
Abstract
Background and purpose
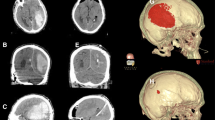
Spontaneous intracerebral hemorrhage (ICH) continues to be a major medical and socioeconomic problem. While the surgical procedure failed to show benefits over functional outcome, a less invasive and quicker surgical decompression might improve the outcome. The authors introduced endoscopy-guided evacuation in managing ICH and reports the benefits over the conventional method.
Materials and methods
Twenty-seven cases underwent endoscopic evacuation of ICH (Group E). The clinical features and outcomes were compared to the retrospective data of 20 cases who underwent computer tomography (CT)-guided stereotactic removal of ICH (Group C). Confidence level less than 0.05 was considered statistically significant.
Results
While the clinical features of the two groups were not significantly different except for the ICH volume, outcomes were better in all aspects in Group E. The patients in Group E required shorter operative time (72 min vs 102 min, p < 0.01) with better hematoma evacuation (95.5% vs 75%, p < 0.01), shorter stay in the intensive care unit (ICU; 4.2 days vs 6.9 days, p < 0.01) and less frequent CT scanning (6.4 times vs 8.6 times, p < 0.01) compared to the patients in Group C. Neurological outcome improved significantly in Group E 1 week after surgery (p < 0.01), but not in Group C. Glasgow outcome scale at 6 months were better in Group E than in Group C (p < 0.05). Nine patients (33%) showed good recovery at 6 months postoperatively after endoscopic evacuation of ICH.
Conclusion
Endoscopic hematoma evacuation provided the quick, adequate decompression of ICH. The outcomes were better than the CT-guided hematoma removal. Further study is necessary to evaluate the real benefit of this surgical procedure over the functional outcome of ICH.

Similar content being viewed by others


References
Auer LM, Deinsberger W, Niederkorn K, Gell G, Schneider G, Holzer P, Bone G, Mokky M, Korner E, Kleinert G, Haussch S (1989) Endoscopic surgery versus medical treatment for spontaneous intracerebral hematoma; a randomized study. J Neurosurg 70:804–811
Backlund EO, Holst H (1978) Controlled subtotal evacuation of intracerebral hematomas by stereotactic technique. Surg Neurol 9:99–101
Batjer HH, Reisch JS, Allen BC, Plaizier LJ, Su CJ (1990) Failure of surgery to improve outcome in hypertensive putaminal hemorrhage. A prospective randomized trial. Arch Neurol 47:1103–1106
Broderick JP, Adams HP Jr, Barsan W, Feinberg W, Feldmann E, Grotta J, Kase C, Krieger D, Mayberg M, Tilley B, Zabramski JM, Zuccarello M (1999) Guidelines for the management of spontaneous intracerebral hemorrhage: a statement for healthcare professionals from a special writing group of the Stroke Council, American Heart Association. Stroke 30:905–915
Jennett B, Bond M (1975) Assessment of outcome after severe brain damage. A practical scale. Lancet 1:480–484
Juvela S, Heiskanen O, Poranen A, Valtonen S, Kuurne T, Kaste M, Troupp H (1989) The treatment of spontaneous intracerebral hemorrhage. A prospective randomized trial of surgical and conservative treatment. J Neurosurg 70:755–758
Kanaya H, Yukawa H, Itoh Z, Kagawa Y, Kanno T, Kuwabara T, Mizukami K (1978) A neurological grading for patients with hypertensive intracerebral hemorrhage and a classification for hematoma location on computed tomography. In: Proceeding, seventh conference on surgical treatment of stroke, Tokyo. Neuron, pp 265–270 (Jpn)
Kanaya H, Kuroda K (1992) Development in neurosurgical approaches to hypertensive intracerebral hemorrhage. In: Kaufman H (ed) Intracerebral hematomas. Raven, New York, pp 197–210
Matsumoto K, Hondo H (1984) CT-guided stereotaxic evacuation of hypertensive intracerebral hematomas. J Neurosurg 61:440–448
McKissock W, Richardson A, Taylor J (1961) Primary intracerebral haemorrhage. A controlled trial of surgical and conservative treatment in 180 unselected cases. Lancet 2:221–226
Mohadjer M, Braus DF, Myers A, Scheremet R, Krauss JK (1992) CT-stereotactic fibrinolysis of spontaneous intracerebral hematomas. Neurosurg Rev 15:105–110
Morgenstern LB, Frankowski RF, Shedden P, Pasteur W, Grotta JC (1998) Surgical treatment for intracerebral hemorrhage (STICH): a single-center, randomized clinical trial. Neurology 51:1359–1363
Niizuma H, Suzuki J (1988) Stereotactic aspiration of putaminal hemorrhage using a double track aspiration technique. Neurosurgery 22:432–436
Niizuma H, Suzuki J (1989) Results of stereotactic aspiration in 175 cases of putaminal hemorrhage. Neurosurgery 24:814–819
Nishihara T, Teraoka A, Morita A, Ueki K, Kakai K, Kirono T (2000) A transparent sheath for endoscopic surgery and its application in surgical evacuation of spontaneous intracerebral hematomas. J Neurosurg 92:1053–1055
Zuccarello M, Brott T, Derex L, Kothari R, Sauerbeck L, Tew J, Van Loveren H, Yeh HS, Tomsick T, Pancioli A, Khoury J, Broderick J (1999) Early surgical treatment for supratentorial intracerebral hemorrhage: a randomized feasibility study. Stroke 30:1833–1839
Author information
Authors and Affiliations
Corresponding author
Additional information
Presented at the Third World Conference of the International Study Group on Neuroendoscopy (ISGNE), Marburg, Germany, 15–18 June 2005.
Rights and permissions
About this article
Cite this article
Nishihara, T., Morita, A., Teraoka, A. et al. Endoscopy-guided removal of spontaneous intracerebral hemorrhage: comparison with computer tomography-guided stereotactic evacuation. Childs Nerv Syst 23, 677–683 (2007). https://doi.org/10.1007/s00381-007-0325-6
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00381-007-0325-6