
Abstract
The design of efficacious and cost-effective therapeutic vaccines against cancer remains both a research priority and a challenge. For more than a decade, our laboratory has been involved in the development of synthetic peptide-based anti-cancer therapeutic vaccines. We first dedicated our efforts in the identification and validation of peptide epitopes for both CD8 and CD4 T cells from tumor-associated antigens (TAAs). Because of suboptimal immune responses and lack of therapeutic benefit of peptide vaccines containing these epitopes, we have focused our recent efforts in optimizing peptide vaccinations in mouse tumor models using numerous TAA epitopes. In this focused research review, we describe how after taking lessons from the immune system’s way of dealing with acute viral infections, we have designed peptide vaccination strategies capable of generating very high numbers of therapeutically effective CD8 T cells. We also discuss some of the remaining challenges to translate these findings into the clinical setting.
Similar content being viewed by others


Introduction
Although the main function of the immune system is to offer protection against infections, it also is capable of recognizing and responding to alterations resulting from malignant cell transformation. In both instances, the cells that become infected or transformed express antigens in the form of peptide/MHC-I complexes that can be recognized by CD8 T lymphocytes. Various studies reported that immunization of mice with synthetic peptides representing viral CD8 T cell epitopes induces immune responses that protect against infections [1–3]. This observation together with the identification of peptide epitopes derived from tumor-associated antigens (TAAs) has led to the development of peptide-based vaccines to treat various cancer types. However, although these vaccines induced some level of measurable T cell responses and occasional antitumor effects in murine models, their efficacy in the clinic has predominantly been disappointing [4]. We believe that this discouraging outcome is primarily due to the generation of low numbers of tumor-reactive T cells that cannot eradicate or control established tumors. In this review, we describe our experimental approach to design more potent peptide-based vaccines capable of inducing vast numbers of antigen-specific CD8 T cells exhibiting anti-tumor effects. This strategy is based on understanding how the immune system reacts quickly and strongly during acute viral infections, generating remarkable quantities of T cells that successfully eliminate the pathogen and offer long-term protection (memory) against reinfection.
Identification of CD8 T cell epitopes for peptide vaccine development
The definition of peptide-binding motifs to many of the common human and mouse MHC-I alleles facilitated the prediction of potential CD8 T cell epitopes from TAAs [5, 6]. Subsequently, we utilized synthetic peptides corresponding to the predicted epitopes to generate in vitro CD8 T cells that were tested for their ability to recognize tumor cells expressing the corresponding TAA and restricting MHC-I molecule [7–9]. Similarly, many groups have described various tumor-related CD8 T cell epitopes, and the list keeps growing every year [5, 10]. With this information on hand, clinical studies have been conducted in cancer patients that were vaccinated with recombinant TAAs, plasmid DNA encoding these antigens or synthetic peptides representing the identified CD8 T cell epitopes. Such vaccines have been administered either alone or in combination with various immune adjuvants [11–15], which were obviously suboptimal for generating substantive immune responses capable of curtailing the established malignancies. While in some instances T cell responses to the immunizing antigens were detected, in reality the frequency of TAA-specific CD8 T cells observed in blood, accounting for <1 % of the overall CD8 T cell population, was not very impressive. Moreover, it is also uncertain whether the vaccine-generated T cells exhibited the level of quality (i.e. had sufficient avidity and specificity) necessary to recognize and kill tumor cells [16]. In view of these outcomes, it is not surprising that “homeruns” (dramatic anti-tumor effects such as tumor eradications or long-term survival) have not yet been reported with the use of conventional anti-tumor vaccines. On the other hand, researchers working in the field adoptive T cell therapy (ACT) have observed many homeruns, where a substantial number of cancer patients experienced objective responses and some complete tumor regressions [17]. This approach initially was based on the isolation of the tumor-infiltrating lymphocytes, ex vivo expansion of tumor-specific cells to a large number and subsequently re-infusing these cells back into the patients alongside the administration of high doses of IL-2 to support their survival. Later, combination of ACT with host lymphodepletion (by using chemotherapy or whole-body irradiation) led to further improvement in the clonal repopulation of transferred cells by depleting T cells (including regulatory T cells), which presumably compete for cytokines [18]. Nevertheless, it is clear that ACT, even if it is effective in many patients, at this time is not very practical since it remains technically challenging, is not cost effective, and cannot be applied to those cancer patients where tumor-infiltrating lymphocytes are not readily available. In addition, procedures to allow in vivo T cell expansions of the transferred T cells (lymphodepletion, high-dose IL-2) generate severe undesirable effects. Despite these challenges, ACT provides a proof of concept that tumor eradication/control can be achieved in circumstances where huge numbers of tumor-reactive T cells are generated in the cancer patients. Evidently, this is something that therapeutic anti-cancer vaccines have so far failed to accomplish.
