
Abstract
Purpose
Wide-Awake Local Anaesthesia No Tourniquet (WALANT), a groundbreaking anaesthetic technique resurging in practice, warrants a comprehensive safety analysis for informed adoption. Our study aimed to identify complications/side effects of WALANT upper limb procedures through a systematic review and meta-analysis.
Methods
This PROSPERO-registered study was performed with strict adherence to PRISMA guidelines. Embase, OVIDMedline, Cochrane, Web of Science, and Scopus databases were searched until February 2023. Inclusion criteria involved English articles, reporting complications/side effects in primary WALANT upper limb surgeries. Outcomes included all complications and side effects, data on the anaesthetic mixture, publication year/location, study type, and procedures performed. The meta-analysis employed the Freeman-Tukey Double Arcsine Transformation, computed I2 statistics, and utilized common or random effects models for pooled analysis.
Results
2002 studies were identified; 79 studies met the inclusion criteria representing 15,595 WALANT patients. A total of 301 patients had complications, and the meta-analysis using a random effects model provided a complication rate of 1.7% (95% CI: 0.93–2.7%). The most reported complications were superficial infection (41%, n = 123/300), other/specified (12%, n = 37/300), and recurrent disease (6.7%, n = 20/300). A decade-by-decade analysis revealed no statistically significant difference in complication rates spanning the last three decades (p = 0.42). Adding sodium bicarbonate to the anaesthetic solution significantly reduced postoperative complications (p = 0.025).
Conclusion
WALANT has a low overall complication rate of 1.7%, with no significant temporal variation and a significant reduction in complications when sodium bicarbonate is added to the anaesthetic solution. Our findings support the safety of WALANT in upper limb procedures.
Registration
PROSPERO: CRD42023404018.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Healthcare systems are facing substantial challenges with increasing costs and a growing ageing population. In the USA, costs for healthcare soared over 500% in the past five decades, with the upward trend expected to persist [1]. As of 2022, the UK orthopaedic surgery waitlists surged to over 60,000 patients, up from 435 in January 2020 [2]. Wide-Awake Local Anaesthesia No Tourniquet (WALANT), as described by Lalonde, utilizes epinephrine and local anaesthetic mixtures for intra-operative injections, serving as an alternative to traditional anaesthesia [3]. This technique not only ensures effective pain control and anaesthesia but also promotes patient participation, which improves surgical outcomes [4,5,6].
Anesthetized patients endure a maximum tourniquet time of two h with inherent risks and limitations [7, 8]. However, WALANT eliminates tourniquet use in upper limb surgery, minimizing patient discomfort, easing resource burdens, and enhancing surgical care accessibility [9,10,11]. Surgeons have successfully utilized WALANT in diverse procedures, including skin flap surgery, joint replacements, upper and lower limb fracture fixations, and tendon transfers [12,13,14,15]. This technique proved crucial during the COVID-19 pandemic, preserving hospital resources and ensuring timely orthopaedic care [16,17,18,19,20,21,22,23,24].
However, its global adoption requires a thorough safety assessment. Presently, a lack of pooled data analysis from studies hinders the understanding of WALANT complications and side effects. This study aims to assess complications and side effects in upper limb procedures with the hypothesis that WALANT is a safe and effective technique, with a low complication rate.
Materials and methods
This PROSPERO-registered systematic review was conducted with strict adherence to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) [25]. The focus was studies reporting complications and side effects with the use of WALANT technique in upper limb surgeries.
Search strategy
Five online databases (Embase, OVIDMedline, Cochrane, Web of Science, and Scopus) were searched on 26 February 2023. All articles from inception till the search date were eligible for screening. Terms for the database search included: “walant”, “wide-awake”, “wide awake”, “wide awake no tourniquet”, “wide awake without tourniquet”, “walant”, “local anaesthetic no tourniquet”, “local anaesthetic without tourniquet” (Supplementary Fig. 1).
Inclusion criteria
Clinical studies that reported complications and/or side effects of the WALANT technique in primary upper limb surgeries performed in adults (> 18 years).
Exclusion criteria
Non-clinical studies, revision surgeries, case reports, conference abstracts, animal studies, cadaveric studies, technique studies, unpublished manuscripts, non–English language studies, paediatric patient population (< 18 years), and those not reporting postoperative complications/side effects.
Study screening
Two authors (JL, FB) performed an independent and blind title and abstract screening. For the full-text review phase, two authors screened the eligible articles independently and blindly, and any discrepancy was discussed with the senior author (EH) to reach a consensus.
Data extraction process and data items
Two authors extracted and summarized data from included articles independently, using Google Sheets (Google LLC, Mountain View, CA, USA). Data extracted were: demographics, study characteristics, follow-up period, comorbidities, local anaesthetic mixture, epinephrine dilution concentration, the use of added sodium bicarbonate, type of surgery, operative time, reoperation, conversion to general anaesthesia, and complications. The complications noted were infections, wound complications, nerve complications, and others. Infections were categorized into superficial and deep infections. Wound complications included delayed healing, wound dehiscence, and drainage. Nerve complications included digital nerve scarring and neuropraxia. Other complications included hematoma, finger necrosis, vascular injury, vasovagal response, development of complex regional pain syndrome, recurrent disease, tendon rupture, nonunion, lateral band subluxation, and unspecified.
Statistical methodology
Our comprehensive data analysis aggregated and analysed data synthesis from individual studies using R (version 4.2.0). To gauge the prevalence of complications across the spectrum of included studies, we used meta library package from R software for conducting meta-analysis of proportions. Notably, our dataset often featured proportions that approached zero or were exactly zero. In such instances, it is considered best practice to utilize the Freeman-Tukey Double Arcsine Transformation [26]. This statistical technique not only stabilizes variance but also substantially enhances the precision of the estimated confidence intervals. We computed the I2 statistic which quantifies the proportion of variation in the study outcomes that is due to true between-study differences rather than random error. An I2 greater than 50% was regarded as the presence of substantial heterogeneity, and the random effects model rather than the common effects model was reported in the result [27]. Additionally we also did meta-analysis using subgroups and constructed informative forest plots that facilitated a comparative analysis of complication rates across several crucial variables, including age, gender, study design, publication year, geographical region, follow-up duration, lidocaine concentration (1% or 2%), epinephrine concentration, use of sodium carbonate, and the specific surgical procedures undertaken (carpal tunnel release, trigger finger release, and flexor tendon repair).
Results
Overall complication rate and types of complications
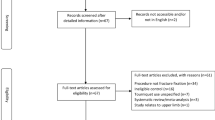
In our comprehensive analysis of 15,595 patients treated under WALANT, 79 studies were included in our analysis, as depicted in Fig. 1 PRISMA diagram [4, 9,10,11, 14,15,16, 19, 20, 28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97]. The meta-analysis using a random effect model indicates an overall complication rate of 1.7% (95% CI: 0.93–2.7%), as shown in Fig. 2. Of the complications reported, superficial infection was the most common (41%, n = 123/15,595) followed by other/unspecified (12%, n = 37/15,595), and wound dehiscence (7%, n = 20/15,595). Two studies reported nerve-related complications, in a total of four patients (0.02%). Three patients suffered complications following needle aponeurotomy for Dupuytren’s contracture (two neurapraxia, one permanent digital nerve injury), and the fourth was a transient painful neuroma following burn contracture release.

