
Abstract
Importance
Rectal cancers occupy the eighth position worldwide for new cases and deaths for both men and women. These cancers have a high tendency to form metastases in the mesorectum but also in the lateral lymph nodes. The therapeutic approach for the involved lateral lymph nodes remains controversial.
Objective
We performed a systematic review and meta-analysis to assess the prevalence of metastatic lateral lymph nodes in patients with lateral lymph node dissection (LLND) for rectal cancer, which seems to be a fundamental and necessary criterion to discuss any possible indications for LLND.
Methods
Data sources–study selection–data extraction and synthesis–main outcome and measures. We searched MEDLINE, EMBASE and COCHRANE from November 1, 2018, to November 19, 2018, for studies reporting the presence of metastatic lateral lymph nodes (iliac, obturator and middle sacral nodes) among patients undergoing rectal surgery with LLND. Pooled prevalence values were obtained by random effects models, and the robustness was tested by leave-one-out sensitivity analyses. Heterogeneity was assessed using the Q-test, quantified based on the I2 value and explored by subgroup analyses.
Results
Our final analysis included 31 studies from Asian countries, comprising 7599 patients. The pooled prevalence of metastatic lateral lymph nodes was 17.3% (95% CI: 14.6–20.5). The inter-study variability (heterogeneity) was high (I2 = 89%). The pooled prevalence was, however, robust and varied between 16.6% and 17.9% according to leave-one-out sensitivity analysis. The pooled prevalence of metastatic lymph nodes was not significantly different when pooling only studies including patients who received neoadjuvant treatment or those without neoadjuvant treatment (p = 0.44). Meta-regression showed that the pooled prevalence was associated with the sample size of studies (p < 0.05), as the prevalence decreased when the sample size increased.
Conclusion
The pooled prevalence of metastatic lateral lymph nodes was 17.3% among patients who underwent rectal surgery with LLND in Asian countries. Further studies are necessary to determine whether this finding could impact the therapeutic strategy (total mesorectal excision with LLND versus total mesorectal excision with neoadjuvant radiochemotherapy).
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Rectal cancer metastasizes to the perirectal lymph nodes contained within the mesorectum and along the iliac arteries [1]. Assessment of lymph node involvement is a strong predictor of recurrence-free survival and overall survival in patients with rectal cancer [2]. Currently, total mesorectal excision constitutes the gold standard for removing perirectal lymph nodes [3]. However, the therapeutic strategy regarding lymph nodes, notably those located along the iliac arteries, may include neoadjuvant radiochemotherapy, as performed in Western countries [3], or lateral lymph node dissection (LLND), as performed in Japan when the lower border of the tumour is located under the reflection of the peritoneum and when it has passed the muscularis propria [4].
However, to date, only two randomized controlled trials (RCTs) [5, 6] have compared the outcomes of the two therapeutic strategies in terms of survival, looking at local and distant recurrences and complications. Furthermore, the choice of the best strategy, either LLND or radiochemotherapy or the combination of the two treatments, is difficult to identify, as the prevalence of metastatic lateral lymph nodes in patients with rectal cancer is poorly documented. Indeed, before comparing two therapeutic strategies and their outcomes, it is necessary and more relevant to know if it is legitimate to propose them as a treatment; in other words, if they would even correctly target metastatic lateral lymph nodes (LLNs).
Therefore, our objective was to perform a systematic review and meta-analysis reporting on the prevalence of metastatic lateral lymph nodes in patients with rectal cancer with the hypothesis that this meta-analysis will elucidate the best therapeutic strategy in the current absence of reliable assessment of tumour aggressiveness.
Materials and methods
The present methodology is in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklist (Table S1).
Literature search and study selection
A literature search was conducted in MEDLINE, EMBASE and COCHRANE from inception (DATE??) until November 19, 2018. Keyword combinations are reported in Table S2. Additional records were identified by manually searching the reference lists of the included publications. To be included, studies had to be written in English or French and to report the prevalence of metastatic lateral lymph nodes among patients with rectal cancer who underwent surgery with LLND. LLND was defined by the dissection of nodes included in areas such as the common iliac (IC), internal iliac (II), external iliac (EI), obturator (O), middle sacral (MS) and aorta bifurcation (Ao).
