
Abstract
Chronic inflammatory gastrointestinal diseases such as Crohn's disease (CD) and ulcerative colitis (UC) are known as inflammatory bowel disorders (IBD). Patients with inflammatory bowel illnesses are more susceptible to viral infections. In people with IBD, viral infections have emerged as a significant issue. Viral infections are often difficult to identify and have a high morbidity and fatality rate. We reviewed studies on viral infections and IBD, concentrating on Cytomegalovirus (CMV), SARS-CoV-2, Epstein-Barr virus (EBV), enteric viruses, and hepatitis B virus (HBV). Also, the effect of IBD on these viral infections is discussed. These data suggest that patients with IBD are more likely to get viral infections. As a result, practitioners should be aware of the increased risk of viral infections in inflammatory bowel disease patients.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Inflammatory bowel disorders (IBD) are persistent inflammation of the lining of the colon and small intestine, including Crohn's disease (CD) and ulcerative colitis (UC), which refer to a range of chronic inflammatory conditions affecting the gastrointestinal tract [1, 2]. Whereas UC often comprises superficial inflammation of the rectum with expansion into adjacent mucosa in a continuous manner, Crohn's disease is defined by transmural inflammation affecting any portion of the gastrointestinal tract. A third IBD subtype, indeterminate colitis (IC), is characterized by mucosal inflammation and shares characteristics with UC and CD. Internationally, IBD incidence is on the rise, according to recent studies. As many as 11.4 new cases per 100,000 people have been reported annually in North America children and teenagers under 18 accounts for 25% of all IBD cases. Compared to IBD that develops in adults, pediatric IBD is frequently more severe and widespread [3]. Crohn's disease causes inflammation throughout the gastrointestinal (GI) system, from the mouth to the rectum, with the terminal ileum and colon most affected. On the other hand, ulcerative colitis usually produces long-term inflammation and ulcers in the rectum mucosa and colon. The CD is distinguished histologically by thickened submucosa, transmural inflammation, non-ceasing granulomas, and fissuring ulceration. In contrast, UC causes superficial inflammatory changes limited to the mucosa, and sepulcher and cryptitis abscesses [4]. Recent studies have demonstrated the potential of mAbs to treat IBD, particularly moderate-to-severe UC, and CD. These studies show how mAbs can precisely target inflammatory pathways at the molecular level. Vedolizumab (VDZ), ustekinumab (UST), Infliximab (IFX), and adalimumab (ADA) for both UC and CD, as well as golimumab (GOL) for UC, are biological treatments that have become available for patients who have not responded adequately to conventional therapies such as immunosuppressants, corticosteroids, and aminosalicylates (5-ASAs) [5]. Patients with UC often are undertreated because of the possibility of curative colectomy and the perception that the disease burden is lower than that of CD. Earlier initiation of disease-modifying drugs might reduce the progression of UC after surgery. However, UC might not cause the irreversible damage observed in patients with CD [6].
Persistent pain in the abdomen is a common sign of IBD, but it is poorly recognized. Furthermore, many people experience pain in their extraintestinal joints or musculoskeletal system [7]. Other common symptoms of IBD include stomach pain, weakness, delayed diarrhea, weight loss, fever, and, in severe cases, rectal bleeding [8].
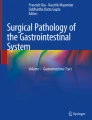
There are several potential methods by which food may cause intestinal inflammation, including effects on gastrointestinal permeability, changes in the gut microbiome, and direct dietary antigens. Many immune-mediated inflammatory illnesses are linked to dysregulated reactions to the common microbiota, which can cause inflammation. This includes the inflammatory bowel illnesses UC and CD, which are generally acknowledged to derive from dysregulated adaptive immune responses to the microbiota in genetically vulnerable individuals. Even though many genetic polymorphisms overlap, UC and CD have different seroreactivities to microbiota antigens. Patients with CD respond to various antigens, while those with UC specifically react to a cross-reactive antigen with perinuclear antineutrophil cytoplasmic antibodies [9, 10]. An increasing body of evidence suggests that gut bacteria play a role in the intestinal epithelial injury. Many factors can affect the microbial composition and its diversity in the gut, including diet, environmental factors, stress, lifestyle, exogenous probiotics, and antimicrobial medicines, which may influence intestinal homeostasis [11]. IBD pathogenesis involves both innate and adaptive immune system cells. T helper 9 (Th9), Th17, Th92, Treg 6 cells, B cells, and Th1 have all been linked to the beginning or development of intestinal inflammation in IBD. T cells have received a great deal of attention, which has led to breakthroughs such as the creation of efficient medications that target T-cell migration. However, various innate and adaptive immune cells with significant immunological functions are present in the intestinal mucosa (Fig. 1) [12]. The Th2 cytokines IL-4, IL-13, and IL-5 have also been shown to play a role in the pathogenesis of UC, according to numerous studies. NKT cells also contribute to producing these Th2 cytokines [13]. Interferon (IFN-γ), IL-6, and tumor necrosis factor-α (TNF-α), which encourage IL-23A and IL-12 release by dendritic cells and macrophages, are the central Th1-type cytokines produced in CD. Production of Th2-type cytokines and, to a lesser extent, IFN- distinguishes UC [14]. IBD can be treated with immunomodulators such as steroids and azathioprine, and biologics such as anti-tumor necrosis factor (TNF) and anti-integrin monoclonal antibodies. However, anti-TNF treatment can lead to opportunistic infections (such as bacterial, fungal, and viral infections) (Table 1), and the danger is more significant when it is used with steroids [15]. In this article, we look at viruses that play a role in the onset or progression of IBD.