PRISMA flow chart

Forest plot of WALANT complication incidence
We observed only one case of permanent digital ischemia requiring partial amputation amongst 15,595 patients, with a detailed complication breakdown in Fig. 3. Furthermore, there exists a notable uniformity in the prevalence of complication rates across diverse procedures ranging from carpal tunnel release (CTR; 0.05%, 95% CI: 0.0–0.23%), trigger finger release (TFR; 0.49%, 95% CI: 0.0–1.9%), and flexor tendon repair (FTR; 1.2%, 95% CI: 0.0–6.9%) as depicted in Table 1, and Supplementary Figs. 2–4.

Breakdown of WALANT complications by type
A subsequent subanalysis, comparing elective procedures (CTR, TFR) to traumatic procedures (FTR), identified a significant difference in complication rates, with traumatic procedures showing a higher rate of complications (p = 0.036), as illustrated in Supplementary Fig. 5.
Complications over time
A decade-by-decade analysis of the studies included revealed no statistically significant difference in complication rates spanning the last three decades (p = 0.42; see Supplemental Fig. 6).
Study design and complications reported
When studies were grouped into retrospective and prospective study design groups, it was found that prospective studies reported statistically higher rates of complications as compared to retrospective studies (p = 0.033; see Supplemental Fig. 7).
Complication rate in relation to age
In a subgroup analysis that classified included studies by mean age of participants into three age groups: < 45, 45–65, and > 65 years, encompassing 20, 30, and 7 studies, respectively, no statistically significant differences in complication rates were noted (p = 0.58). The forest plot is available in Supplemental Fig. 8.
Geographical distribution of publications and complications
The 79 studies included in this review originated from 26 countries. Most publications (32%) were from Europe, followed by North America (30%) and Asia with publications at 29%. Aside from Australia and Antarctica, all continents were represented. Figure 4 displays the global distribution of included studies, whilst Supplementary Fig. 9 depicts the meta-analysis.

Geographic variation in publication density and complication prevalence: a random effects meta-analysis
Correlation of anaesthetic mixture and complication rate
All studies reported using anaesthetic mixtures within the accepted dosage (7 mg/kg lidocaine), and as tumescent (subcutaneous) anaesthesia. Studies on WALANT and fracture surgery (no = 26) additionally added anaesthesia in the periosteal areas where fracture fixation was planned. Amongst 49 studies reporting the exact anaesthetic mixtures, 28 used sodium bicarbonate (NaHCO3; 8.4% concentration) with the anaesthetic solution, at a ratio of 1 cc NaHCO3:10 cc lidocaine solution. The addition of NaHCO3 was found to reduce overall complications, with a 0.53%, 95% CI: 0.12–1.1% complication rate compared to 1.3%, 95% CI: 0.12–2.1% in solutions without NaHCO3, a statistically significant difference (p = 0.025). Of the included studies, 60 reported the concentration of epinephrine, and 49 out of these 60 studies used 1% lidocaine instead of 2%. Notably, no significant difference in complication prevalence was observed between the various lidocaine concentrations (p = 0.23). Additionally, grouping the concertation of epinephrine into low (> 100,000), medium (1:1000–1:100,000), and high (< 1:1000) revealed no statistically significant complications between the groups (p = 0·23). Table 2 provides detailed anaesthetic mixture components and combined complication rates, whilst Supplemental Figs. 10, 11, and 12 display meta-analysis forest plots of sodium bicarbonate, lidocaine concentration, and epinephrine concentration, respectively.
Discussion
This systematic review and meta-analysis, encompassing 15,595 patients from 79 publications, presents the global patient demographic profile for WALANT-based hand and upper limb surgeries. The findings support the safety of WALANT in both emergency and elective procedures. Importantly, the study identifies a significant association between WALANT mixtures containing sodium bicarbonate and a reduced risk of complications, providing evidence for the safety of WALANT in upper limb surgeries.
Prior research, such as Lipira et al.’s study of over 10,000 hand surgery cases, reported a 2.5% complication rate within the first month post-surgery, mainly under general anaesthesia [98]. Another recent review of 59,040 hand surgery procedures also found superficial wound infection as the most common complication, with a prevalence of less than 1% [99]. This is equivalent to our analysis, where superficial wound infection was the most common complication (52% of complications found, < 1% of the total number of cases). Additionally, only a single instance of irreversible necrosis was observed. This unique occurrence involved necrosis of the digit tip, which resulted from a crush injury to the distal phalanx and was treated with Kirschner wire fixation [88]. This isolated incident mitigates the initial concern of epinephrine-induced digital necrosis.
In our meta-analysis, we examined the association between WALANT solution components and complication prevalence, as a higher lidocaine concentration is at times used to enhance the anaesthetic effect but carries with it the disadvantage of higher toxicity. The addition of sodium bicarbonate has been shown to give 1% lidocaine solution an anaesthetic effect that is equivalent to that of 2% lidocaine solution whilst reducing the risk of anaesthetic toxicity [100, 101]. The primary use of sodium bicarbonate is to reduce the pain of injections by neutralizing the pH value of the injected solution, and double-blinded trials have proven that this is the case [102]. We found no difference in complication rates between 1 and 2% lidocaine solutions, but a significant difference if the lidocaine was buffered with sodium bicarbonate. In acute wound healing, as after a surgical procedure, a neutral pH has been found to optimize protease activity and cell migration, thus enhancing the potential of wound healing [103]. Given that wound healing complications were the most common in our systematic review of WALANT surgery, we recommend adding sodium bicarbonate. This addition helps lower injection pain, enhances lidocaine’s anaesthetic effect, and reduces the risk of both lidocaine toxicity and postoperative complications.
In our analysis of three common hand procedures—CTR, TFR, and FTR—we observed a complication rate of 0.05% for CTR. Notably, the largest study to date, a national cohort analysis of over 850,000 CTR cases, reported a similar overall complication rate of around 0.1% [104]. For TFR, reported complication rates vary widely, ranging from 1 to 43% [105,106,107,108,109]. Everding et al. found a complication rate of 12% in their review of 795 TFR, and another retrospective review of 3428 patients reported a rate of 16% of complications [110, 111]. Kardestuncer et al., in their review of 527 fingers that underwent trigger release under local anaesthesia without using epinephrine, found a complication rate of 6.3% [112]. In our systematic review, we report a 0.5% rate which is low in comparison to all previous studies and thus adds to the strength and safety of using WALANT.
Amongst traumatic hand surgery procedures, FTR is one of the most common, and whilst our subanalysis indicated a significantly higher complication prevalence for traumatic procedures (FTR) under WALANT compared to elective procedures (CTR, TFR) (p = 0.036), our review revealed a notably low complication rate of 1.2%. In comparison, a comprehensive review of 39 studies (3800 cases) showed a 4–6% complication rate, including reoperations, adhesions, and ruptures [113]. This favourable outcome may be attributed to the unique ability to intraoperatively test suture strength and motion, thus underscoring the continued viability of WALANT for traumatic hand surgeries. Therefore, despite the higher complication prevalence in traumatic procedures with WALANT compared to elective ones, WALANT should still be considered for traumatic hand surgeries, as it results in a lower prevalence of complications than what is typically reported in the literature without WALANT, likely due to the active intraoperative testing of suture strength and motion.
