
Abstract
Aims
Sleep-disordered breathing (SDB) and its subtype central sleep apnoea (CSA) are highly prevalent in patients with heart failure and associated with worse prognosis. Whereas pharmacological therapy of heart failure has been shown to ameliorate CSA, results from previous studies on the effect of mitral regurgitation therapy on SDB are contradicting. The aim of this study was to assess the impact of transcatheter edge-to-edge mitral valve repair (TEER) on prevalence and severity of CSA.
Methods and results
We enrolled 47 patients undergoing TEER for symptomatic mitral regurgitation in a prospective study. Secondary mitral regurgitation and left ventricular ejection fraction < 50% were present in 79% and 68% of patients, respectively. Respiratory polygraphy was performed before TEER in a compensated condition and four weeks after the procedure. 34 patients completed the follow-up. At baseline, 19 (56%) patients showed moderate-to-severe SDB, of whom 13 (68%) were classified as CSA. Both apnoea-hypopnoea index and percentage of recorded time spent in Cheyne-Stokes respiration strongly decreased from baseline to follow-up (median [IQR] 16 [7–30] vs. 7 [4–15] /h, p = 0.007; 6 [0–34] vs. 0 [0–8] %, p = 0.008). Median relative reduction of central apnoea index was 75% (p = 0.023), while obstructive apnoea index did not change significantly. Increase in stroke volume after TEER and high systolic pulmonary artery pressure at baseline predicted a > 50% reduction of both Apnoea-hypopnoea index and Cheyne-Stokes respiration.
Conclusion
TEER is associated with a significant short-term reduction of CSA and Cheyne-Stokes respiration in high-risk patients, strengthening its value as an effective treatment option for advanced heart failure.
Graphical abstract

Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Sleep-disordered breathing (SDB) is highly prevalent in the population suffering from chronic heart failure (HF), affecting approximately half of the patients with systolic dysfunction [1]. Both obstructive sleep apnoea (OSA) and central sleep apnoea (CSA) occur more frequently in HF and are independently associated with worse prognosis [2]. In particular, the presence of significant periodic Cheyne–Stokes respiration (CSR) may identify patients at high risk for cardiovascular death [3]. Whereas specific treatment of OSA may be beneficial in HF, management of CSA primarily focuses on the therapy of the underlying condition, such as myocardial ischemia, dilated cardiomyopathy, or valvular heart disease [4]. In patients with symptomatic mitral regurgitation (MR), previous studies evaluating the effect of surgical or transcatheter edge-to-edge mitral valve repair (TEER) are contradicting. While surgery has been shown to effectively reduce SDB and eliminate CSA in individual patients [5,6,7], a small case series of patients undergoing MitraClip implantation did not detect a reduction of SDB severity [8]. With another study demonstrating modest SDB amelioration after TEER in a population largely suffering from OSA [9], the value of minimal-invasive MR therapy in reducing CSA, particularly in comparison to surgery, remains to be established. Therefore, the aim of the present study was to investigate the effect of TEER on CSA and elucidate potential mechanisms associated with SDB attenuation.
Methods
Study population
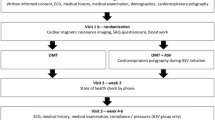
From October 2019 to February 2021, we enrolled consecutive patients in a prospective observational study at the University Heart Center Regensburg (Fig. 1). Inclusion criterion was symptomatic moderate-to-severe or severe MR treated with TEER. Patients with previously established specific SDB therapy were excluded. The decision for TEER in each patient was made by an interdisciplinary Heart Team consisting of an interventional cardiologist, a cardiac surgeon, and an anaesthesiologist. Participants with failure to implant the device, incomplete follow-up, or initiation of specific SDB therapy before follow-up were excluded from analysis.

Study flow chart. SDB, sleep-disordered breathing; TEER, transcatheter edge-to-edge mitral valve repair
Study design
Baseline respiratory polygraphy was performed during the hospital stay in the night before TEER. Patients underwent prior cardiac recompensation therapy, if needed. Follow-up recordings were acquired four weeks after TEER in an outpatient setting, instructing participants to use the device for one night at home. Additionally, all participants underwent comprehensive clinical and echocardiographic assessment at baseline and four weeks after TEER, including New York Heart Association (NYHA) functional class, six-minute walk distance, and laboratory measurements of natriuretic peptides. Patient-reported quality of life was evaluated using the EuroQol EQ-5D-5L questionnaire; results are reported as EQ-5D index value (from 0 [worst] to 1 [best]) and EQ visual analogue scale (from 0 [worst] to 100 [best]). MR grading was based on colour and continuous wave Doppler examination in accordance with current guidelines [10, 11]. Regurgitation grade was scored from I to IV (I: mild, II: mild-to-moderate, III: moderate-to-severe, IV: severe). Stroke volume was estimated noninvasively by measuring doppler-derived velocity time integral of the left ventricular outflow tract. TEER was performed by experienced interventionalists using the MitraClip (Abbott Vascular, Menlo Park, USA) or PASCAL system (Edwards Lifesciences, Irvine, USA) under general anaesthesia, guidance by fluoroscopy, and three-dimensional transoesophageal echocardiography.