(A) In pathogenic bacteria and viruses (dysbiosis), injury, or xenobiotics, microbe-associated molecular patterns stimulate the production of pro-inflammatory cytokines (IL-1, IL-6, and IL-18 from epithelial cells and IL-6, IL-12, and IL-23 from DCs and macrophages) that induce the development of the effector CD4 + T cells TH1 and TH17. Depending on the cytokine milieu, TH2 or TH9 cells are generated that mediate TH2-type responses or impair epithelial barrier function, respectively. Intestinal innate lymphoid cells, including NK-like cells, respond to pro-inflammatory cytokines upregulating IL-22, which protects the epithelial barrier. (B) A balanced commensal microbiota (eubiosis), intestinal epithelial cells secrete mucins and antimicrobial peptides, and MAMPs induce the secretion of epithelial cytokines (TSLP, IL-33, IL-25, and TGF-β) that promote the development of tolerogenic DCs and macrophages. Activated antigen-presenting cells (APC) initiate differentiation of naïve CD4 + T-cells into Th-2 effector cells (which produce pro-inflammatory cytokines such as TNF-α, IL-5, IL-6, and IL-13). TNF-α and IL-1 activate the nuclear factor κB (NF-κB) pathway, facilitating the expression of pro-inflammatory and cell survival gene expression [100]
Cytomegalovirus (CMV)
The CMV genome has the largest genome in the human herpesvirus family, with a genome size of 236 kbp and more than 200 open reading frames (ORFs). Herpesviruses have an icosahedral capsid that contains a double-stranded DNA genome [16]. Previous studies indicated that pro-inflammatory cytokines in IBD patients, such as interferon-γ, TNF-α, and IL-2, can increase the production of chemokines and transcription molecules, leading to activated T-cells and increased CMV reactivation [17]. CMV is more frequent in pediatric patients with severe refractory colitis with colonic biopsies. CMV load in mucosal biopsies, on the other hand, did not appear to be associated with clinical outcomes, particularly viral clearance from mucosal biopsies and the ultimate requirement for colectomy. This means that even a tiny amount of CMV can trigger a cascade of inflammatory responses in the patient, leading to refractory disease [18]. Because CMV is a common cause of refractory disease, individuals with acute severe steroid-refractory ulcerative colitis should be tested for the infection. Herpes simplex colitis is less prevalent in ulcerative colitis patients and is usually associated with immunosuppression [19]. In immunocompromised hosts, CMV colitis is an end-organ infectious consequence that is relatively frequent and hurts clinical outcomes. The development of CMV colitis, linked to unfavorable effects, is more likely to occur in adults with IBD. Due to the lack of clinical or endoscopic signs that distinguish CMV colitis from colitis linked to inflammatory illness, diagnosing CMV colitis in IBD patients is challenging. It relies solely on identifying histological or viral markers in the intestinal mucosa [20]. CMV colitis has been linked to active illness, immunosuppressive medicine, steroid therapy, and steroid-refractory disease progression in IBD patients [21, 22]. CMV disease requires antiviral therapy, but the timing and duration of the treatment depend on the amount of virus in the tissues. CMV infection must be treated in high-grade cases, whereas immunosuppression may be effective in low-grade cases. Generally, the drug for treating CMV disease is ganciclovir [23]. Researchers compared non-overlapping years from 2003 to 2016 from the Kids Inpatient Database (KID) and National Inpatient Sample (NIS). Researchers examined an overall total of 254,839 hospitalizations for IBD. All patients under 21 who had CD and UC were included. Measures of outcomes, such as in-hospital mortality, the use of medical resources, and the severity of the disease, were compared between patients with and without concurrent CMV infection at the time of admission. The total prevalence rate of CMV infection was 0.3%, and there was a general trend toward higher prevalence (P = 0.001). Two-thirds of patients with CMV infection had UC, linked to a nearly 3.6-fold higher risk of CMV infection. Patients with IBD and CMV had more coexisting diseases. In-hospital mortality was significantly elevated by CMV infection (odds ratio (OR): 3.58; confidence interval (CI): 1.85 to 6.93, P 0.001), as was the likelihood of having severe IBD (OR: 3.31; CI: 2.54 to 4.32, P 0.001). In children with IBD, CMV infection is becoming more common. CMV infections significantly increase mortality risk and IBD severity, resulting in more extended hospital stays and more expensive hospitalization [24].
Examining the Connection Between the Pandemic SARS-CoV-2 and IBD
COVID-19 is a contagious respiratory illness that causes a wide range of symptoms. The first case of COVID-19 patients was discovered in Wuhan, China, and it immediately became a public health disaster [25, 26]. This virus's genome contains several smaller open reading frames (ORFs). The ORF gene family encodes structural proteins such as the spike (S) glycoprotein, nucleocapsid (N) proteins, membrane (M), and nonstructural proteins (NSP). Angiotensin-converting enzyme 2 (ACE2) host cell is a receptor for the S protein of SARS-CoV-2 [25, 27]. A recent meta-analysis of 14 studies, extensively included 50,706 IBD patients, investigated the risk of COVID-19 or COVID-19-related death in patients with IBD. By October 2020, 1% of patients with IBD have COVID-19, a very low prevalence. Only the use of steroids appears to affect the risk of COVID-19, contrary to the presumption that immunosuppressed individuals would be more susceptible to COVID-19 and severe COVID-19 [28]. In a study, Aziz et al. reported that in IBD patients receiving immunosuppressive drugs, SARS-COV-2 reduced ACE2 expression in the gastrointestinal tract of IBD patients [29]. Therefore, treating IBD patients with immunosuppressive drugs has little effect on protecting IBD patients against COVID-19 because the reduced expression of ACE2 in gastrointestinal epithelial cells facilitates viral entry and infection in the patient [29, 30]. Researchers identified high cytoplasmic proteins ACE2 and TMPRSS2 in the colonic epithelium in UC. ACE2 may have a broader role in modulating gut homeostasis, microbiota, and inflammatory response [31, 32]. Notable are the plasma cells that express ACE2 in the inflamed IBD gut. The high expression of ACE2 and TMPRSS2, along with the opposition of plasma cells in the gut lamina propria, suggests that the digestive tract may play a role in SARS-CoV-2 entry and the antecedent host humoral immune response in COVID-19, even though primary data does not explicitly link gut inflammation to the SARS-CoV-2 entry mechanism [33, 34].
There were 73 HCs, and 235 patients in total (IBD unclassified (IBDU): 1.7%. CD: 28.9%, UC: 69.4%), of the 235 patients, 128 (54.5%) were using immunosuppressants, while 107 (45.5%) were not. Two (0.9%) of the 74 seropositive patients had a history of SARS-CoV-2 infection, and none had received the COVID-19 vaccine. Patients with and without immunosuppressants had similar seroprevalence (32% vs. 27%, p > 0.05) and between patients with and without IBD (28.1% vs. 36%, p > 0.05). Indicating a high seroprevalence in patients with IBD from Northern India, up to 1/3 of IBD patients were seropositive for immunoglobulin G (IgG) SARS-Cov-2 antibodies [35]. In other investigations, researchers found that patients with IBD treated with the anti-TNF drug infliximab, which was linked to an increased risk of SARS-CoV-2 infection, had vaccine-induced antibody responses that were less robust and lasting than patients treated with the anti-integrin drug vedolizumab, which has a gut-specific mode of action and does not result in systemic immunosuppression. These findings, and data from other immunosuppressed patient populations, have given evidence supporting the prioritization of third primary SARS-CoV-2 vaccine doses for patients with IBD who receive immunosuppressive therapy [36, 37].