WALANT, in addition to its safety, offers a distinct advantage by facilitating direct surgeon–patient interaction and intra-operative assessment of functional. With the patient fully awake and cooperative, intraoperative motion control can be assessed without a tourniquet, which is particularly beneficial in tendon repair and transfers. This dynamic engagement allows for immediate feedback, crucial adjustments, and contributes to superior surgical outcomes, precision, functional recovery, and heightened patient satisfaction [5, 114,115,116,117].
Most of the included studies originated in the USA, akin to most of the published literature in orthopaedics [118,119,120].This can be attributed to the high research activity in the USA, in addition to the overall high health expenditure [118]. However, a closer look at the studies’ geographical distribution demonstrated that Europe was the primary source with 25 publications, followed by North America with 24, and Asia with 23 publications. This trend might reflect the cost-effectiveness and relative accessibility of WALANT. Seven countries (USA, Malaysia, France, Korea, UK, Canada, and Taiwan) contributed to 65% of the total publications. Most of the studies (71%) were published between 2020 and 2023. This surge can be explained by a general dramatic increase in publications during the COVID-19 pandemic [121]. In contrast, only 25% of the publications were published between 2010 and 2019, and only 4% before 2009, reflecting the increase in WALANT utilization over the last 20 years. This temporal pattern also underscores the steady increase in WALANT across the globe.
WALANT offers a cost-effective approach to delivering surgical care by eliminating the need for an anesthesiologist and the expenses related to anaesthetic drugs, monitoring equipment, pre-operative evaluations, and post-anaesthesia care. This accessibility expands the reach of surgical interventions to a wider population whilst sparing operating room and anaesthesia-related costs [22,23,24, 81]. By requiring fewer personnel and being suitable for office-based procedures, WALANT facilitates the timely delivery of surgical care in remote or resource-limited regions. This has the potential to bridge healthcare gaps by reaching underserved areas globally.
In the context of sustainability, the increasing problem of surgical waste presents environmental challenges. Addressing this concern is possible through alternative surgical techniques. One effective approach involves minimizing the use of general anaesthesia and its associated disposables, leading to a substantial reduction in surgical waste generation [122]. According to a recent global survey involving 876 hand surgeons, over 50% identified WALANT as a key factor in making their surgical practices more sustainable [123]. Incorporating WALANT into office-based settings enhances sustainable practices in surgery.
This study concludes that WALANT is a remarkably safe technique with a low complication rate. The success of WALANT in upper limb surgery has led to its application across diverse surgical procedures highlighting its versatility and potential to revolutionize surgical care [124,125,126]. Our analysis of WALANT provides evidence for its adoption in our in upper limb and hand practice, inspiring consideration by other surgical specialties and proposing WALANT as a potentially effective model for providing care in resource-constrained areas. Based on these findings, healthcare administrators and professionals are urged to recognize the transformative potential of the WALANT technique in upper limb procedures. Its noteworthy combination of low complication rates, cost-effectiveness, and high adaptability can catalyse a transformative shift in orthopaedic and plastic surgery.
We noticed outlier studies with significantly higher complication rates, likely stemming from complex procedures including digit replantation [94], stage four Dupuytren contracture [41, 43], extensor central slip tenotomy for chronic mallet finger [30], and flexor tendon repair [91] during our analysis.
Limitation
This research study is not without its inherent limitations, which should be considered when interpreting the findings. It is important to acknowledge that the studies included in this analysis did not uniformly investigate the same complications but rather all complications reported. This heterogeneity in the outcomes assessed across the selected studies can introduce variability in the data and impact the generalizability of our findings. Moreover, the included studies exhibited discrepancies in follow-up periods, study designs, and WALANT solution concentration or mixtures, and were conducted by different surgeons within diverse patient populations, each presenting unique medical conditions. Based on the meta-analysis performed the levels of heterogeneity were always substantial (I2 > 50%) in most of the subgroup analysis, and random effects models were reported.
Moreover, subgroup analyses were performed whenever possible to discern potential patterns or trends within the data. Therefore, the findings of this study should be interpreted with a recognition of the above limitations. The number of included studies with large sample sizes and representation from various regions in the world adds strength to this systematic r.
Data Availability
Data supporting this study are included within the article and/or supporting materials.
References
Kurani N, Ortaliza J, Wager E, Fox L, Amin K. How has U.S. (2022) Spending on healthcare changed over time? Peterson-KFF health system tracker. https://www.healthsystemtracker.org/chart-collection/u-s-spending-healthcare-changed-time/#Total%20national%20health%20expenditures,%20US%20$%20Billions,%201970-2022
British Orthopedic Association (2022) T&O waiting list the largest for over a decade. https://www.boa.ac.uk/resource/t-o-waiting-list-the-largest-for-over-a-decade.html.