Lessons from acute systemic infections
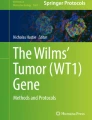
Unlike the weak immune responses to TAAs (observed during the course of the disease or resulting from vaccination studies), the immune system has the capacity to generate huge responses against infectious agents, where in some instances frequencies of 10–30 % of all CD8 T cells are specific against the pathogen, limiting the spread of the infectious agent and leading to the elimination of the invading microorganism [19, 20]. The generation of the large CD8 T cell responses against infectious agents involves highly controlled interactions between members of the innate and the adaptive immune systems. The innate immune system can recognize pathogen-associated molecular patterns through their stimulation of pattern recognition receptors (PRRs) providing the first line of defense against the infectious agent [21]. Some of the key PRRs for the initiation of innate immune responses are members of the toll-like receptor (TLR) family, which are widely expressed on professional antigen-presenting cells (APCs) such as dendritic cells (DCs) [22]. TLR activation leads to APC activation, the production of cytokines (IL-2, IL-12, interferon), and the upregulation of surface MHC-I/II and costimulatory molecules (CD80/CD86 and CD40), which are essential to initiate (prime) T cell responses [23]. The interaction of CD40 on DCs with its ligand on CD4 T helper lymphocytes further increases the efficacy of these APCs to generate effector and memory CD8 T cells [24]. Thus, during a typical viral infection, tissue-resident DCs will pick up viral antigens and TLR ligands (TLR-Ls) either by becoming infected or through the engulfment of viral immune complexes, or dead infected cells (Fig. 1). After activation by the TLR-Ls, the antigen-loaded DCs migrate to the draining lymph nodes where they prime the naïve T cells [25]. Subsequently, the activated T cells migrate to the infection site where they encounter antigen for a second time on infected non-professional APCs (npAPCs) and exert their effector function to control the infection. The infected cells, in addition to presenting antigen to the T cells, will emit an “I am infected” signal enabling the T cells to survive and continue to proliferate to large numbers until the infection is eradicated. What is this “I am infected” signal that potentially any cell is capable of emitting, which enables CD8 T cells to survive and proliferate upon antigen stimulation? Most if not all nucleated cells produce type-I IFN (IFN-I) as a result of detecting foreign genetic material through the stimulation of some cytoplasmic PRRs such as RNA helicases of the retinoic acid-inducible gene-I (RIG-I)-like receptor family or the DNA sensor, stimulator of interferon genes (STING). Notably, IFN-I has been shown to provide costimulation in the form of “signal 3” (S3) to CD8 T cells, allowing them to survive and proliferate upon antigen stimulation [26]. At the infection site, the activated CD8 T cells may also encounter Ag on tissue-resident activated DCs that are capable of providing alternative forms of S3 such as IL-2, IL-15, and cell surface costimulation. It is foreseeable that during the course of a viral infection, some CD8 T cells reactive to self-non-viral-antigens could become primed by activated DCs that present viral and non-viral antigens, and that these self-reactive T cells could generate autoimmunity. However, in most circumstances, when activated auto-reactive T cells migrate out of the lymphoid tissues to the periphery and encounter antigen on non-infected cells, in the absence of the “I am infected” signal, these T cells will have limited effector activity and will not survive nor proliferate.

T cell responses during an acute viral infection. 1 At the infection site, resident DCs acquire viral antigens either by becoming infected or through engulfment of viral immune complexes or dead infected cells. DCs become activated by viral pathogen-associated molecular patterns (DNA, RNA) through the stimulation PRRs. 2 After activation, antigen-presenting DCs migrate to secondary lymphoid tissues where they prime Ag-specific naïve T cells. 3 The Ag-stimulated CD8 T cells migrate to infection sites where they kill infected npAPCs and extensively expand after second encounter with Ag in the presence of IFN-I, which functions as S3. 4 At the infection site, activated CD8 T cells can also encounter Ag on tissue-resident DCs that are able to provide other sources of S3 such as IL-2, IL-15, and cell surface costimulation (4-1BBL, OX40L) to promote T cell survival and expansion
Developing effective peptide vaccines
The importance of the priming immunization
We believe that to achieve massive T cell expansions, the priming event is critical because it needs spawn a substantial number of activated T cells that will serve as a foundation for the subsequent expansion phase during the second encounter with antigen. Therefore, one must ensure that antigen reaches primarily DCs and that these APCs become suitably activated to stimulate naïve T cells in a way that they are capable of persisting and later proliferating when encountering antigen on npAPCs. It has been advocated that if naïve T cells see antigen first on npAPCs (or in non-activated DCs), either these T cells will ignore the stimulus or that suboptimal T cell activation will result in apoptosis or anergy [27–29]. One strategy to assure that the peptide will only be presented by DCs is the use of vaccines made with “long peptides” (LPs), which require antigen processing to produce the minimal MHC-I-binding peptide [30]. Some DC subsets are well adept to capture exogenous antigens and produce peptide/MHC-I complexes in a process known as cross-presentation [31]. The LP strategy assumes that vaccines containing the minimal MHC-I-binding peptide, or “short peptides” (SPs), will preferentially target the antigen to npAPCs. However, some of our results indicate that peptide size alone is not the only factor that determines whether a peptide will be presented effectively by DCs. For example, we showed that some vaccines made with SPs such as HPV16-E749–57, Ova257–264, and Trp2180–188 were highly immunogenic if administered with the right combination of immune adjuvants [32, 33]. Moreover, LPs containing the HPV16-E749–57 epitope when administered with the same adjuvants were substantially less immunogenic as compared to the SP (Fig. 2a) [34]. Close examination of the peptide’s composition revealed that synthetic peptides (SPs or LPs) exhibiting amphiphilic properties (a highly hydrophobic terminal end and the remainder portion being relatively hydrophilic) were considerably more immunogenic than hydrophilic or hydrophobic peptides. While the SP HPV16-E749–57 is highly amphiphilic, both of the LPs, HPV16-E745–57 and HPV16-E743–77, are not. When properly formulating these amphiphilic peptides in aqueous solutions, they will self-assemble into nanostructures [35] resembling viral particles that perhaps could be appealing for DC uptake. The immunogenicity of non-amphiphilic SPs such as Ova257–264 and Trp1455–463/9M was dramatically increased (>tenfold) by turning them into amphiphilic constructs (extending these peptides with hydrophobic residues or with palmitic acid chains) [34] (Fig. 2b). Thus, multiple factors determining antigen capture and processing by DCs and the ability of adjuvants/costimulatory antibodies to concomitantly activate DCs are probably more important than simply peptide size.

