra-articular type compared with intra-articular calcaneal fractures [47].
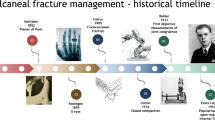
Extra-articular fractures of the calcaneus are compression or avulsion type fractures. According to several classifications, i.e. by Böhler [8], Essex-Lopresti [26] and others [66, 67, 73], they are historically divided into three different groups: anterior portion, tuberosity (posterior calcaneal) and sustentaculum tali fractures (Table 1, Fig. 1). Several decades later additional calcaneal avulsion fractures of the calcaneus were identified [13, 55, 58].

Combined classification of extra-articular calcaneal fractures according to several authors (Table 1). 1 Undisplaced (1a) beak fracture; undisplaced (1b) avulsion fracture at Achilles-tendon insertion site; displaced (1c) “beak” avulsion fracture postero-superior aspect tuberosity; 2 medial (2a) or lateral (2b) process fracture; 3 isolated sustentaculum tali fracture; 4a vertical fracture; 4b, apophysis avulsion fracture; 5a, anterior superior avulsion or compression fracture; 5b, calcaneocuboid joint fracture; 5c, distal inferolateral portion fracture; 6a, extensor digitorum avulsion fracture; 6b, plantar fascia avulsion fracture; 6c, posterior capsular avulsion fracture
The aim of the current study was to assess the incidence of different types of extra-articular calcaneal fractures in a Level-1 trauma centre, and comparing patients with an extra- or intra-articular fracture. In addition, a review of the literature was conducted concerning the incidence, treatment and outcome of common extra-articular calcaneal fractures.
Patients and methods
Patients
All radiological records between January 1, 2003 and December 31, 2005 were electronically reviewed for the combination “calcaneus” AND “fracture” (in Dutch) at a Level 1 Trauma centre, with ∼24,000 patients presenting at the ED annually. The starting point of this search coincided with the introduction of digital radiographs [Picture Archiving and Communication System PACS]. These records were reviewed manually and when a fracture of the calcaneus was suspected, the original radiographs were re-examined by two reviewers (TS, AG). Patient who had radiographs taken on more than one occasion, were included only once.
Fractures of the calcaneus were classified as extra- or intra-articular, with involvement of the posterior talocalcaneal joint in the latter. The extra-articular fractures were further divided into anterior calcaneal portion fractures (anterior process, calcaneocuboid joint fractures), sustentaculum tali fractures (mid calcaneal portion) posterior calcaneal portion fractures (tuberosity avulsion, vertical, lateral and medial process fractures) and a group consisting of various avulsion fractures.
Statistical analysis
Statistical analysis was performed using the Statistical Package for the Social Sciences (SPSS) version 12.0 (SPSS, Chicago, IL, USA). The median age between groups was compared with the non-parametric Mann–Whitney U test. The difference in gender distribution and number of bilateral fractures between groups was analysed using the Chi-square test. Correlations were considered statistically significant with a P value of <0.05.
Literature search
The literature was reviewed for the various types of extra-articular calcaneal fractures; their incidence, treatment and outcome. This search was conducted in the electronic databases of Embase, Cochrane Library and Pubmed using the following search-terms and Boolean operators: (“calcaneus” or “os calcis” or “calcaneum” OR “calcaneal”) and “fracture(s)” and/or “avulsion” and/or “extra-articular” up to July 2007. In addition a hand search of reference lists of eligible manuscripts and review articles was conducted to identify additional studies.
Results
Patients
A total of 540 patients with the terms “calcaneus” AND “fracture” mentioned in their radiological records were retrieved in the three year study period. In 140 cases a fracture of the calcaneus was encountered and in an additional 97 patients a calcaneal fracture was sustained prior to the investigatory period; meaning these were control radiographs to assess healing or in cases with persisting physical complaints. These patients were excluded from further analysis.
Out of the 140 patients with a calcaneal fracture, 49 patients sustained 50 extra-articular fractures. The different types of extra-articular calcaneal fractures and their frequency of appearance are shown in Table 2. The most commonly encountered extra-articular calcaneal fractures were the anterior process (n = 19), the extensor digitorum brevis avulsion (n = 8) and tuberosity medial process fractures (n = 8).
Patients with an intra-articular fracture had a median age of 40.3 years, compared with those with an extra-articular fracture 32.7 (P = 0.04). The proportion of male patients was 79% in the first group, and in 63% the latter. This difference was statistically significant (P = 0.04). A total of ten patients with an intra-articular fracture sustained a bilateral fracture (11%), in the extra-articular group one patient (2%) sustained a bilateral fracture (P = 0.06).
