
Abstract
Purpose
Since the KRAS mutation is not responsible for all metastatic colorectal cancer (mCRC) patients with resistance to anti-epidermal growth factor receptor (EGFR) monoclonal antibody (MoAb) therapy, new predictive and prognostic factors are actively being sought.
Methods
We retrospectively evaluated the efficacy of anti-EGFR MoAb-based therapies in 91 patients with mCRC according to KRAS, BRAF, and PIK3CA mutational status as well as PTEN and MET expression.
Results
In the patient group with wild-type KRAS, the presence of BRAF mutation or PIK3CA mutations was associated with lower disease control rate (DCR), shorter progression-free survival (PFS), and shorter overall survival. Patients with MET overexpression also showed lower DCR and shorter PFS when compared with patients with normal MET expression. In a separate analysis, 44 patients harboring wild-type KRAS tumors were sorted into subgroups of 25 patients without abnormality in three molecules (BRAF, PIK3CA and MET) and 19 patients with abnormality in at least one of these three molecules. The former group showed significantly higher DCR and longer PFS following anti-EGFR therapy than the latter group.
Conclusions
Our data point to the usefulness of MET overexpression, in addition to BRAF and PIK3CA mutations, as a new predictive marker for responsiveness to anti-EGFR MoAbs in mCRC patients with wild-type KRAS. This study also suggests that application of multiple biomarkers is more effective than the use of a single marker in selecting patients who might benefit from anti-EGFR therapy.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Cetuximab and panitumumab are monoclonal antibodies (MoAbs) that inhibit the activation of the epidermal growth factor receptor (EGFR) and its downstream pathways, namely the RAS/RAF/MAPK and the PI3K/PTEN/Akt axes [1, 2]. As the response rate (RR) to anti-EGFR MoAbs remains as low as 10–20 % in patients with metastatic colorectal cancer (mCRC) [2], several studies have been performed to identify markers predicting the efficacy of these agents. Tumors carrying oncogenic KRAS mutations typically do not respond to anti-EGFR MoAbs therapy [3]. This finding led the European Medicines Agency and, subsequently, the US Food and Drug Administration to limit the use of cetuximab and panitumumab only to patients with wild-type KRAS tumors [4]. However, since only 40–60 % of patients with wild-type KRAS tumors respond to anti-EGFR MoAb therapy, new predictive and prognostic factors are actively being sought [5, 6]. In this regard, the presence of oncogenic deregulation of EGFR and other members of its downstream signaling pathways, such as BRAF, PIK3CA, and PTEN, has been shown to influence the responsiveness to cetuximab and panitumumab and could, therefore, help to identify nonresponder patients [4, 6–10]. While many studies have demonstrated the BRAF mutation, PIK3CA mutation, and PTEN overexpression as markers for resistance to anti-EGFR MoAb therapy, some failed to show such association [4, 7, 8, 10–13]. Therefore, analysis of these genetic markers in different patient populations, in particular in different ethnic groups, will help determine their clinical significance.
Furthermore, recent studies also have suggested that activation of MET, a tyrosine kinase that acts as a receptor for hepatocyte growth factor (HGF) and can activate the RAS/RAF/MAPK and PTEN/PI3K/Akt pathways, may be a novel mechanism of cetuximab resistance in CRC [13–18]. However, it remains unclear whether MET activation can serve as a predictive marker for the response to the anti-EGFR therapy in patients with wild-type KRAS.
Therefore, we investigated the status of MET expression together with PTEN expression and mutations of BRAF and PIK3CA in tumors of Japanese mCRC patients with wild-type KRAS. The main purpose of this study was to examine these genetic profiles for potential correlations with clinical response to anti-EGFR MoAb therapy.
Materials and methods
Patients
Clinical outcomes of anti-EGFR MoAb therapy were retrospectively analyzed for possible associations with the molecular features of tumors in mCRC patients. The study enrolled 91 patients who were treated at the Department of Gastroenterological Surgery and Medical Oncology, Kyorin University Hospital, between November 2008 and December 2012. All patients had presented with histologically confirmed mCRC and had been treated with salvage chemotherapy incorporating anti-EGFR MoAbs. Clinical features of the patients and pathological profiles of the tumors were obtained from patient medical records.