Lalonde D, Martin A (2013) Epinephrine in local anesthesia in finger and hand surgery: the case for wide-awake anesthesia. J Am Acad Orthop Surg 21(8):443–447. https://doi.org/10.5435/JAAOS-21-08-443
Okamura A, Moraes VY, Fernandes M, Raduan-Neto J, Belloti JC (2021) WALANT versus intravenous regional anesthesia for carpal tunnel syndrome: a randomized clinical trial. Sao Paulo Medical Journal Revista Paulista de Medicina 139(6):576–578
Ayhan E, Akaslan F (2020) Patients’ perspective on carpal tunnel release with WALANT or intravenous regional anesthesia. Plast Reconstr Surg 145(5):1197–1203. https://doi.org/10.1097/PRS.0000000000006741
Moscato L, Helmi A, Kouyoumdjian P, Lalonde D, Mares O (2023) The impact of WALANT anesthesia and office-based settings on patient satisfaction after carpal tunnel release: a patient reported outcome study. Orthopaedics & Traumatol, Surgery Res: OTSR 109(3):103134. https://doi.org/10.1016/j.otsr.2021.103134
Stimpson J, Gill DF, Memarzadeh A, Dunne M, Perry L, Magan A, Devany A, Pasapula C (2019) Reducing the hypertensive effects of the prolonged surgical tourniquet using a dual-cuff strategy: a prospective randomized controlled trial. The J Foot Ankle Surg 58(6):1177–1186. https://doi.org/10.1053/j.jfas.2019.03.019
Pedowitz RA, Gershuni DH, Schmidt AH, Fridén J, Rydevik BL, Hargens AR (1991) Muscle injury induced beneath and distal to a pneumatic tourniquet: a quantitative animal study of effects of tourniquet pressure and duration. The J Hand Surg 16(4):610–621. https://doi.org/10.1016/0363-5023(91)90183-c
Oakes TC, Wong KC, Schank KJ, Haan P, Bray SM, Clarkson JHW (2022) Infection rate comparison during transition from hospital to office WALANT enabled by virtual reality. Plast Reconstr Surg Glob Open 10(5):e4285. https://doi.org/10.1097/GOX.0000000000004285
Abd Hamid MH, Abdullah S, Ahmad AA, Narin Singh PSG, Soh EZF, Liu CY, Sapuan J (2021) A randomized controlled trial comparing wide-awake local anesthesia with no tourniquet (WALANT) to general anesthesia in plating of distal radius fractures with pain and anxiety level perception. Cureus 13(1):e12876. https://doi.org/10.7759/cureus.12876
Far-Riera AM, Perez-Uribarri C, Serrano MJE, González JMR (2022) Impact of WALANT hand surgery in a secondary care hospital in Spain Benefits to the patient and the health system. J Hand Surg Global Online 5(1):73–79
Apard T, Odoemene M, Descamps J (2022) Wrist hemiarthroplasty of irreparable distal radius fracture under wide-awake local anesthetic and no tourniquet. Life (Basel, Switzerland) 12(10):1624. https://doi.org/10.3390/life12101624
Tahir M, Chaudhry EA, Zaffar Z, Anwar K, Mamoon MAH, Ahmad M, Jamali AR, Mehboob G (2020) Fixation of distal radius fractures using wide-awake local anaesthesia with no tourniquet (WALANT) technique: a randomized control trial of a cost-effective and resource-friendly procedure. Bone & Joint Res 9(7):429–439. https://doi.org/10.1302/2046-3758.97.BJR-2019-0315.R1
Xu J, Yin L, Cao S, Zhan H, Zhang J, Zhou Q, Gong K (2021) Application of WALANT technique for repairing finger skin defect with a random skin flap. J Orthop Surg Res 16(1):164. https://doi.org/10.1186/s13018-021-02319-3
Higgins A, Lalonde DH, Bell M, McKee D, Lalonde JF (2010) Avoiding flexor tendon repair rupture with intraoperative total active movement examination. Plast Reconstr Surg 126(3):941–945. https://doi.org/10.1097/PRS.0b013e3181e60489
Georgieva G, Srbov B, Nikolovska B, Tusheva S, Jovanovska K, Jovanoski T, Dzonov B, Gjorgova ST, Pejkova S (2022) WALANT as an optimal approach in hand surgery during pandemics. Prague Med Report 123(2):88–94. https://doi.org/10.14712/23362936.2022.9
Sutcliffe A, Khera B, Khashaba H (2022) Wide-awake local anaesthesia no tourniquet (WALANT) procedures during COVID: a single centre experience. Acta bio-medica : Atenei Parmensis 93(1):e2022013. https://doi.org/10.23750/abm.v93i1.12134
Bamal R, Alnobani O, Bastouros E, Nolan G, Morris E, Griffiths S, Bell D (2023) Wide-awake local anesthesia no tourniquet (WALANT) for flexor tendon repairs as change in practice during the COVID-19 pandemic: a retrospective cohort study with outcomes. Cureus 15(3):e36728. https://doi.org/10.7759/cureus.36728
Ruterana P, Abitbol A, Castel LC, Gregory T (2022) WALANT technique versus locoregional anesthesia in the surgical management of metacarpal and phalangeal fractures: Lessons from the Covid-19 crisis. Hand Surg Rehabilitation 41(2):220–225. https://doi.org/10.1016/j.hansur.2021.12.002
Turcotte JJ, Petre BM, Jones CM, Gelfand JM (2020) Maintaining access to orthopaedic surgery during periods of operating room resource constraint: expanded use of wide-awake surgery during the COVID-19 pandemic. J Am Acad Orthop Surgeons Global Res Rev 4(12):e20.00100. https://doi.org/10.5435/JAAOSGlobal-D-20-00100
Turcotte JJ, Gelfand JM, Jones CM, Jackson RS (2021) Development of a low-resource operating room and a wide-awake orthopedic surgery program during the COVID-19 pandemic. Surgical Innov 28(2):183–188. https://doi.org/10.1177/15533506211003530
Clark DM, Dingle ME, Wade SM, Mescher PK, Nanos GP 3rd, Tintle SM (2023) Utilization of a clinic-based hand surgery procedure room in the US Military Health System: a performance improvement analysis of resource savings and patient satisfaction. J Hand Surg Am S0363-5023(23)00165-X. https://doi.org/10.1016/j.jhsa.2023.03.014
Maliha SG, Cohen O, Jacoby A, Sharma S (2019) A cost and efficiency analysis of the WALANT technique for the management of trigger finger in a procedure room of a major city hospital. Plast Reconstr Surg Glob Open 7(11):e2509. https://doi.org/10.1097/GOX.0000000000002509
Long CW, Wilson A, Daniels CL, Brown ME, Carreon L, Robinson L (2022) Improved resource utilization using WALANT hand surgery in sdolescents. Hand (N Y). https://doi.org/10.1177/15589447221126764
Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group (2010) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Int J Surg (London, England) 8(5):336–341. https://doi.org/10.1016/j.ijsu.2010.02.007
Doi SA, Xu C (2021) The Freeman-Tukey double arcsine transformation for the meta-analysis of proportions: recent criticisms were seriously misleading. J Evid Based Med 14(4):259–261. https://doi.org/10.1111/jebm.12445
Higgins JP, Thompson SG, Deeks JJ, Altman DG (2003) Measuring inconsistency in meta-analyses BMJ (Clinical research ed) 327(7414):557–560. https://doi.org/10.1136/bmj.327.7414.557
