
Avoid common mistakes on your manuscript.
Introduction
Different image-guided percutaneous techniques can be used for treatment or pain palliation in patients with primary or secondary bone tumours. Curative ablation can be applied for the treatment of specific benign or in selected cases of malignant localized bone tumours [1]. Pain palliation therapy of primary and secondary bone tumours [2, 3] can be achieved with safe, fast, effective, and tolerable percutaneous methods [4]. Ablation (chemical, thermal, mechanical), cavitation (radiofrequency ionization), and consolidation (cementoplasty) techniques can be used separately or in combination. Each technique has its indications as well as its own advantages and drawbacks.
Definitions
-
Curative treatment The therapeutic goal of curative treatment is to completely and definitively ablate the tumour.
-
Palliative treatment The therapeutic goal of palliative treatment is not to completely ablate the tumour but to achieve pain palliation.
Consolidation Techniques
-
Cementoplasty Percutaneous injection of methylmethacrylate provides bone strengthening and pain relief [5, 6]. Cementoplasty is a symptomatic and not a curative treatment [7, 8].
Ablation Techniques
-
Chemical ablation Injection of ethanol is used to ablate osteolytic bone tumours as well as achieve pain management (neurolysis) [9].
-
Thermal ablation procedures consist of the following:
-
1.
Laser photocoagulation Thermoablation is produced with near-infrared wavelength lasers (neodymium yttrium aluminum garnet [Nd:YAG] diode laser 800–1000 nm).
-
2.
Radiofrequency ablation Thermoablation is produced by altering the electric current at the tip of the electrode, thus causing local ionic agitation and subsequent frictional heat.
-
3.
Cryoablation The application of extreme cold aims to destroy cells by causing both direct cellular and vascular injury [10, 11].
-
1.
-
Radiofrequency ionisation (decompression ablation technique) consists of the following:
-
1.
Low-temperature bipolar technique: This produces a plasma field at the tip of the electrode that breaks the intermolecular bonds, thus creating a cavity inside the tissue, which leads in turn to decompression.
-
1.
Treatment Strategy
The management of patients with bone tumours requires consideration of the following:
-
histology of the tumour with differentiation of benign and malignant tumours;
-
careful evaluation of the patient’s general condition;
-
understanding of the disease process;
-
appreciation of the degree of bone destruction (consolidation);
-
thorough working knowledge of available treatment options and multidisciplinary decision making; and
-
precision of the treatment goal, i.e., curative or palliative.
Tumour Biopsy
Percutaneous image-guided biopsy of the tumour should be obtained when needed. Specific benign bone tumours have characteristic imaging findings (e.g., osteoid osteoma) and thus usually do not require a pretreatment biopsy specimen. For the rest, i.e., benign and primary malignant neoplasms, histologic confirmation is necessary. For chondroblastoma, a biopsy should always be performed to differentiate it from clear cell chondrosarcoma.
Secondary metastatic tumours usually do not require a biopsy specimen. Biopsy should be performed only in cases of unknown primary tumour or multiple primary neoplasms or when there is doubt if the lesion is a secondary localization of the known primary neoplasm.
Curative Percutaneous Bone Tumour Management
Indications
-
Benign lesions
-
1.
Osteoid osteoma;
-
2.
osteoblastoma (when the maximum diameter is <3cm); and
-
3.
chondroblastoma.
-
1.
-
Malignant lesions (primary or secondary in nonsurgical patients) are made by multidisciplinary decision. Treatement is reserved for slow-growing cancers with the following typical features:
-
1.
with <3 proven locations, and
-
2.
measuring <3 cm in diameter.
-
1.
Palliative Percutaneous Bone Tumour Management
Indications
In the palliative treatment of painful bone tumours (primary or secondary), the therapeutic goal is not complete ablation of the tumour but rather:
-
pain palliation;
-
tumour reduction;
-
prevention of impending pathologic fractures; and/or
-
decompression and debulking of bone tumours (especially for tumours bulging into the spinal canal).
Procedure Set-Up and Sedation
General Considerations
Coagulation studies (prothrombin time, activated partial prothrombin time, international normalized ratio) as well as platelet and white blood counts should be normal. All infections located remotely from the surgical site should be identified and resolved before the intervention is performed. Informed written consent should be obtained before the procedure.