All patients received cetuximab- or panitumumab-based therapy for mCRC (11 as first-line, 29 as second-line, 39 as third-line, and 12 as fourth-line or greater). Cetuximab, as monotherapy or in combination with irinotecan, was administered intravenously (i.v.) at a loading dose of 400 mg/m2 over 2 h, followed by weekly doses administered at 250 mg/m2 over 1 h. Panitumumab was administered i.v. every 2 weeks at a dose of 6 mg/kg. Treatment was continued until disease progression (PD) or toxicity occurred. Clinical evaluation and tumor response was analyzed according to Response Evaluation Criteria in Solid Tumors (RECIST) [19]. This study was approved by the Research Ethics Committee, Hospital of Kyorin University School of Medicine.
Mutational analysis of KRAS, BRAF, and PIK3CA by direct sequencing
Paraffin-embedded tissues (primary or metastatic) were sectioned at 10 μm thicknesses and mounted as three separate slides per tissue. The resulting slides were treated three times with xylene and then washed with ethanol. To minimize contamination by normal DNA, areas in which at least 70 % of the cells exhibited disease-specific pathology were dissected under a binocular microscope, from which DNA was extracted using the QIAamp FFPE Tissue Kit (QIAGEN). Segments of the KRAS, BRAF, and PIK3CA genes were amplified using gene-specific primers and subjected to direct DNA sequencing as previously described [4, 13, 20]. KRAS point mutations were screened for codons 12 and 13 within exon 2, two hot spots that cumulatively include >95 % of mutations in this gene [21]. BRAF mutations were screened for V600E within exon 15, in which >95 % of point mutations occur [7, 9]. PIK3CA mutations were screened within exons 9 and 20, in which >80 % of point mutations occur [4, 10, 12].
Immunohistochemistry of PTEN and MET
PTEN and MET expression levels were evaluated by immunohistochemistry performed on 4-μm tissue sections of paraffin-embedded specimens. PTEN was assessed using the 17.A mouse MoAb (1:25 dilution; Neomarkers, Thermo Fisher Scientific Inc., Fremont, CA); MET was assessed using the SP44 rabbit MoAb (Spring Biosciences, Pleasanton, CA) [22, 23]. Negative controls were incubated with nonimmune solution instead of primary antibody. Endothelial cells and hepatocellular carcinoma cells were used as positive controls for PTEN and MET expression, respectively. The PTEN and MET staining intensities were evaluated by a pathologist (Y.O.) who was blinded to the diagnosis of individual patients.
To our knowledge, there currently are no validated scoring systems for interpretation of PTEN or MET staining intensity. Both PTEN and MET are localized primarily in the cytoplasm [11, 24, 25]; we therefore adopted a scoring system that has been used for other cytoplasmic proteins and is based on the intensity of immunoreactivity and percentage of stained cells [26, 27]. Specifically, intensity was scored according to a four-tier system: 0, no staining; 1, weak; 2, moderate; and 3, strong. An additional one, two, or three points were assigned if the percentage of positive cells was <25, 25–50 %, or >50 %, respectively [4, 11].
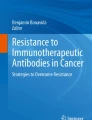
We defined normal PTEN expression as a score of 4 or greater; scores of 0–3 were classified as loss of expression (Fig. 1a, b). We defined normal/low expression of MET as a score of 0–3; scores of 4 or greater were classified as MET overexpression (Fig. 1c, d).

Representative examples of immunohistochemical staining in colorectal cancer. PTEN, normal expression (a) and loss of expression (b); MET, low expression (c) and overexpression (d)
Statistical analysis
Comparison of categorical variables was performed with the χ 2 test or the Fisher’s exact test. The progression-free survival (PFS) and overall survival (OS) were calculated using the Kaplan–Meier method. Comparisons between different groups were performed using log-rank tests. To identify independent biomarkers, multivariate analyses were performed using a logistic regression model for response and a Cox regression model for PFS and OS. Two-tailed P values of <0.05 were considered significant. All analyses were performed using SPSS software (SPSS for Windows Version 15.0; SPSS Inc., Chicago, IL).