We excluded case series, conference abstracts, letters to the editor and secondary analyses of previously published papers.
Data extraction
Two independent reviewers (NC and JM) independently selected articles for inclusion and extracted the data according to a pre-established data collection form. Discrepancies were resolved by reaching a consensus with the senior authors (NCB and FR). The following data were extracted: first author; publication year; country where the study took place; study period, after and before 2010 due to modifications of the Japanese Guidelines for LLND; study design; number of patients who underwent LLND, prophylactic: dissection and removal of nodes that seem invaded (enlarged) based on pre- and peri-operative examinations, versus therapeutic/curative: removal of all nodes in the “lateral lymph area”; sex; number of patients with metastatic lateral lymph nodes; number of patients who underwent pre-operative radio- and/or chemotherapy; type of neoadjuvant treatment in those patients; and oncological stages of included patients.
Statistical analysis
Models with random effects (DerSimonian and Laird’s approach [7]) were used to combine the prevalence of metastatic lateral lymph nodes across the studies. A logit transformation was applied to prevalence before statistical pooling, and the pooled logit of prevalence was then transformed back. Heterogeneity was assessed by using the I2 statistic, and a leave-one-out sensitivity analysis was conducted to check the robustness of the pooled prevalence. Potential sources of heterogeneity were investigated by comparing the pooled prevalence between subgroups of studies. A sensitivity analysis was also conducted excluding stage 4 patients from the denominator and from the numerator of the prevalence because stage 4 patients were assumed to have metastatic lateral lymph nodes (model with random effects). In addition, a meta-regression analysis was conducted to assess the relationship between the sample size of studies and the prevalence with the restricted maximum likelihood method. [8] All analyses were performed with the Meta and Metafor packages for R version 3.3.1 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Literature search and study characteristics
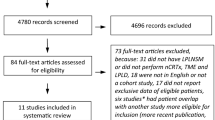
Two hundred and sixty-five publications were identified in MEDLINE, EMBASE and COCHRANE. Three publications were identified from other sources. Fifteen duplicates were removed. Of the 250 publications that were identified as eligible, 155 were excluded after title/abstract screening, and 64 were excluded after full-text screening (44 publications did not report the number of patients with metastatic lateral lymph nodes and 20 publications did not distinguish patients with metastatic lateral lymph nodes from those with metastatic lymph nodes from other areas). Ultimately, 31 publications [5, 6, 9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37] were included in the quantitative synthesis, all coming from Japan except one from China (Fig. 1, Table 1).

Flow chart showing the selection of publications for quantitative review. Forest plot of the prevalence of metastatic lateral lymph nodes in patients who underwent lateral lymph node dissection. Each horizontal bar summarizes a study. The bars represent 95% confidence intervals. The grey squares represent each of the studies’ weights in the meta-analysis. The diamond in the lower part of the graph depicts the pooled estimate along with 95% confidence intervals. Events = number of patients with metastatic lateral lymph nodes, total = number of patients who underwent lateral lymph node dissection for rectal cancer
Among the included publications, 28 were retrospective cohort studies [9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35, 37], one was a prospective cohort study [36] and two were RCTs [5, 6]. Thirty studies were performed in Japan [5, 6, 9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33, 35,36,37] and one in China [34]. Eleven studies only included patients with TNM cancer stages 2 and 3 [5, 9,10,11,12,13, 15, 31, 32, 35, 38]. In 24 studies [5, 6, 9,10,11, 15, 17,18,19,20,21,22,23,24,25,26,27,28, 31,32,33,34,35, 37], systematic LLND was performed in all included patients, whereas in six studies [12,13,14, 16, 29, 30, 36], LLND was performed only in patients with enlarged lateral lymph nodes on pre-operative imaging, which distinguished these patients from others who had confirmation by histopathological results. In one study, the type of LLND was not described [28]. In two studies, patients underwent systematic bilateral dissection [22, 32]; in 27 studies, uni- or bilateral dissection was defined according to clinical and/or imaging findings [6, 12,13,14,15,16,17,18,19,20,21, 23, 25, 26, 28,29,30,31, 37,38,39] and in four studies, lateralization of dissection was not documented [24, 34,35,36]. Nine studies included patients who received neoadjuvant treatment [6, 11, 13,14,15,16,17, 30, 31]. Indications for neoadjuvant treatment were not documented in four studies [11, 15,16,17] and depended on tumour stage in five studies [13, 14, 16, 30, 31]. The characteristics of the included studies are reported in Tables 2, 3, S3, S4. It is worth noting that the study of Yano et al. has been classified above as a study with “curative LLND” because pre-imaging with enlarged nodes was considered the main decision-making criterion for LLND. However, in fact, after the flow chart analysis, dissection was also performed in a systematic way (Table S4). Thus, for statistical analysis, we classified it as a “prophylactic study”.
