
Abstract
Background
Laser Hemorrhoidoplasty (LHP) is a minimally invasive surgical option for the management of hemorrhoidal disease that has been increasingly adopted by surgeons over the last decade. Two wavelengths; 980 nm and 1470 nm have been employed in LHP. However, no data exist comparing the effects of these two wavelengths for this indication. This systematic review investigates both wavelengths for the management of hemorrhoids via the LHP procedure.
Methods
This systematic analysis and meta-analysis was performed following the PICOS and PRISMA guidelines. A systematic research of MEDLINE, Scopus, Clinicaltrials.gov, Embase, Cochrane Central Register of Controlled Trials, CENTRAL and Google Scholar databases from inception until March 2024 was performed.
Results
Overall, 19 studies including seven randomized control trials (RCT) and 12 non-randomized control trials with a total of 2492 patients were included in this systematic review and meta-analysis. The duration of LHP with both wavelengths was significantly shorter compared to open hemorrhoidectomy, postoperative pain and the rate of postoperative complications were significantly lower following LHP. There was no statistically significant difference in the rate of recurrence between LHP with the 980-nm wavelength and open hemorrhoidectomy. However, LHP with 1470-nm wavelength resulted in significantly higher recurrence rate compared to hemorrhoidectomy.
Conclusion
Although no direct studies have compared the two wavelengths used in LHP, the outcomes of LHP seem to be independent of the wavelength used. Both wavelengths, when correctly used provide similar results, which are mostly better compared to open hemorrhoidectomy in terms of postoperative complications and postoperative pain, but not in terms of recurrence, where at least for the 1470-nm wavelength, LHP seems to show a higher recurrence rate when compared to open hemorrhoidectomy. Although a direct comparison of both wavelengths was not possible, technical issues regarding number of shots and energy per pile represent relevant parameters for recurrence after LHP.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Laser Hemorrhoidoplasty (LHP) describes a minimally invasive procedure for the management of symptomatic hemorrhoids using laser energy [1,2,3,4]. In the standard LHP, the laser energy is first applied just above the dentate line to coagulate the feeding vessels and thereafter into the engorged hemorrhoidal tissue causing its shrinkage and secondary adhesion onto the bowel wall [2, 5,6,7]. Because of its many advantages (e.g. small wounds at the puncture sites, low pain levels, outpatient procedure, early return to work, no continence disturbance), LHP has rapidly been adopted as a minimally invasive and tissue preserving technique in the management of hemorrhoidal disease [8,9,10,11,12]. While the results following LHP have been encouraging so far, there are still a lot of unanswered questions. Technically, two different wavelengths; 980 nm and 1470 nm have been employed by different users to perform LHP [13, 14]. The amount of energy applied to the hemorrhoidal tissue is directly proportional to both the wavelength of the laser used and the duration of application. This heterogeneity can also be easily identified amongst different users with regard to the amount of energy per pile and the number of piles treated [15]. Since both the efficacy and safety of laser-based surgery depends, at least partly, on the amount of energy, energy-correlated outcomes for laser surgery are a reasonable research topic. To the best of our knowledge, a direct comparison of the two wavelengths used in LHP has not been performed so far. Looking at the direct relationship between energy and outcome, studying this possible association may provide more insight to guide clinical practice. The aim of this study, therefore, was to investigate the two available laser wavelengths for LHP regarding postoperative outcomes.
Methods
This study was conducted in strict accordance with the Cochrane Handbook of Systematic Reviews and Meta-analysis ver. 6.2 and reported according to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) statement guideline. A systematic literature review was conducted for articles published in Web of Science, Embase, Cochrane Library, PubMed. Articles were identified using search terms ‘hemorrhoids’ (Mesh term), ‘Laser’, ‘Open’, ‘Milligan-Morgan’, ‘Conventional’, ‘Excisional’, ‘Hemorrhoidectomy’ (Mesh term), and ‘Clinical Trial’ (Mesh term), and ‘1470 nm’, ‘980 nm’. This systematic review was registered with PROSPERO.
