
Abstract
Purpose
In fracture and realignment surgery, the contralateral unaffected side is often used as a model or template for the injured bone even though clinically valuable quantitative data of bilateral symmetry are often unavailable. Therefore, the objective of the present study was to quantify and present the bilateral symmetry of the tibia and fibula.
Methods
Twenty bilateral lower-leg CT scans were acquired in healthy volunteers. The left and right tibia and fibula were segmented resulting in three-dimensional polygons for geometrical analyses (volume, surface and length). The distal and proximal segment of the right tibia of each individual was subsequently matched to the left tibia to quantify alignment differences (translation and rotation). Bone symmetry on group level was assessed using the Student’s t test and intra-individual differences were assessed using mixed-models analyses.
Results
Intra-individuals differences were found for tibia volume (5.2 ± 3.3 cm3), tibia surface (5.2 ± 3.3 cm2), translations in the lateral (X-axis; 9.3 ± 8.9 mm) and anterior direction (Y-axis; 7.1 ± 7.0 mm), for tibia length (translation along Z-axis: 3.1 ± 2.4 mm), varus/valgus (φz: 1.7o ± 1.4°), and endotorsion/exotorsion (φz: 4.0o ± 2.7°).
Conclusion
This study shows intra-individual tibia asymmetry in both geometric and alignment parameters of which the surgeon needs to be aware in pre-operative planning. The high correlation between tibia and fibula length allows the ipsilateral fibula to aid in estimating the original tibia length post-injury. Future studies need to establish whether the found asymmetry is clinically relevant when the contralateral side is used as reference in corrective surgery.
Level of evidence
III cohort study.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
In fracture treatment and the correction of symptomatic malunions or other acquired deformities (for example as late complications of trauma), an anatomical reconstruction is considered of paramount importance for good clinical outcome [1, 2]. Additionally in knee arthroplasty, ankle arthrodesis and arthroplasty adequate alignment may be essential to restore function. Physicians often use the unaffected contralateral side of the patient as a rough reference standard in pre-operative planning although precise knowledge may further improve functional outcome [3,4,5,6,7,8,9,10,11]. From an anatomical and embryological perspective, assuming symmetry in development of the upper and lower extremities, using the contralateral unaffected side as a template may be an accurate option, though its validity is an assumption rather than a given fact [12,13,14]. A hypothesis explaining observed bilateral asymmetry originates from asymmetrical development that finds its genesis from the prenatal stage up to maturity [12, 15,16,17]. This asymmetry may also be explained by differences in mechanical stress during development, which in turn may cause kinematic asymmetry [18].
Detailed knowledge on anatomy and thus bone geometry is essential to restore function. For the ankle joint, not only the tibia is of paramount importance for optimal function, but also the fibula is essential to ensure joint congruency and prevent (sub) luxation of the talus [19]. In addition to providing stability to the ankle joint during a great range of mobility tasks, the fibula may help in correction surgery when it concerns correction of tibia bone length (comparable to the radius and ulna) [20].
Bilateral bone asymmetry is a current topic of interest for those who perform surgical corrections. Studies on bone asymmetry of the lower extremity have predominantly focused on the femur and tibia [12, 13, 15, 21,22,23,24,25]. Previously conducted studies have some limitations that make the results less generally applicable, such as comparison of injured with uninjured individuals, usage of cadaveric specimens with an unknown medical (lower-extremity) history, and a low number of subjects being studied (i.e., < 10). Moreover, none of the previous studies included a full three-dimensional in vivo analysis of geometrical and alignment differences of the tibia within healthy individuals (right–left differences) nor translated significant findings to implications for surgical practice.
The objective of the present study is therefore to quantify the bilateral asymmetry of the tibia in healthy volunteers using a computed tomography (CT-) scan and advanced 3D image analysis techniques.