Literature review
Calcaneal tuberosity fractures
Hippocrates already described tuberosity fractures of the calcaneus, resulting in gangrene and death if treated wrongly [25]. These fractures can be divided into avulsion (“beak” and Achilles avulsion) and shear-compression (vertical, lateral and medial process) fractures, although combinations have been described [68]. Tuberosity fractures, mainly shear-compression, comprise 12–40% of all calcaneal fractures encountered [9, 26, 73].
Fractures of the tuberosity result mainly from a fall from height or striking the heel on a ledge (Fig. 2a, b) [9]. Medial process fractures are thought to be the first stage of complex fractures [68], but can occur as avulsion fractures of the medial plantar fascia insertion [26] or abductor hallucis muscle insertion at the medial process [58]. Lateral process fractures and trochlear process fractures are rare [53].

Examples of several subtypes of extra-articular calcaneal fractures. a Medial process fracture, b vertical tuberosity fracture, c anterior process (Degan type I) fracture, d avulsion fracture at the insertion site of the extensor digitorum brevis muscle
The avulsion fractures of the postero-superior portion of the tuberosity (“beak” fractures) are caused by contraction of the calf-muscles while landing on the forefoot [20, 70]. Instead of rupturing the Achilles-tendon a fragment of approximately 2–3 cm is avulsed of the calcaneus (“Boyer fracture”) [6, 16, 26, 70]. Fractures alike type 1a are probably caused by deeper fibres of the soleus muscle, tilting the fragment upwards or by a more proximal insertion of the Achilles-tendon, as the Achilles-tendon usually inserts at level 1b (Fig. 1) [48, 62]. These avulsion fractures are more common in elderly women, in which osteoporosis plays an important role [6, 24, 44, 48, 57, 62, 65, 68, 70]. Other trauma mechanisms for the avulsion fracture are isolated muscle contractions, as seen in an athlete starting a run, or by direct trauma to the heel [32].
Two additional distinct avulsion fracture types of the tuberosity exist, namely the neuropathic Charcot-like fractures in diabetics and avulsion fractures of the apophysis of the calcaneus [2, 6, 35, 43, 50, 52]. The type 1 “Iowa fracture” according to Hedlund et al. [35] is an extra-articular tuberosity avulsion fracture near the insertion of the Achilles-tendon, occurring in patients with a history of diabetes.
The epiphysiolysis, a Salter-Harris type III fracture, occurs in children [2, 7, 40, 52]. It can be mistaken for Severs’ disease (apophysitis by repeated stress) if the fracture is not displaced [7].
Tuberosity avulsion fractures treated inadequately lead to stiffness, pain en swelling at the insertion site of the Achilles-tendon. Residual complaints after conservative treatment are muscle weakness especially in plantar flexion, resulting in difficulty in climbing stairs or while walking on toes [6, 62]. Most displaced tuberosity avulsion fractures are treated by open reduction and internal fixation (ORIF) with (tension-)wiring or screw fixation and an after-treatment in a above or below-knee cast for 4 or more weeks with the foot in plantar flexion (Table 3). Patients with low physical demands or fractures with minimally displaced fractures are manageable with conservative treatment [62, 65]. Medial process and minimally displaced vertical tuberosity fractures are managed conservatively with satisfactory outcome [53, 68].
Sustentaculum tali fractures
One of the earliest descriptions of sustentacular fractures was by Abel in 1878, who described three cases by direct force [25]. Isolated fractures of the sustentaculum tali are rare. Their incidence ranges from 0.3 to 4% [9, 26, 67, 73].
According to Essex-Lopresti the sustentaculum tali fracture is an intra-articular one, whereas all other classifications group the sustentacular fractures as extra-articular [26, 66, 67]. Treatment of isolated sustentaculum tali fractures is usually conservative with satisfactory results, as the sustentaculum tali remains in position by strong fixation to the talus by the deltoid ligament and the interosseous ligament [8, 15, 17, 31, 37, 72].
