
Abstract
Introduction
Patients with variants in the GNAO1 gene may present with life-threatening dystonic storm. There is little experience using pallidal deep brain stimulation (DBS) as an emergency treatment in such cases.
Case description
We report on a 16-year-old girl with a variant in the GNAO1 gene (c.626G > T; p.(Arg209Leu)) who was admitted to the intensive care unit with medically refractory dystonic storm with secondary complications inducing rhabdomyolysis and acute colitis. Emergency pallidal DBS resulted in rapid improvement of dystonic storm and the subsidence of rhabdomyolysis and colitis. There were no further episodes of dystonic storm during follow-up of 2 years.
Conclusion
Pallidal DBS is a useful treatment option for GNAO1-related dystonic storm with secondary complications which can be performed as an emergency surgery.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Dystonic storm can present as a life-threatening condition with a high risk of mortality and morbidity due to respiratory and metabolic complications [1,2,3]. The management of status dystonicus includes administration of high doses of sedatives, antispasmodic drugs, and treatment of triggering conditions such as infection [2, 4, 5]. In patients who do not respond well to medical treatment, both deep brain stimulation (DBS) and pallidal radiofrequency lesioning have been shown to provide rapid and effective relief [1, 3, 6, 7].
Variants in the GNAO1 gene (guanine-nucleotide-binding protein) have been identified in few patients with dystonic storm [7]. Such patients have been described to respond well to pallidal DBS [7,8,9,10,11,12,13,14,15,16,17]. Here, we report on the use of pallidal DBS as an emergency treatment in a 16-year-old girl with a variant in the GNAO1 gene who presented with a medically refractory dystonic storm complicated by severe rhabdomyolysis and acute colitis.
Case report
This 16-year-old girl was admitted to the pediatric intensive care unit (ICU) with severe dystonic storm which had started after a tooth extraction under general anesthesia. She had a history of markedly delayed development since infancy. Seizures started during the first months of life, and she also developed episodes of varying intensity of dystonic movements of her arms and legs and later involving also the trunk. Initially, she had a diagnosis of cerebral palsy. She never learned to speak, but developed understanding of language, and she was later able to communicate with a talking device. She could not walk independently and was mobilized with a wheelchair and a walking frame. Further symptoms included hypersalivation and multiple contractures and luxations of her extremities which needed surgical correction.
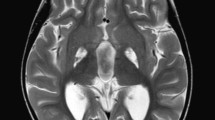
Over the years, she had several episodes of dystonic storm, occasionally associated with rhabdomyolysis and renal impairment which were managed conservatively. Genetic analysis revealed a de novo heterozygous variant in the GNAO1 gene (c.626G > T; p.(Arg209Leu)). MR imaging of her brain was unremarkable (Fig. 1a).

a MRI of the brain: T2-weighted axial image shows no abnormalities. b Postoperative stereotactic CT shows the positioning of the electrodes in the posteroventral lateral globus pallidus internus
After admission to the ICU at age 16, treatment was started with infusions of clonidine, midazolam, and morphine. Thereafter, continuous infusions of hydromorphone (6 µg/kg/h) and clonidine (1.2 µg/kg/h) were given which yielded little improvement of the dystonic storm. Additional treatment with clobazam, tetrabenazine, and gabapentin was ineffective.
Subsequently, hyperkalemia (6.9 mmol/l) and rhabdomyolysis (creatine kinase > 100.00 U/l) developed. Sedation with chloral hydrate resulted in improvement of dystonic storm; however, upon reduction of medication, dystonic storm reemerged over a period of 3 weeks. In the following, her state was further complicated by the development of acute colitis and pneumatosis hepatis.
With regard to her deteriorating condition, she was scheduled for emergency DBS surgery under general anesthesia. Quadripolar DBS electrodes (Vercise Cartesia Directional, Boston Scientific) were implanted bilaterally into the posteroventral lateral globus pallidus internus with CT stereotactic guidance supplemented by preoperative MR imaging and microelectrode recording as described in detail elsewhere [18, 19].