Respiratory polygraphy
Nocturnal respiratory polygraphy was performed using a three-channel SDB-monitoring device (ApneaLink plus, ResMed, USA), recording nasal flow, thoracic effort, and pulse oximetry. Performance of the device with automatic scoring in patients without known heart disease was validated in several studies, reporting a sensitivity of 73–94% and a specificity of 85–95% using an apnoea-hypopnoea index (AHI) cutoff value of 15/h [12,13,14]. A previous study on the use of the SDB-monitoring device in patients with chronic HF reported a sensitivity of 73% and a specificity of 87% for detecting SDB when compared with the gold standard polysomnography [1]. Recordings were analysed and scored by trained medical staff. The default settings of the device were used for the definitions of apnoea, hypopnoea, and desaturation: apnoea was defined as a ≥ 80% decrease in airflow for ≥ 10 s, hypopnoea as a decrease in airflow by ≥ 50–80% for ≥ 10 s, and desaturation as a ≥ 4% decrease in oxygen saturation. If > 50% of apnoeas were obstructive, patients were classified as OSA. Otherwise, patients were classified as CSA. CSR was defined as ≥ 3 episodes of continuous cycles of waxing and waning tidal volumes with periods of hyperventilation separated by apnoea/hypopnoeas. A prior validation study on CSR detection in both HF and non-HF patients reported a sensitivity of 87% and specificity of 95% for the device [15]. AHI cut-off values for mild and moderate-to-severe SDB were defined as ≥ 5/h and ≥ 15/h, respectively.
Statistical analysis
Continuous variables are reported as mean ± standard deviation when normally distributed, continuous variables with skewed distribution as median with interquartile range [first quartile-third quartile]. Categorical variables are presented in numbers and percentages. Differences in unpaired data were assessed using students t-test for normally distributed data, Mann–Whitney-U test for ordinal or skewed data, Pearson’s chi-squared test for nominal data, and Fisher’s exact test for dichotomous data. Differences in paired samples were tested using paired t tests for normally distributed data, Wilcoxon signed-rank tests for skewed or ordinal data, and McNemar’s test for dichotomous data. To identify predictors of SDB and CSR improvement, binary logistic regression models were calculated. Predictors with p < 0.05 in univariate analysis were included in the multivariate analysis. A two-sided p value of < 0.05 was considered statistically significant. All statistical analyses were performed using SPSS Statistics 26 (IBM, Armonk, USA).
Results
Baseline characteristics and procedural outcome
Of 78 patients who underwent TEER from October 2019 to February 2021, 47 patients were enrolled. A total of 34 patients completed the follow-up and were available for analysis (Fig. 1). Mean age of the study population was 72 ± 12 years, and 14 (41%) patients were of female gender. Most patients presented with MR grade IV (74%) of secondary or mixed aetiology (79%). Reduced left ventricular ejection fraction (< 50%) was present in 23 (68%) participants. With 26 (74%) patients exhibiting NYHA functional class III or worse, the study population showed clinical signs of advanced HF.
Baseline characteristics in relation to the presence of SDB are shown in Table 1. Patients with moderate-to-severe SDB (AHI ≥ 15/h) had worse functional status at baseline in terms of NYHA class (III or IV 90% vs. 53%, p = 0.036). Also, SDB was associated with more severe tricuspid regurgitation (severe in 63% vs. 20%, p = 0.047) and worse quality of life (EQ visual analogue scale 50 [40–55] vs. 60 [50–70], p = 0.045). No differences were detected in MR severity, left ventricular ejection fraction, or comorbidities. Yet, we noted a trend towards patients with moderate-to-severe SDB being more frequently male (74% vs. 40%, p = 0.080) and having higher systolic pulmonary artery pressure (sPAP, 46 ± 15 vs. 37 ± 11 mmHg, p = 0.086).