Materials and methods
High-resolution lower-leg CT scans were acquired in twenty healthy volunteers. Subsequently, 3D polygons were created and used to quantify intra-individual tibia differences in terms of geometry (volume, surface area and length) and anatomical alignment (translation and rotation) of the distal tibial segment with respect to the proximal segment of the tibia. Fibula polygons were also created to investigate its length in relation to tibia length.
Study population
To ensure a balanced sample from the general population and to investigate the effect of gender specific characteristics, 10 males and 10 females were included [26, 27].
Prior to inclusion, volunteers were screened for health (i.e., no systemic diseases and no previous trauma to the lower leg requiring medical attention). The volunteers had to be at least 18 years old to provide consent for participation. To minimize the radiation load, volunteers were excluded if they had undergone a CT scan in the previous year, or were planned to undergo a CT scan in the upcoming year. Volunteers with musculoskeletal complaints of the lower extremity at the time of scanning were excluded. Additionally, females were excluded if they were pregnant or wanted to become pregnant.
Informed consent was obtained from all individual volunteers before inclusion in the study. Of each included volunteer sex, age, weight, body height and leg dominance were recorded.
Ethical approval
All the procedures performed in this study involving human participants were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki declaration and its later amendments (reference: 2017_039#B2017175a, approval date 24-03-2017).
Image acquisition
Of each volunteer, a bilateral CT scan was carried out of the knees, lower leg and feet using a Brilliance 64 CT scanner (Philips, Amsterdam, The Netherlands) (voxel size 0.46 × 0.46 × 0.45 mm, 120 kV, and 160 mAs) [28].
Creating virtual bone models
All CT scans were analyzed for symmetry in the same way as described by Vroemen et al. with proven excellent reliability (ICC 0.81–0.94) [20, 29]. In short, both tibiae and fibulae were segmented by threshold-connected region growing followed by a binary closing algorithm for filling of residual holes and closing of the outline [4]. A Laplacian level-set segmentation growth algorithm was subsequently used to grow toward the boundary of the bone. The Marching cubes algorithm was then used to extract a polygon mesh at the zero level of the level-set image. The polygon meshes represented the virtual 3D surface models of the bones.
Bone symmetry parameters
Primary outcome measures included geometric and alignment parameters for defining bone symmetry expressed by parameters representing (absolute) intra-individual differences. To evaluate if tibiae were symmetrical, geometric parameters of left and right tibiae were statistically compared on both group level and within individuals. The relative difference in geometric parameters was calculated based on the percentage difference between the mean intra-individual difference and mean geometric parameter. The relative difference in translation parameters was calculated based on the mean intra-individual difference in relation to the axis length (in percentages). As secondary outcome measures, we evaluated if symmetry parameters were related to gender or leg dominance.
Geometric parameters
Based on the polygon meshes of the tibiae, the following geometric parameters were automatically calculated: volume (cm3), surface area (cm2) and length (cm). The bone surface represented the cortical bone surface. A difference in bone length was represented by translation along the Z-axis of the distal bone segment with respect to the proximal bone segment.
Alignment parameters
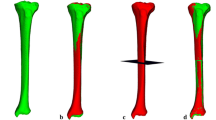
Alignment of the left and right tibiae was quantified by first aligning the left and right tibiae proximally, by registration. The relative position of a distal segment with respect to the proximal tibia was then used to find translational and rotational alignment parameters. This procedure effectively required registration of a proximal and distal bone segment. To this end, a proximal segment of 15% of the total tibia bone length and a distal segment of 10% of the total tibia bone length were selected from the 3D polygon. These segment lengths were pragmatically chosen and included the majority of the bone epiphysis, which helps matching polygons efficiently (Fig. 1). The distal and proximal segments were registered to the mirrored image of the other side using a point-to-image registration algorithm and provided the three translations (Δx, Δy, Δz), and three rotations (Δφx, Δφy, Δφz) of the distal segment, which are expressed in terms of an anatomical coordinate system [4, 30].