Inclusion and exclusion criteria
We conducted a systematic review and meta-analysis of clinical trials and observational studies. Since no studies directly compared both wavelengths, the outcomes of each wavelength were compared with open hemorrhoidectomy. Thus, the meta-analysis was done on studies comparing LHP 1470 nm and 980 nm) against open surgery.
The inclusion criteria using the PICOS statement are as follows:
-
P—patients undergoing management for hemorrhoidal disease.
-
I—a group of patients who received LHP using either 980 nm or a1470 nm wavelength.
-
C: a group of patients who underwent conventional hemorrhoidectomy.
-
O: report at least one of the following results: operative time, complications, recurrence rate, postoperative day 1 pain using the visual analog pain (VAS) scale; (5)
-
S: randomized or non-randomized clinical trials, observational studies (cohort or case–control) and case series; (6) full-text report (including preprint).
The exclusion criteria were as follows: (1) articles reported in languages other than English; (2) studies on stapler fixation; (3) no control studies; (4) unpublished studies or abstracts.
Study selection and data extraction
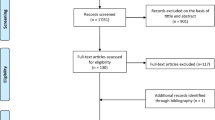
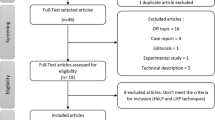
Two independent investigators (ZL and JW) screened included articles according to the PRISMA guidelines for systematic reviews. Since no studies directly compared both wavelengths, the outcomes of each wavelength were compared with open hemorrhoidectomy. The initial step was to screen the title and abstract by two investigators to determine which articles met the criteria. Additionally, the references of eligible studies were hand-searched for more potential articles. The repeated articles were deleted. Finally, the full text is selected independently by two investigators, and the inconsistencies were resolved through discussion with PCA (Fig. 1).

PRISMA flow chart for the selection of studies included in the study
Statistical analysis
The RevMan 5.3 software provided by Cochrane Collaboration was used for data analysis. For dichotomous data, the risk ratio (RR) of 95% confidence interval (CI) was calculated, while for continuous data, average difference (MD) and standard average difference (95%CI) were calculated. Chi-square test and I2 statistics were used to evaluate the heterogeneity to determine whether the results of different studies were uniform.
Results
Overall, 19 studies with 2492 patients were included in this article. The basic characteristics of these studies are revealed in Table 1.
Assessment of risk of bias
The quality of 7 RCTs was assessed by the Cochrane Handbook for Systematic Reviews and the 12 non-RCTs’ quality was assessed by the Newcastle–Ottawa Scale. The details and results are shown in Fig. 2 and Table 2.

Assessment of risk of bias of RCTS
Operative time
The 980-nm group had a significantly shorter operative time (7 studies, n = 485) than the hemorrhoidectomy group (mean difference [MD], − 15.04; 95% CI, − 18.08 to − 12.00; p < 0.0001) (Fig. 3a, b).

Forest plots for the length of surgery. Pooled analysis indicated LHP to be significantly faster compared to hemorrhoidectomy, irrespective of the wavelength used (a 980 nm, b 1470 nm)
The 1470-nm group also had a significantly shorter operative time (8 studies, n = 842) than the hemorrhoidectomy group (mean difference [MD], − 2.60; 95% CI, − 2.99 to − 2.21; p < 0.00001).
Complications
There was significant difference in the rate of complications between the 980-nm group and the hemorrhoidectomy group of 4 studies (n = 276), with a OR of 0.34 (CI:0.16–0.69) p = 0.003 (Fig. 4a, b).

Forest plots for complication. The rate of postoperative complications (urinary retention, postoperative bleeding and acute postoperative thrombosis) was significantly lower in the LHP (irrespective of wavelength: a 980 nm, b 1470 nm) in comparison with open hemorrhoidectomy
There was significant difference in the rate of complications between the 1470-nm group and the hemorrhoidectomy group from the pooled estimate of 5 studies (n = 483), with a OR of 0.34 (CI:0.14–0.83) p = 0.02.
The VAS on postoperative day 1
A total of three studies reported pain through the VAS on postoperative day 1 for the 980-nm wavelength with 289 patients. The LHP group had significantly reduced pain compared to the hemorrhoidectomy group with a mean difference of 2.45 (CI: 1.54–3.44, p < 0.0001) (Fig. 5a, b).