Abdullah S, Tokiran MF, Ahmad AA, Soh EZF, Makpol S, Sapuan J (2023) Safety of lidocaine during wide-awake local anesthesia no tourniquet for distal radius plating. J Hand Surg Global Online 5(2):196–200. https://doi.org/10.1016/j.jhsg.2022.12.003
Abitbol A, Merlini L, Masmejean EH, Gregory T (2021) Applying the WALANT technique to surgical treatment of distal radius fractures. Hand Surg Rehab 40(3):277–282. https://doi.org/10.1016/j.hansur.2021.02.001
Apard T, Candelier G (2017) Wide-awake ultrasound-guided percutaneous extensor central slip tenotomy for chronic mallet finger: a prospective study of 14 cases (with videos). Hand Surg Rehab 36(2):86–89. https://doi.org/10.1016/j.hansur.2016.12.006
Apard T, Mares O, Duparc F, Michelin P (2022) Percutaneous Ultrasound-guided release of the lacertus fibrosus for median nerve entrapment at the elbow. Cardiovasc Intervent Radiol 45(8):1198–1202. https://doi.org/10.1007/s00270-022-03123-0
Avoricani A, Dar QA, Levy KH, Koehler SM (2021) WALANT hand surgery: do the AORN guidelines apply? J Surg Orthop Adv 30(3):156–160
Avoricani A, Dar QA, Levy KH, Kurtzman JS, Koehler SM (2022) WALANT hand and upper extremity procedures performed with minor field sterility are associated with low infection rates. Plastic surgery (Oakville, Ont) 30(2):122–129. https://doi.org/10.1177/22925503211003840
Bas CE, Ayhan E, Kunu O, Kuru CA (2022) Successful boutonniere reconstruction with wide-awake local anesthesia no tourniquet. J Hand Surg Global Online 4(6):421–425. https://doi.org/10.1016/j.jhsg.2022.05.001
Bashir MM, Qayyum R, Saleem MH, Siddique K, Khan FA (2015) Effect of time interval between tumescent local anesthesia infiltration and start of surgery on operative field visibility in hand surgery without tourniquet. The J Hand Surg 40(8):1606–1609. https://doi.org/10.1016/j.jhsa.2015.03.034
Boukebous B, Maillot C, Castel LC, Donadio J, Boyer P, Rousseau MA (2023) Wide awake local anesthesia no tourniquet (WALANT) versus axillary brachial plexus block for carpal tunnel release in a French public university hospital: care pathways and operating room costs. Orthopaedics & Traumatol Surg Res: OTSR 109(3):103358. https://doi.org/10.1016/j.otsr.2022.103358
Braza ME, Kelley JP, Kelpin JP, Fahrenkopf MP, Do VH (2023) Treatment of pyogenic flexor tenosynovitis in the emergency department setting with WALANT technique. Hand (New York, N.Y) 18(3):473–477. https://doi.org/10.1177/15589447211030695
Castro Magtoto IJ, Alagar DL (2019) Wide awake local anesthesia no tourniquet: a pilot study for carpal tunnel release in the Philippine Orthopedic Center. The J Hand Surg Asian-Pacific 24(4):389–391. https://doi.org/10.1142/S2424835519500486
Chowdhry S, Seidenstricker L, Cooney DS, Hazani R, Wilhelmi BJ (2010) Do not use epinephrine in digital blocks: myth or truth? Part II A retrospective review of 1111 cases. Plastic Reconstructive Surg 126(6):2031–2034
Ciobanu P, Poroch V, Moraru DC, Velenciuc N, Aladari N (2021) Wide awake local anesthesia no tourniquet technique in hand surgery during the COVID-19 pandemic—personal experience. Medical-Surgical Journal-Revista Medico-Chirurgicala 125(3):386–394
Denkler K (2005) Dupuytren’s fasciectomies in 60 consecutive digits using lidocaine with epinephrine and no tourniquet. Plast Reconstr Surg 115(3):802–810. https://doi.org/10.1097/01.prs.0000152420.64842.b6
Denkler KA (2011) Needle fasciotomy for stage IV Dupuytren’s: a wide-awake approach—level 4 evidence. J Hand Surg 36(8):15–16
Denkler KA, Park KM (2022) Needle aponeurotomy for stage IV Dupuytren contracture: a wide-awake first step approach in 204 consecutive rays. Plast Reconstr Surg 150(5):1033e–1036e. https://doi.org/10.1097/PRS.0000000000009641
Dukan R, Krief E, Nizard R (2020) Distal radius fracture volar locking plate osteosynthesis using wide-awake local anaesthesia. The Journal of hand surgery, European 45(8):857–863. https://doi.org/10.1177/1753193420916418
Duru Ç, Yaşar B, Ergani HM, Acicbe O, Utku Ö, Ünlü RE (2023) Outcomes of wide-awake flexor tendon repairs in 58 fingers and 9 thumbs. The Journal of hand surgery 48(7):734.e1-734.e8. https://doi.org/10.1016/j.jhsa.2022.01.015
Enechukwu AOM, Bucher F, Dastagir K, Jokuszies A, Vogt PM, Könneker S (2021) Treatment of hand infections using WALANT -when the anesthesiologist is not available: a retrospective cohort study. Ann Med Surg (Lond) 71:102993. https://doi.org/10.1016/j.amsu.2021.102993
Farkash U, Herman A, Kalimian T, Segal O, Cohen A, Laish-Farkash A (2020) Keeping the finger on the pulse: cardiac arrhythmias in hand surgery using local anesthesia with adrenaline. Plast Reconstr Surg 146(1):54e–60e. https://doi.org/10.1097/PRS.0000000000006902
Farzam R, Deilami M, Jalili S, Kamali K (2021) Comparison of anesthesia results between wide awake local anesthesia no tourniquet (WALANT) and forearm tourniquet bier block in hand surgeries: a randomized clinical trial. The Arch Bone Joint Surg 9(1):116–121
Gunasagaran J, Sean ES, Shivdas S, Amir S, Ahmad TS (2017) Perceived comfort during minor hand surgeries with wide awake local anaesthesia no tourniquet (WALANT) versus local anaesthesia (LA)/tourniquet. J Orthop Surg (Hong Kong) 25(3):2309499017739499. https://doi.org/10.1177/2309499017739499
Hernandez A, Rosario M, Mendoza-Torres R, Taguba CRM, Garcia A, Battad G (2020) Evaluating clinical outcomes for determining the optimal delay to skin incision under WALANT: a prospective series of 34 patients from a low-resource tertiary setting. Adv Orthop 2020:9351354. https://doi.org/10.1155/2020/9351354
Hong J, Kang HJ, Whang JI, Sung SY, Kim SH, Shin SC, Kim SN, Kim JS (2020) Comparison of the wide-awake approach and conventional approach in extensor indicis proprius-to-extensor pollicis longus tendon transfer for chronic extensor pollicis longus rupture. Plast Reconstr Surg 145(3):723–733. https://doi.org/10.1097/PRS.0000000000006611
How HM, Khoo BLJ, Ayeop MAS, Ahmad AR, Bahaudin N, Ahmad AA (2022) Application of WALANT in diaphyseal plating of forearm fractures: an observational study. J Hand Surg Global Online 4(6):399–407. https://doi.org/10.1016/j.jhsg.2022.02.004
Huang YC, Chen CY, Lin KC, Yang SW, Tarng YW, Chang WN (2019) Comparison of wide-awake local anesthesia no tourniquet with general anesthesia with tourniquet for volar plating of distal radius fracture. Orthopedics 42(1):e93–e98. https://doi.org/10.3928/01477447-20181206-01