Proximal and distal segments (green) that were used to match the proximal and distal tibial segments to the contralateral side. Alignment parameters are represented by translations (Δx, Δy, Δz) along, and rotations (φx, φy, φz) about the axes of the anatomical coordinate system, as visualized in the enlarged image. NB. The X-axis is in a medial–lateral direction, the Y-axis is in an anterior–posterior direction, the Z-axis is in a cranial-caudal direction (i.e., shorter/longer). φx represents a flexion/extension angulation, φy represents a varus/valgus angulation, and φz represents endotorsion/exotorsion
The anatomical coordinate system was determined automatically based on the polygon mesh, as described by de Roo et al. In short: the inertia tensor is calculated based on the points of the polygon mesh of the proximally aligned right tibia [31]. Eigenvector analysis yields three eigenvectors. The vector with the smallest eigenvalue points in the direction of the bone axis and serves as Z-axis. The X-axis is perpendicular to the Z-axis and points to the lowest point of the polygon mesh as measured along the Z-axis, this is approximately in the direction of the medial malleolus. The Y-axis points perpendicular to the X- and Z-axes in agreement with the definition of a right-handed coordinate system.
Tibiofibular length ratio
The fibula has an important role specifically in the stability during mobility tasks of the ankle. Additionally, the fibula may be used as a reference standard for the initial pre-injury tibia length in case of a strong correlation between the tibia and fibula, which is expected based on previous research on the radius and ulna [20]. Therefore, the bilateral length difference was calculated, providing the tibiofibular length ratio (ΔZfibula/ΔZtibia).
Statistical analysis
After checking for normality, the mean and standard deviation (SD) were calculated. To provide additional information on the symmetry parameters also, the ranges were determined. The degree of intra-individual bone symmetry was assessed using the paired Student’s t test comparing geometric and alignment parameters in case of a normal distribution and the Wilcoxon signed-rank test in the case of skewed data. A one-sample t test was used to assess whether intra-individual differences significantly differed from ‘0’. For correlated measurements (i.e., left–right legs within individuals), mixed-models analyses were used to assess differences between men and women and Pearson’s cq. Spearman’s correlation coefficients were used to assess whether there was a difference in bone geometry comparing the left and right lower leg.
A p value of < 0.05 was considered statistically significant. For the statistical analyses, SPSS Statistics was used (IBM Corp. Released 2016. IBM SPSS Statistics for Windows, Version 26.0. Armonk, NY: IBM Corp).
Results
Population demographics
Twenty healthy volunteers were included. The mean age of the individuals in this study for men was 37.7 years (± 11.1), and for women 34.0 years (± 10.3). The mean weight was 82.7 (± 5.6) kilograms (kg) for men and 71.0 kg (± 11.6) for women. The mean height was 185 cm (± 5) for men and 173 cm (± 8) for women. Sixteen volunteers reported right leg dominance and one left leg dominance, of three leg dominance was unknown.
Geometric parameters
Tibia volume showed largest percentage intra-individual right–left difference (1.47%), followed by bone surface (1.12%) and bone length (0.78%) subsequently (Table 1). See Fig. 2 for the intra-individual differences in geometric parameters.

Intra-individual right-to-left difference of geometric parameters. The lines connect the left (circles) and right (squares) tibia parameter of one individual representing the intra-individual difference
At group level, males (391 cm3 ± 39) had a significantly greater bone volume compared to women (301 cm3 ± 55). Gender did not influence any of the other geometric parameters.
Volume
The mean tibia bone volume, not taking gender or side into account, was 345.8 cm3 (SD ± 65.8). In seven cases, the right tibia had a greater bone volume compared to the left tibia. The absolute intra-individual volume difference ranged from 0.2 to 12.2 cm3 in men and 0.4–6.8 cm3 in women (Table 1).