Prevalence of metastatic lateral lymph nodes
We obtained a pooled prevalence of metastatic lateral lymph nodes of 17.3% (95% CI: 14.6–20.5) (31 studies, 7599 patients) (Fig. 2). The inter-study variability (heterogeneity) was noteworthy, with I2 = 89%. In other words, the variation in study outcome (prevalence) between studies was high. Furthermore, the prediction interval was 6.5 to 38.6%. This means that if a new study is conducted, the assessed prevalence is likely, with a probability of 95%, to fall between 6.5 and 38.6%. However, the pooled prevalence was robust according to leave-one-out sensitivity analysis. The pooled prevalence varied from 16.6% (14.0 to 19.5%), when the study by Yano et al. [36] was omitted, to 17.9% (15.1 to 21.1%), when the study by Min et al. [16] was omitted (Fig. S1). The heterogeneity, however, remained stable, as the I2 statistic for heterogeneity varied from 85%, when the study by Sato et al. [18] was omitted, to 89.1%, when one of the following studies was omitted [6, 10, 13, 15, 21, 23, 25, 26, 32, 34, 35].

Meta-analysis of the prevalence of metastatic lateral lymph nodes
To determine whether neoadjuvant treatment could alter the prevalence of metastatic lateral lymph nodes, we performed subgroup analyses by separately pooling studies reporting patients who received neoadjuvant treatment from others (Fig. S2). The difference in pooled prevalence of metastatic lateral lymph nodes between studies with versus without neoadjuvant treatment was 16.9% (95% CI: 14.1–20.2), but the inter-study variability (heterogeneity) was high important, with I2 = 88%.
Then, we explored whether the heterogeneity could be explained by changes in the therapeutic strategies across the years. The pooled prevalence of metastatic lateral lymph nodes between studies published before and after 2010 was 17.3% (95% CI: 14.6–20.4), but the inter-study variability (heterogeneity) was noteworthy, with I2 = 89% (Fig. S3).
Furthermore, we excluded patients with TNM stage IV (in six studies). After exclusion of these patients, the pooled prevalence of metastatic lateral lymph nodes was 15.8% (95% CI 13.1 to 18.9) (Fig. S4).
Then, we separately pooled studies according to the type of LLND performed (systematic versus curative). The difference in the pooled prevalence of metastatic lateral lymph nodes between studies with systematic or curative dissection was not statistically significant (p = 0.7111) (Fig. S5).
However, the pooled prevalence of metastatic lateral lymph nodes appeared to be associated with the sample size of studies (p = 0.005): the prevalence decreased when the sample size increased (Fig. S6). Meta-regression showed that, on average, a study with a sample size that was 10 times larger than that of some other study had an estimated odds ratio for prevalence that was reduced by approximately 50% (Fig. S7).