Huang YC, Hsu CJ, Renn JH, Lin KC, Yang SW, Tarng YW, Chang WN, Chen CY (2018) WALANT for distal radius fracture: open reduction with plating fixation via wide-awake local anesthesia with no tourniquet. J Orthop Surg Res 13(1):195. https://doi.org/10.1186/s13018-018-0903-1
Kadhum M, Georgiou A, Kanapathy M, Reissis D, Akhavani M, Burr N, Nikkhah D (2022) Operative outcomes for wide awake local anesthesia versus regional and general anesthesia for flexor tendon repair. Hand Surg Rehabilitation 41(1):125–130. https://doi.org/10.1016/j.hansur.2021.10.312
Kafiabadi MJ, Sabaghzadeh A, Biglari F, Sadighi M, Ebrahimpour A (2023) Effects of fixation of clavicle fracture using wide-awake local anesthesia no tourniquet (WALANT) technique on intra-operative bleeding volume, surgical duration, and post-operatively visual analog scale (VAS). A Case Series Study Injury 54(2):557–560. https://doi.org/10.1016/j.injury.2022.11.063
Kang SW, Park HM, Park JK, Jeong HS, Cha JK, Go BS, Min KT (2019) Open cubital and carpal tunnel release using wide-awake technique: reduction of postoperative pain. J Pain Res 12:2725–2731. https://doi.org/10.2147/JPR.S210366
Ki Lee S, Gul Kim S, Sik Choy W (2020) A randomized controlled trial of minor hand surgeries comparing wide awake local anesthesia no tourniquet and local anesthesia with tourniquet. Orthopaedics & Traumatol Surg Res: OTSR 106(8):1645–1651. https://doi.org/10.1016/j.otsr.2020.03.013
Lalchandani GR, Halvorson RT, Rahgozar P, Immerman I (2019) Wide-awake local anesthesia for minor hand surgery associated with lower opioid prescriptions, morbidity, and costs: a nationwide database study. Journal of Hand Surg Global Online 2(1):7–12. https://doi.org/10.1016/j.jhsg.2019.09.011
Larsen LP, Hansen TB (2021) Total trapeziometacarpal joint arthroplasty using wide awake local anaesthetic no tourniquet. The J Hand Surg Europ 46(2):125–130. https://doi.org/10.1177/1753193420932465
Lee S, Oh S, Son D (2020) Open carpal release using local anesthesia without a tourniquet: does bleeding tendency affect the outcome? Arch Plast Surg 47(6):597–603. https://doi.org/10.5999/aps.2020.01732
Lee SK, Kim SG, Kim H, Choy WS (2023) Carpal tunnel release under wide awake local anesthesia with no tourniquet in hemodialysis patients with arteriovenous shunt. Orthopaedics & Traumatol Surg Res: OTSR 109(3):103413. https://doi.org/10.1016/j.otsr.2022.103413
Lin YC, Chen WC, Chen CY, Kuo SM (2021) Plate osteosynthesis of single metacarpal fracture: WALANT technique is a cost-effective approach to reduce postoperative pain and discomfort in contrast to general anesthesia and wrist block. BMC Surg 21(1):358. https://doi.org/10.1186/s12893-021-01362-5
Liu WC, Lu IC, Chang CC, Chen CT, Chen CH, Shih CL, Fu YC, Jupiter JB (2022) Less fluctuation in hemodynamics of the wide-awake local anesthesia no tourniquet technique than general anesthesia in distal radius plating surgery: a prospective case-control study. J Clin Med 11(4):1123. https://doi.org/10.3390/jcm11041123
Luciani P, Delgove A, Pelissier P (2022) Retrospective evaluation of WALANT in emergency hand surgery in the Bordeaux university hospital. Hand Surg Rehabilitation 41(4):435–440. https://doi.org/10.1016/j.hansur.2022.03.003
Ly TV, Urban V, Meuli-Simmen C, Pasternak I (2019) Endoscopic carpal tunnel release using wide-awake anesthesia. J Hand Surg Global Online 2(1):13–15. https://doi.org/10.1016/j.jhsg.2019.10.005
McKnight KN, Smith VJS, MacFadden LN, Chong ACM, Van Demark RE, Jr (2022) Wide-Awake Hand Surgery Has Its Benefits: A Study of 1,011 Patients. J Hand Surg Glob Online 4(6):394–398. https://doi.org/10.1016/j.jhsg.2022.05.008
Meunier V, Mares O, Gricourt Y, Simon N, Kouyoumdjian P, Cuvillon P (2022) Patient satisfaction after distal upper limb surgery under WALANT versus axillary block: a propensity-matched comparative cohort study. Hand Surg Rehabilitation 41(5):576–581. https://doi.org/10.1016/j.hansur.2022.06.005
Mohd Rashid MZ, Sapuan J, Abdullah S (2019) A randomized controlled trial of trigger finger release under digital anesthesia with (WALANT) and without adrenaline. J Orthop Surg (Hong Kong) 27(1):2309499019833002. https://doi.org/10.1177/2309499019833002
Moog P, Dozan M, Betzl J, Sukhova I, Kükrek H, Megerle K (2021) WALANT-epinephrine injection may lead to short term, reversible episodes of critical oxygen saturation in the fingertips. Arch Orthop Trauma Surg 141(3):527–533. https://doi.org/10.1007/s00402-020-03744-5
Naude JJ, Koch O, Schmidt LW, le Roux TLB (2021) Positive patient experience of Wide Awake Local Anaesthesia No Tourniquet (WALANT) hand surgery in the government setting: a prospective descriptive study. SA Orthopaedic J 20(3):141–146. https://doi.org/10.17159/2309-8309/2021/v20n3a1
Nelson R, Higgins A, Conrad J, Bell M, Lalonde D (2010) The wide-awake approach to Dupuytren’s disease: fasciectomy under local anesthetic with epinephrine. Hand (New York N.Y) 5(2):117–124. https://doi.org/10.1007/s11552-009-9239-y
Noureddine H, Vejsbjerg K, Harrop JE, White MJ, Chakravarthy J, Harrison JWK (2020) Fasciectomy under local anaesthetic and adrenaline for Dupuytren's contracture in a community setting in the UK with a cost analysis. Bone Joint J 102-B(10), 1354-1358. https://doi.org/10.1302/0301-620X.102B10.BJJ-2019-1685.R2
Orbach H, Rozen N, Rubin G (2018) Open reduction and internal fixation of intra-articular distal radius fractures under wide-awake local anesthesia with no tourniquet. J Int Med Res 46(10):4269–4276. https://doi.org/10.1177/0300060518793036
Öztürk İA, Öztürk K, Orman O, Baydar M, Aykut S, Köse A (2018) Comparison of the cost and efficacy of axillary anesthesia and wide-awake anesthesia in finger surgeries. Sisli Etfal Hastanesi tip bulteni 52(2):119–123. https://doi.org/10.14744/SEMB.2017.17363
Pertea M, Grosu OM, Veliceasa B, Velenciuc N, Ciobanu P, Tudor R, Poroch V, Lunca S (2019) Effectiveness and safety of wide awake local anesthesia no tourniquet (WALANT) technique in hand surgery. Revista de Chimie 70(10):3587–3591. https://doi.org/10.37358/RC.19.10.7602
Poggetti A, Nucci AM, Giesen T, Calcagni M, Marchetti S, Lisanti M (2018) Percutaneous intramedullary headless screw fixation and wide-awake anesthesia to treat metacarpal fractures: early results in 25 patients. J Hand Microsurg 10(1):16–21. https://doi.org/10.1055/s-0037-1618911
Prénaud C, Merlini L, Hurst SA, Gregory T, Dacheux C (2022) A study of hand flap viability when using a wide awake local anesthesia no tourniquet (WALANT) technique. J Hand Microsurg 15(4):270–274. https://doi.org/10.1055/s-0042-1742456