Procedural details of TEER are shown in Supplementary Table 1. SDB was not associated with an increase in periinterventional ventilation time or length of hospital stay. In the follow-up examination four weeks after the procedure, reduction of MR to grade I or II was achieved in 29 (85%) patients. Concomitantly, echocardiography revealed a reduction of left atrial volume (82 ± 45 vs. 71 ± 41 ml/m2, p < 0.001) and systolic pulmonary artery pressure (42 ± 14 vs. 37 ± 14 mmHg, p = 0.003). Patients showed significant improvement in both NYHA functional status (class III or IV 74% vs. 15%, p < 0.001) and six-minute walk distance (252 ± 92 vs 295 ± 104 m, p = 0.002). This was accompanied by an increase in patient-reported quality of life (EQ-5D index 0.80 [0.66–0.87] vs. 0.88 [0.66–0.94], p = 0.032). Of note, intake of HF medication or diuretics and body weight did not change from baseline to the four weeks follow-up (Supplementary Table 2).
Respiratory parameters
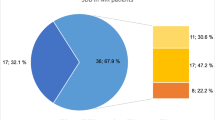
Results of respiratory polygraphy of the whole study population are shown in Table 2. At baseline, 19 (56%) patients showed moderate-to-severe SDB (AHI ≥ 15/h), of whom 13 (68%) had CSA (Fig. 2). In the follow-up examination 4 weeks after TEER, the number of patients with moderate-to-severe SDB was reduced by more than half to 9 (24%, p = 0.007). Alongside, AHI decreased substantially from a median of 16 [7–30] to 7 [4–15]/h (p = 0.007). This reduction was driven by a decrease of central events: central apnoea index significantly decreased by a median of 75% from baseline to follow-up (p = 0.023). Similarly, proportion of recorded time spent in CSR significantly decreased from 6 [0–34] to 0 [0–8] % (p = 0.008). As a consequence, CSA resolved in 9 of the 13 affected patients (p = 0.022). In contrast, the frequency of obstructive apnoeas remained similar (p = 0.153).

Prevalence of moderate-to-severe SDB (A), Apnoea-Hypopnoea index (B) and proportion of Cheyne-Stokes respiration (C) at baseline and four weeks after TEER. B Data are shown as tukey-style box plots. C Data are shown as mean ± SEM. AHI, Apnoea-Hypopnoea index; CSA, central sleep apnoea; CSR, Cheyne-Stokes respiration; OSA, obstructive sleep apnoea; SDB, sleep-disordered breathing
Additionally, we performed a subanalysis of patients with at least mild SDB (AHI ≥ 5/h; Supplementary Table 3). Similar to above findings, AHI, central apnoea events, and CSR significantly decreased from baseline to four weeks after TEER. Yet, we also observed a trend towards a reduction of obstructive apnoeas from baseline to follow-up (2 [1–5] vs. 1 [0–3]/h, p = 0.056).
Predictors of reduction of sleep-disordered breathing
To identify predictors of significant AHI reduction four weeks after TEER, univariate and multivariate logistic binary regression was conducted in patients with at least mild SDB at baseline (Table 3). Successful reduction of AHI was defined as a > 50% decrease from baseline to follow-up. Both increase in cardiac stroke volume (odds ratio [OR] per ml 1.26 [1.07–1.49], p = 0.006) and higher sPAP at baseline (OR per mmHg 1.11 [1.02–1.20], p = 0.016) were predictors of successful AHI reduction (Fig. 3). In multivariate analysis, increase in stroke volume remained an independent predictor (OR per ml 1.24 [1.05–1.48], p = 0.013). Nor echocardiographic reduction of MR grade or change in serum NTproBNP levels were associated with AHI reduction. Also, gender, left ventricular function, MR of secondary aetiology, or cardiac comorbidities were not predictive of an improvement of SDB. To confirm our results, we additionally evaluated predictors of successful reduction of CSR, defined as a > 50% decrease from baseline to follow-up (Supplementary Table 4). Congruous to above findings, higher sPAP at baseline and increase in stroke volume were predictive of CSR reduction in univariate analysis (OR per mmHg 1.14 [1.00–1.31], p = 0.046; OR per ml 1.17 [1.01–1.34], p = 0.034).

Correlation between AHI reduction four weeks after TEER and baseline systolic pulmonary artery pressure (A) or stroke volume increase (B) in patients with at least mild SDB (AHI ≥ 5/h, n = 28). Data are shown as scatter plots with linear regression lines. AHI, Apnoea-Hypopnoea index; sPAP, systolic pulmonary artery pressure
Clinical outcome in patients with central sleep apnoea
Considering the observed strong effects of TEER on central respiratory events, we conducted a subanalysis of clinical and echocardiographic outcomes in patients with CSA (n = 13; Supplementary Table 5). Mirroring the results of the whole study population, the procedure was associated with a strong reduction of MR grade (III or IV 100% vs. 16%, p < 0.001) and improvement in NYHA functional status (class III or IV 84% vs 31%, p = 0.001) at the four weeks follow-up. Whereas left ventricular parameters and serum NTproBNP levels remained unchanged, left atrial reverse remodeling was observed (left atrial volume index 71 ± 26 vs. 64 ± 21 ml/m2, p = 0.030). Also, patients reported a pronounced increase in quality of life four weeks after the procedure (EQ-5D index 0.65 [0.43–0.76] vs. 0.80 [0.54–0.95], p = 0.004).