Peptide vaccines eliciting vast immune responses in mice. a Mice were immunized intravenously with equimolar amounts of the SP E749–57 (RAHYNIVTF, 30 µg/dose), or the LPs E745–57 (AEPDRAHYNIVTF, 44 µg/dose), and E743–77 (GQAEPDRAHYNIVTFCCKCDSTLRLCVQSTHVDIR, 117 µg/dose), a booster shot was given 7 days later, and the absolute number of tetramer positive CD8 T cells was determined in spleens 22 days after the prime (modified from Cho et al. [34]). b Mice were immunized intravenously with 2 identical doses (14 days apart) of equimolar amounts of the minimal (100 µg/dose) or palmitoylated (Pam, 120 µg/dose) peptides containing the Trp1455–463/9M (TAPDNLGYM) or Ova257–263 (SIINFEKL) epitopes, and the percentage of Ag-specific (tetramer positive) CD8 T cells was determined in blood 7 days after the prime and 7 days after the boost (modified from Cho et al. [34]). c Mice received TriVax (prime and boost) containing the Trp2180–188 (SVYDFFVWL, 200 µg dose) CD8 T cell epitope through different routes of administration (iv = intravenous; sc = subcutaneous). T cell responses were measured using purified CD8 T cells from spleens against Trp2-expressing B16 melanoma cells and peptide-pulsed and peptide-unpulsed target cells with an IFN-γ ELISPOT assay. Modified from Cho and Celis [33]. d Mice were immunized using BiVax containing the Pam peptide form of the Trp1455–463/9M epitope through different routes of administration (iv = intravenous; sc = subcutaneous; im = intramuscular). In these experiments, both TriVax and BiVax used poly-ICLC (Hiltonol) at a 50-µg dose. For TriVax, anti-CD40 mAb (clone FGK45.5) was included at a 100- or 50-µg dose (for prime or boost, respectively). All vaccine components were mixed for prior immunization. The presence of antigen-specific CD8 T cells in blood was measured by tetramer analyses 7 days after the prime and the boost (modified from Cho et al. [34]). In all panels, each dot represents an individual mouse, and horizontal bars are the mean responses for each group
The impact of route of administration on vaccine efficacy
Another element that will influence the priming efficacy of a vaccine is related to its capacity to recruit the bulk of the naïve CD8 T cell precursors that circulate throughout the secondary lymphoid tissues in search for their respective antigens and are presumably found in very low numbers in non-immunized individuals. Therefore, one would predict that non-infectious vaccines that are administered systemically (i.e. intravenously) would be highly immunogenic since this approach would disseminate antigen and adjuvants throughout numerous lymphoid tissues. On the other hand, conventional vaccines, which have been routinely injected in a sequestered site (i.e. subcutaneous, intradermal), will mostly target its components to the local draining lymph nodes, reaching only a limited fraction of the antigen-reactive naïve T cell precursor pool. Indeed, our studies have shown that intravenous peptide administration generates a substantially larger CD8 T cell response as compared to the conventional subcutaneous immunizations using the same peptide and adjuvants (Fig. 2c) [33]. Safety concerns regarding the use of the intravenous route of administrations can be somewhat alleviated by intramuscular vaccinations, which also deliver the vaccine components systemically (Fig. 2d) [34]. In summary, 2 major factors will determine the extent of a primary response: (1) peptide and adjuvant delivery to DCs; and (2) systemic distribution of peptide and adjuvants to recruit a majority of the naïve T cells.
The significance of the boosting event
Our vaccination model, which attempts to mimic a systemic infection, postulates that secondary antigen encounters (after adequate priming) will be decisive for generating massive CD8 T cell expansions. Thus, following this rationale, we predicted that secondary immunizations (boosts) using non-amphiphilic SPs that presumably can be presented by npAPCs would be effective in triggering such massive T cell expansions. However, our model dictates that these npAPCs must exhibit signs of having been infected such as producing IFN-I. Indeed, our results showed that boosters with non-amphiphilic SPs together with polyinosinic–polycytidylic acid (poly-IC) were effective in expanding T cell responses in WT mice but not in IFN-I-receptor-deficient (IFNαβR-KO) mice. On the other hand, secondary immunizations using the palmitoylated amphiphilic peptide (which forces presentation by professional APCs) induced the expansion of the CD8 T cells in an IFN-I-independent manner (Fig. 3a) [34], implying that DCs can provide other types of S3 in addition to IFN-I.