Anterior process fractures
The anterior process is a bony prominance situated at the anterior-superior front of the os calcis and goes by several names [30, 33]. It is connected to both the cuboid and the navicular bone through the bifurcate ligamant [21]. Anterior process, or anterior-superior promontory, fractures (Fig. 2c) are overlooked or misdiagnosed as ankle-sprains in up to 40% of the cases in the Emergency Department [5, 21, 27, 28, 30, 42, 46, 71]. Anterior process fractures represent 8–13% of all calcaneal fractures [26, 73]. Approximately 5% of patients with the history of an ankle-sprain has an anterior processus fracture, with a predominance in women [1, 10, 18, 27, 28, 54, 56].
Almost simultaneously Drachtler and Christopher reported this type of fracture for the first time in 1931 [18, 28, 64]. Different trauma mechanisms were postulated: forcible plantar-flexion (inversion-adduction, equinovarus, supination) of the foot [5, 10, 18, 21, 28, 30] and, less common, dorsiflexion–eversion trauma or forcefull abduction of the forefoot with the heel fixed to the ground [21, 27, 61]. The first mechanism results in a avulsion fracture, the latter in a compression fracture [21]. Concomitant occurance of additonal injuries (talar, navicular, cuboid and calcaneal fracture or ligamental injuries) or calcaneo-navicular coalition are seen frequently [56, 59].
Clinical presentation includes: immediate pain at the dorsolateral side of the foot, losing the ability to bear weight after a few hours, swelling and later discoloration [10]. Tenderness is usually found by placing the thumb on the lateral malleolus and the third digit on the base of the fifth metatarsal, with the index finger pointing out the area of maximum pain (“Gellman grip”) [28].
Radiographic investigation involves a lateral view of the calcaneus and a 45° inverted oblique view or a 10°–15° cephalad, 10°–15° posterior view [27, 61]. Other views are less sensitive [63]. If there is high suspectancy magnetic resonance imaging can be considered [56, 64]. The anterior process fracture must be distuinguised from a calcaneus secundarius, which can be found in 2–5% on autopsy [36, 38, 39, 51]. Others consider the secondary ossicle to be a non-united anterior process fracture [64]. The fractures can be divided into three types according to Degan: Type I; an undisplaced fracture of only the tip of the anterior process, type II; displaced fracture of the anterior process not involving the calcaneocuboid joint, type III; large displaced fracture involving the calcaneocuboid joint [21]. Type I and II are sprain-fractures caused by inversion trauma, and type III is a compression fracture [61].
A successful treatment of anterior process fractures relies almost completely on the early detection of the fracture [10]. If not treated well this injury can cause persistent complaints for up to 18 months [46]. Conservative treatment, usually with a short leg cast for 4 weeks and increased weight-bearing, results in satisfactory outcome in most cases (Table 4) [10, 21, 36, 64]. In Degan type III fractures ORIF can be considered [39, 71]. The two most prognostic features of outcome are the type of injury and whether the fracture unites [21]. Overall outcome is satisfactory, but non-union rates range from zero to 40%, depending on adequately made diagnosis and treatment [21, 28, 64]. “It is such injuries that very probably lead to the well-known expression that a bad sprain is worse than a fracture” [63].
Anterior avulsion fractures
The extensor digitorum brevis originates from the dorsolateral portion of the anterior portion of the calcaneus, and inserts at the lateral sides of the extensor digitorum longus tendons of the second to fourth toe, extending them with the foot in dorsal flexion.
If the foot is subjected to forceful inversion an avulsion fracture of the insertion of the extensor muscle may occur (Fig. 2d). Clinically it is difficult to distinguish between an anterior process (avulsion) fracture and an extensor digitorum brevis insertion avulsion fracture [34]. The haematoma, the point of maximum swelling and the point of maximum tenderness are situated in the same area as in anterior process fractures [55].
Norfray et al. [55] found 10 cases in a series of 100 consecutive patients suspected for an ankle fracture. The avulsion fracture was best seen at the dorsoplantar view of the foot and on the anteroposterior view of the ankle. An additional view recommended is the reversed oblique view of the foot, with the foot in approximately 35°–40° exorotation, e.g. supination [13, 29]. Brijs identified 62 avulsions of the antero-lateral aspect of the calcaneus, situated more peripherally than fractures caused by avulsion of the extensor digitorum brevis. Brijs [13] suggested that these small fractures are caused by avulsions at the insertion site of the bifurcate ligament. Usually the avulsion is an isolated fracture and avulsed fragments resolved within a few months [11, 13, 29, 55]. Treatment is usually conservatively consisting of 2 weeks non-weight bearing, bandaging and early active motion exercises, and outcome is favourable in all patients [13, 29, 55].