Procedure Set-Up
Dealing with bone tumours requires strict sterile conditions. Antibiotics can be administered intravenously on the day of the procedure to prevent infection.
Sedation
Bone tumour management is usually painful and requires sedation and analgesia. Tumour ablation usually needs deeper sedation, such a general anaesthesia, nerve root blocks, or spinal anaesthesia. For single-level cementoplasty, general anaesthesia is not mandatory; conscious sedation is usually sufficient.
Types of Image Guidance
-
Fluoroscopy is the most commonly used imaging modality for skeletal interventions, especially when real-time imaging is needed (e.g., cement injection during cementoplasty).
-
Ultrasound can be used in superficial lytic tumours, i.e., those with a soft-tissue component.
-
Computed axial tomography (CAT) guidance provides high-resolution images that are useful for tumour ablation (three-dimensional [3-D] imaging is necessary) and help decrease the complication rate.
-
Magnetic resonance imaging (MRI) guidance is promising for its thermal-monitoring capacity. It also offers the possibility of 3-D imaging, which is necessary for tumour ablation.
-
Flat-panel cone-beam CAT is becoming more accurate, faster, and therefore very promising.
-
Multimodality imaging, which is associated with fluoroscopy and CAT scan, allows faster, safer, and more accurate procedures and is particularly useful for complex cases (e.g., spine).
Review of Techniques
Cementoplasty
Patient Selection and Technique
Osteolytic tumours (e.g., metastasis, multiple myeloma, lymphoma) that are located near the vertebral body, acetabulum, and condyles and that cause local pain, disability, and a risk of compression fracture are excellent indications for cementoplasty.
Cementoplasty can be performed with the patient under sedation or general anaesthesia (especially for multilevel vertebroplasty) [12, 13] using fluoroscopic or/and CAT guidance. For vertebroplasty, a 10- or 15-gauge beveled needle (for thoracic/lumbar and cervical level, respectively) should be used. Cement injection should be performed under real-time imaging (fluoroscopic-lateral view, multislice fluoro-CAT).
Patient Outcome
Significant pain relief (>50% decrease in narcotic analgesics used or >50% pain decrease per visual analogue scale) has been reported in 75% to 85% of patients [8, 14–16]. Improved results have been obtained by combining thermal ablation and cementoplasty in cases of paravertebral tumor extension or soft-tissue extension [17].
Complications
Cement leakage has been reported to occur in 38% to 72.5% of patients [18]; lung embolism, infection, and fracture in <1% of patients; and allergic reaction, puncture-site bleeding, and acute increased pain or new areas of pain in 14% of patients [16].
Chemical Ablation with Ethanol
Patient Selection and Technique
Palliative treatment can be offered to patients with osteolytic painful bone tumours without risk of fracture [5]. The procedure should be performed strictly with the patient under deep sedation or general anaesthesia (due to the pain induced during ethanol injection in bone and soft tissue) and under CAT guidance. According to the size and number of lesions and level of pain relief desired, alcoholization using 3 to 25 ml sterile 95% ethanol is administered either as a multisession technique or as a one-shot technique through a 22-gauge needle.
Nonionic iodinated contrast medium should be always injected into the lesion before ethanol injection to predict the distribution. In patients with large tumours, alcohol should be selectively instilled into regions considered to be responsible for pain (usually the periphery of the tumour and osteolytic areas). The size and shape of the necrosis induced with ethanol is not always reproducible and depends on the degree of vascularization, necrosis, and tissue consistency.
Patient Outcome
Pain relief has been reported in 74% of patients and usually occurs within 24 hours. In 26% of cases, decreased tumour size has been observed, whereas in 18.5% of cases tumour size continues to increase. Duration of pain relief ranges from 10 to 27 weeks. The best results are obtained in patients with small lytic metastases (i.e., diameter ranging from 3 to 6 cm) [9].
Complications
Minor complications include low-grade fever (17%), hyperuricemia, and pain during the first 6 hours. Major complications include infection and accidental leakage causing damage to the contiguous neurologic structures (<1.5%).
Laser Ablation
Patient Selection and Technique
Because of the small size of the ablation zone produced, laser is mostly used for patients with small tumours or in those with contraindications to radiofrequency ablation (RFA) (e.g., metallic implants). Multiple fibres are required for patients with larger tumours.