Epstein-Barr Virus (EBV)
EBV, a herpes virus that infects 95 percent of the world's population, spreads through bodily fluids and blood [38]. The EBV, particularly well-known for infecting B cells, is linked to several cancers and autoimmune diseases and can cause inflammatory diseases such as Crohn's disease and ulcerative colitis. Earlier studies have indicated that EBV-positive cells are detected in the colonic mucosa of IBD patients, which are caused by increased B cells and increased EBV replication after immunosuppressive therapy [39, 40]. Another study indicated that EBV DNA induced pro-inflammatory responses by activating Toll-like receptor (TLR) signaling [41]. Andari et al. reported that administration of EBV DNA to a mouse colitis model increased the expression of IL-17A, IFN-λ, and TNF-α in the colon tissues of the colitis mice compared to the control group. As a result, it increases the severity of colon damage. These findings indicate that EBV DNA increases pro-inflammatory responses in colitis [42]. Study results showed that EBV infection increases the prevalence of lymphoproliferative disorders in IBD patients after using immunosuppressive drugs [43]. Resulting in a refractory response and increasing severity to anti-TNF-α agents, corticosteroids, and viral surveillance for EBV in individuals with refractory UC may aid in understanding the patient’s pathophysiology. In addition to predicting medication response, developing antiviral therapies may improve the outcomes of the patients [44]. A 37-year-old man with CD and two men with UC, aged 52 and 38, also developed non-B-cell Hodgkin's lymphoma linked to the EBV while receiving therapy for IBD. The first two patients underwent proctocolectomy, and immunosuppressive agents were discontinued, after which the lymphoma disappeared. For treating steroid-refractory IBD, azathioprine and 6-mercaptopurine are the main choices. These immunomodulatory agents have been implicated in developing EBV-positive lymphomas in solid organ transplant settings. Although this type of lymphoma is a rare complication of IBD, the incidence in referral centers seems to be rising. Since azathioprine is a vital medication for IBD, it is necessary to identify IBD patients at risk for developing lymphoma. EBV-DNA in blood or feces may be a potential tumor marker [45]. In a cutting-edge study, researchers in China conducted a cross-sectional analysis and discovered that 33 of 99 IBD patients (33.3%) had EBV detectable in their bodies. High clinical disease activity in IBD patients may be caused by EBV prevalence in colonic mucosa [46]. In a different investigation, researchers demonstrated that a UC patient had EBV found in the rectum and terminal ileum. Overall clinical findings in this patient were consistent with UC. His condition improved after receiving the recommended UC treatment, as the colonoscopy showed. Whether EBV is an accelerator or a bystander in the etiology of IBD is difficult to ascertain [47].
EBV-associated lymphoproliferative disorders (LDP) are commonly observed in patients with congenital or acquired immunodeficiency. The liver, spleen, bone marrow, skin, and lymph nodes, the most implicated organs, are classified as EBV + B cell LPD or EBV + T/NK cell LPD, covering disease entities with a wide clinicopathologic range. Because the symptoms of EBV-associated LPD are similar to those of IBD in immunocompetent people, most patients are misdiagnosed [48, 49]. The following clinical distinctions between IBD and EBV-LPD with gastrointestinal involvement are listed: 1. In EBV-LPD patients, fever, particularly unexplained high fever, is more common. Suspected IBD cases with a fever, but no infection is detected [48]. 2. Enlargement of the liver, spleen, and lymph nodes is commonly observed in EBV-LPD patients. The differential diagnosis of EBV-LPD is difficult if the lesions are only found in the gastrointestinal system. In contrast to EBV-LPD cases, some IBD patients may experience extraintestinal symptoms such as primary sclerosing cholangitis, fatty liver, cholelithiasis, and IgG4-related cholangitis [41]. EBV-associated LPD with digestive tract involvement in immunocompetent patients is relatively rare and often misdiagnosed; therefore, diagnosing these entities is often challenging. However, testing for EBV-DNA, VCA-IgG, and EA-IgG may aid in the differential diagnosis of EBV-associated LPD [48]. Researchers conducted a study to describe the EBV status in a juvenile IBD population, focusing on patients starting thiopurines. Of the 688 juvenile IBD patients we studied, only 150 (22%) had verified EBV status, regardless of course of therapy or age. 83% of those underwent screening, but only 17% had any reason to suspect an acute illness. Before beginning treatment, 64 (52%) of the screened patients were examined, and only 40% had IgG-positive results. The mean age of the seronegative and seropositive groups did not differ. Most (63%) patients receiving thiopurine therapy had negative IgG antibodies before treatment. At a mean (SD) of 2 1.5 years after starting medication, thiopurines were associated with 80% of primary EBV infections. Most pediatric IBD patients with verified EBV status were IgG-negative when thiopurine therapy was started. Thiopurines were additionally linked to initial EBV infection [50].
Association of Enteric Viruses with IBD
Enteric viruses include enteroviruses, rotaviruses, norovirus, adenovirus, and sapovirus. Enteroviruses are RNA viruses of the Picornaviridae family. Enteric viruses could cause gastroenteritis, encephalitis, respiratory infections, hepatitis, and paralysis [51]. Interactions between enteric viruses and bacteria in the gastrointestinal tract show that these interactions are crucial in regulating enteric virus infections in IBD [52]. The enterovirus was found in the terminal ileum of CD patients, according to Nystrom et al. [53]. Interactions between enterovirus and HBGA-like molecules explain why these viruses are harmful during IBD [54]. The most extensive current study included data-crossing from 9403 patients in whom 13,231 stool tests were carried out using a gastrointestinal pathogen PCR panel over two years. It demonstrated a clear connection between enteric viruses and IBD flare-ups. In this study, Axelrad et al. compared 577 IBD patients (277 CD and 300 UC) to 8826 controls and found that both CD and UC patients experienced higher rates of Enteroinvasive Escherichia coli (EIEC) and enteric infections (such as norovirus; p 0.001) during IBD flare-ups [55, 56]. During their 1-year trim-estral follow-up, 286 IBD patients participated in a prospective study in the Dutch cohort to look for enteric viruses in stool samples. The findings revealed a low incidence of enteric viruses in both active and baseline IBD, and there was no epidemiological evidence between enteric virus infections and disease activity [57].
Biological processes of enteric viral interactions during IBD include the recruitment of inflammatory cells in the mucosa and the production of pro-inflammatory cytokines. TNF-α and IFN-λ secretion is induced by enteric viruses and is implicated in IBD pro-inflammatory pathways. Cytokines such as IL-17, IFN-λ, Th1, and Th17 worsen the symptoms of CD and UC [58]. Enteric viral infections in children have been studied to discover whether immune suppression increases the risk of viral gastroenteritis. Research gathered 151 fecal samples from HIV-infected infants and adults, both with and without diarrhea. Calicivirus (norovirus family) infection was more common in HIV-positive children (51% vs. 24%) than in HIV-negative children [59] (see Table 2).
Rotavirus (RV)
RV is a non-enveloped triple-layered segmented double-stranded RNA (dsRNA) virus that infects mature intestinal epithelial cells (IECs). It is the most significant cause of dehydration, diarrhea, and severe gastroenteritis in young children and newborns worldwide, with over 200,000 deaths each year [60]. RV has long been considered a winter illness, particularly in temperate climates. RVs are divided into ten different species (A-J). Rotaviruses of species A are the most common source of infections in children, with species B and C accounting for a lesser but significant percentage of infections worldwide [61]. The RV vaccination, approved for use in newborns in 2006, was suspected of causing an increase in the frequency of IBD among children in the United States. Attenuated RV vaccination may cause immunological dysregulation and inflammation of the gut mucosa. The findings of this sizeable pediatric cohort show a slight increase in IBD incidence in young children over ten years. Still, according to the results, RV vaccination is not associated with the development of IBD [62, 63]. In the past, 6-TG was used to treat cancer, but nowadays, it is widely used to suppress the immune system during organ transplantation. Additionally, it is used to treat autoimmune disorders and pediatric acute lymphoblastic leukemia [64]. To understand the mode of action of 6-TG on RV replication, researchers used laboratory RV strain (SA11). 6-TG decreases RV replication in the intestinal epithelium. Rac1 gene knockout or knockdown, a cellular target of 6-TG, significantly reduces RV replication, showing that Rac1 plays a supporting role in RV infection. They also showed that 6-TG might effectively suppress the active form of Rac1 (GTP-Rac1), which is thought to cause 6-TG's anti-RV activity. Unlike overexpression of GTP-Rac1, RV replication is inhibited by an inactive Rac1 (N17) or a particular Rac1 inhibitor (NSC23766). Finally, 6-TG inhibits RV replication by inhibiting Rac1 activation. Thus, the 6-TG is a reasonable therapeutic option for IBD patients infected with RV or at risk of RV infection [64].