Discussion
Thirty-five percent of all calcaneal fractures in the current study occurred outside the posterior subtalar joint. This percentage is slightly higher than previous incidences presented in the literature [4, 12, 26]. These percentages were calculated before the description of various types of avulsion fractures and might have been underscoring the number of extra-articular calcaneal fractures [13, 55].
Patients with an extra-articular calcaneal fractures were significantly younger, male predominance was less pronounced and the occurrence of a bilateral extra-articular calcaneal fractures is lower. This is explained largely by the difference in trauma-mechanism. The intra-articular calcaneal fractures occur frequently as work-related high-energy accidents and the extra-articular mainly as distortion injuries [5, 10, 18, 21, 28, 30, 55].
A total of 66 tuberosity avulsion fractures were retrieved from the literature, including four epiphysiolyses. Patients treated conservatively reached a satisfactory result in 64% compared with 88% of patients treated operatively. Patients return to their daily activities earlier after operative treatment. No randomised trials exist on the subject and half of the patients were not available for follow-up. Nevertheless the tendency nowadays is to operate these avulsion fractures.
Some 268 cases with an anterior process fractures were identified, with 90% of the patients reaching satisfactory result after conservative treatment. As fragments are usually too small to fixate, operative treatment is not treatment of choice. Important in obtaining best outcome is an early detection of the injury and adequate immobilisation.
The 78 anterior avulsion fractures from the insertion of the extensor digitorum brevis muscle or bifurcate ligament described in the literature did well in 100% after conservative treatment, and only one large fragment was corrected operatively.
Conclusion
One-third of the calcaneal fractures are extra-articular. Statistically significant differences exist in patient characteristics, age and gender, between the intra- and extra-articular fractures. Evidence-based treatment options of extra-articular calcaneal fractures do not exist. Due to the low incidence of this type of fractures only retrospective case series and one prospective study regarding treatment options were found in the literature. Most extra-articular calcaneal fractures can be treated conservatively with overall satisfactory results. Displaced posterior superior avulsion fractures, displaced medial process and vertical fractures of the tuberosity and large anterior process fractures are best treated by ORIF according to the available literature.
References
Agnholt J, Nielsen S, Christensen H (1988) Lesion of the ligamentum bifurcatum in ankle sprain. Arch Orthop Trauma Surg 107(5):326–328
Alvarez Fernandez JL, Villalba Vaquero M, Gomez Cimiano J (1989) Epiphysiolysis of the great tuberosity of the calcaneum: brief report. J Bone Joint Surg Br 71(2):321
Arner O, Lindholm A (1959) Avulsion fracture of the os calcaneus. Acta Chir Scand 117:258–260
Atkins RM, Allen PE, Livingstone JA (2001) Demographic features of intra-articular fractures of the calcaneum. Foot Ankle Surg 7:77–84
Backman S, Johnson SR (1953) Torsion of the foot causing fracture of the anterior calcaneal process. Acta Chir Scand 105(6):460–466
Biehl WC 3rd, Morgan JM, Wagner FW Jr, Gabriel R (1993) Neuropathic calcaneal tuberosity avulsion fractures. Clin Orthop Relat Res 296:8–13
Birtwistle SJ, Jacobs L (1995) An avulsion fracture of the calcaneal apophysis in a young gymnast. Injury 26(6):409–410
Böhler L (1931) Diagnosis, pathology and treatment of fractures of the os calcis. J Bone Joint Surg 1:75–89
Böhler L (1957) Die Technik der Knochenbruchbehandlung. Verlag Wilhelm Maudrich, Wien Band II, pp 2148–2217
Bradford CH, Larsen I (1951) Sprain-fractures of the anterior lip of the os calcis. N Engl J Med 244(26):970–972