Osteoid Osteomas
The best indication is tumour size (<1 cm in diameter). The procedure should always be performed with the patient under general anaesthesia or regional block (severe pain is typically experienced during penetration of the nidus). The laser fibre (400–600 μm) is always inserted coaxially into the tumour under CAT guidance through a spinal needle or drill needle when necessary. The choice of access route (all neurovascular structures should be avoided) and diffusion of heat should be taken into account to avoid complications. If required, additional insulation techniques and thermal monitoring should be applied to protect adjacent vulnerable structures. The positioning of the fibre exactly in the centre of the nidus is the key to a successful procedure. Two-watt power is applied for 6–10 min depending on tumour size. At the end of ablation, 5–10 ml rupivacaine 2 mg/ml is injected (strictly extravascularly) in contact with the periosteum to decrease postprocedural pain.
Painful Bone Metastases
Painful bone metastases can be treated by inserting ≤8 simultaneously energized bare fibres into the tumour with approximately 1.5-cm spacing.
Patient Outcome
The success rate for ablation of osteoid osteomas is similar to that of RF, with a 95% success rate in a single session [1, 19, 20].
Major Complications
Major complications include neurologic damage of contiguous structures and neurodystrophia (<0.5% of patients) [21].
Recurrence Rate
The recurrence rate for osteoid osteoma is approximately 5% (mainly in intra-articular lesions) [1].
RFA
Patient Selection and Technique
The indications for RFA in bone can be curative or palliative [22].
Major Indications
Curative indications include patients with primary (e.g., osteoid osteoma, osteoblastoma, chondroblastoma) or secondary bone tumours with contraindications to surgery or patient refusal of surgery (tumour size should be <5 cm in diameter). Palliative indications include painful bone metastases (pain not controlled by conventional therapies).
Ablation protocols vary according to lesion size and generator used. The best guidance modality is CAT with or without fluoroscopy [23]. Bone RFA requires regional block or general anaesthesia. At the end of ablation, 5 to 10 ml rupivacaine 2 mg/ml is injected (strictly extravascularly) in contact with the periosteum to decrease postprocedural pain.
In osteoid osteoma, RFA technique is similar to that for laser ablation. The small size of the nidus does not require large ablation with expandable and multitined or perfusion and internally cooled electrodes. A 1-cm active-tip electrode is used to reach a temperature of 90°C within 6 to 10 minutes. If cortical bone must be passed through, a bone biopsy needle must be used, and the electrode is coaxially inserted into the lesion. Because the bone needle is not insulated, it should not come into contact with the active part of the RFA electrode. For tumours in close proximity to neurologic structures or other organs, thermal protection techniques are required [24]. RFA seems to be promising for the treatment of chondroblastomas, although few published data exist on outcomes exist [25–27].
For large volumes of ablation in tumours involving weight-bearing bones, additional consolidation with cementoplasty or surgery should be considered to prevent the risk of secondary fracture [28]. If cementoplasty is performed in the same session with RFA, the injection should be delayed until the tumour temperature has decreased to normal levels to avoid setting the cement too quickly.
The major advantage of RFA compared with chemical ablation (ethanol) is better delimitation of the ablation zone without risk of leak. The difficulty in treating bone tumours with RFA lies in thermal protection of vulnerable surrounding structures (particularly nerve roots) and penetration of the lesion, which in some cases requires coaxial introducer systems [2, 29].
Patient Outcome
For osteoid osteoma, the success rate of bone RFA is similar to that of laser therapy (>85% of patients), and the recurrence rate has been reported to be 5–10% [20, 30]. A 10–15% recurrence rate has been noted for typical osteoblastoma, and a 50% rate has been reported for aggressive osteoblastoma. An acute postablation inflammatory reaction can occur and should be prevented with administration of anti-inflammatory therapy. When using RFA for pain palliation in painful malignant bone tumours, significant (>50%) and rapid pain relief, including a subsequent substantial decrease in medication, has been reported in 70–95% of patients [4, 21, 31–34]. Because of advanced disease, recurrence of pain in relation to other metastases is common, but most patients remain pain free at the ablated area.
Complications
Complications include thermal damage of contiguous structures (insulation techniques and thermal monitoring are mandatory to decrease theses risks) and infection.