Discussion
Our study provides systematic investigation on SDB in patients treated with minimal-invasive mitral valve repair in a high-risk population with symptomatic MR. As the main finding, TEER was associated with a significant reduction in central sleep apnoea and hypopnoea events in the short term, resulting in the resolution of moderate-to-severe SDB in approximately half of the affected patients. Likewise, proportion of CSR, a hallmark of advanced HF [3], substantially decreased after treatment of MR. Furthermore, we identified elevated baseline sPAP and increase in cardiac stroke volume as independent predictors of AHI and CSR reduction after TEER.
Therapy of mitral regurgitation ameliorates central sleep apnoea and Cheyne-Stokes respiration
Previous data on the effects of MR therapy on SDB and its subtype CSA are limited. In two case reports, nearly complete resolution of CSA was observed after surgical mitral valve therapy, accompanied by a reduction in circulation delay [6, 7]. In a systematic investigation of 82 patients, mitral valve surgery was associated with a significant reduction in AHI three months postoperatively [5]. Yet, due to the lack of respiratory effort measurements, the effect on SDB subtypes remained unclear. In this context, our study adds two important aspects to current knowledge on the impact of MR therapy on SDB: First, the effect of mitral valve surgery on SDB was reproduced using transcatheter repair, both confirming previous results and demonstrating the equivalence of TEER to surgical therapy with a view to improving central sleep apnoea. Second, our findings confirm that the effect of successful mitral valve therapy on SDB is strongly connected with a reduction of CSA and CSR.
Two previous studies investigated the course of SDB in patients undergoing TEER. Contrary to our findings, Spiesshoefer et al. did detect a reduction in respiratory event lengths, but not in SDB severity in a study of 20 patients undergoing MitraClip implantation [8]. With baseline characteristics, MR severity, SDB prevalence, and subtype distribution being comparable to our study population, we may only speculate about the reasons for this discrepancy. While follow-up polygraphy was performed 4 weeks after TEER in our protocol, Spiesshoefer et al. conducted the second polygraphy only days after the intervention. As such, their findings might have been confounded by postoperative fluid overload and/or anaesthesia. More importantly, it has been shown that restoration of impaired chemoreceptor sensitivity after therapeutic intervention takes 2–6 weeks to set in [16]. Likewise, cardiac reverse remodeling and its systemic effects after successful TEER might manifest after a certain delay. In summary, we consider it likely that the follow-up polygraphy in Spiesshoefer et. al was carried out too early to evaluate the effect. Still, the observed decrease of respiratory event lengths is well in line with our results and may constitute a precursor to the remarkable effect on SDB severity in our study.
In another study, Daher et al. investigated the effect of TEER on SDB in a population with baseline characteristics similar to our study [9]. They observed less pronounced results, with AHI reduction only being significant in a subgroup of patients with moderate-to-severe SDB. The vast majority of patients in Daher et al. showed predominant OSA, with only four patients suffering from CSA and only two exhibiting significant CSR. This is distinct from the phenotype found in our study and in large registry studies on SDB in chronic HF, which reported predominant CSA in 31% and periodic breathing in 41% of patients [3, 17]. Consequently, the results from the previous study might more adequately reflect the effect of TEER on OSA, whereas our study adds insight on the course of SDB in a population with high CSA burden. As we observed that the reduction in apnoeas was driven by a decrease in central events, it is likely that the larger proportion of patients with CSA led to stronger effects on SDB severity in our study.
Reduction of central sleep apnoea after transcatheter mitral valve repair is associated with increased cardiac stroke volume and pulmonary decongestion
In our study, high baseline sPAP and increase in cardiac stroke volume after TEER were predictive of both AHI and CSR reduction. Considering the pathophysiology of SDB in HF, these findings offer conclusive mechanistic explanations for the observed effect of TEER. CSA is characterized by a dysregulation of the feedback loop between chemoreceptors and respiratory effort [18]. The hemodynamic consequences of HF promote CSA by compromising two components of the feedback loop: reduced cardiac output increases circulatory delay between lungs and chemoreceptors, perpetuating the cycle of periodic ventilatory over- and undershoot which results in CSR [19]. Second, elevated left ventricular filling pressure and left atrial distension increase chemoreceptor sensitivity, aggravating the chemoreflex response to fluctuations in blood oxygen and carbon dioxide levels (loop gain) initiating the Cheyne-Stokes cycle [20, 21].