Role of adjuvants and IFN-I in the magnitude of immune responses elicited by peptide vaccines. a WT or IFNαβR-KO mice were primed with palmitoylated (Pam) peptide Trp1455–463/9M (120 µg dose) followed by a booster containing either the same Pam peptide or the minimal peptide (100 µg dose). The percentage of Ag-specific (tetramer positive) CD8 T cells was determined in the blood 7 days after the prime or the boost (modified from Cho et al. [34]). b WT mice were immunized with 2 identical doses of TriVax prepared with the minimal Ova257–264 peptide using one of the following TLR-Ls: poly-IC (TLR3-L), CpG (TLR9-L), LPS (TLR4-L), GDQ (TLR7-L), and FSL1 (TLR6/2-L). The percentage of tetramer positive cells was determined in the blood 7 days after the prime and the boost (modified from Cho and Celis [33]). c Mice were immunized BiVax/CpG (prime and boost 12 days apart) and boosted one more time with BiVax/poly-IC on day 24. The presence of antigen-specific CD8 T cells in blood was evaluated by tetramer analysis on the following days: 7, post-prime; 19, post-boost; and 31, post 2nd boost (modified from Cho et al. [34]). d Mice were immunized on days 0 and 14 with TriVax containing the hgp10025–33 (KVPRNQDWL) in the presence or absence of the STING agonist c-di-GMP. Antigen-specific CD8 T cell responses in blood were evaluated by tetramer analysis on day 7, post-prime and on day 21, post-boost (modified from Wang and Celis [39])
The role of adjuvants and APC costimulation
We have compared various TLR-Ls for their ability to function as adjuvants when administered in combination with synthetic peptides to induce CD8 T cell responses using two types of vaccines. We initiated our studies with a vaccine, TriVax that contained three components: a non-amphiphilic SP (Ova257–264), an agonistic anti-CD40 mAb, and a TLR-L [33]. Later, with BiVax, a vaccine that required the use of amphiphilic peptides, we were able to omit the use of the anti-CD40 mAb [34]. With TriVax, we established that TLR2/6-L, TLR3-L, TLR4-L, TLR7-L, or TLR9-L was similarly effective in priming substantial CD8 T cell responses, generating 10–20 % antigen-specific cells of all CD8 T cells in blood 7 days post-vaccination. Intriguingly, these TLR-Ls had very different effects in their ability to boost the T cell responses. Boosting with poly-IC (TLR3-L) generated an almost unbelievably huge CD8 T cell response accounting >70 % antigen-specific CD8 T cells in blood. LPS (TLR4-L) and gardiquimod (TLR7-L) were also effective, but to a lesser extent, in boosting the T cell responses inducing 30–40 % antigen-specific T cells. Conversely, FSL-1 (TLR2/6-L) and CpG-ODN (TLR9-L) downright failed to boost the response (Fig. 3b) [33]. Nonetheless, TriVax boosts using poly-IC were effective in expanding CD8 T cell responses in mice primed with TriVax prepared with CpG-ODN, indicating that the antigen-reactive T cells generated during the CpG-ODN prime were not defective and that poly-IC possesses an additional immune-stimulatory activity necessary for T cell expansion, which is absent in CpG-ODN (Fig. 3c) [34]. Indeed, poly-IC in addition to functioning as a TLR3-L has the capacity to stimulate cytoplasmic retinoic acid-inducible gene-I-like receptors such as melanosomal differentiation-associated protein 5 (MDA5) [36], resulting in the production of IFN-I. In contrast to TLR3, which is predominantly expressed by DCs [37], expression of MDA5 can be induced in a variety of tissues including non-hematopoietic stromal cells [38]. Similar to the results obtained with TriVax, the only TLR-L that was effective in inducing CD8 T cell responses using BiVax with amphiphilic peptides was poly-IC [34]. Thus, our results suggested that the unique ability of poly-IC to elicit huge CD8 responses after a boost relies on MDA5 stimulation, which generates the IFN-I, providing S3 to the antigen-stimulated T cells. Using mice deficient of TLR3 or MDA5, we evaluated the role of these PRRs in the CD8 T cell responses induced by BiVax with poly-IC after the prime and the boost. While priming was highly dependent on TLR3 activation, MDA5-deficient mice responded to the primary immunization to the same extent as WT mice [34]. On the other hand, T cell responses induced by the secondary immunization in MDA5-deficient mice were reduced by 50 % as compared to WT controls. Recently, we observed that the inclusion of a STING agonist to TriVax had a little effect during the priming response using an amphiphilic LP, but was very effective in potentiating the expansion of the T cells after boosting with non-amphiphilic SP, in an IFN-I-dependent manner (Fig. 3d) [39]. Altogether these results provide additional support to our infectious disease vaccination model where the dramatic CD8 T cell expansions after priming probably take place when the primed, previously activated T cells meet APCs that are not necessarily professional APCs in circumstances where IFN-I is being produced by activation of cytoplasmic PRRs such as MDA5 or STING.