Cryoablation
Patient Selection and Technique
The indications and procedural technique are similar to those for RFA. Cryoablation is efficient for both lytic and sclerotic tumours. Procedure planning remains the same. However, compared with RFA, ≤25 cryoprobes (17-gauge; best gap between probes is 2 cm) can be inserted simultaneously [35].
The procedure is performed with the patient under sedation or general anaesthesia using CAT or MRI guidance (MRI-compatible cryoprobes exist on the market). Percutaneous cryoablation appears to require less analgesia than RFA [36]. Cryoablation of skeletal metastases is a time-consuming procedure [37] because two 10-minute freeze cycles, separated by an 8-min passive thaw, should be performed per position. Monitoring of the ice ball (of predictable geometry based on the length and diameter of the expansion room at the tip of the probe) is necessary and can be achieved with CAT imaging (e.g., hypodense ice ball). For complete necrosis of the tumour, it is important to extend the margins of the ice ball by a minimum 5-mm distance beyond the tumour margins to ensure complete cell death.
When thermal insulation is required, fluid should be avoided. For the best tissue insulation and protection of surrounding organs, carbon dioxide (CO2) should be used [24].
For large volumes of ablation in tumours involving weight-bearing bones, additional consolidation with cementoplasty or surgery should be considered to prevent the risk of secondary fracture [28, 38]. If cementoplasty is performed in the same session with cryoablation, injection should be delayed until the temperature of the tumour has increased to normal levels to avoid cement leakage.
Compared with other ablation techniques, cryotherapy offers the major advantages of direct visualization of the ice ball, simultaneous use of ≤25 probes, and less postprocedural pain [37, 39].
Effective cryoablation tissue injury depends on four criteria:
-
1.
excellent monitoring of the process;
-
2.
fast cooling to a lethal temperature;
-
3.
slow thawing; and
- 4.
Patient Outcome
Percutaneous cryoablation is a safe and effective method for palliation of pain caused by metastatic disease and has been reported to provide significant pain relief in ≤75% of patients [37].
Complications
Complications include cryoshock phenomenon, a rare syndrome that happens after large ablations, especially in the liver, occurs in 1% to 3.8% of patients [45–47] as well as thermal damage to contiguous neural structures (temporary neuropraxia at –20°C and permanent neurologic damage at ≤40°C) [48].
Radiofrequency Ionization
Patient Selection and Technique
The best candidates for this technique are (1) patients having painful nonsurgical spinal tumours with intracanalar extension and (2) patients with rupture of the posterior wall of the vertebral body and thus a high risk of cement leakage or shift of the tumour in the canal, both of which have neurologic consequences.
A bone trocar is used to allow tumoral access and coaxial insertion of the RFA 16-gauge bipolar electrode. A side-arm catheter is connected to the electrode to slowly inject saline solution for activation of the plasma field. The angled tip of the electrode allows the digging of several channels inside the tumour by rotation of the electrode on its axis. In spinal lesions after cavitation, acrylic cement is injected into the cavity for consolidation [21, 48].
Patient Outcome
Decreased neuralgia has been reported in ≤87% of patients [48] (due to tumour decompression). Decreased cement leakage, although reported, requires further evaluation.
Complications
Complications include accidental damage to nerve roots and perforation of adjacent organs.
Thermal Insulation and Monitoring
Thermal insulation and monitoring is used to protect important anatomic structures from thermal injury during application of different thermal ablation techniques. Heating at ≥45°C has been shown to be neurotoxic to the spinal cord and the peripheral nerves. Interposition of bone increases the insulation but depends on the thickness of bone lamella [2]. Precautionary measures should be taken when no intact insulating cortex remains between the tumour and the neurologic structures. The risk of thermal damage increases with the size of the active tip of the electrode [29, 49]. Thermal insulation techniques and thermal monitoring can be used alone or in combination, if necessary, to decrease unintended thermal injury to nontarget structures.
Thermal Insulation
Thermal insulation consists of fluid, gas, or balloon interposition between adjacent nontarget structures and the ablation zone [1, 50–52]. Hydrodissection is one of the most commonly used techniques. With aerodissection, CO2 is injected using a dedicated CO2 injection syringe, which allows precise control of the volume of gas insufflated in the desired zone under positive pressure [24].
-
RFA Saline is not a suitable solution (because of its high electrical conductivity), and dextrose in water 5% has been advocated.