Brandser E, Braksiek R, El-Khoury G, Saltzman C, Marsh J, Clark W, Prokuski L (1997) Missed fractures on emergency room radiographs: an analysis of 433 patients. Emerg Radiol 4(5):295–302
Bremner AE, Warrick CK (1951) Fractures of the calcaneus. J Fac Radiol 2(3):235–241
Brijs S, Brijs A (1992) Calcaneal avulsion: a frequent traumatic foot lesion. Rofo 156(5):495–496
Brunet JA (2000) Calcaneal fractures in children. Long-term results of treatment. J Bone Joint Surg Br 82(2):211–216
Burdeaux BD Jr (1993) The medial approach for calcaneal fractures. Clin Orthop Relat Res 290:96–107
Cahill GF (1917) Fractures of the os calcis. Ann Surg 66(6):711–717
Carey DJ, Lance EM, Wade PA (1965) Extra-articular fractures of the os calcis—a follow-up study. J Trauma 8:362–372
Christopher F (1931) Fracture of the anterior process of the calcaneus. J Bone Joint Surg Am 1:877–879
Cole RJ, Brown HP, Stein RE, Pearce RG (1995) Avulsion fracture of the tuberosity of the calcaneus in children. A report of four cases and review of the literature. J Bone Joint Surg Am 77(10):1568–1571
Coote H (1867) Fracture of the os calcis from muscular action. Lancet 89(2270):270–271
Degan TJ, Morrey BF, Braun DP (1982) Surgical excision for anterior-process fractures of the calcaneus. J Bone Joint Surg Am 64(4):519–524
Dieterle J (1940) A case of so-called “open-beak” fracture of the os calcis. J Bone Joint Surg Am 2:740
Drachtler H (1931) Fractures of the anterior superior portion of the os calcis due to indirect violence. Am J Roentgenol 25(5):629–631
Eisendrath DN (1905) Fractures of the tarsal bones. Ann Surg 41(3):363–371
Ely LW (1906) Old fracture of the tarsus. Ann Surg 45(1):69–89
Essex-Lopresti P (1952) Mechanism, reduction technique and results in fractures of os calcis. Br J Surg 3:395–419
Garvin EJ, Rominger CJ (1957) Fractures of the anterior process of the calcaneus. Am J Surg 94(3):468–471
Gellman M (1951) Fractures of the anterior process of the calcaneus. J Bone Joint Surg Am 33-A(2):382–386
Geusens E, Geyskens W, Brys P, Janzing H (2000) The role of the reversed oblique radiograph in trauma of the foot and ankle. Eur Radiol 10(3):476–479
Gilheany M (2002) Injuries to the anterior process of the calcaneum. Foot 1:142–149
Gilmer PW, Herzenberg J, Frank JL, Silverman P, Martinez S, Goldner JL (1986) Computerized tomographic analysis of acute calcaneal fractures. Foot Ankle 6(4):184–193
Glanzmann M, Vereb L, Habegger R (2005) [Avulsion fracture of the calcaneal tuberosity in athletes]. Unfallchirurg 108(4):325–326
Golder WA (2004) Anterior process of the calcaneus: a clinical–radiological contribution to anatomical vocabulary. Surg Radiol Anat 26(3):163–166
Hall FM (1999) Calcaneal avulsion fractures. AJR Am J Roentgenol 173(3):854–855
Hedlund LJ, Maki DD, Griffiths HJ (1998) Calcaneal fractures in diabetic patients. J Diabetes Complications 12(2):81–87
Hellpap W (1962) Bone injuries of the anterior calcaneus process. Arch Orthop Unfallchir 5:329–338
Herzenberg JE (1986) CT of calcaneal fractures. AJR Am J Roentgenol 146(3):644–645
Hodge JC (1999) Anterior process fracture or calcaneus secundarius: a case report. J Emerg Med 17(2):305–309
Hunt DD (1970) Compression fracture of the anterior articular surface of the calcaneus. J Bone Joint Surg Am 52(8):1637–1642
Imai Y, Kitano T, Nakagawa K, Takaoka K (2007) Calcaneal apophyseal avulsion fracture. Arch Orthop Trauma Surg 127(5):331–333
Inokuchi S, Usami N, Hiraishi E, Hashimoto T (1998) Calcaneal fractures in children. J Pediatr Orthop 18(4):469–474
Judd DB, Kim DH (2002) Foot fractures frequently misdiagnosed as ankle sprains. Am Fam Physician 66(5):785–794
Kathol MH, el-Khoury GY, Moore TE, Marsh JL (1991) Calcaneal insufficiency avulsion fractures in patients with diabetes mellitus. Radiology 180(3):725–729
Levi N, Garde L, Kofoed H (1997) Avulsion fracture of the calcaneus: report of a case using a new tension band technique. J Orthop Trauma 11(1):61–62