Subsequently, the electrodes were connected to an implantable pulse generator (Vercise PC, Boston Scientific). Postoperative stereotactic CT-imaging demonstrated appropriate electrode placement in the target bilaterally (Fig. 1b). Pallidal stimulation was started directly after completion of the surgery with the following settings: amplitude 2 mA, frequency 130 Hz, and triple monopolar electrode montage on both sides.
The dystonic movements improved rapidly after weaning from general anesthesia. On the second day after implantation of the electrodes, the medication with midazolam, clonidine, and hydromorphone could be reduced and was completely stopped over the next few days. The stimulation amplitude was increased in parallel to 2.9 mA. The rhabdomyolysis ceased, and the colitis subsided. The patient was discharged from the hospital 17 days after DBS surgery.
At 3-month follow-up, there was sustained marked improvement. No further episodes of dystonic storm had occurred. The patient could participate in daily activities again. She lived at home with her parents who were very satisfied with the result. At 2-year follow-up, she was in a stable condition.
Discussion
Mutations in the GNAO1 gene were first identified in patients with epileptic encephalopathy. Subsequently, various phenotypes were defined characterized by severe developmental delay and hyperkinetic movement disorders [20]. GNOA1 is located on the long arm of chromosome 16 (16q12.2). It encodes the Gαo subunit of the guanine-nucleotide-binding protein, which has an important function in modulating transmembrane systems. Loss of function variants in the GNAO1 gene are associated with epilepsy, whereas gain of function variants are reported in patients with movement disorders [7, 14, 21]. In particular, disruption of the G-protein-cAMP pathway axis may be a key contributor to the pathophysiology of dystonia in these patients [7].
Pallidal DBS has become an accepted treatment option for various forms of dystonia [9, 22, 23]. In particular, inherited forms of dystonia tend to respond well to chronic pallidal stimulation [9]. While the benefit of DBS is often seen only with a delay of weeks and months in patients with dystonia [24], in some forms of dystonia, in particular in the case of dystonic storm, improvement may be observed within hours or days [9, 13, 15].
There is a limited experience with DBS in patients with GNAO1-related dystonia. According to the limited experience published thus far, these patients tend to respond well to pallidal DBS in the context of dystonic storm [7,8,9,10,11,12,13,14,15,16,17]. For instance, pallidal DBS has been used as an emergency measure to abate the severe dyskinesias and to restore normal daily functioning including feeding and sleeping [7, 13].
Our report highlights that pallidal DBS may be used as a life-saving treatment in an emergency context in patients with GNAO1-related dystonic storm abating also subsequent severe complications such as rhabdomyolysis and the rare occurrence of acute colitis.
Data availability
Upon reasonable request.
References
Allen NM, Lin JP, Lynch T, King MD (2014) Status dystonicus: a practice guide. Dev Med Child Neurol 56(2):105–112
Termsarasab P (2017) Frucht SJ (2017) Dystonic storm: a practical clinical and video review. J Clin Mov Disord 4:10. https://doi.org/10.1186/s40734-017-0057-z
Walcott BP, Nahed BV, Kahle KT et al (2012) Deep brain stimulation for medically refractory life-threatening status dystonicus in children. J Neurosurg Pediatr 9(1):99–102
Garone G, Graziola F, Nicita F et al (2020) Prestatus and status dystonicus in children and adolescents. Dev Med Child Neurol 62(6):742–749
Iodice A, Pisani F (2019) Status dystonicus: management and prevention in children at high risk. Acta Biomed 90(3):207–212
Levi V, Zorzi G, Messina G et al (2019) Deep brain stimulation versus pallidotomy for status dystonicus: a single-center case series. J Neurosurg 134:197–207
Danti FR, Galosi S, Romani M et al (2017) GNAO1 encephalopathy: broadening the phenotype and evaluating treatment and outcome. Neurol Gen 3(2):e143
Tisch S, Kumar KR (2021) Pallidal deep brain stimulation for monogenic dystonia: the effect of gene on outcome. Front Neurol 11:630391. https://doi.org/10.3389/fneur.2020.630391