-
Cryoablation Carbon dioxide can be used to displace the nontarget structures away from the treatment zone, thus creating an excellent thermal insulator blanket. Fluid is not suitable because it can freeze in contact with the ice ball. In ultrasound-guided interventions, CO2 dissection cannot be used (the ring-down artifact from gas deteriorates the image).
Thermal Monitoring
Thermal monitoring is achieved with thermocouples inserted coaxially through an 18-gauge spinal needle [53]. Special care is needed with RFA because the tip of metal-based thermocouple should never be placed too close to the RFA electrode (this could result in arcing and electrical conductivity).
Conclusion: Proposed Treatment Strategy
-
Precise clinical evaluation of the patient is mandatory and should include origin and location of pain, previous treatment, patient-tolerated anaesthesia, and life expectancy.
-
Whole-body 3-D imaging should be used to precisely analyze the lesions and their relation to surrounding structures.
-
Multidisciplinary decision making is required to choose the most efficient and least disabling technique.
-
1.
For a painful tumour involving a flat weight-bearing bone without invasion of surrounding tissues and associated with risk of compression fracture, single cementoplasty is the most appropriate technique.
-
2.
For a painful bone tumour with extension into surrounding soft tissues, thermal ablation is required to control the pain caused by soft-tissue invasion. However, if there is a risk of pathologic fracture, an additional consolidation technique is required (cementoplasty for flat bones or surgery for long bones).
-
3.
For nonsurgical spinal tumours extending toward the canal with rupture of the posterior wall and epidural extension, percutaneous tumour decompression using radiofrequency ionization is the best technique. After tumour decompression, the cavity created can be filled with cement (Algorithm 1).
Algorithm 1 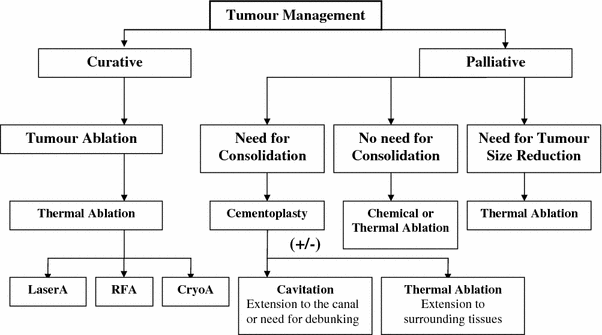
Tumour-management therapeutic option algorithm

References
Gangi A, Alizadeh H, Wong L, Buy X, Dietemann JL, Roy C (2007) Osteoid osteoma: percutaneous laser ablation and follow-up in 114 patients. Radiology 242:293–301
Dupuy DE, Hong R, Oliver B, Goldberg SN (2000) Radiofrequency ablation of spinal tumors: temperature distribution in the spinal canal. AJR 175:1263–1266
Goldberg SN (2001) Image-guided radiofrequency tumour ablation: challenges and opportunities. II. J Vasc Interv Radiol 12:1135–1148
Thanos L, Mylona S, Galani P et al (2008) Radiofrequency ablation of osseous metastases for the palliation of pain. Skeletal Radiol 37:189–194
Gangi A, Dietemann JL, Schultz A, Mortazavi R, Jeung MY, Roy C (1996) Interventional radiologic procedures with CT guidance in cancer pain management. Radiographics 16:1289–1386
Gangi A, Guth S, Imbert JP, Marin H, Dietemann JL (2003) Percutaneous vertebroplasty: indications, technique, and results. Radiographics 23:e10
Jang JS, Lee SH (2005) Efficacy of percutaneous vertebroplasty combined with radiotherapy in osteolytis metastatic spinal tumors. J Neurosurg 2:243–248
Weill A, Chiras J, Simon JM, Rose M, Sola-Martinez T, Enkaoua E (1996) Spinal metastases: indications for and results of percutaneous injections of acrylic surgical cement. Radiology 199:241–247
Gangi A, Kastler B, Klinkert A, Dietemann JL (1994) Injection of alcohol into bone metastases under CT guidance. J Comput Assist Tomogr 18:932–935
Baust J, Chang Z (1995) Underlying mechanisms of damage and new concepts in cryosurgical instrumentation. International Institute of Refrigeration, Paris
Mazur P (1997) The role of intracellular freezing in the death of cells cooled at supraoptimal rates. Cryobiology 14:251–272