Discussion
We performed a systematic review and meta-analysis estimating the prevalence of metastatic lateral lymph nodes in patients with rectal cancer. By pooling 31 studies of Asian origin (30 from Japan and one from China) totalling 7599 patients, we found a prevalence of metastatic lateral lymph nodes of 17.3%, thereby underlining the importance of further examination of the treatment of these node areas to avoid cancer recurrence.
Six studies included patients with TNM stage IV rectal cancer. According to the most recent Japanese guidelines, metastatic disease is not the most important stage to indicate LLND [4]. However, within this stage, some patients may present both primary tumour and resectable distant metastases, thus proceeding to the possibility of undergoing LLND. As a result, to understand the prevalence of metastatic lymph nodes within the most common indications, we excluded patients with TNM stage IV disease by considering them to have metastatic lateral lymph nodes. After exclusion, the pooled prevalence of metastatic lateral lymph nodes remained stable (15.8%).
In the present systematic review and meta-analysis, we were not able to show any improvement in neoadjuvant treatment in terms of lateral lymph node metastasis. However, it should be noted that the power of this subgroup analysis might be insufficient. Additionally, Asian protocols differed from Western protocols, and only a small proportion of patients among studies with neoadjuvant treatment benefited from that modality. Therefore, it is not possible to draw any conclusions about the efficacy of neoadjuvant treatment in terms of the prevalence of metastatic lateral lymph nodes based on our results. Despite this, it is worth noting that neoadjuvant treatments between the studies were quite similar using 5-fluorouracil, oxaliplatin and irinotecan (Table S3).
Some centres performed systematic LLND, whereas others performed LLND in patients with enlarged lateral lymph nodes diagnosed by pre-operative imaging. We pooled these studies separately and found no difference in terms of metastatic lateral lymph nodes. After 2010, as Japanese guidelines changed and recommended limiting LLND for all cT3-T4 tumours with a lower edge below the peritoneal reflection, we reported a subgroup analysis of the pooled prevalence of metastatic LLN according to the publication date. Due to the high heterogeneity, we cannot interpret this result as significant.
Furthermore, we note that meta-regression showed that the pooled prevalence of metastatic lymph nodes was associated with the sample size of studies, as the prevalence of metastatic lymph nodes decreased when the sample size increased. We think that this might be explained by more selective indications for LLND in studies including fewer patients with LLND. Thus, even if the number of studies between curative and systematic LLND intention was not the same, the tendency of the sample size of studies with curative LLND was lower. This indirectly shows that smaller studies were more likely to have a selected population. As a consequence, studies with larger sample sizes (in other words, studies with prophylactic LLND) were more likely to represent the “real” proportion of patients with rectal cancer with LLN metastasis.
Our meta-analysis is the first to examine the prevalence of metastatic lateral lymph nodes, which seems to be an essential prerequisite before considering any treatment. Indeed, recent literature [40,41,42] directly questions the oncological and functional results of LLND without even first investigating whether it is necessary.
Advantages of the study
The strengths of our systematic review and meta-analysis are as follows: 1) the inclusion of a large number of studies reporting the prevalence of metastatic lateral lymph nodes based on histopathological analysis and to clarify, for the first time to our knowledge, its subsequent effects in patients operated on for rectal cancer; and 2) the highlighting of the necessity of systematic treatment of lateral lymph nodes due to the high prevalence (17.3%) of LLN metastasis. Indeed, despite the heterogeneity of the studies, which could have impacted the aim of our work, we were able to make some sound calculations due to a specific statistical analysis methodology.
Limitations of the study
The limitations of the present study are as follows: 1) the high heterogeneity of the calculated pooled prevalence of metastatic lateral lymph nodes, resulting from the quality and heterogeneity of the included publications; and 2) the final analysis included 31 papers, most of which were from Japan and were retrospective studies. Therefore, some patients might have overlapped because these papers were published from some limited leading hospitals. Moreover, it is worth noting that by focussing on patients who have benefited from LLND, a surgical procedure that is most common in Asian countries, selection has been carried out. As a result, it is expected that the selected studies tend to oversample patients with indications for LLND, with these patients being more likely to have advanced disease. Thus, a bias could have been introduced. The percentage of 17.3% of metastatic LLNs could have been overestimated. This element can explain the counter-intuitive (but non-significant) results of a higher prevalence of metastasis in the prophylactic LLND group (17.3%) versus the curative group (15.9%).