Rellán I, Bronenberg Victorica P, Kohan Fortuna Figueira SV, Donndorff AG, De Carli P, Boretto JG (2023) What is the infection rate of carpal tunnel syndrome and trigger finger release performed under wide-awake anesthesia? Hand (N Y) 18(2):198–202. https://doi.org/10.1177/1558944721994262
Reynolds M, Srinivasan RC, Person DW (2022) Complications after clinic-based wide awake local anesthesia no tourniquet hand surgery at a single private practice. Hand (New York N.Y) 17(5):865–868. https://doi.org/10.1177/1558944720975132
Rhee PC, Fischer MM, Rhee LS, McMillan H, Johnson AE (2017) Cost savings and patient experiences of a clinic-based, wide-awake hand surgery program at a military medical center: a critical analysis of the first 100 procedures. The J Hand Surg 42(3):e139–e147. https://doi.org/10.1016/j.jhsa.2016.11.019
Ruxasagulwong S, Kraisarin J, Sananpanich K (2015) Wide awake technique versus local anesthesia with tourniquet application for minor orthopedic hand surgery: a prospective clinical trial. J Med Ass Thailand Chotmaihet Thangphaet 98(1):106–110
Saleh E, Saleh J, Govshievich A, Ferland-Caron G, Lin JC, Tremblay DM (2021) Comparing minor hand procedures performed with or without the use of a tourniquet: a randomized controlled trial. Plast Reconstr Surg Glob Open 9(4):e3513. https://doi.org/10.1097/GOX.0000000000003513
Sasor SE, Cook JA, Duquette SP, Lucich EA, Cohen AC, Wooden WA, Tholpady SS, Chu MW (2020) Tourniquet use in wide-awake carpal tunnel release. Hand (New York N.Y) 15(1):59–63. https://doi.org/10.1177/1558944718787853
Schindelar L, Townsend CB, Ilyas AM, Matzon JL (2022) The impact of intraoperative nursing care on perioperative complications during wide-awake local anesthesia hand surgery. J Hand Surg Global Online 4(6):385–388. https://doi.org/10.1016/j.jhsg.2021.12.006
Sharma S, Ong J, Putti A (2023) Proximal interphalangeal joint arthroplasty using the wide-awake local anesthesia no tourniquet technique. Hand (New York, N.Y) 18(4):612–615. https://doi.org/10.1177/15589447211063545
Sraj S (2021) Carpal tunnel release with wide awake local anesthesia and no tourniquet: with versus without epinephrine. Hand (New York NY) 16(5):592–594. https://doi.org/10.1177/1558944719890038
Steve AK, Shine JJ, Yakaback S, Matthews JL, Yeung J (2022) Low infection rate for hand fractures managed with surgical fixation under wide-awake local anesthesia with no tourniquet in minor surgery. Plast Reconstr Surg 150(4):829–833. https://doi.org/10.1097/PRS.0000000000009542
Tahir M, Mehboob G, R Jamali A, Phillips AM (2020) Use of the wide-awake local anaesthetic no tourniquet in the management of distal radius fractures. J Pak Med Assoc 70(Suppl 1) (2):S42–S48
Teo I, Lam W, Muthayya P, Steele K, Alexander S, Miller G (2013) Patients’ perspective of wide-awake hand surgery—100 consecutive cases. The J Hand Surg Europ 38(9):992–999. https://doi.org/10.1177/1753193412475241
Townsend CB, Henry TW, Matzon JL, Seigerman D, Sodha SC, Beredjiklian PK (2023) Functional outcomes of flexor tendon repair in the fingers: a comparison of wide-awake local anesthesia no tourniquet versus traditional anesthesia. Hand (New York, N.Y) 18(4):635–640. https://doi.org/10.1177/15589447211064364
Wellington I, Cusano A, Ferreira JV, Parrino A (2023) WALANT technique versus sedation for endoscopic carpal tunnel release. Hand (New York N.Y) 18(2):214–221. https://doi.org/10.1177/15589447211003180
Wilhelmi BJ, Blackwell SJ, Miller JH, Mancoll JS, Dardano T, Tran A, Phillips LG (2001) Do not use epinephrine in digital blocks: myth or truth? Plast Reconstr Surg 107(2):393–397. https://doi.org/10.1097/00006534-200102000-00014
Wong J, Lin CH, Chang NJ, Chen HC, Lin YT, Hsu CC (2017) Digital revascularization and replantation using the wide-awake hand surgery technique. The J Hand Surg Europ 42(6):621–625. https://doi.org/10.1177/1753193417703516
Xing SG, Tang JB (2019) Extending applications of local anesthesia without tourniquet to flap harvest and transfer in the hand. Hand Clin 35(1):97–102. https://doi.org/10.1016/j.hcl.2018.08.009
Yen CY, Ma CH, Wu CH, Yang SC, Jou IM, Tu YK (2020) A cost and efficacy analysis of performing arthroscopic excision of wrist ganglions under wide-awake anaesthesia versus general anaesthesia. BMC Musculoskelet Disord 21(1):459. https://doi.org/10.1186/s12891-020-03482-0
Yi LM, Ahmad AA, Ruslan SR, Abdullah S, Ahmad AR (2020) Plating distal radius fractures using wide-awake local anesthesia no tourniquet (WALANT) versus general anesthesia: a cohort study. J Hand Surg Global Online 2(6):331–338. https://doi.org/10.1016/j.jhsg.2020.09.003
Lipira AB, Sood RF, Tatman PD, Davis JI, Morrison SD, Ko JH (2015) Complications within 30 days of hand surgery: an analysis of 10,646 patients. The J Hand Surg 40(9):1852–59.e3. https://doi.org/10.1016/j.jhsa.2015.06.103
Goyal N, Bohl DD, Wysocki RW (2020) Timing of complications following hand surgery. J Hand Microsurg 14(1):31–38. https://doi.org/10.1055/s-0040-1709212
Warren VT, Fisher AG, Rivera EM, Saha PT, Turner B, Reside G, Phillips C, White RP Jr (2017) Buffered 1% lidocaine with epinephrine is as effective as non-buffered 2% lidocaine with epinephrine for mandibular nerve block. J Oral Maxillofacial Surg 75(7):1363–1366. https://doi.org/10.1016/j.joms.2016.12.045
Baker SD, Lee JY, White RP, Collins L, Bodnar W, Philips C, Divaris K (2021) Double-blind, randomized clinical trial comparing one percent buffered versus two percent unbuffered lidocaine injections in children. Pediatr Dent 43(2):88–94
Lee HJ, Cho YJ, Gong HS, Rhee SH, Park HS, Baek GH (2013) The effect of buffered lidocaine in local anesthesia: a prospective, randomized, double-blind study. The J Hand Surg 38(5):971–975. https://doi.org/10.1016/j.jhsa.2013.02.016
Percival SL, McCarty S, Hunt JA, Woods EJ (2014) The effects of pH on wound healing, biofilms, and antimicrobial efficacy. Wound Repair Regen 22(2):174–86. https://doi.org/10.1111/wrr.12125
Lane JCE, Craig RS, Rees JL, Gardiner MD, Green J, Prieto-Alhambra D, Furniss D (2020) Serious postoperative complications and reoperation after carpal tunnel decompression surgery in England: a nationwide cohort analysis. The Lancet Rheumatol 3(1):e49–e57. https://doi.org/10.1016/S2665-9913(20)30238-1