Forest plot for postoperative pain. Overall, postoperative pain was significantly lower following LHP (for both wavelengths a 980 nm, b 1470 nm) compared to hemorrhoidectomy
A total of five studies using 1470-nm wavelength reported pain through the VAS on postoperative day 1 with 539 patients. The LHP group had significantly reduced pain compared to the hemorrhoidectomy group with a mean difference of 3.26 (CI: 1.77–4.76, p < 0.0001).
Recurrence rate
Three studies with 1096 patients reported recurrence rates in the 980-nm group. There was no significant differences in the recurrence rates (OR:0.13; 95% CI, 0.00–3.62; p = 0.23) (Fig. 6a, b).

a and b rates of recurrence
Six studies including 563 patients reported recurrence rates in the 1470-nm group. There was significant difference in the recurrence rates (OR:3.11; 95% CI, 1.53–6.36; p = 0.002). The recurrence rate of the open hemorrhoidectomy group was lower than that of the 1470-nm group.
As the follow-up time is not mentioned in some articles in the 980-nm laser group, and less data are included, further clinical study is needed.
Discussion
The LHP procedure has been increasingly adopted over the last decade for the management of symptomatic hemorrhoids. Traditionally, two different wavelengths: 980 nm and 1470 nm have been used for this indication. However, no comparison has been made between both wavelengths to the best of our knowledge. Since the results of LHP is based on the direct effect of the laser energy applied to the piles, the outcomes of LHP therefore should partly depend on the wavelength used for treatment. Although this systematic review remains inconclusive due to the lack of studies investigating both wavelengths, pooled results confirm the efficacy and safety of both wavelength in performing LHP compared to open hemorrhoidectomy.
Alsisy et al. used the 980-nm wavelength to deliver the energy with a power of 15 W for 1.6 s (24 Joules) per shot in a study from Egypt [13]. In a study comparing hemorrhoidectomy with LHP Maloku et al. from Kosova used the 980-nm wavelength to deliver 13 W for 1.2 s per shot (18 J) [25]. In another study from Baghdad, Mahmood et al. used the 980-nm wavelength beginning with 8 W (which was increased as needed) for 3 s (minimum energy per shot 24 J) to perform LHP [22]. Despite the differences in energy employed in the above studies, the results of LHP in all three studies were similar.
The 1470-nm wavelength has been increasingly used more recently. As with the 980-nm wavelength, different amounts of energy have been used by different authors. Camil et al. for example used 8 W for 3 s per shot (24 J) [27]. While this setting has been used by many authors [24, 26], Khan et al. reported using 8.5 W without stating the duration of application to reach 150–350 J per segment [30]. Equally, little differences have been seen amongst these studies despite the differences in the amount of energy applied.
The minimally invasive nature of LHP is largely based on the means of access to the hemorrhoidal tissue by introducing the laser probe via a 2-mm puncture at level of the anal verge. LHP as a minimally invasive procedure has been shown to be a fast procedure compared to hemorrhoidectomy. This trend could be confirmed for 980-nm wavelength and for 1470-nm wavelength [34, 35]. Similarly, postoperative pain and overall complication rates were similar for both wavelengths in the LHP group, but significantly lower compared to the group managed with hemorrhoidectomy. Similar trends have been reported in the systematic analyses by Lakmal et al. [36] for the 980-nm wavelength as well as by Lie et al. and Tan et al. [34, 37].
An interesting finding from this systematic review was a difference in the rates of recurrence following LHP. While no statistically significant difference was observed between LHP using 980-nm wavelength and hemorrhoidectomy, the recurrence rate was significantly higher following LHP with 1470 nm compared to open hemorrhoidectomy. This finding, however, must be discussed regarding the surgical technique for LHP used in the included studies. In the study by Durgun and Yigit for example, the LHP procedure consisted of just five shot of 24 J per pile [28]. Haluk Tümer and Mevlut Agca also reported using 5–6 shots of 6–6.4 W [31]. The energy used in the LHP group by Eskandaros et al. was not clearly reported [29]. The same argument holds for the publication by Ahmed Hassan and Gamal Shemy [23] who stated 8 Watts for 7 s without reporting the number of shots. Finally, Verma et al. used 8 W for 1.6 s (12.8 J) [32]. Despite giving 8 shots per pile, the cumulative energy of 100.8 J was way below the expected energy needed to achieve a good LHP result. Looking at these technical variations, the piles in the LHP group in these studies were not adequately treated. The techniques used in these five studies about the number of shots and the amount of laser energy used are contrary to what is recommended in the standard LHP technique, i.e. 6–8 shots to manage the pile, resulting in 210–350 J.