Conclusion
In conclusion, this systematic review and meta-analysis of Asian studies indicates that the prevalence of metastatic lateral lymph nodes in patients with low rectal cancer who underwent surgery is 17.3%. This prevalence is of clinical importance, as it may result in cancer recurrence and calls for the systematic treatment of these lymph node areas. Future randomized controlled trials should determine which therapeutic strategy, whether neoadjuvant radiochemotherapy versus systematic or imaging-guided lateral lymph node dissection, offers the best improvement in overall and recurrence-free survival.
Abbreviations
- LLND:
-
Lateral lymph node dissection
- RCT:
-
Randomized controlled trial
References
Funahashi K, Koike J, Shimada M, Okamoto K, Goto T, Teramoto T (2006) A preliminary study of the draining lymph node basin in advanced lower rectal cancer using a radioactive tracer. Dis Colon Rectum 49(10 Suppl):S53-58
Manfredi S, Benhamiche AM, Meny B, Cheynel N, Rat P, Faivre J (2001) Population-based study of factors influencing occurrence and prognosis of local recurrence after surgery for rectal cancer. Br J Surg 88(9):1221–1227
van de Velde CJ, Boelens PG, Borras JM et al (2014) EURECCA colorectal: multidisciplinary management: European consensus conference colon and rectum. Eur J Cancer 50(1):1-e1
Watanabe T, Muro K, Ajioka Y et al (2018) Japanese Society for Cancer of the Colon and Rectum (JSCCR) guidelines 2016 for the treatment of colorectal cancer. Int J Clin Oncol 23(1):1–34
Fujita S, Akasu T, Mizusawa J et al (2012) Postoperative morbidity and mortality after mesorectal excision with and without lateral lymph node dissection for clinical stage II or stage III lower rectal cancer (JCOG0212): results from a multicentre, randomised controlled, non-inferiority trial. Lancet Oncol 13(6):616–621
Masaki T, Matsuoka H, Kobayashi T et al (2010) Quality assurance of pelvic autonomic nerve-preserving surgery for advanced lower rectal cancer–preliminary results of a randomized controlled trial. Langenbecks Arch Surg 395(6):607–613
DerSimonian R, Laird N (1986) Meta-analysis in clinical trials. Control Clin Trials 7(3):177–188
Viechtbauer W, Lopez-Lopez JA, Sanchez-Meca J, Marin-Martinez F (2015) A comparison of procedures to test for moderators in mixed-effects meta-regression models. Psychol Methods 20(3):360–374
Hara M, Hirai T, Nakanishi H et al (2007) Isolated tumor cell in lateral lymph node has no influences on the prognosis of rectal cancer patients. Int J Colorectal Dis 22(8):911–917
Ishibe A, Ota M, Watanabe J et al (2016) Prediction of lateral pelvic lymph-node metastasis in low rectal cancer by magnetic resonance imaging. World J Surg 40(4):995–1001
Kanemitsu Y, Komori K, Shida D et al (2017) Potential impact of lateral lymph node dissection (LLND) for low rectal cancer on prognoses and local control: a comparison of 2 high-volume centers in Japan that employ different policies concerning LLND. Surgery 162(2):303–314
Ishida H, Hatano S, Ishiguro T, Kumamoto K, Ishibashi K, Haga N (2012) Prediction of lateral lymph node metastasis in lower rectal cancer: analysis of paraffin-embedded sections. Jpn J Clin Oncol 42(6):485–490
Kagawa H, Kinugasa Y, Shiomi A et al (2015) Robotic-assisted lateral lymph node dissection for lower rectal cancer: short-term outcomes in 50 consecutive patients. Surg Endosc 29(4):995–1000