RV infection was associated with an increase in bactericides and Akkermansia genera in the ileum over time, and a decrease in Lactobacillus [65]. Increased secretion of the significant mucin protein Muc2 in the small intestine has also been linked to RV infection. Mucin-producing cell lines and human jejunal enteroids were examined in this study. According to in vitro and silico studies, Bacteroides thetaiotaomicron and Akkermansia mucinphila break down glycans that act as RV decoy receptors. The infectivity of RV was lowered when pure Muc2 from germ-free mice was incubated with it before the infection of MA104 cells. This response was blocked when germ-free Muc2 was pre-treated with A. mucinphila and B. thetaiotaomicron. These results suggest that A. mucinphila and B. thetaiotaomicron are involved in RV infection during the acute phase [66]. In another study, researchers used dextran sulfate sodium (DSS) to induce colitis 6 or 14 days after adult RV infection to see if RV imprinted long-lasting alterations in the intestinal immune system or microbiota that would have an effect on intestinal health in the future. In mature mice, viral clearance is often finished by day 6. Significantly, 1% DSS dosing did not change the viral shedding curve when given concurrently in the prior study. RV infection in adult mice is immunogenic but asymptomatic, mainly reflecting the response to vaccination. According to the findings, neither adult RV infection nor immunization affects the gut microbial population or the severity of inflammatory bowel disease in a wild-type environment. Neither the seriousness of subsequent DSS-induced colitis nor any substantial long-term alterations in the small or large intestine's microbial population was influenced by RV infection. Hence, adult mouse RV infection has no long-term consequences on intestinal homeostasis [67].
Norovirus (NV)
Noroviruses constitute a genus in the Caliciviridae family of positive-strand RNA viruses, including several additional genera. The norovirus virion comprises 90 dimers of the major capsid protein VP1 and one or two copies of the minor structural protein VP2. A virion containing a single major capsid protein is unique among animal viruses. It more closely resembles the capsid composition of plant viruses such as tomato bushy stunt, southern bean mosaic, and turnip crinkle. VP1 and VP2 are synthesized from a protein-linked subgenomic RNA containing ORF2 and ORF3 [68]. In humans, NV challenges have demonstrated higher amounts of Th1 lymphocytic cytokines such as IL-8, IL-10, and TNF. Following NV or RV infections, IFN-λ, IFN-α, and IFN-β may trigger an antiviral gene expression cascade. It is still unclear what function enteric virus infections play in IBD-related interferon pathway dysregulation. Because many patients receive anti-TNF drugs, the interferon antiviral response may be downregulated, affecting the course of intestinal epithelial repair. However, other pathways help to explain enteric viruses' preventative function in the onset of IBD. For example, enteric viruses may lessen intestinal inflammation by releasing interferon-β (IFN-β), mediated by TLR3 and TLR7 [57]. Previous studies showed that interactions between NV with tuft cells regulated the inflammatory cytokines such as IL-25 and IL-17 in the pathogenesis of IBD [69]. Other studies indicated that exchanging NVs with Enterobacter cloacae could inhibit NV binding to intestinal cells or increase NV infection in IBD patients [70].
Tarris et al. studied the interaction of human noroviruses (HuNoVs) and blood-type antigens in refractory CD and UC patients using HuNoV virus-like particles (VLPs) and histological tissues. Colon and rectum mucosal regeneration investigation revealed increased expression of sialylated Lewis x (sLex) and Lewis a (sLea) antigens, and HuNoV VLP binding in the absence of ABO antigen expression in CD and UC. Experimental competitions conducted with lectins, monoclonal, and sialidase antibodies revealed that HuNoV attachment was mainly dependent upon Lea and, to a lesser extent, Lex proteins on regenerative mucosa in both UC and CD. This research showed that during CD and UC flare-ups, Lex and Lea antigens, alone or in combination with a sialic acid moiety, were responsible for HuNoV capsid identification on inflammatory and healing tissues [71].
In a case–control retrospective analysis, Khan et al. found that NV infection is linked to IBD exacerbation. The fact that NV illness is more likely in the winter months is backed up by two recent research that implies the same thing. They conducted a retrospective chart analysis of patients with IBD experiencing an aggravation of their disease. An enzyme-linked immunoassay was used to check for the presence of NV in rectal and/or stool swab samples, age, sex, type of IBD, absence or presence of hematochezia, diarrhea, and the requirement for hospitalization were all assessed. The authors conclude that NV infection is more likely associated with hematochezia when IBD is present [72]. In another study, nine patients with IBD (8 UC/1 CD) had exacerbations with diarrhea. Eight had norovirus antigen in at least 1 sample. All nine patients with IBD presented bloody diarrhea and six of the eight norovirus-positive patients with IBD required hospitalization. All control patients experienced diarrhea; however, no hematochezia was noted, and no hospitalization was required. Several patients with IBD and controls remained positive for NV months after the initial positive stool and/or rectal swab sample. The virus appeared to be more common during winter months. This study showed that norovirus might be associated with exacerbations of IBD. When norovirus accompanies IBD, it is more likely to be associated with hematochezia than when the infection occurs without IBD [72].
Hepatitis B Virus and Inflammatory Bowel Disease (HBV and IBD)
The hepatitis B virus is a widespread infection worldwide. HBV is a DNA virus of the Hepadnaviridae family that is a significant cause of morbidity and mortality [73]. The prevalence of HBV infection varies geographically, with areas of low (< 2%), medium (2–7%), and high (> 8%) endemicity [74]. HBV prevalence in IBD patients has been studied in several research [75]. The reactivation of hepatitis is one of the concerns related to immunosuppressive treatments of IBD patients [76]. It is defined as the recurrence of viral replication, also a 1.5–twofold increase in alanine aminotransferase (ALT) levels compared with the baseline level [77]. In patients with IBD, HBV is an increased risk of liver fibrosis [78]. The mechanisms that promote the induction of liver fibrosis in patients with chronic hepatitis B include pathway signalings, such as WNT-signaling PI3K/Akt/mTOR Ras/ERK1/2 and p53 [79].
Immune modulators, monoclonal antibodies, and immune modulators such as anti-integrin drugs and anti-TNF-α agents have transformed the medical care of IBD patients [80]. In individuals with IBD, using these drugs has resulted in a better rate of mucosal healing. Infectious problems, mainly those preventable by immunizations, such as hepatitis B, are more common in patients with IBD. Although HBV's efficacy has been shown in the healthy population, studies on its effectiveness in patients with IBD who are on immunosuppression are limited [81]. In addition, Cekic et el. showed that the likelihood of achieving a sufficient immune response with standard HBV protocol in IBD patients was low, particularly in older patients with illness flare. A more immunogenic vaccination protocol in immunocompromised patients may be a better way to elicit an efficient immune response [82]. Kochhar et al. showed that IBD patients might benefit from a more extended hepatitis-B vaccination program. The authors reported a statistically inferior vaccine response in individuals with IBD compared to those without (healthy controls). According to a meta-analysis of 14 studies involving 2375 patients, IBD patients on immunosuppression had a considerably lower HBV response than the general population [83].