Surface
The mean tibial surface area was 468.3 cm2 (SD ± 62.9). The intra-individual right–left tibia surface difference ranged from 0.6 to 16.1 cm2 in men and 0.7 to 9.6 cm2 in women (Table 1). In eight cases, the right tibial bone surface was larger compared to the left side.
Length
The mean tibial length was 40.2 cm (SD ± 2.7). The absolute intra-individual tibia length difference ranged from 0.1 to 0.8 cm in men and 0.1–0.7 cm in women (Table 1). In 13 cases, the right tibial bone length was larger compared to the left side.
Alignment parameters
Translation
After subsequent mirroring and matching of tibiae, intra-individual absolute translations ranged from 1.4 to 26.2 mm in men and 0.5–34.3 mm in women for the X-axis, 0.5–18.2 mm in men and 0.5–30.1 mm in women for the Y-axis, and 1.5–8.5 mm in men and 0.0–15.7 mm in women for the Z-axis (Table 2). Groupwise, translation expressed along the X-, Y- and Z-axes (Fig. 3), respectively, indicated no significant shifts along any of the axes.

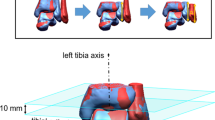
Distal matched segments of two individuals with A the most asymmetrical right (white) and left (green) tibiae and B the most symmetrical tibiae on a dorsolateral view based on intra-individual translational and rotational differences
Rotation
The intra-individual absolute rotations expressed around the X- Y- and Z-axes, described by Δφx/Δφy/Δφz respectively, ranged from 0.4 to 3.6° in men and 0.1–4.1° in women for Δφx, 0.0–5.3° in men and 0.4–4.2° in women for Δφy, and 0.6–12.6° in men and 0.3–8.4° in women for Δφz (Table 2). With zero as reference standard for rotational symmetry for both varus/valgus and endotorsion/exotorsion significant left-to-right differences were found.
Tibiofibular length ratio
The mean tibial length was 40.0 cm (SD ± 2.6). The mean fibular length was 39.3 cm (SD ± 2.9). Comparing the length of the tibia in relation to the length of the fibula showed no significant differences within individuals. The Pearson’s correlation coefficient showed a strong relation between the absolute length of the tibia and the length of the fibula (r 0.95, p < 0.005) and between the mean intra-individual difference of tibia length and fibula length (ΔZtibia/ΔZfibula; r 0.75, p < 0.005) (Fig. 4).

Scatterplot showing the relation between tibial length (ΔZtibia) and fibular length (ΔZfibula)
Confounders in bone symmetry
When defining bilateral symmetry, our data indicated for both quantification of the geometric and alignment symmetry multiple outliers. For geometric bone symmetry parameters, outliers were mainly seen for bone volume (see Figs. 5, 6). There was no evident statistic relation between symmetry parameters and age, nor was either parameter more pronounced for the left or right side. For leg dominance, statistical assessment was not possible as only one volunteer reported left-leg dominance.

Boxplot for geometric parameters

Boxplot for alignment parameters
Discussion
In this study, we quantified the tibial symmetry in 20 healthy individuals using geometric and alignment parameters. Groupwise, significant absolute intra-individual geometric differences were found, although these differences were smaller than two percent of the tibia volume, surface area and length. For tibia alignment, both translation and rotation differences were found. Gender did not affect the degree of symmetry. The strong correlation with fibula length may be used in the pre-operative planning to correct for tibia length differences [32]. The intra-individual differences are generally small, compared to some post-traumatic deformities. There were, however, outliers in whom the intra-individual asymmetry was greater. In these cases, the varus/valus and endotorsion/exotorsion position of the tibia was greater affecting the dynamics in the tibiotalar joint. As these patients have developed their motion pattern based on their bone geometry, post-traumatic correction may work disadvantageous as it will require patients to adapt to this correction leading to new loading patterns in the full chain (including also the knee and hip). It is yet unknown if the bilateral differences are of any clinical importance when the contralateral side is used as template for corrective surgery. Future clinical research is needed to answer this important question.