Results
Patient characteristics
All study patients were Japanese; they were 66 men and 25 women with a mean age of 67 years (range 38–85 years). At a median follow-up of 13.3 months (range 1.3–24.4 months), 78 patients (86 %) had progressed, and 41 patients (45 %) had died. Response to anti-EGFR therapy was evaluable in all patients. We observed no patients with complete response (CR), 27 with partial response (PR), 24 with stable disease (SD), and 40 with PD. Therefore, the overall RR was 29.7 %, and the disease control rate (DCR) was 56.0 %. In the whole group, PFS and OS were 3.9 and 13.3 months, respectively.
KRAS mutational analysis
The mutational status of KRAS exon 2 was determined in all patients, with mutations detected in 24 patients (26.4 %). PR was observed in 26 patients with wild-type KRAS (38.8 %) and in one patient with mutation (4.2 %). RR and DCR were significantly lower in patients with KRAS mutations than in those with wild-type KRAS: For RR, the values were 4.2 versus 38.8 % (P < 0.001); for DCR, the values were 16.7 versus 70.2 % (P < 0.001). Median PFS was significantly shorter in patients whose tumors carried KRAS mutations than in those without such mutations (2.0 vs. 5.4 months; hazard ratio (HR) 1.67; 95 % confidence interval (CI) 1.29–2.14; P < 0.001; Supplementary Table 1, Supplementary Fig. 1A). Median OS was shorter in patients whose tumors carried KRAS mutations than in those without such mutations, although the difference was not statistically significant (9.9 vs. 13.4 months; HR 1.35; 95 % CI 0.96–1.85; P = 0.069; Supplementary Table 1, Supplementary Fig. 1B). Thus, our results indicated that KRAS mutations were reproducibly associated with less favorable outcomes for anti-EGFR MoAb therapy, consistent with the previous reports. Therefore, our further analyses focused primarily on patients with wild-type KRAS tumors. Table 1 summarizes the characteristics of the 67 patients who harbored tumors with wild-type KRAS genes.
BRAF mutational analysis
The mutational status of BRAF exon 15 was determined in all but one patient. Five (7.7 %) of 65 patients with wild-type KRAS harbored BRAF mutations, while none of 24 patients with KRAS mutation harbored mutations in BRAF (Supplementary Table 2). None of the BRAF mutant patients exhibited a response to MoAb therapy. In the patients with wild-type KRAS, the presence of the BRAF mutation was associated with a significantly reduced DCR (P = 0.002; Table 2). In this cohort, BRAF mutations were significantly associated with shorter PFS (1.2 vs. 5.5 months; HR 3.03; 95 % CI 1.78–4.86; P < 0.001; Table 3, Fig. 2a) and shorter OS (3.1 vs. 16.8 months; HR 3.74; 95 % CI 2.11–6.53; P < 0.001; Table 3, Fig. 2b). The PFS and OS of these patients were shorter than those of patients with KRAS mutations (median PFS 1.2 vs. 2.0 months; HR 1.70; 95 % CI 0.95–2.83; P = 0.037; and median OS 3.1 vs. 9.9 months; HR 0.52; 95 % CI 0.31–0.92; P = 0.009).

a Progression-free survival (PFS) and b overall survival (OS) in wild-type KRAS patients classified by BRAF mutational status. c Progression-free survival (PFS) and d overall survival (OS) in wild-type KRAS patients classified by PIK3CA mutational status. e Progression-free survival (PFS) and f overall survival (OS) in wild-type KRAS patients classified by PTEN expression status. g Progression-free survival (PFS) and h overall survival (OS) in wild-type KRAS patients classified by MET expression status
PIK3CA mutational analysis
The mutational status of PIK3CA was determined in 84 patients. Mutations were detected in three (13 %) of 23 patients with KRAS mutations and three (5.2 %) of 58 patients with wild-type KRAS (P = 0.339; Supplementary Table 2). None of the PIK3CA-mutant patients exhibited a response to MoAb therapy. When analysis was limited to patients with wild-type KRAS, DCR was significantly associated with the PIK3CA mutational status (P = 0.027; Table 2). PIK3CA mutations also were significantly associated with shorter PFS (1.8 vs. 5.4 months; HR 2.22; 95 % CI 1.07–3.86; P = 0.005) and shorter OS (5.1 vs. 15.4 months; HR 2.16; 95 % CI 0.84–4.29; P = 0.031) (Table 3, Fig. 2c, d).