Levine J, Kenin A, Spinner M (1959) Nonunion of a fracture of the anterior superior process of the calcaneus; case report. J Bone Joint Surg Am 41-A(1):178–180
Lindsay WR, Dewar FP (1958) Fractures of the os calcis. Am J Surg 95(4):555–576
Lowery RB, Calhoun JH (1996) Fractures of the calcaneus. Part II: Treatment. Foot Ankle Int 17(6):360–366
Lowy M (1969) Avulsion fractures of the calcaneus. J Bone Joint Surg Br 51(3):494–497
Lyngstadaas S (1971) Treatment of avulsion fractures of the tuber calcanei. Acta Chir Scand 137(6):579–581
Matsumura H, Jimbo Y, Kato T, Imai S (1998) Spontaneous calcaneal fracture after deep heel burns with diabetes. Burns 24(7): 683–686
Mercer J (1931) The secondary os calcis. J Anat 66(1):84–97
Mooney V (1935) Avulsion of the epiphysis of the os calcis. J Bone Joint Surg 17(4):1056–1057
Moore GE (1933) Fractures of the tuber calcanei involving the medial and lateral processes. Surg Gynecol Obstet 5:400–405
Nielsen S, Agnholt J, Christensen H (1987) Radiologic findings in lesions of the ligamentum bifurcatum of the midfoot. Skeletal Radiol 16(2):114–116
Norfray JF, Rogers LF, Adamo GP, Groves HC, Heiser WJ (1980) Common calcaneal avulsion fracture. AJR Am J Roentgenol 134(1):119–123
Ouellette H, Salamipour H, Thomas BJ, Kassarjian A, Torriani M (2006) Incidence and MR imaging features of fractures of the anterior process of calcaneus in a consecutive patient population with ankle and foot symptoms. Skeletol Radiol 35(11):833–837
Partridge (1852) Fracture of the os calcis. Lancet 60(1512):177
Pelletier JP, Kanat IO (1990) Avulsion fracture of the calcaneus at the origin of the abductor hallucis muscle. J Foot Surg 29(3):268–271
Petrover D, Schweitzer ME, Laredo JD (2007) Anterior process calcaneal fractures: a systematic evaluation of associated conditions. Skeletal Radiol 36(7):627–632
Piatt AD (1956) Fracture of the promontory of the calcaneus. Radiology 67(3):386–390
Pillai A, Arora J, Williams C, Ferdinand R (2005) The sprain fracture of the calcaneus revisited. Foot 1:198–201
Protheroe K (1969) Avulsion fractures of the calcaneus. J Bone Joint Surg Br 51(1):118–122
Renfrew DL, el-Khoury GY (1985) Anterior process fractures of the calcaneus. Skeletal Radiol 14(2):121–125
Robbins MI, Wilson MG, Sella EJ (1999) MR imaging of anterosuperior calcaneal process fractures. AJR Am J Roentgenol 172(2):475–479
Rothberg A (1939) Avulsion fracture of the os calcis. J Bone Joint Surg Am 2:218–220
Rowe C, Sakellarides H, Freeman P, Sorbie C (1963) Fractures of the os calcis. JAMA 184(12):98–101
Schmidt TL, Weiner DS (1982) Calcaneal fractures in children. An evaluation of the nature of the injury in 56 children. Clin Orthop Relat Res 171:150–155
Squires B, Allen PE, Livingstone J, Atkins RM (2001) Fractures of the tuberosity of the calcaneus. J Bone Joint Surg Br 83(1):55–61
Struppler V (1939) Avulsion fracture of the calcaneal tuberosity. Arch Orthop Trauma Surg 39(5):651–658
Thomson R (1900) A rare case of fracture of the os calcis by muscular force. Lancet 156(4025):133–134
Trnka HJ, Zettl R, Ritschl P (1998) Fracture of the anterior superior process of the calcaneus: an often misdiagnosed fracture. Arch Orthop Trauma Surg 117(4–5):300–302
Vollrath T, Eberle C, Grauer W (1987) Computed tomography of intra-articular calcaneal fractures. Rofo 146(4):400–403
Warrick CK, Bremner AE (1953) Fractures of the calcaneum, with an atlas illustrating the various types of fracture. J Bone Joint Surg Br 35-B(1):33–45
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License (https://creativecommons.org/licenses/by-nc/2.0), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
About this article
Cite this article
Schepers, T., Ginai, A.Z., Van Lieshout, E.M.M. et al. Demographics of extra-articular calcaneal fractures: including a review of the literature on treatment and outcome. Arch Orthop Trauma Surg 128, 1099–1106 (2008). https://doi.org/10.1007/s00402-007-0517-2
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00402-007-0517-2