Our results indicate that the hemodynamic effects of TEER target both components of the feedback loop: an increase in cardiac stroke volume, which was shown to predict SDB reduction, improves cardiac output, reducing circulatory delay. Additionally, as observed in our study, sPAP and left atrial distension decrease after TEER, which reduces loop gain by lowering chemoreceptor sensitivity. In accordance with this consideration, we found that high sPAP at baseline is predictive of SDB reduction after TEER, identifying patients with high left ventricular filling pressure who profit from pulmonary decongestion. Apart from these mechanisms, nocturnal fluid shifts from the legs into neck and lungs occurring in HF have been shown to promote upper airway narrowing and hyperventilation, triggering both OSA and CSA in a unifying pathophysiological concept [22]. Hence, amelioration of right-heart failure by successful therapy of MR may have contributed to the observed effect on SDB.
Strengths and limitations
Our study provides insight on the course of SDB in a well-characterized group of high-risk patients with symptomatic MR, reflecting the population treated with TEER in contemporary clinical care. By combining comprehensive non-invasive cardiac evaluation and polygraphy, we were able to elucidate hemodynamic changes associated with SDB improvement. As the baseline polygraphy was performed in the night before TEER, it was ensured that the patients were in a compensated condition during the measurement. This conclusion is strengthened by the fact that the participants did not show weight loss from baseline to the four weeks follow-up. In addition, neither HF medication nor diuretics changed from baseline to the four weeks follow-up. Considering that both fluid overload and escalation of HF medication have been shown to attenuate SDB [23,24,25], the absence of these confounders support the validity of the main findings of our study.
Our study might have several limitations. Like previous investigations on SDB in mitral valve disease, our study lacks a control group. Therefore, we cannot rule out that unknown confounders influenced the results. To enable SDB diagnostics timely before TEER and in an outpatient setting for follow-up, a portable three-channel device was used instead of polysomnography. While the latter is the diagnostic gold standard, portable devices have been validated in multiple studies and have shown adequate diagnostic accuracy in patients with chronic HF [1]. The limited sample size may have restricted statistical power. In particular, results of multivariate analysis may be considered exploratory and should be validated in a larger cohort.
Subjective sleepiness is a key feature of SDB in patients without HF, guiding both diagnosis and therapy. However, the opposite is true for HF patients with sleep apnoea: this population is characterized by the remarkable absence of sleepiness symptoms despite objective evidence of reduced sleep quality [26]. Multiple observational studies consistently failed to demonstrate differences in patient-reported daytime sleepiness in HF patients with or without SDB, encompassing both CSA and OSA [27,28,29]. Hence, we refrained from assessing subjective sleepiness in our patients, as we deemed it unhelpful in giving additional insight into the relationship between SDB and TEER. This consideration is strengthened by the results of Daher et al., who did not find differences in self-reported sleepiness in patients with or without sleep apnoea undergoing TEER [9].
Clinical implications
SDB is a very common comorbidity in patients with chronic HF and associated with worse prognosis [1, 2]. While treatment of OSA by positive airway pressure may improve quality of life in subjects with HF, the therapeutic approach to CSA, which is more common in these patients, remains challenging [4]. Although adaptive servo ventilation effectively reduces CSA, it counter-intuitively increases mortality in patients with reduced left ventricular ejection fraction [30]. This detrimental effect was shown to be even more pronounced in patients with a high proportion of CSR. These results foster the concept of CSA being a compensatory mechanism with protective effects in severe HF [31], which in consequence must not be suppressed by ventilation therapy. Instead, given its strong prognostic burden [32], the presence of CSA may serve as an indicator of advanced disease which warrants intensified guideline-based therapy of the underlying heart condition by HF medication, cardiac resynchronization, and TEER. In line with this consideration, SDB was associated with worse functional status, quality of life, and more severe tricuspid regurgitation in our study. Noteworthy, tricuspid regurgitation itself has been demonstrated to predict poor outcome in HF patients in general [33, 34] as well in those with MR in particular [35], corroborating the link between CSA and advanced HF.
Conversely, attenuation of CSA may be a surrogate marker for successful HF therapy. In this context, the observed amelioration of CSA after TEER in our study may imply a significant reduction of total cardiovascular risk, mirroring the results of the COAPT study on mortality and morbidity [36]. Indeed, CSA patients showed favourable clinical outcomes in our study in terms of MR reduction, functional status, and quality of life, substantiating the relationship between SDB and cardiac function. Of note, while SDB has been shown to predict pulmonary complications after cardiac surgery [37], it was not associated with increased ventilation time or adverse events in our study, confirming the good safety profile the procedure. As a reduction in CSA was also observed after well-established therapies such as ACE inhibition [23] and cardiac resynchronization [38], our data underline the value of TEER being an effective therapy for advanced HF.