The Role of Bacteriophages in the Formation of Intestinal Dysbiosis and the Progression of IBD
Bacteriophages, as bacterial predators, are essential in microbial species evolution [84]. The structural contents of bacteriophages are composed of nucleic acid and protein. Phages exert their effects on their host, including four main methods: the lithic phase, the lysogenic phase, the quasi-lysogenic phase, and prophage. Since the human intestinal microbiome is essential in many diseases, it is expected to play an important role in IBD [85]. Bacteriophages, which predominate in the gut, have a role in forming intestinal dysbiosis, which aids the progression of IBD [86]. Caudovirales phages include Myoviridae, Podoviridae, Siphoviridae, and Microviridae members, all common in the human gastrointestinal tract [85]. The presence of phages in various kinds of IBD, such as UC and CD, is generally manifested differently. Phages are expressed differently in IBD patients than in healthy people (one phage may be more or less expressed than another). The caudovirales phage, for example, is negatively associated with various intestinal bacteria and is more prevalent in CD patients than in UC patients [87]. Phages in the gut are anticipated to impact the abundance and diversity of bacteria in IBD significantly. Bacteriophages influence the bacterial flora in the gut through multifactorial methods [87] (Fig. 2).

A simplified model of bacteriophages' potential function in gut flora management. A: Bacteriophages may boost the fitness of commensal bacteria in the healthy gut by transmitting genes that aid in eliminating dangerous bacteria or are environmentally advantageous. Furthermore, phages interact directly with glycoproteins in the mucous layer, providing defense against invading pathogens. The presence of phages in some healthy people's blood shows that they may be able to breach the gut epithelial barrier. B: In inflammatory bowel disease, more phages are detected in the mucous layer. Higher phage populations may have a role in reducing the number of commensal bacteria and accelerating the transfer of genes that benefit the environment to pathogenic bacteria. Because of the thinner mucosal barrier, phage interactions with mucosal glycoproteins may be decreased. If the epithelial barrier is breached, phage particles may travel into the lamina propria or circulation. In the lamina propria, phages may operate as a local immune response activators. After translocation into the systemic circulation, a systemic immune response may develop
Studies on the microviridae phage suggest an essential link between this virus and IBD. Microviridae and crAss-like phages, on the other hand, are primarily observed in healthy people [88]. Other studies have shown that in the early form of IBD, the ratio of caudovirales to microviridae is higher than in healthy individuals [89]. The virome is regarded as one of the most influential factors in the human gut microbiota but is also one of the least known [90]. Bacteriophages dominate the virome in many microbial communities, enhancing diversity, increasing nutrient turnover, and facilitating horizontal gene transfer. Understanding the role of bacteriophages in microbial community structures is crucial for recognizing and treating changes in the composition and diversity of the human gut microbiome, which are associated with various disorders, including IBD [91].
In a study published in 2020, Nishiyama et al. detected a bacteriophage in stool samples of UC patients that contaminates beneficial bacteria in intestinal homeostasis and causes IBD [92]. By bioinformatics tools, Farahmandzad et al. investigated differences in bacteria, fungi, archaea, and bacteriophage interactions in the gut microbial community of females and males in IBD patients. They discovered four bacteriophages for further research into IBD metabolism, including Enterobacteria phage If1, Escherichia phage pro147, Streptococcus phage SpSL1, and Streptococcus virusSfi19. In terms of microbial interactions, this finding demonstrated a remarkable similarity between females and males with UC and those of other study groups. According to this research, bacteriophages were the most common microbes detected in microbial interactions [93]. Because of the thinner mucosal barrier, phage interactions with mucosal glycoproteins may be decreased. Furthermore, defects in the epithelial barrier may allow numerous phage particles to migrate into the lamina propria or the bloodstream. In the lamina propria, the phage may function as a local immune response acivator. After transfer to the systemic circulation, a systemic immune response may ensue [87].
Conclusion
Inflammatory bowel disease, also known as the "disease of the century", is a complex condition affecting millions worldwide. Many variables, including lifestyle, gut microbial ecology, and genetics, influence IBD. However, the role of microorganisms in disease causation and treatment is unknown. We reviewed the evidence on viral infections and IBD, focusing on CMV, SARS-CoV-2, EBV, EV, and HBV. The studies discussed herein suggest that the risk of viral infections may be higher in individuals with IBD. Viral infections and IBD are intimately linked on numerous levels, including disease pathogenesis, consequences, and treatment, as well as, as a standalone therapy. Infections are still a leading cause of death in patients with IBD, a significant source of concern. Future research should be conducted to determine the link between viral infection and IBD, and the best treatment options for people infected with these viruses. Because no test exists to assess the degree of immunosuppression in people with IBD, future research should focus on biomarkers that can predict who is more likely to get opportunistic infections. Such biomarkers would allow for improved surveillance and preventative steps to be implemented during an outbreak. In addition, we must clarify and integrate the effects of the microbiome and environment on IBD and gain new insights into the mechanisms governing critical aspects of IBD, such as horizontal gene transfer, immunogenicity, and the composition and pathways of viruses.