Matsuoka H, Nakamura A, Masaki T et al (2007) Optimal diagnostic criteria for lateral pelvic lymph node metastasis in rectal carcinoma. Anticancer Res 27(5B):3529–3533
Miyake Y, Mizushima T, Hata T et al (2017) Inspection of perirectal lymph nodes by one-step nucleic acid amplification predicts lateral lymph node metastasis in advanced rectal cancer. Ann Surg Oncol 24(13):3850–3856
Min BS, Kim JS, Kim NK et al (2009) Extended lymph node dissection for rectal cancer with radiologically diagnosed extramesenteric lymph node metastasis. Ann Surg Oncol 16(12):3271–3278
Sato T, Ozawa H, Hatate K et al (2011) A Phase II trial of neoadjuvant preoperative chemoradiotherapy with S-1 plus irinotecan and radiation in patients with locally advanced rectal cancer: clinical feasibility and response rate. Int J Radiat Oncol Biol Phys 79(3):677–683
Sato H, Maeda K, Maruta M (2011) Prognostic significance of lateral lymph node dissection in node positive low rectal carcinoma. Int J Colorectal Dis 26(7):881–889
Shimoyama M, Yamazaki T, Suda T, Hatakeyama K (2003) Prognostic significance of lateral lymph node micrometastases in lower rectal cancer: an immunohistochemical study with CAM5.2. Dis Colon Rectum 46(3):333–339
Yokoyama S, Takifuji K, Hotta T et al (2014) Survival benefit of lateral lymph node dissection according to the region of involvement and the number of lateral lymph nodes involved. Surg Today 44(6):1097–1103
Komori K, Kanemitsu Y, Kimura K et al (2013) Detailed stratification of TNM stage III rectal cancer based on the presence/absence of extracapsular invasion of the metastatic lymph nodes. Dis Colon Rectum 56(6):726–732
Masaki T, Takayama M, Matsuoka H et al (2008) Intraoperative radiotherapy for oncological and function-preserving surgery in patients with advanced lower rectal cancer. Langenbecks Arch Surg 393(2):173–180
Wu ZY, Wan J, Li JH et al (2007) Prognostic value of lateral lymph node metastasis for advanced low rectal cancer. World J Gastroenterol 13(45):6048–6052
Hida J, Yasutomi M, Fujimoto K, Maruyama T, Okuno K, Shindo K (1997) Does lateral lymph node dissection improve survival in rectal carcinoma? examination of node metastases by the clearing method. J Am Coll Surg 184(5):475–480
Ueno M, Oya M, Azekura K, Yamaguchi T, Muto T (2005) Incidence and prognostic significance of lateral lymph node metastasis in patients with advanced low rectal cancer. Br J Surg 92(6):756–763
Ueno H, Mochizuki H, Hashiguchi Y et al (2007) Potential prognostic benefit of lateral pelvic node dissection for rectal cancer located below the peritoneal reflection. Ann Surg 245(1):80–87
Steup WH, Hojo K, Moriya Y et al (1994) An analysis on the effect of blood transfusion on recurrence and survival in patients undergoing extended lymphadenectomy for colorectal cancer. Hepatogastroenterology 41(3):253–259
Mori T, Takahashi K, Yasuno M (1998) Radical resection with autonomic nerve preservation and lymph node dissection techniques in lower rectal cancer surgery and its results: the impact of lateral lymph node dissection. Langenbecks Arch Surg 383(6):409–415
Tan KY, Yamamoto S, Fujita S, Akasu T, Moriya Y (2010) Improving prediction of lateral node spread in low rectal cancers–multivariate analysis of clinicopathological factors in 1046 cases. Langenbecks Arch Surg 395(5):545–549
Nagasaki T, Akiyoshi T, Fujimoto Y et al (2017) Preoperative chemoradiotherapy might improve the prognosis of patients with locally advanced low rectal cancer and lateral pelvic lymph node metastases. World J Surg 41(3):876–883