Conclusion
Predominant central SDB is very common in high-risk patients with MR. Reduction of MR by TEER is associated with a strong improvement in SDB severity, primarily driven by a decrease of central events and CSR. Increase in cardiac stroke volume and high pulmonary artery pressure at baseline predict SDB improvement and CSR resolution, suggesting decrease of circulatory delay and pulmonary decongestion as the underlying mechanisms. Considering the strong prognostic burden of CSA, our results underline that TEER is an effective treatment option in advanced HF.
Availability of data and material
The data that support the findings of this study are available from the corresponding author upon request.
References
Arzt M, Woehrle H, Oldenburg O, Graml A, Suling A, Erdmann E, Teschler H, Wegscheider K (2016) Prevalence and predictors of sleep-disordered breathing in patients with stable chronic heart failure: the SchlaHF registry. JACC Heart Fail 4:116–125. https://doi.org/10.1016/j.jchf.2015.09.014
Jilek C, Krenn M, Sebah D, Obermeier R, Braune A, Kehl V, Schroll S, Montalvan S, Riegger GAJ, Pfeifer M, Arzt M (2011) Prognostic impact of sleep disordered breathing and its treatment in heart failure: an observational study. Eur J Heart Fail 13:68–75. https://doi.org/10.1093/eurjhf/hfq183
Arzt M, Oldenburg O, Graml A, Erdmann E, Teschler H, Wegscheider K, Suling A, Woehrle H (2017) Phenotyping of sleep-disordered breathing in patients with chronic heart failure with reduced ejection fraction-the SchlaHF registry. J Am Heart Assoc. https://doi.org/10.1161/JAHA.116.005899
Javaheri S, Barbe F, Campos-Rodriguez F, Dempsey JA, Khayat R, Javaheri S, Malhotra A, Martinez-Garcia MA, Mehra R, Pack AI, Polotsky VY, Redline S, Somers VK (2017) Sleep apnea: types, mechanisms, and clinical cardiovascular consequences. J Am Coll Cardiol 69:841–858. https://doi.org/10.1016/j.jacc.2016.11.069
Gerçek M, Oldenburg O, Gerçek M, Fox H, Rudolph V, Puehler T, Omran H, Wolf LK, Hakim-Meibodi K, Zeiher AM, Gummert J, Dimitriadis Z (2021) Prevalence of sleep disordered breathing in patients with primary mitral regurgitation undergoing mitral valve surgery. J Clin Med 10:2039. https://doi.org/10.3390/jcm10092039
Yasuma F, Hayashi H, Noda S, Tsuzuki M, Tanaka M, Okada T (1995) A case of mitral regurgitation whose nocturnal periodic breathing was improved after mitral valve replacement. Jpn Heart J 36:267–272. https://doi.org/10.1536/ihj.36.267
Rubin AE, Gottlieb SH, Gold AR, Schwartz AR, Smith PL (2004) Elimination of central sleep apnoea by mitral valvuloplasty: the role of feedback delay in periodic breathing. Thorax 59:174–176. https://doi.org/10.1136/thorax.2003.007799
Spiesshoefer J, Spieker M, Klose S, Keymel S, Boentert M, Krüger S, Horn P, Kelm M, Westenfeld R (2019) Reduction of sleep-disordered breathing following effective percutaneous mitral valve repair with the MitraClip system. Sleep Breath 23:815–824. https://doi.org/10.1007/s11325-018-1764-x
Daher A, Müller T, Marx N, Schröder J, Almalla M, Keszei AP, Reith S, Dreher M (2021) Effects of transcatheter mitral valve repair using MitraClip® device on sleep disordered breathing in patients with mitral valve regurgitation. J Clin Med 10:3332. https://doi.org/10.3390/jcm10153332
Zoghbi WA, Adams D, Bonow RO, Enriquez-Sarano M, Foster E, Grayburn PA, Hahn RT, Han Y, Hung J, Lang RM, Little SH, Shah DJ, Shernan S, Thavendiranathan P, Thomas JD, Weissman NJ (2017) Recommendations for noninvasive evaluation of native valvular regurgitation: a report from the American society of echocardiography developed in collaboration with the society for cardiovascular magnetic resonance. J Am Soc Echocardiogr 30:303–371. https://doi.org/10.1016/j.echo.2017.01.007