Mathis JM WW (2003) Percutaneous vertebroplasty: technical cinsiderations. J Vasc Interv Radiol 14:953–960
McGraw JK, Cardella J, Barr JD et al (2003) Society of Interventional Radiology quality improvement guidelines for percutaneous vertebroplasty. J Vasc Interv Radiol 14(Suppl):S311–S315
Yamada K, Matsumoto Y, Kita M, Yamamoto K, Kobayashi TTT (2004) Long-term pain-relief effects for patients undergoing percutaneous vertebroplasty for metastatic vertebral tumor. J Ansth 18:292–295
Cotten A, Dewatre F, Cortet B et al (1996) Percutaneous vertebroplasty for osteolytic metastases and myeloma: effects of the percentage of lesion filling and the leakage of methyl methacrylate at clinical follow-up. Radiology 200:525–530
Shimony JS, Gilula LA, Zeller AJ, Brown DB (2004) Percutaneous vertebroplasty for malignant compression fractures with epidural involvement. Radiology 232:846–853
Buy X, Basile A, Bierry G, Cupelli J, Gangi A (2006) Saline-infused bipolar radiofrequency ablation of high-risk spinal and paraspinal neoplasms. AJR Am J Roentgenol 186(Suppl):S322–S326
Laredo JD, Hamze B (2004) Complications of percutaneous vertebroplasty and their prevention. Skeletal Radiol 33:493–505
Witt JD, Hall-Craggs MA, Ripley P, Cobb JP, Bown SG (2000) Interstitial laser photocoagulation for the treatment of osteoid osteoma. J Bone Joint Surg Br 82:1125–1128
Rosenthal DI, Hornicek FJ, Torriani M, Gebhardt MC, Mankin HJ (2003) Osteoid osteoma: percutaneous treatment with radiofrequency energy. Radiology 229:171–175
Gangi A, Guth S, Guermazi A (2009) Imaging in percutaneous musculoskeletal interventions. Springer, Berlin-Heidelberg, Germany
Gangi A, Basile A, Buy X, Alizadeh H, Sauer B, Bierry G (2005) Radiofrequency and laser ablation of spinal lesions. Semin Ultrasound CT MR 26:89–97
Gangi A, Kastler BA, Dietemann JL (1994) Percutaneous vertebroplasty guided by a combination of CT and fluoroscopy. AJNR Am J Neuroradiol 15:83–86
Buy X, Tok CH, Szwarc D, Bierry G, Gangi A (2009) Thermal protection during percutaneous thermal ablation procedures: interest of carbon dioxide dissection and temperature monitoring. Cardiovasc Intervent Radiol 32:529–534
Christie-Large M, Evans N, Davies AM, James S (2008) Radiofrequency ablation of chondroblastoma: procedure, technique and MR imaging follow up of four cases. Skeletal Radiol 37:1011–1017
Erickson JK, Rosenthal DI, Zaleske DJ, Gebhardt M, Cates J (2001) Primary treatment of chondroblastoma with percutaneous radiofrequency heat ablation: report of three cases. Radiology 221:463–468
Rybak DL, Rosenthal ID, James WC (2009) Chondroblastoma: radiofrequency ablation—alternative to surgical resection in selected cases. Radiology 251:599–604
Toyota N, Naito A, Kakizawa H et al (2005) Radiofrequency ablation therapy combined with cementoplasty for painful bone metastases: initial experience. Cardiovasc Intervent Radiol 28:578–583
Bitsch RG, Rupp R, Bernd L, Ludwig K (2006) Osteoid osteoma in an ex vivo animal model: temperature changes in surrounding soft tissue during CT-guided radiofrequency ablation. Radiology 238:107–112
Rosenthal DI, Springfield DS, Gebhardt MC, Rosenberg AE, Mankin HJ (1995) Osteoid osteoma: percutaneous radio-frequency ablation. Radiology 197:451–454
Callstrom MR, Charboneau JW, Goetz MP et al (2002) Painful metastases involving bone: feasibility of percutaneous CT- and US-guided radio-frequency ablation. Radiology 224:87–97
Kojima H, Tanigawa N, Kariya S, Komemushi A, Shomura YSS (2006) Clinical assessment of percutaneous radiofrequency ablation for painful metastatic bone tumors. CVIR 29:1022–1026
Callstrom MR, Charboneau JW (2007) Image-guided palliation of painful metastases using percutaneous ablation. Tech Vasc Interv Radiol 10:120–131