References
Vernon-Roberts A et al (2020) Validation of a revised knowledge assessment tool for children with inflammatory bowel disease (IBD-KID2). Inflamm Intest Dis 5(2):70–77
Wong DJ et al (2019) Surgery in the age of biologics. Gastroenterol Rep 7(2):77–90. https://doi.org/10.1093/gastro/goz004
Ghione S et al (2018) Dramatic increase in incidence of ulcerative colitis and Crohn’s disease (1988–2011): a population-based study of French adolescents. Off J Am Coll Gastroenterol ACG 113(2): 265-272. https://doi.org/10.1038/ajg.2017.228
Kmieć Z, Cyman M, Ślebioda TJ (2017) Cells of the innate and adaptive immunity and their interactions in inflammatory bowel disease. Adv Med Sci 62(1):1–16. https://doi.org/10.1016/j.advms.2016.09.001
Mocci G et al (2023) Real-world efficacy and safety of vedolizumab in managing ulcerative colitis versus Crohn’s disease: results from an Italian multicenter study. Expert Opin Biol Ther. https://doi.org/10.1080/14712598.2023.2185510
Le Berre C et al (2020) Ulcerative colitis and Crohn’s disease have similar burden and goals for treatment. Clin Gastroenterol Hepatol 18(1):14–23. https://doi.org/10.1016/j.cgh.2019.07.005
Sweeney L et al (2021) Pain management in inflammatory bowel disease: feasibility of an online therapist-supported CBT-based self-management intervention. Pilot Feasibility Stud 7(1):1–15. https://doi.org/10.1186/s40814-021-00829-9
Zhang M et al (2017) Interactions between Intestinal Microbiota and Host Immune Response in inflammatory bowel disease. Front Immunol. https://doi.org/10.3389/fimmu.2017.00942
Lee HS, Lee KJ (2019) Immunoglobulin G4-related immune responses to common food antigens in patients with ulcerative colitis and Crohn’s disease. Turk J Gastroenterol 30(5):408. https://doi.org/10.5152/tjg.2019.18466
Alexander KL et al (2021) Human microbiota flagellins drive adaptive immune responses in Crohn’s disease. Gastroenterology 161(2):522-535.e6. https://doi.org/10.1053/j.gastro.2021.03.064
Sheehan D, Moran C, Shanahan F (2015) The microbiota in inflammatory bowel disease. J Gastroenterol 50(5):495–507. https://doi.org/10.1007/s00535-015-1064-1
Dharmasiri S et al (2021) Human intestinal macrophages are involved in the pathology of both ulcerative colitis and Crohn disease. Inflamm Bowel Dis 27(10):1641–1652. https://doi.org/10.1093/ibd/izab029
Lai LJ, Shen J, Ran ZH (2019) Natural killer T cells and ulcerative colitis. Cell Immunol 335:1–5. https://doi.org/10.1016/j.cellimm.2018.08.010
Mitsialis V et al (2020) Single-cell analyses of colon and blood reveal distinct immune cell signatures of ulcerative colitis and Crohn’s disease. Gastroenterology 159(2):591-608.e10. https://doi.org/10.1053/j.gastro.2020.04.074
Mushtaq K et al (2020) Trends and outcomes of fungal infections in hospitalized patients of inflammatory bowel disease: a nationwide analysis. Transl Gastroenterol Hepatol 5:35–35. https://doi.org/10.21037/tgh.2019.10.14
Weiss K, Gard S (2013) Cytomegaloviruses. Rinderpest Virus. Lumpy Skin Disease Virus. Springer, New York
Hommes DW et al (2004) The pathogenicity of cytomegalovirus in inflammatory bowel disease: a systematic review and evidence-based recommendations for future research. Inflamm Bowel Dis 10(3):245–250. https://doi.org/10.1097/00054725-200405000-00011
Temtem T et al (2021) Cytomegalovirus in pediatric inflammatory bowel disease patients with acute severe colitis. Clin Res Hepatol Gastroenterol 45(6):101625. https://doi.org/10.1016/j.clinre.2021.101625
Leal T et al (2021) Colitis due to cytomegalovirus and herpes simplex type 2 as a complication of a first presentation of inflammatory bowel disease. GE Port J Gastroenterol. https://doi.org/10.1159/000514715
Jentzer A et al (2020) Cytomegalovirus and inflammatory bowel diseases (IBD) with a special focus on the link with ulcerative colitis (UC). Microorganisms 8(7):1078. https://doi.org/10.3390/microorganisms8071078
Ibsen P 18F-FDG PET/CT Findings in Cytomegalovirus Colitis. https://doi.org/10.3390/diagnostics9010003
Ouali SE, Achkar J-P (2022) Management of Hospitalized Patients with Inflammatory Bowel Disease and CMV Infection or Clostridium Difficile Infection. Management of Inpatient Inflammatory Bowel Disease. Springer, New York, pp 161–180
Jena A et al (2022) Cytomegalovirus in ulcerative colitis: an evidence-based approach to diagnosis and treatment. Expert Rev Gastroenterol Hepatol 16(2):109–120. https://doi.org/10.1080/17474124.2022.2032662
Thavamani A et al (2023) Cytomegalovirus infection is associated with adverse outcomes among hospitalized pediatric patients with inflammatory bowel disease. Gastroenterol Res 16(1):1–8. https://doi.org/10.14740/gr1588
Yasamineh S et al (2022) Spotlight on therapeutic efficiency of mesenchymal stem cells in viral infections with a focus on COVID-19. Stem Cell Res Ther 13(1):257. https://doi.org/10.1186/s13287-022-02944-7
Yasamineh S et al (2023) Future Prospects of Natural Polymer-Based Drug Delivery Systems in Combating Lung Diseases. Natural Polymeric Materials based Drug Delivery Systems in Lung Diseases. Springer, Singapore, pp 465–482
Yasamineh S et al (2022) An overview on nanoparticle-based strategies to fight viral infections with a focus on COVID-19. J Nanobiotechnol 20(1):440. https://doi.org/10.1186/s12951-022-01625-0
Amiot A et al (2023) Risk of SARS-CoV-2 infection in healthcare workers with inflammatory bowel disease: a case-control study. Infect Prev Pract 5(1):100267. https://doi.org/10.1016/j.infpip.2022.100267
Aziz M et al (2020) The incidence and outcomes of COVID-19 in IBD patients: a rapid review and meta-analysis. Inflamm Bowel Dis 26(10):e132–e133. https://doi.org/10.1093/ibd/izaa170
Hanrahan TP, Lubel JS, Garg M (2021) Lessons From COVID-19, ACE2, and Intestinal Inflammation: could a virus trigger Chronic Intestinal Inflammation? Clin Gastroenterol Hepatol 19(1):206. https://doi.org/10.1016/j.cgh.2020.07.036
Neurath MF (2020) COVID-19 and immunomodulation in IBD. Gut 69(7):1335. https://doi.org/10.1136/gutjnl-2020-321269
Penninger JM, Grant MB, Sung JJ (2021) The role of angiotensin converting enzyme 2 in modulating gut microbiota, intestinal inflammation, and coronavirus infection. Gastroenterology 160(1):39–46. https://doi.org/10.1053/j.gastro.2020.07.067
McAllister MJ et al (2022) Intestinal protein characterisation of SARS-CoV-2 entry molecules ACE2 and TMPRSS2 in inflammatory bowel disease (IBD) and fatal COVID-19 infection. Inflammation. https://doi.org/10.1007/s10753-021-01567-z
Verstockt B et al (2020) Intestinal receptor of SARS-CoV-2 in inflamed IBD tissue is downregulated by HNF4A in ileum and upregulated by interferon regulating factors in colon. biorxiv. https://doi.org/10.1093/ecco-jcc/jjaa185
Kante B et al (2023) High seroprevalence against SARS-Cov-2 in non-vaccinated patients with inflammatory bowel disease from Northern India. Indian J Gastroenterol. https://doi.org/10.1007/s12664-022-01310-y