Yamaoka Y, Kinugasa Y, Shiomi A et al (2017) Preoperative chemoradiotherapy changes the size criterion for predicting lateral lymph node metastasis in lower rectal cancer. Int J Colorectal Dis 32(11):1631–1637
Numata M, Yamaguchi T, Kinugasa Y et al (2017) Index of estimated benefit from lateral lymph node dissection for middle and lower rectal cancer. Anticancer Res 37(5):2549–2555
Yamaguchi T, Kinugasa Y, Shiomi A, Tomioka H, Kagawa H, Yamakawa Y (2016) Robotic-assisted vs. conventional laparoscopic surgery for rectal cancer: short-term outcomes at a single center. Surg Today 46(8):957–962
Yu YY, Wang C, Xu D, Shen XG, Ding SQ, Zhou ZG (2011) Mesorectal and lateral node metastasis and micrometastasis in lower rectal cancer. Hepatogastroenterology 58(107–108):745–748
Kobayashi H, Mochizuki H, Kato T et al (2009) Outcomes of surgery alone for lower rectal cancer with and without pelvic sidewall dissection. Dis Colon Rectum 52(4):567–576
Yano H, Saito Y, Takeshita E, Miyake O, Ishizuka N (2007) Prediction of lateral pelvic node involvement in low rectal cancer by conventional computed tomography. Br J Surg 94(8):1014–1019
Kinugasa T, Akagi Y, Ochi T et al (2013) Lateral lymph-node dissection for rectal cancer: meta-analysis of all 944 cases undergoing surgery during 1975–2004. Anticancer Res 33(7):2921–2927
Yamaguchi T, Kinugasa Y, Shiomi A, Tomioka H, Kagawa H (2016) Robotic-assisted laparoscopic versus open lateral lymph node dissection for advanced lower rectal cancer. Surg Endosc 30(2):721–728
Steup WH, Moriya Y, van de Velde CJ (2002) Patterns of lymphatic spread in rectal cancer. a topographical analysis on lymph node metastases. Eur J Cancer. 38(7):911–918
Du R, Zhou J, Li D, Zhang Q, Liu J, Ma C, et al. (2020) Postoperative morbidity and mortality after mesorectal excision with laparoscopic versus conventional open lateral lymph node dissection for advanced rectal cancer: a meta-analysis. Asian J Surg [Internet]. 11 août 2020; Disponible sur: http://www.sciencedirect.com/science/article/pii/S1015958420301950
Yang X, Yang S, Hu T, Gu C, Wei M, Deng X et al (2020) What is the role of lateral lymph node dissection in rectal cancer patients with clinically suspected lateral lymph node metastasis after preoperative chemoradiotherapy? a meta-analysis and systematic review. Cancer Med 9(13):4477–4489
Gao X, Wang C, Yu Y, Yang L, Zhou Z (2020) Lateral lymph node dissection reduces local recurrence of locally advanced lower rectal cancer in the absence of preoperative neoadjuvant chemoradiotherapy: a systematic review and meta-analysis. Disponible sur: https://europepmc.org/article/ppr/ppr216100
Author information
Authors and Affiliations
Contributions
JM conceived and designed the study. JM and NC acquired the data. CC analysed the data. NC, JM, CC, AB, NCB and FR interpreted the data. NC, JM, CC, AB, JRY, NCB and FR contributed to the writing of the manuscript and to its critical revision. NC, JM, CC, AB, JRY, NCB and FR approved the final version of the manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflicts of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Christou, N., Meyer, J., Combescure, C. et al. Prevalence of Metastatic Lateral Lymph Nodes in Asian Patients with Lateral Lymph Node Dissection for Rectal Cancer: A Meta-analysis. World J Surg 45, 1537–1547 (2021). https://doi.org/10.1007/s00268-021-05956-1
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-021-05956-1