PTEN immunohistochemical evaluation
Of 91 patients, 75 patients were evaluable for PTEN. Twenty-four patients (32 %) showed loss of PTEN expression in the cytoplasmic compartment of the tumor cells. No significant correlation was found between PTEN expression and KRAS mutational status (Supplementary Table 2). No significant association between PTEN expression and RR, DCR, PFS, or OS was detected in patients with wild-type KRAS, although patients with loss of PTEN tended to show lower RR and DCR than those with normal PTEN expression (Tables 2, 3, Fig. 2e, f).
MET immunohistochemical evaluation
Of 91 patients, 75 patients were evaluable for MET, with overexpression of the protein detected in 36 samples (48 %) (Supplementary Table 1). As with PTEN, there was no correlation between MET expression and KRAS mutational status (Supplementary Table 2). In 54 wild-type KRAS patients evaluable for MET, MET overexpression was associated with lower DCR (53.9 % vs. 82.1 %, P = 0.040; Table 2). Furthermore, MET overexpression was associated with shorter PFS (4.7 vs. 6.8 months; HR 1.46; 95 % CI 1.06–2.02; P = 0.018; Table 3), but exhibited no correlation with OS (12.8 vs. 15.4 months; HR 1.16; 95 % CI 0.73–1.82; P = 0.524) in this patient subgroup (Table 3, Fig. 2g, h).
Multivariate analyses
Multivariate analysis among patients with wild-type KRAS did not identify BRAF mutation, PIK3CA mutation, loss of PTEN expression, or MET overexpression as independent biomarkers for lower RR and DCR. However, the BRAF mutation and MET overexpression were identified as independent factors for shorter PFS among patients with wild-type KRAS (BRAF, P = 0.004; MET, P = 0.046) (Table 4). The BRAF mutation was also identified as an independent factor for shorter OS among patients with wild-type KRAS (OS, P = 0.001) (Table 5).
Discussion
In the present study, the MET expression, PTEN expression, and mutations of BRAF and PIK3CA in mCRC patients with wild-type KRAS were investigated in association with clinical response to anti-EGFR MoAb therapy. The most striking finding in this study was that MET overexpression was associated with lower DCR and shorter PFS in patients with wild-type KRAS. One previous study reported an association of MET overexpression with the response to anti-EGFR therapy in mCRC [13], although those researchers did not report the KRAS status of their study subjects. To the best of our knowledge, the present study is the first to clarify an association of MET overexpression with inferior clinical response to anti-EGFR MoAbs in mCRC patients with wild-type KRAS. The rate of MET overexpression in mCRC in the present study was 48 %, similar to those examined in the previous studies (17–79 %) [13, 28, 29].
MET is involved in many mechanisms of cancer proliferation and metastasis. MET contains a tyrosine kinase domain that initiates a range of signals to regulate various cellular functions [30]. MET can activate the RAS/RAF/MAPK and PTEN/PI3K/Akt pathways by itself or via EGFR transphosphorylation [15–18]. In fact, MET overexpression or genetic alteration has been shown to play a role in the pathogenesis of several tumor types. In CRC, overexpression of MET has been suggested to be associated with tumor progression [28, 31]. In addition, MET also contributes to cancer resistance against EGFR inhibitors through bypass signaling. In nonsmall cell lung cancer, amplification of MET is associated with resistance to gefitinib, the reversible EGFR tyrosine kinase inhibitor, via ErbB3 activation [17, 18, 32]. Resistance in that example is mediated by MET-ErbB3 transactivation, leading to restored signaling via the PI3K/AKT pathway [14]. Our present data revealed that MET overexpression is associated with shorter PFS, but not with altered OS, in mCRC patients with wild-type KRAS who received anti-EGFR MoAbs, suggesting that MET contributes to resistance against these therapies. If confirmed, these results attest to the feasibility of the recent development of MET-targeted agents against malignant diseases, a therapeutic approach that has already been reported in several phase I and II trials [33]. MET-targeted agents, alone or in combination with EGFR inhibitors, may offer the potential for improving patients’ outcome in mCRC.
