
Abstract
Background
Multimorbidity is gaining increasing attention due to its substantial medical, healthcare political and social challenges. So far, however, there have been only few studies attempting to characterize the underlying pathogenesis.
Method
A selective literature search was carried out in PubMed.
Results
There is no generally accepted definition of multimorbidity. In the studies published so far, attempts have mostly been made to identify frequent clusters of diseases. In order to prevent multimorbidity, however, it is necessary to characterize the underlying mechanisms of development in more detail. For this purpose, a concept is presented based on the previously published data, in particular from longitudinal studies showing the importance of known risk factors. Possible pathogenetic processes involving multimorbidity are briefly discussed.
Conclusion
For most pathogenetic processes leading to multimorbidity there is no suitable pharmacological treatment available; however, behavior such as lack of exercise, dietary habits, smoking and high alcohol consumption are of considerable importance for the development of multimorbidity and can in principle be influenced by treatment.
Zusammenfassung
Hintergrund
Das Thema Multimorbidität gewinnt aufgrund der großen damit verbundenen medizinischen, gesundheits- und sozialpolitischen Herausforderungen zunehmend an Aufmerksamkeit. Bisher gibt es aber nur wenige Studien, in denen versucht wurde, die Entstehungsmechanismen näher zu charakterisieren.
Methode
Selektive Literaturrecherche in PubMed und einige Beispielberechnungen auf der Basis eigener Daten (GePsy-Studie).
Ergebnisse
Noch gibt es keine allgemein anerkannte Definition für Multimorbidität. In den bisher vorliegenden Untersuchungen wurde vor allem versucht, häufige Kombinationen von Erkrankungen (sog. Cluster) zu identifizieren. Zur Prävention und Behandlung der Multimorbidität ist es aber notwendig, die vielfältigen Entstehungsmechanismen näher zu charakterisieren, um so eine Differenzierung vornehmen und entsprechende therapeutische Strategien entwickeln zu können. Hierzu wird ein Konzept vorgestellt, das auf den bisher publizierten Daten, insbesondere aus Verlaufsstudien beruht. Diese zeigen die Bedeutung bekannter Risikofaktoren. Mögliche, einer Multimorbidität zugrundeliegende pathogenetische Prozesse werden kurz dargestellt.
Schlussfolgerungen
Die vielfältigen pathogenetischen Prozesse, die zu einer Multimorbidität führen können, sind bisher medikamentös kaum beeinflussbar. Aber Verhaltensweisen wie Bewegungsmangel, Ernährungsgewohnheiten, Rauchen und hoher Alkoholkonsum sind für die Entwicklung einer Multimorbidität von erheblicher Bedeutung und prinzipiell therapeutisch beeinflussbar.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
For affected persons multimorbidity is a major burden that leads to impairment of the quality of life, including mobility and restrictions on self-sufficiency. As a result, mental disorders, particularly depression, often occur [4]. Multimorbidity is also commonly associated with cognitive disorders [12] and leads to increased mortality [29]. In view of these facts, the number of scientific publications on the topic of multimorbidity has significantly increased in recent years.
A difficulty in considering the studies is that a generally accepted definition of multimorbidity and standardized assessment tools has so far been lacking. This is due to a variety of aspects to be taken into account. In most proposals for a definition (see overview [24, 28]), multimorbidity is defined as the simultaneous presence of three or more chronic diseases [6]. A closer look at the different definitions reveals that a wide range of physical impairments are also included [28]: risk factors such as hyperlipidemia and symptoms such as back pain. In Anglo-American literature, therefore, the term multiple chronic conditions is used as well. It is also not clearly defined what is meant by chronic. In most cases, a duration of at least 1 year is considered to be necessary.
Most of the previous studies on multimorbidity are cross-sectional ones related to the actual state, the conditions of occurrence (e.g. age, education, socioeconomic status) and the consequences of multimorbidity, in particular increased frailty and mortality during the course [30]. In order to design strategies for prevention and treatment, probable routes of development of multimorbidity and possible underlying pathomechanisms have be elucidated.
Methods
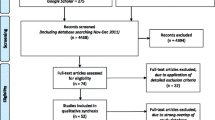
A systematic review was carried out by searching PubMed for articles with the key words multimorbidity, longitudinal and follow-up study (Fig. 1). The retrieval of relevant studies was conducted via title screening, abstract screening, and full-text eligibility assessment applying the defined inclusion criterion endpoint multimorbidity. The literature research (conducted on 15 August 2019) yielded 583 publications.