Anti-tumor effects of TriVax and BiVax
As mentioned early on, the main purpose of designing potent peptide-based vaccines capable of generating vast T cell responses is to treat established tumors. Thus, our studies evaluated the ability of the TriVax and BiVax strategies to reduce/limit tumor growth in established mouse cancer models. Early on, we observed that TriVax using the CD8 T cell epitope Trp2180–188 exhibited dramatic prophylactic and therapeutic anti-tumor effects against the transplantable B16 melanoma tumor, when injected intravenously to mimic lung metastases [33]. However, the magnitude of the therapeutic effect depended on the tumor cell dose and the time of the first immunization. In these experiments, mice received the priming TriVax immunization 3 and 14 days after tumor injection and 80 and 60 % long-term survival (>100 days) was observed in mice that received 3 × 104 and 1 × 105 B16 cells, respectively. In these instances, all non-vaccinated mice and control vaccinated mice (irrelevant peptide) died between days 30 and 40 post-tumor injection. On the other hand, with higher tumor doses (3 × 105 cells), all of vaccinated mice died by day 60 (but exhibited a significant death delay). When the priming vaccine was given on days 5 or 7 post-tumor injection, anti-tumor effects were still observed but mice ultimately developed tumors and died. All mice that survived were re-challenged subcutaneously with live B16 cells, and none developed tumors indicating the establishment of immunological memory. The optimal therapeutic effect of TriVax against established B16 tumors required that the vaccine be administered intravenously. It should be noted that subcutaneous peptide vaccination in either PBS or incomplete Freund’s adjuvant, even when administered with poly-IC and anti-CD40 antibody, had a minimal, but significant therapeutic effect. In later studies, using the Trp1455–463/9M epitope with BiVax, we observed that the therapeutic effect against established B16 tumors could be dramatically enhanced by the concurrent administration of anti-PD-L1 antibodies, even when the vaccine was administered 7 days after tumor injection [34] resulting in complete tumor eradication. Similar dramatic therapeutic anti-tumor effects have been observed in a mouse tumor model of cervical/head and neck cancer expressing human papillomavirus antigens, where both TriVax [32] and BiVax [34] using the SP HPV16-E749–57 peptide were able to reject established TC1 subcutaneous tumors, and in this case, without the need of PD1 blockade.
Remaining questions and future challenges
One yet unanswered question is the identification of the specific APCs responsible for the priming and expansion phases of T cell responses generated by peptide/poly-IC vaccines. Since DCs are considered to be the only type of APC capable of processing exogenous antigens to the MHC-I pathway (cross-presentation), we assume that these cells are the major players in priming of T cell responses generated by amphiphilic peptides. Furthermore, DCs also possess costimulatory activities such as the expression of CD80/CD86 and production of cytokines (IL-12) that are necessary to stimulate naïve T cells. Experiments are ongoing to determine the effects of DC depletions using CD11c-diphtheria toxin receptor mice [40]. Because CD8a+ DCs are best suited for cross-priming CTLs [31], we will determine whether these APCs are responsible for TriVax and BiVax priming using CD8α+ DC-deficient mice [41]. The nature of the APCs involved in the expansion resulting from antigen reencounter could be diverse, depending on the type of peptide used during the boosting. While amphiphilic peptide boost may also require DCs to restimulate the antigen-primed T cell, it is possible that the non-amphiphilic SPs, which do not require further processing, can be effectively presented by any APC. The mechanisms involved in the stimulation of MDA5 by exogenous poly-IC remain a mystery. Either poly-IC gains direct access from the extracellular environment into the cytoplasm or after endocytosis it escapes endosomal compartments. One possible explanation is that poly-IC may induce endosomal destabilization followed by endosomal rupture and leaking of poly-IC from the endosomal compartments to the cytoplasm [42]. We also do not know whether poly-IC targets the same APC that is presenting the peptide to the T cells or if it works in a trans-mode on a different nearby cell. Paradoxically, there are reports that non-hematological stromal cells are the main producers of IFN-I after poly-IC stimulation [43, 44], but it is unclear how these non-phagocytic cells are able to capture exogenous poly-IC. It is considered that the main consequence of MDA5 stimulation is the production of IFN-I, which functions as S3 and enhances survival of antigen-specific CD8 T cells by increasing Bcl-3 expression [38]. However, the ability of BiVax containing amphiphilic peptide to boost T cell responses in IFN-I-receptor-deficient (IFNαβR-KO) mice (Fig. 3a) suggests that MDA5 activation can generate, in addition to IFN-I, other T cell stimulatory activities capable of providing S3. Thus, we hypothesize that when peptide is presented by DCs during the boost, MDA5 stimulation by poly-IC in the same cell results in the production of T cell stimulatory cytokines (e.g. IL-2, IL-15), or expression of cell surface costimulatory molecules (e.g. 4-1BBL, OX40L) that allow the expansion of the CTL response. On the other hand, when a npAPC presents peptide to the T cells in the absence of DC costimulation, IFN-I produced by either the same cell or a nearby (stromal?) cell is essential as S3. Although both TriVax and BiVax were able to induce substantial immune responses in mice, translation of these vaccines to the clinic could be challenging. One concern is adjusting the appropriate dose for each vaccine component to be reasonable for clinical use. For example, we routinely use ~ 100 μg peptide/20 g mouse, which is equivalent to 350 mg peptide/70 kg average adult, and such a high peptide dose could be impractical for the clinic. Another obstacle in taking TriVax into the clinic is the present unavailability of agonistic anti-CD40 mAbs for clinical use. This, together with safety concerns regarding the use of anti-CD40 mAbs in humans [45] and the availability of poly-IC (poly-ICLC, Hiltonol™), which has been safely used in many clinical studies [46, 47], enticed us to design and develop the BiVax approach [34].