The clinical relevance of the present study is underlined by the provided novel insights into the presence or absence of bilateral symmetry in healthy volunteers. We found that there is an intra-individual tibia asymmetry in both geometric and alignment parameters. This information is important to take into account in fracture and realignment surgery as well as arthroplasty surgery. The current findings may function as a clinical and research stepping stone to identify the thresholds above which asymmetry parameters are of clinical relevance.
Previous 3D studies performed on tibial bone asymmetry by Eckhoff et al. and Schenk et al. indicated that bones did not significantly differ regarding translational parameters, but significant asymmetry existed for rotational parameters of the aforementioned bones [1, 12]. Our data, however, indicated intra-individual differences for both translation and rotation parameters. To ensure consistency and reliability of results, we assigned the coordinate system automatically instead of manually [12]. For Schenk et al., it was unclear whether the coordinate system was assigned manually or automatically [1, 27]. Additionally, we included geometric parameters to further define bone asymmetry and only included healthy volunteers, ensuring a reliable baseline in contrast to studies using cadavers with an unknown medical history [1, 7, 11, 12, 14]. Compared to Vroemen et al., who also compared asymmetry parameters in terms of translation and rotation of the distal radius and ulna, comparable right–left differences were found, although the range of left–right differences was larger, potentially caused by the larger tibia dimensions [20].
Although the findings of the aforementioned studies in addition to the present study suggest that the contralateral side may be utilized as a template concerning alignment features when performing (re) alignment surgery, there is an evident degree of asymmetry within individuals. To what degree this bilateral asymmetry may affect clinical outcome is unknown. It is necessary for future clinical studies to investigate the relation between residual malalignment and patient satisfaction in which the contralateral side is used as reference bone. In addition, as not only the tibia is paramount in leg function, also the effect of joint alignment requires more attention. Future studies will need to assess the tibiotalar and subtalar joint in light of alignment and bilateral symmetry to ensure optimal function after an ankle arthrodesis or arthroplasty.
The major strength of the current study, compared to previous research is that the current study included a full three-dimensional in vivo analysis of geometrical and alignment differences of the tibia within healthy individuals (left–right differences) instead of using a 2D projection.
Although our semi-computerized matching procedure may be the optimal procedure for assessing bone symmetry and minimized bias through manual measurements, we still had to cope with limitations. Due to the small sample size, small differences in certain bony landmarks, such as bowing of the bone leading to manual misplacement of the bone before the automatic matching procedure, may have created a variation in matching results and therefore simulated bone asymmetry. Also, our results are limited to only the tibia and fibula. The talus and calcaneus were not taken into consideration, limiting our conclusion to bone osteotomy and not being able to take lower-leg function and joint alignment into consideration.
In conclusion, this study quantifies small but significant intra-individual tibia asymmetry in both geometric and alignment parameters. The surgeon needs to be aware of these differences, especially the existence of outliers, when using the contralateral side as reference for realignment planning. However, the ranges in intra-individual asymmetry are on average below two percent and may therefore not be clinically relevant. Intra-individual symmetry was greatest for tibia surface and length, and in the sagittal plane (flexion/extension). The high correlation between tibia and fibula length allows the ipsilateral fibula to aid in estimating the true tibia length in pre-operative planning. The greatest asymmetry was seen for translation, and rotation in the coronal (varus/valgus) and axial (endotorsion/exotorsion) plane.