A major limitation of this manuscript is the lack of studies with direct comparison of both wavelengths for LHP. Therefore, a direct analysis of pooled data to study the effect of the chosen wavelength was not possible. Also, there is a wide heterogeneity amongst users with regard to the technique of performing LHP that renders comparison of outcomes difficult [38]. Only studies in English language were included in this systematic review, thus there is a possibility that potentially relevant studies in languages other than English that may have affected the overall effects seen in this study were not included. More so, it is also possible that our search strategy may have missed some relevant studies.
Despites these limitations, our study clearly identifies a relevant gap in current literature about LHP and laser surgery in proctology in general. This gap may be of clinical relevance since the safety and efficacy of laser-based interventions in proctology are energy dependent and the amount of energy is obviously related to the chosen wavelength. Our study therefore may be instrumental in defining future research in this domain.
Conclusion
Although no direct studies have compared the two wavelengths used in LHP, the outcomes of LHP seem to be independent of the wavelength used. Both wavelengths, when correctly used provide similar results, which are mostly better compared to open hemorrhoidectomy in terms of postoperative complications and postoperative pain, but not in terms of recurrence, where at least for the 1470-nm wavelength, LHP seems to show a higher recurrence rate when compared to open hemorrhoidectomy. Although a direct comparison of both wavelengths was not possible, technical issues regarding number of shots and energy per pile represent relevant parameters for recurrence after LHP.
This systematic review shows the need to standardize the LHP technique in order to achieve more homogenous results and better define the real role of LHP in the treatment of hemorrhoidal disease.
Data availability
All data used for this study have been included in the manuscript.
References
Alam A (2021) Laser surgery for treatment of haemorrhoid and anal fissure and its outcome. Sch J App Med Sci 5:663–669
Azadgoli B, Baker RY (2016) Laser applications in surgery. Ann Transl Med 4(23):452
Boarini P, Boarini LR, Candelaria PdAP, Lima EMd, Boarini MR (2017) LASER hemorrhoidal dearterialization. J Coloproctol (Rio de Janeiro) 37:38-43
Boerhave NH, Klicks RJ, Dogan K (2023) The efficacy of laser haemorrhoidoplasty (LHP) in the treatment of symptomatic haemorrhoidal disease: an observational cohort study. Color Dis 25(6):1202–1207
Danys D, Pacevicius J, Makunaite G, Palubeckas R, Mainelis A, Markevicius N, Strupas K, Poskus T (2020) Tissue coagulation in laser hemorrhoidoplasty–an experimental study. Open Med 15(1):185–189
Elfallal AH, Fathy M, Elbaz SA, Emile SH (2022) Comprehensive literature review of the applications of surgical laser in benign anal conditions. Lasers Med Sci 37(7):2775–2789
Gupta K (2022) Lasers in surgery: from past to present. In: Lasers in proctology. Springer, Published online November 22, 2022:1-335
Chong H-Y, Roslani AC, Rajandram R, Kumar S, Malik AA, Law C-W, Chan S-H, Rajasingam V, Kasipillai J (2022) Clinical short-term outcomes of laser hemorrhoidoplasty: a multicenter study: received 2021–07-29; accepted 2022–01-07; published 2022–07-01. J Health Transl Med 25(2):73–78