This study also adds to the growing evidence that BRAF mutational status predicts efficacy of anti-EGFR therapy in mCRC patients with wild-type KRAS. Therefore, assessment of BRAF mutations before initiation of anti-EGFR therapy appears to be justified in this patient group. However, the clinical impact of BRAF gene testing depends on the prevalence of BRAF mutations. In this study, the frequency of BRAF mutations was 5 %, a value lower than that previously reported (7.9–16.6 %), possibly reflecting the fact that BRAF mutation is a negative prognostic marker that affects OS [34, 35]. In the present study, OS was shorter in BRAF-mutated patients compared with patients with wild-type BRAF, an observation that is consistent with the results of previous studies [4, 34, 35]. Therefore, some patients with BRAF mutations may not have survived long enough to be recruited into this study. The frequency of BRAF mutations might have been higher in a prospective study, which is expected to enroll all CRC patients. In addition, the prevalence of BRAF mutations was reported to be lower in Asian people than in Western people [34]. Taken together, these data suggest that the clinical relevance of analyzing BRAF mutation in Asian mCRC patients should be assessed by prospective studies in the future.
The frequency of PIK3CA mutations in the present study (8 %) was comparable to those in previous reports (7–18 %) [4, 10, 25]. Previous studies employing wild-type KRAS patients generally reported shorter median PFS or OS in PIK3CA-mutant patients than in patients with wild-type PIK3CA [4, 7, 10]. In concordance with these results, our patients with PIK3CA mutation showed significantly shorter PFS and OS and lower DCR than those without mutation. The present results confirmed that mutation of PIK3CA is also a predictive marker for response to anti-EGFR MoAb.
Low PTEN expression has been associated with shorter PFS in CRCs treated by anti-EGFR MoAbs in several reports [4, 11, 25], while no correlation was demonstrated in another report [8, 13]. We did not detect any association between PTEN expression status and clinical response to anti-EGFR MoAb therapy. This discrepancy may reflect differences in patient characteristics or study design, and notably, the distinct IHC scoring algorithms used in the present study. The use of a standardized methodology for assessment of PTEN expression would be crucial in the future studies.
This study has some limitations. Our study was performed retrospectively in a relatively small and heterogeneous population. The majority of our population (90 %) was treated with two or more chemotherapy regimens before anti-EGFR MoAb therapy. In addition, the anti-EGFR treatment protocols were heterogeneous. The discrepancy observed in the results between univariate and multivariate analyses might reflect these factors. Our findings therefore should be validated in subsequent prospective studies before they are applied in the clinical practice.
In conclusion, our data point out the usefulness of MET overexpression and mutations of BRAF, as a new predictive marker for response to anti-EGFR MoAbs in mCRC patients with wild-type KRAS. Using these two genes may be more useful for predicting the response to anti-EGFR MoAbs. These results support the emerging view that a comprehensive assessment of genetic alterations in EGFR signaling pathways will enable an accurate identification of patients who will benefit from anti-EGFR treatment and other molecular-targeting therapies, including MET inhibitors.