Goetz MP, Callstrom MR, Charboneau JW et al (2004) Percutaneous image-guided radiofrequency ablation of painful metastases involving bone: a multicenter study. J Clin Oncol 22:300–306
Theodorescu D (2004) Cancer cryotherapy: evolution and biology. Rev Urol 6(Suppl 4):S9–S19
Allaf ME, Varkarakis IM, Bhayani SB, Inagaki T, Kavoussi LR, Solomon SB (2005) Pain control requirements for percutaneous ablation of renal tumors: cryoablation versus radiofrequency ablation—Initial observations. Radiology 237:366–370
Callstrom MR, Atwell TD, Charboneau JW et al (2006) Painful metastases involving bone: percutaneous image-guided cryoablation—prospective trial interim analysis. Radiology 241:572–580
Bickels J, Kollender Y, Merimsky O, Isaakov J, Petyan-Brand R, Meller I (2004) Closed argon-based cryoablation of bone tumours. J Bone Joint Surg Br 86:714–718
Beland MD, Dupuy DE, Mayo-Smith WW (2005) Percutaneous cryoablation of symptomatic extraabdominal metastatic disease: preliminary results. AJR Am J Roentgenol 184:926–930
Baust JG, Gage AA (2004) Progress toward optimization of cryosurgery. Tech Cancer Res Treat 3:95–101
Clarke DM, Robilotto AT, Rhee E et al (2007) Cryoablation of renal cancer: variables involved in freezing-induced cell death. Technol Cancer Res Treat 6:69–79
Gage AA, Baust J (1998) Mechanisms of tissue injury in cryosurgery. Cryobiology 37:171–186
Hoffmann NE, Bischof JC (2002) The cryobiology of cryosurgical injury. Urology 60:40–49
Littrup PJ, Ahmed A, Aoun HD et al (2007) CT-guided percutaneous cryotherapy of renal masses. J Vasc Interv Radiol 18:383–392
Bageacu S, Kaczmarek D, Lacroix M, Dubois J, Forest J, Porcheron J (2007) Cryosurgery for resectable and unresectable hepatic metastases from colorectal cancer. Eur J Surg Oncol 33:590–596
Seifert JK, France MP, Zhao J et al (2002) Large volume hepatic freezing: association with significant release of the cytokines interleukin-6 and tumor necrosis factor a in a rat model. World J Surg 26:1333–1341
Seifert JK, Morris DL (1999) World survey on the complications of hepatic and prostate cryotherapy. World J Surg 23:109-113 (discussion 113–104)
Georgy BA, Wong W (2007) Plasma-mediated radiofrequency ablation assisted percutaneous cement injection for treating advanced malignant vertebral compression fractures. AJNR Am J Neuroradiol 28:700–705
Adachi A, Kaminou T, Ogawa T et al (2008) Heat distribution in the spinal canal during radiofrequency ablation for vertebral lesions: study in swine. Radiology 247:374–380
Diehn FE, Neeman Z, Hvizda JL, Wood BJ (2003) Remote thermometry to avoid complications in radiofrequency ablation. J Vasc Interv Radiol 14:1569–1576
Laeseke PF, Sampson LA, Brace CL, Winter TC III, Fine JP, Lee FT Jr (2006) Unintended thermal injuries from radiofrequency ablation: protection with 5% dextrose in water. AJR Am J Roentgenol 186(Suppl):S249–S254
Kam AW, Littrup PJ, Walther MM, Hvizda J, Wood BJ (2004) Thermal protection during percutaneous thermal ablation of renal cell carcinoma. J Vasc Interv Radiol 15:753–758
Nakatsuka A, Yamakado K, Takaki H et al (2009) Percutaneous radiofrequency ablation of painful spinal tumors adjacent to the spinal cord with real-time monitoring of spinal canal temperature: a prospective study. CVIR 32:70–75
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License ( https://creativecommons.org/licenses/by-nc/2.0 ), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
About this article
Cite this article
Gangi, A., Tsoumakidou, G., Buy, X. et al. Quality Improvement Guidelines for Bone Tumour Management. Cardiovasc Intervent Radiol 33, 706–713 (2010). https://doi.org/10.1007/s00270-009-9738-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00270-009-9738-9