PRISMA flow diagram showing the search strategy. MM multimorbidity, MM+ second keyword
Results
Clues for the development of multimorbidity can be obtained by two different ways:
1) Investigations in cross-sectional studies showing statistical relationships of the different diseases in multimorbidity
The associations of diseases in multimorbidity are very complex and can only be calculated using different mathematical models (e.g. cluster or factor analyses). The clusters of the most common combinations of diseases show a considerable heterogeneity [23]. A recent review of 51 studies identified a total of 407 different multimorbidity profiles [5].
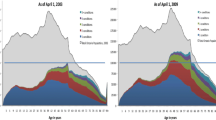
Attempts were made to visualize the relationships between the diseases using various methods for calculation, i.e. the strength of the statistical relationship of corresponding diseases [19]. For illustration see Fig. 2, calculated on previously published own data [25]. Due to the complexity, i.e. the variety of combination options, a tabular form is also suitable for an overview. Additional data, such as age group and statistical correlations (odds ratios) can increase the significance [3].

Relations between risk factors and diseases of different organs. Diagramed are all relations with odds ratios >1 (blue lines), in case of significant correlation with the odds ratio (black lines)
These descriptions of the actual state, however, say little about the development of multimorbidity. Above all, they show the manifold interrelationships. These can be used, especially when respecting different age groups, for initial considerations and hypotheses on etiology. For this purpose, correlations with high odds ratios have to be primarily evaluated; however, meaningful data on the etiology of multimorbidity can only be obtained from longitudinal studies. Our data (shown in Fig. 2) revealed more significant relationships between risk factors and diseases than interrelationships of different organs diseases.
2) Follow-up studies with the endpoint multimorbidity
An Australian study [16] attempted to clarify which disease was the first to occur in later manifest multimorbidity. The results showed a heterogeneous picture with hyperlipidemia as the most common first manifestation. Other longitudinal studies (Table 1) mainly considered behavioral disorders, i.e. behavior that differs from the normal population or from the recommendations of medical societies (lack of physical activity, smoking, increased alcohol consumption and obesity or dietary habits). These increase the likelihood of multimorbidity developing during follow-up.
The longitudinal studies revealed a significant increase in the likelihood of developing multimorbidity with cumulative number of risk factors or, if a chronic disease already exists [7, 9].
Proposal for a concept model
In view of the complexity of the development of multimorbidity, it seems appropriate to propose a classification into few categories, which consider etiological aspects as far as known. Furthermore, such a classification should facilitate the decision of drug treatment in problematic constellations as well as approaches to prevention. So far, there are only few publications attempting to classify different types of multimorbidity taking into account different etiologies or pathomechanisms [13, 24].
The first step towards a concept for categorizing multimorbidity is the comparison of the expected and observed frequency of simultaneous occurrence of diseases on the basis of epidemiological data. If in epidemiological studies the observed frequency of a common occurrence is significantly higher than the expected one, an analysis of possible underlying pathogenesis should be conducted in a second step (see Fig. 3). In order to clarify possible etiological connections, it is helpful to observe the occurrence of the various diseases over time. There are three possibilities basically conceivable: occurrence sequentially, simultaneously and not known.

Schema of the different types of multimorbidity (MM) as described in the text. Adapted from [24], modified. a MM type 1 no common pathogenesis known, b MM type 2 statistical correlation only, c MM type 3 known risk factor, d MM type 4 known causal relation, e MM type 5 multiple associations. 1 disease 1, 2 disease 2, wearing i.e. deterioration, mechanical stress or fatigue of functionality
If there is a combination of two diseases in which, on the basis of epidemiological data, the expected and observed frequencies of simultaneous occurrence do not significantly differ, the probability of mutual influences has to be judged as absent. Thus, the first type of multimorbidity (MM type 0) includes combinations of coexistent impairments of various organs, in which no etiological connection is known.
Often the search for possible common etiological factors reveals only an age dependence of both diseases, so that age may be the essential factor for coexistence. This MM type 1 is often based on physical processes in the broadest sense, e.g. mechanical stress (e.g. osteoarthritis) or fatigue of functionality (e.g. presbycusis, presbyopia).