References
Ciardiello F, Tortora G (2008) EGFR antagonists in cancer treatment. N Engl J Med 358(11):1160–1174
Cunningham D, Humblet Y, Siena S, Khayat D, Bleiberg H, Santoro A et al (2004) Cetuximab monotherapy and cetuximab plus irinotecan in irinotecan-refractory metastatic colorectal cancer. N Engl J Med 351(4):337–345
Benvenuti S, Sartore-Bianchi A, Di Nicolantonio F, Zanon C, Moroni M, Veronese S et al (2007) Oncogenic activation of the RAS/RAF signaling pathway impairs the response of metastatic colorectal cancers to anti-epidermal growth factor receptor antibody therapies. Cancer Res 67(6):2643–2648
Saridaki Z, Tzardi M, Papadaki C, Sfakianaki M, Pega F, Kalikaki A et al (2011) Impact of KRAS, BRAF, PIK3CA mutations, PTEN, AREG, EREG expression and skin rash in ≥2 line cetuximab-based therapy of colorectal cancer patients. PLoS ONE 6(1):e15980
Di Fiore F, Blanchard F, Charbonnier F, Le Pessot F, Lamy A, Galais MP et al (2007) Clinical relevance of KRAS mutation detection in metastatic colorectal cancer treated by cetuximab plus chemotherapy. Br J Cancer 96(8):1166–1169
Lievre A, Bachet JB, Le Corre D, Boige V, Landi B, Emile JF et al (2006) KRAS mutation status is predictive of response to cetuximab therapy in colorectal cancer. Cancer Res 66(8):3992–3995
De Roock W, Claes B, Bernasconi D, De Schutter J, Biesmans B, Fountzilas G et al (2010) Effects of KRAS, BRAF, NRAS, and PIK3CA mutations on the efficacy of cetuximab plus chemotherapy in chemotherapy-refractory metastatic colorectal cancer: a retrospective consortium analysis. Lancet Oncol 11(8):753–762
Ulivi P, Capelli L, Valgiusti M, Zoli W, Scarpi E, Chiadini E et al (2012) Predictive role of multiple gene alterations in response to cetuximab in metastatic colorectal cancer: a single center study. J Transl Med 10:87
Bardelli A, Siena S (2010) Molecular mechanisms of resistance to cetuximab and panitumumab in colorectal cancer. J Clin Oncol 28(7):1254–1261
Sartore-Bianchi A, Martini M, Molinari F, Veronese S, Nichelatti M, Artale S et al (2009) PIK3CA mutations in colorectal cancer are associated with clinical resistance to EGFR-targeted monoclonal antibodies. Cancer Res 69(5):1851–1857
Loupakis F, Pollina L, Stasi I, Ruzzo A, Scartozzi M, Santini D et al (2009) PTEN expression and KRAS mutations on primary tumors and metastases in the prediction of benefit from cetuximab plus irinotecan for patients with metastatic colorectal cancer. J Clin Oncol 27(16):2622–2629
Souglakos J, Philips J, Wang R, Marwah S, Silver M, Tzardi M et al (2009) Prognostic and predictive value of common mutations for treatment response and survival in patients with metastatic colorectal cancer. Br J Cancer 101(3):465–472
Inno A, Di Salvatore M, Cenci T, Martini M, Orlandi A, Strippoli A et al (2011) Is there a role for IGF1R and c-MET pathways in resistance to cetuximab in metastatic colorectal cancer? Clin Colorectal Cancer 10(4):325–332
Liska D, Chen CT, Bachleitner-Hofmann T, Christensen JG, Weiser MR (2011) HGF rescues colorectal cancer cells from EGFR inhibition via MET activation. Clin Cancer Res 17(3):472–482
Guo A, Villen J, Kornhauser J, Lee KA, Stokes MP, Rikova K et al (2008) Signaling networks assembled by oncogenic EGFR and c-met. Proc Natl Acad Sci U S A 105(2):692–697
Bachleitner-Hofmann T, Sun MY, Chen CT, Liska D, Zeng Z, Viale A et al (2011) Antitumor activity of SNX-2112, a synthetic heat shock protein-90 inhibitor, in MET-amplified tumor cells with or without resistance to selective MET inhibition. Clin Cancer Res 17(1):122–133
Sattler M, Salgia R (2009) The MET axis as a therapeutic target. Update Cancer Ther 3(3):109–118
Sattler M, Reddy MM, Hasina R, Gangadhar T, Salgia R (2011) The role of the c-met pathway in lung cancer and the potential for targeted therapy. Ther Adv Med Oncol 3(4):171–184
Therasse P, Arbuck SG, Eisenhauer EA, Wanders J, Kaplan RS, Rubinstein L et al (2000) New guidelines to evaluate the response to treatment in solid tumors. European organization for research and treatment of cancer, national cancer institute of the United States, national cancer institute of Canada. J Natl Cancer Inst 92(3):205–216