Liu Z et al (2023) Neutralising antibody potency against SARS-CoV-2 wild-type and omicron BA. 1 and BA. 4/5 variants in patients with inflammatory bowel disease treated with infliximab and vedolizumab after three doses of COVID-19 vaccine (CLARITY IBD): an analysis of a prospective multicentre cohort study. Lancet Gastroenterol Hepatol 8(2):145–156. https://doi.org/10.1016/s2468-1253(22)00389-2
Kennedy NA et al (2023) Vaccine escape, increased breakthrough and reinfection in infliximab-treated patients with IBD during the Omicron wave of the SARS-CoV-2 pandemic. Gut 72(2):295–305. https://doi.org/10.1136/gutjnl-2022-327570
Çolak M et al (2018) Relationship between Epstein-Barr Virus (EBV) infection and viral load in Immunosuppressive patients. Istanbul Med J 19(1):7–13. https://doi.org/10.5152/imj.2018.93357
Wallaschek N et al (2021) Ephrin receptor A2, the epithelial receptor for Epstein-Barr virus entry, is not available for efficient infection in human gastric organoids. PLoS Pathogens 17(2):e1009210. https://doi.org/10.1371/journal.ppat.1009210
Lu F et al (2021) Defective Epstein-Barr Virus Genomes and atypical viral gene expression in B-cell lines derived from multiple Myeloma patients. J Virol 95(13):e00088-e121. https://doi.org/10.1128/jvi.00088-21
Salloum N et al (2018) Epstein-Barr virus DNA modulates regulatory T-cell programming in addition to enhancing interleukin-17A production via Toll-like receptor 9. PLoS One 13(7):e0200546. https://doi.org/10.1371/journal.pone.0200546
Andari S et al (2021) Epstein-Barr virus DNA exacerbates Colitis symptoms in a Mouse model of inflammatory bowel disease. Viruses 13(7):1272. https://doi.org/10.3390/v13071272
Wu S et al (2019) A review on co-existent Epstein-Barr virus-induced complications in inflammatory bowel disease. Eur J Gastroenterol Hepatol 31(9):1085–1091. https://doi.org/10.1097/meg.0000000000001474
Kato S et al (2021) Substantial Epstein-Barr virus reactivation in a case of severe refractory ulcerative colitis: a possible role in exacerbation. Clin J Gastroenterol 14(2):584–588. https://doi.org/10.1007/s12328-020-01319-w
Juffermans N et al (2005) Epstein-Barr virus-related lymphomas in patients with inflammatory bowel disease. Ned Tijdschr Geneeskd 149(33):1859–1863
Li X et al (2019) The status of Epstein-Barr virus infection in intestinal mucosa of Chinese patients with inflammatory bowel disease. Digestion 99(2):126–132. https://doi.org/10.1159/000489996
Xu W et al (2020) Chronic active Epstein-Barr virus infection involving gastrointestinal tract mimicking inflammatory bowel disease. BMC Gastroenterol 20(1):1–7. https://doi.org/10.1186/s12876-020-01395-9
Zhou Y et al (2019) EBV-associated lymphoproliferative disorder involving the gastrointestinal tract which mimic IBD in immunocompetent patients: case reports and literature review. Int J Colorectal Dis 34(11):1989–1993. https://doi.org/10.1007/s00384-019-03400-4
Patton K et al (2018) Epstein-barr virus associated colitis: Another mimic of IBD? Pathology 50:S142. https://doi.org/10.1016/j.pathol.2017.11.056
Gordon J et al (2016) EBV status and thiopurine use in pediatric IBD. J Pediatr Gastroenterol Nutr 62(5):711–714. https://doi.org/10.1097/mpg.0000000000001077
Kocwa-Haluch R (2001) Waterborne enteroviruses as a hazard for human health. Pol J Environ Stud 10(6):485–488
Craviotto V et al (2021) Viral infections in inflammatory bowel disease: tips and tricks for correct management. World J Gastroenterol 27(27):4276. https://doi.org/10.3748/wjg.v27.i27.4276
Nyström N et al (2013) Human enterovirus species B in ileocecal Crohn’s disease. Clin Transl Gastroenterol 4(6):e38. https://doi.org/10.1038/ctg.2013.7
Lei S et al (2016) Enterobacter cloacae inhibits human norovirus infectivity in gnotobiotic pigs. Sci Rep 6(1):1–10. https://doi.org/10.1038/srep25017
Axelrad JE et al (2018) Enteric infections are common in patients with flares of inflammatory bowel disease. Am J Gastroenterol 113(10):1530. https://doi.org/10.1038/s41395-018-0211-8
Axelrad JE et al (2020) Systematic review: gastrointestinal infection and incident inflammatory bowel disease. Aliment Pharmacol Ther 51(12):1222–1232. https://doi.org/10.1111/apt.15770
Tarris G et al (2021) Enteric viruses and inflammatory bowel disease. Viruses 13(1):104. https://doi.org/10.3390/v13010104
Yang J-Y et al (2016) Enteric viruses ameliorate gut inflammation via toll-like receptor 3 and toll-like receptor 7-mediated interferon-β production. Immunity 44(4):889–900. https://doi.org/10.1016/j.immuni.2016.03.009
Rodriguez-Guillen L et al (2005) Calicivirus infection in human immunodeficiency virus seropositive children and adults. J Clin Virol 33(2):104–109. https://doi.org/10.1016/j.jcv.2004.09.031
Hamza KH et al (2021) Minor alterations in the intestinal microbiota composition upon Rotavirus infection do not affect susceptibility to DSS colitis. Sci Rep 11(1):13485. https://doi.org/10.1038/s41598-021-92796-7
LeClair CE and DP Budh (2021) Rotavirus. StatPearls [Internet]
Liles E et al (2021) Incidence of pediatric inflammatory bowel disease within the Vaccine Safety Datalink network and evaluation of association with rotavirus vaccination. Vaccine 39(27):3614–3620. https://doi.org/10.1016/j.vaccine.2021.05.032
Smith RC et al (2020) Is Rotavirus immunization safe in infants born to mothers treated with immunosuppressive drugs for inflammatory bowel disease during pregnancy? J Immunol Scie. https://doi.org/10.29245/2578-3009/2020/4.1195
Yin Y et al (2018) 6-Thioguanine inhibits rotavirus replication through suppression of Rac1 GDP/GTP cycling. Antiviral Res 156:92–101. https://doi.org/10.1016/j.antiviral.2018.06.011
Kroneman A et al (2006) Increase in norovirus activity reported in Europe. Weekly releases (1997–2007) 11(50):3093. https://doi.org/10.2807/esw.11.50.03093-en
Engevik MA et al (2020) Rotavirus infection induces glycan availability to promote ileum-specific changes in the microbiome aiding rotavirus virulence. Gut microbes 11(5):1324–1347. https://doi.org/10.1080/19490976.2020.1754714
Hamza KH et al (2021) Minor alterations in the intestinal microbiota composition upon Rotavirus infection do not affect susceptibility to DSS colitis. Sci Rep 11(1):1–11. https://doi.org/10.1038/s41598-021-92796-7
Zhao B et al (2021) Norovirus protease structure and antivirals development. Viruses 13(10):2069. https://doi.org/10.3390/v13102069
Ting H-A, von Moltke J (2019) The immune function of tuft cells at gut mucosal surfaces and beyond. J Immunol 202(5):1321–1329. https://doi.org/10.4049/jimmunol.1801069
Lei S et al (2019) Enhanced GII. 4 human norovirus infection in gnotobiotic pigs transplanted with a human gut microbiota. J Gen Virol 100(11): 1530. https://doi.org/10.1099/jgv.0.001336
Tarris G et al (2021) Specific norovirus interaction with Lewis x and Lewis a on human intestinal inflammatory mucosa during refractory inflammatory bowel disease. Msphere 6(1):e01185-e1220. https://doi.org/10.1128/msphere.01185-20
Khan RR et al (2009) Gastrointestinal norovirus infection associated with exacerbation of inflammatory bowel disease. J Pediatr Gastroenterol Nutr 48(3):328–333. https://doi.org/10.1097/mpg.0b013e31818255cc