Conclusions
Clearly, the immune system has the ability to respond efficiently to viruses, bacteria, and other invading pathogens, and it also has the capacity to control malignant disease. Although the immune response may become alert after malignant transformation, in many instances, this response alone is not sufficiently strong enough to overcome the tumor’s inherently immune suppressive nature. Our philosophy is that vaccines must elicit T cell responses resembling the magnitude and duration of the responses observed during acute viral infections and that combining these vaccines with blockade of the tumor immune suppression [48–50], we may be able to eradicate established tumors. Our studies with BiVax and TriVax in mouse tumor models provide support to this possibility, but challenges remain to translate these approaches into the clinic.
Abbreviations
- ACT:
-
Adoptive cell therapy
- Ag:
-
Antigen
- APC:
-
Antigen-presenting cell
- BiVax:
-
Vaccine containing synthetic peptide and a TLR-L
- CpG-ODN:
-
Unmethylated cytosine-guanine containing oligodeoxynucleotide
- CTL:
-
Cytotoxic T lymphocyte
- DC:
-
Dendritic cell
- IFN-I:
-
Type-I interferon
- LP:
-
Long peptide
- mAb:
-
Monoclonal antibody
- MDA5:
-
Melanosomal differentiation-associated protein 5
- MHC-I/II:
-
Major histocompatibility class I/II
- npAPC:
-
Non-professional antigen-presenting cell
- poly-IC:
-
Polyinosinic–polycytidylic acid
- PRR:
-
Pattern recognition receptor
- RIG-I:
-
Retinoic acid-inducible gene-I
- S3:
-
Signal 3
- SP:
-
Short peptide
- STING:
-
Stimulator of interferon genes
- TAA:
-
Tumor-associated antigen
- TLR:
-
Toll-like receptor
- TLR-L:
-
Toll-like receptor ligand
- TriVax:
-
Vaccine containing synthetic peptide, anti-CD40 mAb, and a TLR-L
References
Aichele P, Hengartner H, Zinkernagel RM, Schulz M (1990) Antiviral cytotoxic T cell response induced by in vivo priming with a free synthetic peptide. J Exp Med 171:1815–1820
Langeveld JP, Casal JI, Osterhaus AD, Cortes E, de Swart R, Vela C, Dalsgaard K, Puijk WC, Schaaper WM, Meloen RH (1994) First peptide vaccine providing protection against viral infection in the target animal: studies of canine parvovirus in dogs. J Virol 68:4506–4513
Casal JI, Langeveld JP, Cortes E, Schaaper WW, van Dijk E, Vela C, Kamstrup S, Meloen RH (1995) Peptide vaccine against canine parvovirus: identification of two neutralization subsites in the N terminus of VP2 and optimization of the amino acid sequence. J Virol 69:7274–7277
Rosenberg SA, Yang JC, Restifo NP (2004) Cancer immunotherapy: moving beyond current vaccines. Nat Med 10:909–915. doi:10.1038/nm1100
Rammensee H, Bachmann J, Emmerich NP, Bachor OA, Stevanovic S (1999) SYFPEITHI: database for MHC ligands and peptide motifs. Access via: http://www.syfpeithi.de. Immunogenetics 50:213-9
Appella E, Padlan EA, Hunt DF (1995) Analysis of the structure of naturally processed peptides bound by class I and class II major histocompatibility complex molecules. EXS 73:105–119
Celis E, Fikes J, Wentworth P, Sidney J, Southwood S, Maewal A, Del Guercio MF, Sette A, Livingston B (1994) Identification of potential CTL epitopes of tumor-associated antigen MAGE-1 for five common HLA-A alleles. Mol Immunol 31:1423–1430
Celis E, Tsai V, Crimi C, DeMars R, Wentworth PA, Chesnut RW, Grey HM, Sette A, Serra HM (1994) Induction of anti-tumor cytotoxic T lymphocytes in normal humans using primary cultures and synthetic peptide epitopes. Proc Natl Acad Sci USA 91:2105–2109
Kawashima I, Hudson SJ, Tsai V, Southwood S, Takesako K, Appella E, Sette A, Celis E (1998) The multi-epitope approach for immunotherapy for cancer: identification of several CTL epitopes from various tumor-associated antigens expressed on solid epithelial tumors. Hum Immunol 59:1–14
Vita R, Overton JA, Greenbaum JA, Ponomarenko J, Clark JD, Cantrell JR, Wheeler DK, Gabbard JL, Hix D, Sette A, Peters B (2015) The immune epitope database (IEDB) 3.0. Nucleic Acids Res 43:D405–D412. doi:10.1093/nar/gku938