Zoghbi WA, Asch FM, Bruce C, Gillam LD, Grayburn PA, Hahn RT, Inglessis I, Islam AM, Lerakis S, Little SH, Siegel RJ, Skubas N, Slesnick TC, Stewart WJ, Thavendiranathan P, Weissman NJ, Yasukochi S, Zimmerman KG (2019) Guidelines for the evaluation of valvular regurgitation after percutaneous valve repair or replacement: a report from the American Society of Echocardiography developed in collaboration with the society for cardiovascular angiography and interventions, Japanese Society of Echocardiography, and society for cardiovascular magnetic resonance. J Am Soc Echocardiogr 32:431–475. https://doi.org/10.1016/j.echo.2019.01.003
Chen H, Lowe AA, Bai Y, Hamilton P, Fleetham JA, Almeida FR (2009) Evaluation of a portable recording device (ApneaLink) for case selection of obstructive sleep apnea. Sleep Breath 13:213–219. https://doi.org/10.1007/s11325-008-0232-4
Crowley KE, Rajaratnam SMW, Shea SA, Epstein LJ, Czeisler CA, Lockley SW (2013) Evaluation of a single-channel nasal pressure device to assess obstructive sleep apnea risk in laboratory and home environments. J Clin Sleep Med 9:109–116. https://doi.org/10.5664/jcsm.2400
Erman MK, Stewart D, Einhorn D, Gordon N, Casal E (2007) Validation of the ApneaLink for the screening of sleep apnea: a novel and simple single-channel recording device. J Clin Sleep Med 3:387–392
Weinreich G, Armitstead J, Töpfer V, Wang Y-M, Wang Y, Teschler H (2009) Validation of ApneaLink as screening device for Cheyne–Stokes respiration. Sleep 32:553–557. https://doi.org/10.1093/sleep/32.4.553
Schulz R, Blau A, Börgel J, Duchna HW, Fietze I, Koper I, Prenzel R, Schädlich S, Schmitt J, Tasci S, Andreas S (2007) Sleep apnoea in heart failure. Eur Respir J 29:1201–1205. https://doi.org/10.1183/09031936.00037106
Oldenburg O, Lamp B, Faber L, Teschler H, Horstkotte D, Töpfer V (2007) Sleep-disordered breathing in patients with symptomatic heart failure: a contemporary study of prevalence in and characteristics of 700 patients. Eur J Heart Fail 9:251–257. https://doi.org/10.1016/j.ejheart.2006.08.003
Orr JE, Malhotra A, Sands SA (2017) Pathogenesis of central and complex sleep apnoea. Respirology 22:43–52. https://doi.org/10.1111/resp.12927
Mortara A, Sleight P, Pinna GD, Maestri R, Capomolla S, Febo O, La Rovere MT, Cobelli F (1999) Association between hemodynamic impairment and cheyne-stokes respiration and periodic breathing in chronic stable congestive heart failure secondary to ischemic or idiopathic dilated cardiomyopathy. Am J Cardiol 84:900–904. https://doi.org/10.1016/S0002-9149(99)00462-2
Olson TP, Frantz RP, Snyder EM, O’Malley KA, Beck KC, Johnson BD (2007) Effects of acute changes in pulmonary wedge pressure on periodic breathing at rest in heart failure patients. Am Heart J 153:104.e1–7. https://doi.org/10.1016/j.ahj.2006.10.003
Calvin AD, Somers VK, Johnson BD, Scott CG, Olson LJ (2014) Left atrial size, chemosensitivity, and central sleep apnea in heart failure. Chest 146:96–103. https://doi.org/10.1378/chest.13-0309
Yumino D, Redolfi S, Ruttanaumpawan P, Su M-C, Smith S, Newton GE, Mak S, Bradley TD (2010) Nocturnal rostral fluid shift: a unifying concept for the pathogenesis of obstructive and central sleep apnea in men with heart failure. Circulation 121:1598–1605. https://doi.org/10.1161/CIRCULATIONAHA.109.902452
Walsh JT, Andrews R, Starling R, Cowley AJ, Johnston ID, Kinnear WJ (1995) Effects of captopril and oxygen on sleep apnoea in patients with mild to moderate congestive cardiac failure. Br Heart J 73:237–241. https://doi.org/10.1136/hrt.73.3.237
Valdivia-Arenas MA, Powers M, Khayat RN (2009) Sleep-disordered breathing in patients with decompensated heart failure. Heart Fail Rev 14:183–193. https://doi.org/10.1007/s10741-008-9103-0
Bucca CB, Brussino L, Battisti A, Mutani R, Rolla G, Mangiardi L, Cicolin A (2007) Diuretics in obstructive sleep apnea with diastolic heart failure. Chest 132:440–446. https://doi.org/10.1378/chest.07-0311
Pak VM, Strouss L, Yaggi HK, Redeker NS, Mohsenin V, Riegel B (2019) Mechanisms of reduced sleepiness symptoms in heart failure and obstructive sleep apnea. J Sleep Res 28:e12778. https://doi.org/10.1111/jsr.12778