Moreover, besides age there may be a possibly not yet known association between at least two diseases (MM type 2), but a strong statistical correlation. This type includes a great number of combinations of diseases identified in various cross-sectional studies (see [5, 23]).
The longitudinal studies compiled in Table 1 show the importance of risk factors for the development of multimorbidity. These may become manifested for decades before corresponding diseases occur, e.g. increased alcohol consumption [26]. This type is referred to in the concept presented here as MM type 3. Several different organs may be affected by one single risk factor, e.g. alcohol, smoking or diabetes mellitus. But several risk factors may be responsible for the damage of one organ at the same time as well [22], e.g. in metabolic syndrome.
A disease can also be the result of another, i.e. a kind of causal relation exists, such as in thromboembolic brain infarction in atrial fibrillation. Thus, there is an initial disease (= MM type 4). The organs concerned are often those that are functionally closely related (= systemic multimorbidity). This circumstance often leads to a cascading development of multimorbidity. For example, the disease of one organ (e.g. chronic obstructive pulmonary disease) constantly overwhelms the reserve capacity of another (e.g. heart). Therefore, treatment of the index or first-time disease is particularly important. But here, too, the limitations made above must be taken into account when planning treatment.
A fundamental difficulty in trying to clarify the development of multimorbidity is that connections between the individual diseases are often associative. Frequently, a variety of mostly two-way links between diseases (MM type 5), which can affect each other, are to be taken into account. Often such functional interactions exist not only between two organs, but between several (see Fig. 3). The manifold interactions make adequate treatment planning extremely difficult, especially if a further acute disease (e.g. infection) occurs.
Possible pathogenesis
Such a schematic classification of multimorbidity is plausible only if the corresponding pathogenesis is known. A lot of studies show that the prevalence and the incidence of multimorbidity significantly increase with age. Aging is a multifaceted process, involving numerous molecular and cellular mechanisms in the context of different organ systems. Therefore, it seems worthwhile to look at the possible underlying pathogenetic mechanisms of multimorbidity, considering the age dependency:
-
1.
Degenerative intracellular processes (such as shortening of telomeres, mitochondrial dysfunction, etc. [2]. These are especially found in multimorbidity types (1), 2 and 4. Increasing age has the main impact on degenerative processes.
-
2.
Oxidative stress (formation of free radicals, etc.). This is a biochemical process known in some risk factors. It plays an important role, especially in multimorbidity types 2 and 4 [2].
-
3.
Inflammatory processes. These are found in many chronic diseases (e.g. atherosclerosis) [8], which can lead to multimorbidity, especially in types 2 and 4. Functional and structural alterations in the immune system are an important component of aging, i.e. low-grade inflammation.
-
4.
Allergic mechanisms, especially in multimorbidity typse 2 and 4. Aging is associated with a higher prevalence of autoimmunity.
-
5.
Epigenetic mechanisms (e.g. DNA methylation). Recent research has revealed that epigenetic modifications play an important role in the development of physical consequences of risk factors, e.g. diabetes mellitus [1]. Epigenetic mechanisms are particularly important in multimorbidity types 2 and 4.
So far, such studies usually only relate to one disease or a risk factor, but similar mechanisms are described in many studies. Therefore, it is very likely that these pathomechanisms play an important role in the development of multimorbidity. It should be borne in mind that the processes mentioned in 1–5 are closely related or interrelated.
Therapeutic implications
So far, there are no drugs sufficiently affecting the majority of the pathobiochemical mechanisms mentioned above. Especially age is an untreatable factor. Therefore, the question arises of currently available options for therapy or prevention of multimorbidity.
Prevention is possible by treating the metabolic risk factors like diabetes mellitus. The guidelines of the corresponding German or European medical societies [15, 20, 21] contain treatment recommendations for cases in which several risk factors are present simultaneously; however, the total number of prescribed drugs, in particular their interactions, as well as age and the limited ability to metabolize must be taken into account.
The available follow-up studies with the endpoint multimorbidity (Table 1) have shown the considerable importance of behavior (such as lack of exercise, smoking) which can ultimately be described as harmful to health. These are not only known risk factors, but also have a negative impact on other risk factors that belong to metabolic syndrome (Table 2). As these risk factors are closely linked, early intervention is required.