Weber JS, Hua FL, Spears L, Marty V, Kuniyoshi C, Celis E (1999) A phase I trial of an HLA-A1 restricted MAGE-3 epitope peptide with incomplete Freund’s adjuvant in patients with resected high-risk melanoma. J Immunother 22:431–440
Khleif SN, Abrams SI, Hamilton JM, Bergmann-Leitner E, Chen A, Bastian A, Bernstein S, Chung Y, Allegra CJ, Schlom J (1999) A phase I vaccine trial with peptides reflecting ras oncogene mutations of solid tumors. J Immunother 22:155–165
Markovic SN, Suman VJ, Ingle JN, Kaur JS, Pitot HC, Loprinzi CL, Rao RD, Creagan ET, Pittelkow MR, Allred JB, Nevala WK, Celis E (2006) Peptide vaccination of patients with metastatic melanoma: improved clinical outcome in patients demonstrating effective immunization. Am J Clin Oncol 29:352–360. doi:10.1097/01.coc.0000217877.78473.a4
Celis E (2007) Overlapping human leukocyte antigen class I/II binding peptide vaccine for the treatment of patients with stage IV melanoma: evidence of systemic immune dysfunction. Cancer 110:203–214. doi:10.1002/cncr.22744
Slingluff CL Jr, Petroni GR, Yamshchikov GV, Hibbitts S, Grosh WW, Chianese-Bullock KA, Bissonette EA, Barnd DL, Deacon DH, Patterson JW, Parekh J, Neese PY, Woodson EM, Wiernasz CJ, Merrill P (2004) Immunologic and clinical outcomes of vaccination with a multiepitope melanoma peptide vaccine plus low-dose interleukin-2 administered either concurrently or on a delayed schedule. J Clin Oncol 22:4474–4485. doi:10.1200/jco.2004.10.212
Zaks TZ, Rosenberg SA (1998) Immunization with a peptide epitope (p369–377) from HER-2/neu leads to peptide-specific cytotoxic T lymphocytes that fail to recognize HER-2/neu+ tumors. Cancer Res 58:4902–4908
Rosenberg SA, Restifo NP (2015) Adoptive cell transfer as personalized immunotherapy for human cancer. Science 348:62–68. doi:10.1126/science.aaa4967
Dudley ME, Wunderlich JR, Yang JC, Sherry RM, Topalian SL, Restifo NP, Royal RE, Kammula U, White DE, Mavroukakis SA, Rogers LJ, Gracia GJ, Jones SA, Mangiameli DP, Pelletier MM, Gea-Banacloche J, Robinson MR, Berman DM, Filie AC, Abati A, Rosenberg SA (2005) Adoptive cell transfer therapy following non-myeloablative but lymphodepleting chemotherapy for the treatment of patients with refractory metastatic melanoma. J Clin Oncol 23:2346–2357. doi:10.1200/jco.2005.00.240
Butz EA, Bevan MJ (1998) Massive expansion of antigen-specific CD8+ T cells during an acute virus infection. Immunity 8:167–175
Murali-Krishna K, Altman JD, Suresh M, Sourdive DJ, Zajac AJ, Miller JD, Slansky J, Ahmed R (1998) Counting antigen-specific CD8 T cells: a reevaluation of bystander activation during viral infection. Immunity 8:177–187
Medzhitov R, Janeway C Jr (2000) Innate immunity. N Engl J Med 343:338–344. doi:10.1056/nejm200008033430506
Medzhitov R, Preston-Hurlburt P, Janeway CA Jr (1997) A human homologue of the Drosophila Toll protein signals activation of adaptive immunity. Nature 388:394–397. doi:10.1038/41131
Rescigno M, Granucci F, Citterio S, Foti M, Ricciardi-Castagnoli P (1999) Coordinated events during bacteria-induced DC maturation. Immunol Today 20:200–203
Bennett SR, Carbone FR, Karamalis F, Flavell RA, Miller JF, Heath WR (1998) Help for cytotoxic-T-cell responses is mediated by CD40 signalling. Nature 393:478–480. doi:10.1038/30996
Banchereau J, Steinman RM (1998) Dendritic cells and the control of immunity. Nature 392:245–252. doi:10.1038/32588
Curtsinger JM, Valenzuela JO, Agarwal P, Lins D, Mescher MF (2005) Type I IFNs provide a third signal to CD8 T cells to stimulate clonal expansion and differentiation. J Immunol 174:4465–4469
Iezzi G, Karjalainen K, Lanzavecchia A (1998) The duration of antigenic stimulation determines the fate of naive and effector T cells. Immunity 8:89–95
Suhrbier A, Burrows SR, Fernan A, Lavin MF, Baxter GD, Moss DJ (1993) Peptide epitope induced apoptosis of human cytotoxic T lymphocytes. Implications for peripheral T cell deletion and peptide vaccination. J Immunol 150:2169–2178