Dursun A, Tuncer GK, Tuncer K, Karaali C, Erdoğan G, Emiroglu M (2023) Effectiveness of laser hemorrhoidoplasty in the treatment of hemorrhoidal disease. Cir Cir 91(2):179–185
Faes S, Pratsinis M, Hasler-Gehrer S, Keerl A, Nocito A (2019) Short-and long-term outcomes of laser haemorrhoidoplasty for grade II–III haemorrhoidal disease. Color Dis 21(6):689–696
Gambardella C, Brusciano L, Brillantino A, Parisi S, Lucido FS, Del Genio G, Tolone S, Allaria A, Di Saverio S, Pizza F (2023) Mid-term efficacy and postoperative wound management of Laser Hemorrhoidoplasty (LHP) vs conventional excisional hemorrhoidectomy in grade III hemorrhoidal disease: the twisting trend. Langenbecks Arch Surg 408(1):140
Hossain MS, Bhuiyan MNH, Nahid SMS, Anwar SM, Khan HA, Nipa SA (2022) Comparative study of short-term outcome between laser hemorrhoidoplasty and Milligan-Morgan Hemorrhoidectomy. IAHS Med J 5(2):15–19
Naderan M, Shoar S, Nazari M, Elsayed A, Mahmoodzadeh H, Khorgami Z (2017) A randomized controlled trial comparing laser intra-hemorrhoidal coagulation and Milligan-Morgan hemorrhoidectomy. J Invest Surg 30(5):325–331
Poskus T, Danys D, Makunaite G, Mainelis A, Mikalauskas S, Poskus E, Jotautas V, Dulskas A, Jasiunas E, Strupas K (2020) Results of the double-blind randomized controlled trial comparing laser hemorrhoidoplasty with sutured mucopexy and excisional hemorrhoidectomy. Int J Color Dis 35:481–490
Ambe P (2023) Laser interventions in coloproctology. A plea for standardized treatment protocols. Tech Coloproctol 27(10):953–955
Salem I, Alsisy A, Alkhateep Y (2019) Comparative study between intrahemorrhoidal diode laser treatment and Milligan-Morgan hemorrhoidectomy. Menoufia Med J 32(2):560
Yahya W, Refaat D, AbdElhady W, Elsayed W (2022) Comparison between laser hemorrhoidoplasty procedure and conventional open surgical hemorrhoidectomy. Egypt J Hosp Med 86(1):112–116
Mohammed A, Hussien Al-Sultani D, FlaifelJanabi H (2019) A comparative study between laser hemorrhoidoplasty procedure and conventional hemorrhoidectomy. Jubpas 27(1):69–86
Mert T (2023) Comparison of laser haemorrhoidoplasty and Ferguson haemorrhoidectomy in treating grade III and grade IV haemorrhoids: a prospective randomised study. J Coll Physicians Surg Pak 33(1):41–46
Abdulkarim A, Misoi B, Gathege D (2020) Laser hemorrhoidoplasty: experience at Aga Khan University Hospital. Ann Afr Surg 17(2):76–79
(2015) Comparison of intrahemorrhoidal coagulation with 980 nanometer diode laser and Milligan Morgan hemorrhoidectomy: a randomized clinical trial. J Clin Res gov null(null):null
Kims H (2023) Comparative study between laser hemorrhoidoplasty and Milligan-Morgan hemorrhoidectomy in Baghdad and Babylon cities. J Nat Sci, Biol Med 14(2):68–72
Hassan A, El-Shemy G (2012) Laser hemorrhoidoplasty versus open hemorrhoidectomy in Upper Egypt. Al-Azhar Int Med J 0(0):0–0
Gambardella C, Brusciano L, Brillantino A, Parisi S, Lucido FS, Del Genio G, Tolone S, Allaria A, Di Saverio S, Pizza F et al (2023) Mid-term efficacy and postoperative wound management of Laser Hemorrhoidoplasty (LHP) vs conventional excisional hemorrhoidectomy in grade III hemorrhoidal disease: the twisting trend. Langenbeck Arch Surg 408(1):140
Maloku H, Gashi Z, Lazovic R, Islami H, Juniku-Shkololli A (2014) Laser hemorrhoidoplasty procedure vs open surgical hemorrhoidectomy: a trial comparing 2 treatments for hemorrhoids of third and fourth degree. Acta Inform Med 22(6):365–367