Discussion
Until now, little has been published about the complex ways of development of multimorbidity [13, 24]. This is due, among other things, to the large number of socioeconomic, psychosocial and genetic factors as well as age and environment, to be taken into account. Affected persons and the doctors treating them can have little direct influence on these factors and thus contribute to prevention.
In view to developing a concept for the different routes of multimorbidity formation this article highlighted the medical aspects. A classification of 5 types of multimorbidity formation was proposed.
In the discussion on multimorbidity, the important aspect of harmful behavior (lack of exercise, dietary habits, smoking and high alcohol consumption) was hardly taken into account but the results of the follow-up studies (Table 1) underline their impact. Given the importance of these behaviors for the development of multimorbidity and the enormous costs involved, preventive measures to reduce their prevalence should be stepped up, as these are ultimately factors which are can be intentionally influenced. In principle, they can be treated by means of instructions for behavioral modification, i.e. smoking cessation. The difficulty, however, is that these are favored habits with sometimes signs of addiction, i.e. smoking, alcohol consumption. Interventions to change behavior are limited by a low level of education and a low socioeconomic status. Both are also a risk factor for the development of multimorbidity [14, 18, 30]. Therefore, the conditions for successful prevention of multimorbidity are not favorable.
Limitations
The search strategy has been limited to PubMed possibly missing a significant volume of literature. Furthermore, the methodology and the study design in the cited publications are partly variable and therefore not comparable. More importantly, different definitions of multimorbidity were used. Therefore, these considerations can only be a first attempt to address the complex issue of the development of multimorbidity and its treatment options.
References
Bansal A, Pinney SE (2017) DNA methylation and its role in the pathogenesis of diabetes. Pediatr Diabetes 18:167–177
Barnes PJ (2015) Mechanisms of development of multimorbidity in the elderly. Eur Respir J 45:790–806
Bobo WV, Yawn BP, St. Sauver JL, Grossardt BR, Boyd CM, Rocca WA (2016) Prevalence of combined somatic and mental health multimorbidity: patterns by age, sex, and race/ethnicity. J Gerontol A Biol Sci Med Sci 71:1483–1491
Brettschneider C, Leicht H, Bickel H, Dahlhaus A, Fuchs A et al (2013) Relative impact of multimorbid chronic conditions on health-related quality of life—results from the multicare cohort study. PLoS One 8:e66742
Busija L, Lim K, Szoeke C, Sanders KM, McCabe MP (2019) Do replicable profiles of multimorbidity exist? Systematic review and synthesis. Eur J Epidemiol 34:1025–1053
DEGAM (2017) S3-Leitline Multimorbidität (AWMF-Register Nr. 053-047)
Dhalwani NN, Zaccardi F, O’Donovan G, Carter P, Hamer M et al (2017) Association between lifestyle factors and the incidence of multimorbidity in an older English population. J Gerontol A Biol Sci Med Sci 72:528–534
Ferrucci L, Fabbri E (2018) Inflammageing: chronic inflammation in ageing, cardiovascular disease, and frailty. Nat Rev Cardiol 15:505–522
Jackson CA, Dobson AJ, Tooth LR, Mishra GD (2016) Lifestyle and socioeconomic determinants of multimorbidity patterns among mid-aged women: a longitudinal study. PLoS One 11:e156804
Katikireddi SV, Skivington K, Leyland AH, Hunt K, Mercer SW (2017) The contribution of risk factors to socioeconomic inequalities in multimorbidity across the lifecourse: a longitudinal analysis of the Twenty-07 cohort. BMC Med 15:152
Kivimäki M, Kuosma E, Ferrie JE, Luukkonen R, Nyberg ST et al (2017) Overweight, obesity, and risk of cardiometabolic multimorbidity: pooled analysis of individual-level data for 120813 adults from 16 cohort studies from the USA and Europe. Lancet Public Health 2:e277–e285
Koroukian SM, Schiltz NK, Warner DF, Stange KC, Smyth KA (2017) Increasing burden of complex multimorbidity across gradients of cognitive impairment. Am J Alzheimers Dis Other Demen 32:408–417