Bruijnzeel H, Neuhaus V, Fostvedt S, Jupiter JB, Mudgal CS, Ring DC (2012) Adverse events of open A1 pulley release for idiopathic trigger finger. The J Hand Surg 37(8):1650–1656. https://doi.org/10.1016/j.jhsa.2012.05.014
Cakmak F, Wolf MB, Bruckner T, Hahn P, Unglaub F (2012) Follow-up investigation of open trigger digit release. Arch Orthop Trauma Surg 132(5):685–691. https://doi.org/10.1007/s00402-011-1440-0
Finsen V, Hagen S (2003) Surgery for trigger finger. Hand surgery : an international journal devoted to hand and upper limb surgery and related research : journal of the Asia-Pacific Federation of Societies for Surgery of the Hand 8(2):201–203. https://doi.org/10.1142/s0218810403001820
Lange-Riess D, Schuh R, Hönle W, Schuh A (2009) Long-term results of surgical release of trigger finger and trigger thumb in adults. Arch Orthop Trauma Surg 129(12):1617–1619. https://doi.org/10.1007/s00402-008-0802-8
Lim MH, Lim KK, Rasheed MZ, Narayanan S, Beng-Hoi Tan A (2007) Outcome of open trigger digit release. The J Hand Surg Europ 32(4):457–459. https://doi.org/10.1016/J.JHSB.2007.02.016
Everding NG, Bishop GB, Belyea CM, Soong MC (2015) Risk factors for complications of open trigger finger release. Hand (New York N.Y) 10(2):297–300. https://doi.org/10.1007/s11552-014-9716-9
Koopman JE, Zweedijk BE, Hundepool CA, Duraku LS, Smit J, Wouters RM, Selles RW, Hand-Wrist Study Group, Zuidam, J. M (2022) Prevalence and risk factors for postoperative complications following open A1 pulley release for a trigger finger or thumb. The J Hand Surg 47(9):823–83. https://doi.org/10.1016/j.jhsa.2022.04.017
Kardestuncer M, Kardestuncer T (2022) Office-based open trigger finger release has a low complication rate. J Hand Surg Global Online 4(3):153–155. https://doi.org/10.1016/j.jhsg.2022.01.008
Dy CJ, Hernandez-Soria A, Ma Y, Roberts TR, Daluiski A (2012) Complications after flexor tendon repair: a systematic review and meta-analysis. The J Hand Surg 37(3):543-551.e1. https://doi.org/10.1016/j.jhsa.2011.11.006
Holoyda KA, Farhat B, Lalonde DH, Owusu-Danso O, Agbenorku P, Hoyte-Williams PE, Rockwell WB (2020) Creating an outpatient, local anesthetic hand operating room in a resource-constrained Ghanaian hospital builds surgical capacity and financial stability. Ann Plast Surg 84(4):385–389. https://doi.org/10.1097/SAP.0000000000002196
Lalonde D, Higgins A (2016) Wide awake flexor tendon repair in the finger. Plast Reconstr Surg Glob Open 4(7):e797. https://doi.org/10.1097/GOX.0000000000000756
Lalonde DH, Martin AL (2013) Wide-awake flexor tendon repair and early tendon mobilization in zones 1 and 2. Hand Clin 29(2):207–213. https://doi.org/10.1016/j.hcl.2013.02.009
Khor WS, Langer MF, Wong R, Zhou R, Peck F, Wong JKF (2016) Improving outcomes in tendon repair: a critical look at the evidence for flexor tendon repair and rehabilitation. Plast Reconstr Surg 138(6):1045e–1058e. https://doi.org/10.1097/PRS.0000000000002769
Holzer LA, Holzer G (2014) The 50 highest cited papers in hip and knee arthroplasty. J Arthroplasty 29(3):453–457. https://doi.org/10.1016/j.arth.2013.07.022
Lefaivre KA, Shadgan B, O’Brien PJ (2011) 100 most cited articles in orthopaedic surgery. Clin Orthop Relat Res 469(5):1487–1497. https://doi.org/10.1007/s11999-010-1604-1
Mercurio M, Cofano E, Familiari F, Corona K, Cerciello S, Gasparini G, Galasso O (2022) The 50 highest cited papers on shoulder arthroplasty. Healthcare (Basel, Switzerland) 10(10):2000. https://doi.org/10.3390/healthcare10102000
Raynaud M, Goutaudier V, Louis K, Al-Awadhi S, Dubourg Q, Truchot A, Brousse R, Saleh N, Giarraputo A, Debiais C, Demir Z, Certain A, Tacafred F, Cortes-Garcia E, Yanes S, Dagobert J, Naser S, Robin B, Bailly É, Jouven X, Reese PP, Loupy A (2021) Impact of the COVID-19 pandemic on publication dynamics and non-COVID-19 research production. BMC Med Res Methodol 21(1):255. https://doi.org/10.1186/s12874-021-01404-9
Gasson S, Solari F, Jesudason EP (2023) Sustainable hand surgery: incorporating water efficiency into clinical practice. Cureus 15(4):e38331. https://doi.org/10.7759/cureus.38331
Witt P, Ayhan E, Hagert E, Naqui Z (2022) The global FESSH green survey: sustainability in hand surgery. The J Hand Surg Europ 47(9):983–986. https://doi.org/10.1177/17531934221118658
Abdullah S, Chia Hua L, Sheau Yun L, Thavamany Devapitchai AS, Ahmad AA, Narin Singh PSG, Sapuan J (2021) A review of 1073 cases of wide-awake-local-anaesthesia-no-tourniquet (WALANT) in finger and hand surgeries in an urban hospital in Malaysia. Cureus 13(7):e16269. https://doi.org/10.7759/cureus.16269
Bajuri MY, Saidfudin NS, Mazli N, Azriq NA, Azemi AF (2022) Safety of wide-awake local anesthesia with no tourniquet (WALANT) in for lower limb surgery: a potential alternative in times of emergency. Frontiers Surg 9:848422. https://doi.org/10.3389/fsurg.2022.848422
Connors KM, Kurtzman JS, Koehler SM (2023) Successful use of WALANT in local and regional soft tissue flaps: a case series. Plast Reconstr Surg Glob Open 11(1):e4756. https://doi.org/10.1097/GOX.0000000000004756
Funding
Open Access funding provided by the Qatar National Library.
Author information
Authors and Affiliations
Contributions
EH generated the idea for this work. JL, AH, and EH put together the word search, inclusion, and exclusion criteria. JL and AH registered the study on PROSPERO and performed the literature search. JL and FD managed screening and data extraction, and discrepancies were resolved by senior author EH. All authors contributed to the manuscript text. AF performed the statistical analysis, interpretation of results, and prepared the figures and tables. AF and JL formatted the tables and figures. All authors contributed to the manuscript and agreed to be accountable for all aspects of the work.
Corresponding author
Ethics declarations
Ethical approval
This study is considered secondary research.
Consent to participate
This study is considered secondary research.
Consent for publication
This study is considered secondary research.
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Level of evidence: 3
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Lawand, J., Hantouly, A., Bouri, F. et al. Complications and side effects of Wide-Awake Local Anaesthesia No Tourniquet (WALANT) in upper limb surgery: a systematic review and meta-analysis. International Orthopaedics (SICOT) 48, 1257–1269 (2024). https://doi.org/10.1007/s00264-024-06104-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00264-024-06104-9