Maloku H, Lazovic R, Terziqi H (2019) Laser hemorrhoidoplasty versus Milligan-Morgan hemorrhoidectomy - short term outcome. Vojnosanit Pregl 76(1):8–12
Cemil A, Ugur K, Salih GM, Merve K, Guray DM, Emine BS (2024) Comparison of laser hemorrhoidoplasty and Milligan-Morgan hemorrhoidectomy techniques in the treatment of grade 2 and 3 hemorrhoidal disease. Am Surg 90(4):662–671
Durgun C, Yiğit E (2023) Laser hemorrhoidoplasty versus ligasure hemorrhoidectomy: a comparative analysis. Cureus 15(8):e43119
Eskandaros M, Darwish A (2020) Comparative study between Milligan-Morgan hemorrhoidectomy, stapled hemorrhoidopexy, and laser hemorrhoidoplasty in patients with third degree hemorrhoids: a prospective study. Egypt J Surg 39(2):352
Khan H, Gowda V, Ramesh B, Sandeep D (2021) A comparative evaluation of laser hemorrhoidoplasty versus open surgical hemorrhoidectomy treatment of grade III and IV hemorrhoids. A prospective observational study. J Clin Invest Surg 6(1):30–36
Tümer H, Ağca MH (2023) Comparing outcomes of laser hemorrhoidoplasty and LigaSure hemorrhoidectomy in grade II-III hemorrhoidal disease: a retrospective analysis. ANZ J Surg 93(7–8):1885–1889
Rajkumar V, Narendra K, Vipin M (2024) A comparative study between laser hemorrhoidoplasty with digital-guided hemorrhoidal artery ligation and conventional (Milligan-Morgan) hemorrhoidectomy. Asian J Med Sci 15(2):218–222
Poskus T, Danys D, Makunaite G, Mainelis A, Mikalauskas S, Poskus E, Jotautas V, Dulskas A, Jasiunas E, Strupas K (2020) Results of the double-blind randomized controlled trial comparing laser hemorrhoidoplasty with sutured mucopexy and excisional hemorrhoidectomy. Int j colorectal dis 35(3):481–490
Tan VZZ, Peck EW, Sivarajah SS, Tan WJ, Ho LML, Ng JL, Chong C, Aw D, Mainza F, Foo FJ et al (2022) Systematic review and meta-analysis of postoperative pain and symptoms control following laser haemorrhoidoplasty versus Milligan-Morgan haemorrhoidectomy for symptomatic haemorrhoids: a new standard. Int J Color Dis 37(8):1759–1771
Solari S, Martellucci J, Annicchiarico A, Scheiterle M, Bergamini C, Prosperi P (2023) Laser technology in proctological diseases: is it really the wave of the future? Updates Surg 75(7):1759–1772
Lakmal K, Basnayake O, Jayarajah U, Samarasekera DN (2021) Clinical outcomes and effectiveness of laser treatment for hemorrhoids: a systematic review. World J Surg 45(4):1222–1236
Lie H, Caesarini EF, Purnama AA, Irawan A, Sudirman T, Jeo WS, Budiono BP, Prabowo E, Rivai MI, Sitepu RK (2022) Laser hemorrhoidoplasty for hemorrhoidal disease: a systematic review and meta-analysis. Lasers Med Sci 37(9):3621–3630
Ambe PC (2023) Laser interventions in coloproctology. A plea for standardized treatment protocols. Tech Coloproctol 27(10):953–955
Funding
Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and Affiliations
Contributions
Study Design: PCA Literature search: ZL, JW Statistical Analysis: ZL, JW Manuscript draft: ZL, JW, NNB, PK, KA,PCA Edited the Manuscript: NNB, PK, KA,PCA Final approval: all authors.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Zhicheng Li and Jiong Wu contribute equally to this article and are co-first authors.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Li, Z., Wu, J., Brown, N.K.D. et al. A systematic review comparing the efficacy of 980 nm vs. 1470 nm wavelengths in laser hemorrhoidoplasty. Int J Colorectal Dis 39, 117 (2024). https://doi.org/10.1007/s00384-024-04690-z
Accepted:
Published:
DOI: https://doi.org/10.1007/s00384-024-04690-z