References
Schenk P, Vlachopoulos L, Hingsammer A, Fucentese SF, Furnstahl P (2018) Is the contralateral tibia a reliable template for reconstruction: a three-dimensional anatomy cadaveric study. Knee Surg Sports Traumatol Arthrosc 26:2324–2331
Tischer T, Paul J, Pape D, Hirschmann MT, Imhoff AB, Hinterwimmer S, Feucht MJ (2017) The impact of osseous malalignment and realignment procedures in knee ligament surgery: a systematic review of the clinical evidence. Orthop J Sports Med 5:2325967117697287
Dobbe JG, Kievit AJ, Schafroth MU, Blankevoort L, Streekstra GJ (2014) Evaluation of a CT-based technique to measure the transfer accuracy of a virtually planned osteotomy. Med Eng Phys 36:1081–1087
Dobbe JG, Strackee SD, Schreurs AW, Jonges R, Carelsen B, Vroemen JC, Grimbergen CA, Streekstra GJ (2011) Computer-assisted planning and navigation for corrective distal radius osteotomy, based on pre- and intraoperative imaging. IEEE Trans Biomed Eng 58:182–190
Krishan K, Kanchan T, DiMaggio JA (2010) A study of limb asymmetry and its effect on estimation of stature in forensic case work. Forensic Sci Int 200:181.e181-185
Livingston LA, Mandigo JL (2003) Bilateral rearfoot asymmetry and anterior knee pain syndrome. J Orthop Sports Phys Ther 33:48–55
Pierre MA, Zurakowski D, Nazarian A, Hauser-Kara DA, Snyder BD (2010) Assessment of the bilateral asymmetry of human femurs based on physical, densitometric, and structural rigidity characteristics. J Biomech 43:2228–2236
Santoro D, Tantavisut S, Aloj D, Karam MD (2014) Diaphyseal osteotomy after post-traumatic malalignment. Curr Rev Musculoskelet Med 7:312–322
Ten Berg PW, Dobbe JG, van Wolfswinkel G, Strackee SD, Streekstra GJ (2016) Validation of the contralateral side as reference for selecting radial head implant sizes. Surg Radiol Anat 38:801–807
Thomas TP, Anderson DD, Willis AR, Liu P, Marsh JL, Brown TD (2011) ASB clinical biomechanics award paper 2010 virtual pre-operative reconstruction planning for comminuted articular fractures. Clin Biomech (Bristol, Avon) 26:109–115
Young EY, Gebhart J, Cooperman D, Ahn NU (2013) Are the left and right proximal femurs symmetric? Clin Orthop Relat Res 471:1593–1601
Eckhoff DG, Jacofsky DJ, Springer BD, Dunbar M, Cherian JJ, Elmallah RK, Mont MA, Greene KA (2016) Bilateral symmetrical comparison of femoral and tibial anatomic features. J Arthroplasty 31:1083–1090
Hildebrandt EM, Manske SL, Hanley DA, Boyd SK (2016) Bilateral asymmetry of radius and tibia bone macroarchitecture and microarchitecture: a high-resolution peripheral quantitative computed tomography study. J Clin Densitom 19:250–254
Radzi S, Uesugi M, Baird A, Mishra S, Schuetz M, Schmutz B (2014) Assessing the bilateral geometrical differences of the tibia–are they the same? Med Eng Phys 36:1618–1625
Eckhoff DG, Johnson KK (1994) Three-dimensional computed tomography reconstruction of tibial torsion. Clin Orthop Relat Res 302:42–46
Malina RM, Buschang PH (1984) Anthropometric asymmetry in normal and mentally retarded males. Ann Hum Biol 11:515–531
Yoshioka Y, Siu DW, Scudamore RA, Cooke TD (1989) Tibial anatomy and functional axes. J Orthop Res 7:132–137
Kanchan T, Mohan Kumar TS, Pradeep Kumar G, Yoganarasimha K (2008) Skeletal asymmetry. J Forensic Leg Med 15:177–179
Sheehan FT, Seisler AR, Siegel KL (2007) In vivo talocrural and subtalar kinematics: a non-invasive 3D dynamic MRI study. Foot Ankle Int 28:323–335
Vroemen JC, Dobbe JG, Jonges R, Strackee SD, Streekstra GJ (2012) Three-dimensional assessment of bilateral symmetry of the radius and ulna for planning corrective surgeries. J Hand Surg Am 37:982–988