Meghani SH, Buck HG, Dickson VV, Hammer MJ, Rabelo-Silva ER et al (2013) The conceptualization and measurement of comorbidity: a review of the interprofessional discourse. Nurs Res Pract. https://doi.org/10.1155/2013/192782
Mounce LTA, Campbell JL, Henley WE, Tejerina Arreal MC, Porter I et al (2018) Predicting incident multimorbidity. Ann Fam Med 16:322–329
AWMF online (2014) Nationale VersorgungsLeitlinie Typ2-Diabetes: Therapie. http://www.awmf.org/leitlinien/detail/ll/nvl-001g.html. Accessed 17 Dec 2019
Ruel G, Lévesque JF, Stocks N, Sirois C, Kroger E et al (2014) Understanding the evolution of multimorbidity: evidences from the north west Adelaide health longitudinal study (NWAHS). PLoS ONE 9:e96291
Ryan A, Murphy C, Boland F, Galvin R, Smith SM (2018) What is the impact of physical activity and physical function on the development of multimorbidity in older adults over time? A population-based cohort study. J Gerontol A Biol Sci Med Sci 73:1538–1544
Singh-Manoux A, Fayosse A, Sabia S, Tabak A, Shipley M et al (2018) Clinical, socioeconomic, and behavioural factors at age 50 years and risk of cardiometabolic multimorbidity and mortality: a cohort study. PLoS Med 15:e1002571
Sinnige J, Korevaar JC, Westert GP, Spreeuwenberg P, Schellevis FG, Braspenning JC (2015) Multimorbidity patterns in a primary care population aged 55 years and over. Fam Pract 32:505–513
The Task Force for the management of arterial hypertension of the European Society of Cardiology (ESC), European Society of Hypertension (ESH) (2018) 2018 ESC/ESH guidelines for the management of arterial hypertension. Eur Heart J 39:3021–3104
The Task Force for the management of dyslipidaemias of the European Society of Cardiology (ESC), European Atherosclerosis Society (EAS) (2019) 2019 ESC/EAS guidelines for the management of dyslipidaemias: lipid modification to reduce cardiovascular risk. Atherosclerosis 290:140–205
Tomasdottir MO, Sigurdsson JA, Petursson H, Kirkengen AL, Lund Nilsen TI et al (2016) Does ‘existential unease’ predict adult multimorbidity? Analytical cohort study on embodiment based on the Norwegian HUNT population. BMJ Open 6:e12602
Violan C, Foguet-Boreu Q, Flores-Mateo G, Salisbury C, Blom J et al (2014) Prevalence, determinants and patterns of multimorbidity in primary care: a systematic review of observational studies. PLoS ONE 9:e102149
Wetterling T (2019) Neuropsychiatrische Aspekte der Multimorbidität. Kohlhammer, Stuttgart
Wetterling T, Junghanns K (2019) Führt Multimorbidität bei älteren psychiatrischen Patienten gehäuft zu Verlegungen zwischen der Psychiatrie und somatischen Abteilungen? Z Gerontol Geriatr 52:568–574
Wetterling T, Veltrup C, Driessen M, John U (1999) Drinking pattern and alcohol-related medical disorders. Alcohol Alcohol 34:330–336
Wikström K, Lindström J, Harald K, Peltonen M, Laatikainen T (2015) Clinical and life-style-related risk factors for incident multimorbidity: 10-year follow-up of Finnish population-based cohorts 1982–2012. Eur J Intern Med 26:211–216
Willadsen TG, Bebe A, Køster-Rasmussen R, Jarbøl DE, Guassora AD et al (2016) The role of diseases, risk factors and symptoms in the definition of multimorbidity—a systematic review. Scand J Prim Health Care 34:112–121
Willadsen TG, Siersma V, Nicolaisdóttir DR, Køster-Rasmussen R, Jarbøl DE et al (2018) Multimorbidity and mortality: a 15-year longitudinal registry-based nationwide Danish population study. J Comorb 8(1):2235042X18804063. https://doi.org/10.1177/2235042X18804063
Xu X, Mishra GD, Dobson AJ, Jones M (2018) Progression of diabetes, heart disease, and stroke multimorbidity in middle-aged women: a 20-year cohort study. PLoS Med 15:e1002516
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
T. Wetterling declares that he has no competing interests.
This article does not contain studies on human or animal subjects.
Rights and permissions
Open Access. This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Wetterling, T. Pathogenesis of multimorbidity—what is known?. Z Gerontol Geriat 54, 590–596 (2021). https://doi.org/10.1007/s00391-020-01752-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00391-020-01752-z