Atalla A, Carlisle TW, Simonds AK, Cowie MR, Morrell MJ (2017) Sleepiness and activity in heart failure patients with reduced ejection fraction and central sleep-disordered breathing. Sleep Med 34:217–223. https://doi.org/10.1016/j.sleep.2016.11.022
Hastings PC, Vazir A, O’Driscoll DM, Morrell MJ, Simonds AK (2006) Symptom burden of sleep-disordered breathing in mild-to-moderate congestive heart failure patients. Eur Respir J 27:748–755. https://doi.org/10.1183/09031936.06.00063005
Arzt M, Young T, Finn L, Skatrud JB, Ryan CM, Newton GE, Mak S, Parker JD, Floras JS, Bradley TD (2006) Sleepiness and sleep in patients with both systolic heart failure and obstructive sleep apnea. Arch Intern Med 166:1716–1722. https://doi.org/10.1001/archinte.166.16.1716
Cowie MR, Woehrle H, Wegscheider K, Angermann C, d’Ortho M-P, Erdmann E, Levy P, Simonds AK, Somers VK, Zannad F, Teschler H (2015) Adaptive servo-ventilation for central sleep apnea in systolic heart failure. N Engl J Med 373:1095–1105. https://doi.org/10.1056/NEJMoa1506459
Naughton MT (2012) Cheyne–Stokes respiration: friend or foe? Thorax 67:357–360. https://doi.org/10.1136/thoraxjnl-2011-200927
Corrà U, Pistono M, Mezzani A, Braghiroli A, Giordano A, Lanfranchi P, Bosimini E, Gnemmi M, Giannuzzi P (2006) Sleep and exertional periodic breathing in chronic heart failure: prognostic importance and interdependence. Circulation 113:44–50. https://doi.org/10.1161/CIRCULATIONAHA.105.543173
Nath J, Foster E, Heidenreich PA (2004) Impact of tricuspid regurgitation on long-term survival. J Am Coll Cardiol 43:405–409. https://doi.org/10.1016/j.jacc.2003.09.036
Koelling TM, Aaronson KD, Cody RJ, Bach DS, Armstrong WF (2002) Prognostic significance of mitral regurgitation and tricuspid regurgitation in patients with left ventricular systolic dysfunction. Am Heart J 144:524–529. https://doi.org/10.1067/mhj.2002.123575
Ruel M, Rubens FD, Masters RG, Pipe AL, Bédard P, Mesana TG (2004) Late incidence and predictors of persistent or recurrent heart failure in patients with mitral prosthetic valves. J Thorac Cardiovasc Surg 128:278–283. https://doi.org/10.1016/j.jtcvs.2003.11.048
Stone GW, Lindenfeld J, Abraham WT, Kar S, Lim DS, Mishell JM, Whisenant B, Grayburn PA, Rinaldi M, Kapadia SR, Rajagopal V, Sarembock IJ, Brieke A, Marx SO, Cohen DJ, Weissman NJ, Mack MJ (2018) Transcatheter mitral-valve repair in patients with heart failure. N Engl J Med 379:2307–2318. https://doi.org/10.1056/NEJMoa1806640
Tafelmeier M, Luft L, Zistler E, Floerchinger B, Camboni D, Creutzenberg M, Zeman F, Schmid C, Maier LS, Wagner S, Arzt M (2021) Central sleep apnea predicts pulmonary complications after cardiac surgery. Chest 159:798–809. https://doi.org/10.1016/j.chest.2020.07.080
Gabor JY, Newman DA, Barnard-Roberts V, Korley V, Mangat I, Dorian P, Hanly PJ (2005) Improvement in Cheyne–Stokes respiration following cardiac resynchronisation therapy. Eur Respir J 26:95–100. https://doi.org/10.1183/09031936.05.00093904
Funding
Open Access funding enabled and organized by Projekt DEAL. The study did not receive external funding.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Kurt Debl, Christine Meindl and Bernhard Unsöld received travel support from Abbott Vascular. The other authors declare they have no conflict of interest.
Ethics approval
The study was approved by the ethics committee of the University of Regensburg and followed the ethical principles of the Declaration of Helsinki.
Consent to participate
All participants gave written consent prior to study enrolment.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Paulus, M.G., Liedtke, T., Hamerle, M. et al. Impact of transcatheter edge-to-edge mitral valve repair on central sleep apnoea. Clin Res Cardiol 112, 594–604 (2023). https://doi.org/10.1007/s00392-022-02139-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00392-022-02139-3