Gholizadeh O et al (2023) Hepatitis A: viral structure, classification, life cycle, clinical symptoms, diagnosis error, and vaccination. Can J Infect Dis Med Microbiol. https://doi.org/10.1155/2023/4263309
Gholizadeh O et al (2023) The role of non-coding RNAs in the diagnosis of different stages (HCC, CHB, OBI) of hepatitis B infection. Microb Pathog. https://doi.org/10.1016/j.micpath.2023.105995
Organization WH (2019) Hepatitis B vaccines: WHO position paper, July 2017–Recommendations. Vaccine 37(2):223–225. https://doi.org/10.1016/j.vaccine.2017.07.046
Papa A et al (2013) Prevalence and natural history of hepatitis B and C infections in a large population of IBD patients treated with anti-tumor necrosis factor-α agents. J Crohns Colitis 7(2):113–119. https://doi.org/10.1016/j.crohns.2012.03.001
Beaugerie L, Gerbes AL (2010) Liver dysfunction in patients with IBD under immunosuppressive treatment: do we need to fear? Gut 59(10):1310–1311. https://doi.org/10.1136/gut.2010.217331
Losurdo G et al (2020) Chronic Viral Hepatitis in a Cohort of inflammatory bowel disease patients from southern italy: a case-control study. Pathogens 9(11):870. https://doi.org/10.3390/pathogens9110870
Russo FP et al (2022) Hepatocellular Carcinoma in Chronic Viral Hepatitis: where do we stand? Int J Mol Sci 23(1):500. https://doi.org/10.3390/ijms23010500
Pratt PK et al (2019) Improved antibody response to three additional hepatitis B vaccine doses following primary vaccination failure in patients with inflammatory bowel disease. Dig Dis Sci 64(7):2031–2038. https://doi.org/10.1007/s10620-019-05595-6
Kalogera D et al Complications related to varicella zoster virus infection in patients with inflammatory bowel disease in the pre-JAK inhibitors era: A prospective study. https://www.researchgate.net/profile/Isabel-Perez-Martinez-2/publication/322889992_P377_Complications_related_to_varicella_zoster_virus_infection_in_patients_with_inflammatory_bowel_disease_in_the_pre-JAK_inhibitors_era_A_prospective_study/links/5cabbb27299bf118c4bcf8f4/P377-Complications-related-to-varicella-zoster-virus-infection-in-patientswith-inflammatory-bowel-disease-in-the-pre-JAK-inhibitors-era-A-prospective-study.pdf
Cekic C et al (2015) Evaluation of factors associated with response to hepatitis B vaccination in patients with inflammatory bowel disease. Medicine. https://doi.org/10.1097/md.0000000000000940
Kochhar GS et al (2021) Hepatitis-B vaccine response in inflammatory bowel disease patients: a systematic review and meta-analysis. Inflamm Bowel Dis 27(10):1610–1619. https://doi.org/10.1093/ibd/izaa353
Forero-Junco LM et al (2022) Bacteriophages roam the wheat phyllosphere. Viruses 14(2):244. https://doi.org/10.3390/v14020244
Bai G-H et al (2022) The Human Virome: viral metagenomics, relations with human diseases, and therapeutic applications. Viruses 14(2):278. https://doi.org/10.3390/v14020278
Cornuault JK et al (2018) Phages infecting Faecalibacterium prausnitzii belong to novel viral genera that help to decipher intestinal viromes. Microbiome 6(1):65. https://doi.org/10.1186/s40168-018-0452-1
Babickova J, Gardlik R (2015) Pathological and therapeutic interactions between bacteriophages, microbes and the host in inflammatory bowel disease. World J Gastroenterol: WJG 21(40):11321. https://doi.org/10.3748/wjg.v21.i40.11321
Clooney AG et al (2019) Whole-virome analysis sheds light on viral dark matter in inflammatory bowel disease. Cell Host Microbe 26(6):764-778.e5. https://doi.org/10.1016/j.chom.2019.10.009
Fernandes MA et al (2019) Enteric virome and bacterial microbiota in children with ulcerative colitis and crohn disease. J Pediatr Gastroenterol Nutr 68(1):30–36. https://doi.org/10.1097/mpg.0000000000002140
Mukhopadhya I et al (2019) The gut virome: the ‘missing link’between gut bacteria and host immunity? Adv Gastroenterol 12:1756284819836620. https://doi.org/10.1177/1756284819836620
Glazko VI et al (2021) Domestication and microbiome. Holocene 31(10):1635–1645. https://doi.org/10.1177/09596836211025975
Nishiyama H et al (2020) Ecological structuring of temperate bacteriophages in the inflammatory Bowel Disease-affected gut. Microorganisms 8(11):1663. https://doi.org/10.3390/microorganisms8111663
Farahmandzad F et al (2022) Bacteriophages in gut microbiome interactions in patients with inflammatory Bowel Disease: differences by sex and the disease type. https://www.researchsquare.com/article/rs-1240997/latest.pdf
Cullen G, Baden RP, Cheifetz AS (2012) Varicella Zoster virus infection in inflammatory bowel disease. Inflamm Bowel Dis 18(12):2392–2403. https://doi.org/10.1002/ibd.22950
Martin Cardona A et al (2022) P289 Evaluation of the safety and effectiveness of direct-acting antiviral drugs in the treatment of hepatitis C in patients with inflammatory bowel disease: national multicenter study (ENEIDA registry). MIC project. J Crohn’s Colitis 16(1):321–322. https://doi.org/10.1093/ecco-jcc/jjab232.416
Mosli MH et al (2022) Human papillomavirus bowel colonization in inflammatory bowel disease: a comparative case control study. J Fam Med Prim Care 11(5):1863. https://doi.org/10.4103/jfmpc.jfmpc_1871_21
Wang CJ, Truong AK (2020) COVID-19 infection on IL-23 inhibition. Dermatol Ther. https://doi.org/10.1111/dth.13893
Miyoshi J, Matsuura M, Hisamatsu T (2022) Safety evaluation of ustekinumab for moderate-to-severe ulcerative colitis. Expert Opin Drug Saf 21(1):1–8. https://doi.org/10.1080/14740338.2021.1980536
Pauly MP et al (2018) Incidence of hepatitis B virus reactivation and hepatotoxicity in patients receiving long-term treatment with tumor necrosis factor antagonists. Clin Gastroenterol Hepatol 16(12):1964-1973.e1. https://doi.org/10.1016/j.cgh.2018.04.033
Yeshi K et al (2020) Revisiting inflammatory bowel disease: pathology, treatments, challenges and emerging therapeutics including drug leads from natural products. J Clin Med 9(5):1273. https://doi.org/10.3390/jcm9051273
Acknowledgements
All authors confirmed that this research is supported by TUMS, Tabriz, Iran, which is primarily involved in education and research.
Funding
This research was supported by TUMS in Tabriz, Iran, which is primarily involved in education and research.
Author information
Authors and Affiliations
Contributions
The initial draft was written by OG and SA. The review and design of the figure and table, as well as the completion of the article, were also done by HA MK, PA, ZJ, TD, MD and MMN. VP; corresponding author, The review, editing.
Corresponding author
Ethics declarations
Conflict of interest
The authors declared no conflicts of interest regarding the research, authorship, and publication of this article.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Dehghani, T., Gholizadeh, O., Daneshvar, M. et al. Association Between Inflammatory Bowel Disease and Viral Infections. Curr Microbiol 80, 195 (2023). https://doi.org/10.1007/s00284-023-03305-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s00284-023-03305-0