Elgeti H, Grote R, Giebel G (1980) Measurement of tibial torsion by axial computerized tomography (author’s transl). Unfallheilkunde 83:14–19
Jakob RP, Haertel M, Stussi E (1980) Tibial torsion calculated by computerised tomography and compared to other methods of measurement. J Bone Joint Surg Br 62-b:238–242
Reikeras O, Bjerkreim I, Kolbenstvedt A (1983) Anteversion of the acetabulum and femoral neck in normals and in patients with osteoarthritis of the hip. Acta Orthop Scand 54:18–23
Turner MS, Smillie IS (1981) The effect of tibial torsion of the pathology of the knee. J Bone Joint Surg Br 63-b:396–398
Yoshioka Y, Cooke TD (1987) Femoral anteversion: assessment based on function axes. J Orthop Res 5:86–91
de Baldon RM, Lobato DF, Furlan L, Serrao FV (2013) Gender differences in lower limb kinematics during stair descent. J Appl Biomech 29:413–420
Tamari K, Tinley P, Aoyagi K (2003) Gender and age-related differences in axial alignment of the lower limb among healthy Japanese volunteers: comparative and correlation study. J Jpn Phys Ther Assoc 6:25–34
Dobbe JG, Pre KJ, Kloen P, Blankevoort L, Streekstra GJ (2011) Computer-assisted and patient-specific 3-D planning and evaluation of a single-cut rotational osteotomy for complex long-bone deformities. Med Biol Eng Comput 49:1363–1370
Vuurberg G, Dahmen J, Dobbe JGG, Kleipool RP, Stufkens SAS, Maas M, Kerkhoffs G, van Dijk CN, Streekstra GJ (2019) The effect of foot rotation on measuring ankle alignment using simulated radiographs: a safe zone for pre-operative planning. Clin Radiol 74:e891-897
Dobbe JGG, de Roo MGA, Visschers JC, Strackee SD, Streekstra GJ (2019) Evaluation of a quantitative method for carpal motion analysis using clinical 3-D and 4-D CT protocols. IEEE Trans Med Imaging 38:1048–1057
de Roo MGA, Dobbe JGG, Peymani A, van der Made AD, Strackee SD, Streekstra GJ (2020) Accuracy of manual and automatic placement of an anatomical coordinate system for the full or partial radius in 3D space. Sci Rep 10:8114
Dobbe JG, Vroemen JC, Strackee SD, Streekstra GJ (2013) Corrective distal radius osteotomy: including bilateral differences in 3-D planning. Med Biol Eng Comput 51:791–797
Funding
This study received financial support from the Marti-Keuning Eckhardt Stichting and the Musculoskeletal Imaging Quantification Center (MIQC) to finance the required imaging. Their support had by no means any effect on the content of this manuscript.
Author information
Authors and Affiliations
Contributions
GV: Protocol and project development, data collection and management, data analysis, manuscript writing and editing. JD: Data collection and management, manuscript writing and editing. JGGD: Protocol development, data management, data analysis, manuscript writing and editing. RPK: Protocol development, data collection, manuscript writing and editing. BH: Protocol and project development, manuscript writing. INS: Protocol development, data analysis, manuscript writing and editing. GJS: Data collection and management, data analysis, manuscript writing and editing. GMMJK: Protocol and project development, manuscript writing and editing. SASS: Protocol and project development, data management, data analysis, manuscript writing and editing.
Corresponding author
Ethics declarations
Conflict of interest
The authors of this paper have no conflict of interest to declare.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Vuurberg, G., Dahmen, J., Dobbe, I.G.G. et al. Lower leg symmetry: a Q3D-CT analysis. Surg Radiol Anat 44, 851–860 (2022). https://doi.org/10.1007/s00276-022-02940-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00276-022-02940-9