Ohnishi H, Ohtsuka K, Ooide A, Matsushima S, Goya T, Watanabe T (2006) A simple and sensitive method for detecting major mutations within the tyrosine kinase domain of the epidermal growth factor receptor gene in non-small-cell lung carcinoma. Diagn Mol Pathol 15(2):101–108
Frattini M, Balestra D, Suardi S, Oggionni M, Alberici P, Radice P et al (2004) Different genetic features associated with colon and rectal carcinogenesis. Clin Cancer Res 10(12 Pt 1):4015–4021
Dua R, Zhang J, Parry G, Penuel E (2011) Detection of hepatocyte growth factor (HGF) ligand-c-MET receptor activation in formalin-fixed paraffin embedded specimens by a novel proximity assay. PLoS ONE 6(1):e15932
Torres J, Navarro S, Rogla I, Ripoll F, Lluch A, Garcia-Conde J et al (2001) Heterogeneous lack of expression of the tumour suppressor PTEN protein in human neoplastic tissues. Eur J Cancer 37(1):114–121
Murray S, Karavasilis V, Bobos M, Razis E, Papadopoulos S, Christodoulou C et al (2012) Molecular predictors of response to tyrosine kinase inhibitors in patients with non-small-cell lung cancer. J Exp Clin Cancer Res 31(1):77
Voutsina A, Tzardi M, Kalikaki A, Zafeiriou Z, Papadimitraki E, Papadakis M et al (2012) Combined analysis of KRAS and PIK3CA mutations, MET and PTEN expression in primary tumors and corresponding metastases in colorectal cancer. Mod Pathol 26(2):302–313
Lin B, Utleg AG, Gravdal K, White JT, Halvorsen OJ, Lu W et al (2008) WDR19 expression is increased in prostate cancer compared with normal cells, but low-intensity expression in cancers is associated with shorter time to biochemical failures and local recurrence. Clin Cancer Res 14(5):1397–1406
Halvorsen OJ, Rostad K, Oyan AM, Puntervoll H, Bo TH, Stordrange L et al (2007) Increased expression of SIM2-s protein is a novel marker of aggressive prostate cancer. Clin Cancer Res 13(3):892–897
Takeuchi H, Bilchik A, Saha S, Turner R, Wiese D, Tanaka M et al (2003) C-MET expression level in primary colon cancer: a predictor of tumor invasion and lymph node metastases. Clin Cancer Res 9(4):1480–1488
De Oliveira AT, Matos D, Logullo AF, Da Silva SR, Neto RA, Filho AL et al (2009) MET is highly expressed in advanced stages of colorectal cancer and indicates worse prognosis and mortality. Anticancer Res 29(11):4807–4811
Bottaro DP, Rubin JS, Faletto DL, Chan AM, Kmiecik TE, Vande Woude GF et al (1991) Identification of the hepatocyte growth factor receptor as the c-met proto-oncogene product. Science 251(4995):802–804
Trusolino L, Comoglio PM (2002) Scatter-factor and semaphorin receptors: cell signalling for invasive growth. Nat Rev Cancer 2(4):289–300
Engelman JA, Zejnullahu K, Gale CM, Lifshits E, Gonzales AJ, Shimamura T et al (2007) PF00299804, an irreversible pan-ERBB inhibitor, is effective in lung cancer models with EGFR and ERBB2 mutations that are resistant to gefitinib. Cancer Res 67(24):11924–11932
Adjei AA, Schwartz B, Garmey E (2011) Early clinical development of ARQ 197, a selective, non-ATP-competitive inhibitor targeting MET tyrosine kinase for the treatment of advanced cancers. Oncologist 16(6):788–799
Liou JM, Wu MS, Shun CT, Chiu HM, Chen MJ, Chen CC et al (2011) Mutations in BRAF correlate with poor survival of colorectal cancers in Chinese population. Int J Colorectal Dis 26(11):1387–1395
Richman SD, Seymour MT, Chambers P, Elliott F, Daly CL, Meade AM et al (2009) KRAS and BRAF mutations in advanced colorectal cancer are associated with poor prognosis but do not preclude benefit from oxaliplatin or irinotecan: results from the MRC FOCUS trial. J Clin Oncol 27(35):5931–5937
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution License which permits any use, distribution, and reproduction in any medium, provided the original author(s) and the source are credited.
About this article
Cite this article
Kishiki, T., Ohnishi, H., Masaki, T. et al. Overexpression of MET is a new predictive marker for anti-EGFR therapy in metastatic colorectal cancer with wild-type KRAS . Cancer Chemother Pharmacol 73, 749–757 (2014). https://doi.org/10.1007/s00280-014-2401-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00280-014-2401-4