Honey CM, Malhotra AK, Tarailo-Graovac M et al (2018) GNAO1 mutation–induced pediatric dystonic storm rescue with pallidal deep brain stimulation. J Child Neurol 33(6):413–416
Benato A, Carecchio M, Burlina A (2019) Long-term effect of subthalamic and pallidal deep brain stimulation for status dystonicus in children with methylmalonic acidemia and GNAO1 mutation. J Neural Transm (Vienna) 126(6):739–757
Kulkarni N, Tang S, Bhardwaj R (2016) Progressive movement disorder in brothers carrying a GNAO1 mutation responsive to deep brain stimulation. J Child Neurol 31(2):211–214
Koy A, Cirak S, Gonzalez V et al (2018) Deep brain stimulation is effective in pediatric patients with GNAO1 associated severe hyperkinesia. J Neurolog Sci 391:31–39
Danhofer P, Balintova Z, Balaz M et al (2021) Brittle biballism-dystonia in a pediatric patient with GNAO1 mutation managed using pallidal deep brain stimulation. Mov Disord Clin Pract 8:153–155
Yamashita Y, Ogawa T, Ogaki K et al (2020) Neuroimaging evaluation and successful treatment by using directional deep brain stimulation and levodopa in a patient with GNAO1-associated movement disorder: a case report. J Neurolog Sci 411:116710. https://doi.org/10.1016/j.jns.2020.116710
Yilmaz S, Turhan T, Ceylaner S et al (2016) Excellent response to deep brain stimulation in a young girl with GNAO1-related progressive choreoathetosis. Childs Nerv Syst 32(9):1567–1568
Miyamoto S, Nakashima M, Fukumura S et al (2022) An intronic GNAO1 variant leading to in-frame insertion cause movement disorder controlled by deep brain stimulation. Neurogenetics 23(2):129–135
Waak M, Mohammad SS, Coman D et al (2018) GNAO1-related movement disorder with life-threatening exacerbations: movement phenomenology and response to DBS. J Neurol Neurosurg Psychiatry 89(2):221–222
Alam M, Sanghera MK, Schwabe K et al (2016) Globus pallidus internus neuronal activity: a comparative study of linear and non-linear features in patients with dystonia or Parkinson’s disease. J Neural Transm (Vienna) 123(3):231–240
Runge J, Nagel JM, Cassini L et al (2022) Are transventricular approaches associated with increased hemorrhage? A comparative study in a series of 624 deep brain stimulation surgeries. Oper Neurosurg in press
Nakamura K, Kodera H, Akita T et al (2013) De novo mutations in GNAO1, encoding a Gao subunit of heterotrimeric G proteins, cause epileptic encephalopathy. Am J Hum Gen 93(3):496–505
Arya R, Spaeth C, Gilbert DL et al (2017) GNAO1-associated epileptic encephalopathy and movement disorders c607G>A variant represents a probable mutation hotspot with a distinct phenotype. Epileptic Disord 19(1):67–75
Moro E, Gross RE, Krauss JK (2013) What’s new in surgical treatment for dystonia? Mov Disord 28(7):1013–1020
Lozano AM, Lipsman N, Bergman H et al (2019) Deep brain stimulation: current challenges and future directions. Nat Rev Neurol 15(3):148–160
Reese R, Volkmann J (2017) Deep brain stimulation for the dystonias: evidence, knowledge gaps, and practical considerations. Mov Disord Clin Pract 4(4):486–494
Funding
Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and Affiliations
Contributions
HC, JCSB, and JKK prepared the first version of the manuscript. All authors were involved in taking care and coordinating treatment. All authors critically reviewed, worked on the manuscript, and consented with its final version.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This case report complies with the established ethics rules at Hannover Medical School. The parents gave informed consent to perform surgery.
Consent for publication
Since this case report does not contain any identifying information, consent for publication is not needed.
Conflict of interest
JKK is a consultant for Medtronic and Boston Scientific. All other authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Chaib, H., Schoene-Bake, JC., Saryyeva, A. et al. DBS emergency surgery for treatment of dystonic storm associated with rhabdomyolysis and acute colitis in DYT-GNAO1. Childs Nerv Syst 38, 1821–1824 (2022). https://doi.org/10.1007/s00381-022-05582-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00381-022-05582-9