Toes RE, Offringa R, Blom RJ, Melief CJ, Kast WM (1996) Peptide vaccination can lead to enhanced tumor growth through specific T-cell tolerance induction. Proc Natl Acad Sci USA 93:7855–7860
Melief CJ, van der Burg SH (2008) Immunotherapy of established (pre)malignant disease by synthetic long peptide vaccines. Nat Rev Cancer 8:351–360. doi:10.1038/nrc2373
den Haan JM, Lehar SM, Bevan MJ (2000) CD8(+) but not CD8(−) dendritic cells cross-prime cytotoxic T cells in vivo. J Exp Med 192:1685–1696
Barrios K, Celis E (2012) TriVax-HPV: an improved peptide-based therapeutic vaccination strategy against human papillomavirus-induced cancers. Cancer Immunol Immunother 61:1307–1317. doi:10.1007/s00262-012-1259-8
Cho HI, Celis E (2009) Optimized peptide vaccines eliciting extensive CD8 T-cell responses with therapeutic antitumor effects. Cancer Res 69:9012–9019. doi:10.1158/0008-5472.can-09-2019
Cho HI, Barrios K, Lee YR, Linowski AK, Celis E (2013) BiVax: a peptide/poly-IC subunit vaccine that mimics an acute infection elicits vast and effective anti-tumor CD8 T-cell responses. Cancer Immunol Immunother 62:787–799. doi:10.1007/s00262-012-1382-6
Hartgerink JD, Beniash E, Stupp SI (2001) Self-assembly and mineralization of peptide-amphiphile nanofibers. Science 294:1684–1688. doi:10.1126/science.1063187
Kato H, Takeuchi O, Sato S, Yoneyama M, Yamamoto M, Matsui K, Uematsu S, Jung A, Kawai T, Ishii KJ, Yamaguchi O, Otsu K, Tsujimura T, Koh CS, Reis e Sousa C, Matsuura Y, Fujita T, Akira S (2006) Differential roles of MDA5 and RIG-I helicases in the recognition of RNA viruses. Nature 441:101–105. doi:10.1038/nature04734
Muzio M, Bosisio D, Polentarutti N, D’Amico G, Stoppacciaro A, Mancinelli R, van’t Veer C, Penton-Rol G, Ruco LP, Allavena P, Mantovani A (2000) Differential expression and regulation of toll-like receptors (TLR) in human leukocytes: selective expression of TLR3 in dendritic cells. J Immunol 164:5998–6004
Wang Y, Cella M, Gilfillan S, Colonna M (2010) Cutting edge: polyinosinic: polycytidylic acid boosts the generation of memory CD8 T cells through melanoma differentiation-associated protein 5 expressed in stromal cells. J Immunol 184:2751–2755. doi:10.4049/jimmunol.0903201
Wang Z, Celis E (2015) STING activator c-di-GMP enhances the anti-tumor effects of peptide vaccines in melanoma-bearing mice. Cancer Immunol Immunother 64:1057–1066. doi:10.1007/s00262-015-1713-5
Jung S, Unutmaz D, Wong P, Sano G, De los Santos K, Sparwasser T, Wu S, Vuthoori S, Ko K, Zavala F, Pamer EG, Littman DR, Lang RA (2002) In vivo depletion of CD11c+ dendritic cells abrogates priming of CD8+ T cells by exogenous cell-associated antigens. Immunity 17:211–220
Hildner K, Edelson BT, Purtha WE, Diamond M, Matsushita H, Kohyama M, Calderon B, Schraml BU, Unanue ER, Diamond MS, Schreiber RD, Murphy TL, Murphy KM (2008) Batf3 deficiency reveals a critical role for CD8alpha+ dendritic cells in cytotoxic T cell immunity. Science 322:1097–1100. doi:10.1126/science.1164206
Zou J, Kawai T, Tsuchida T, Kozaki T, Tanaka H, Shin KS, Kumar H, Akira S (2013) Poly IC triggers a cathepsin D- and IPS-1-dependent pathway to enhance cytokine production and mediate dendritic cell necroptosis. Immunity 38:717–728. doi:10.1016/j.immuni.2012.12.007
Longhi MP, Trumpfheller C, Idoyaga J, Caskey M, Matos I, Kluger C, Salazar AM, Colonna M, Steinman RM (2009) Dendritic cells require a systemic type I interferon response to mature and induce CD4+ Th1 immunity with poly IC as adjuvant. J Exp Med 206:1589–1602. doi:10.1084/jem.20090247
McCartney S, Vermi W, Gilfillan S, Cella M, Murphy TL, Schreiber RD, Murphy KM, Colonna M (2009) Distinct and complementary functions of MDA5 and TLR3 in poly(I:C)-mediated activation of mouse NK cells. J Exp Med 206:2967–2976. doi:10.1084/jem.20091181
Vonderheide RH, Burg JM, Mick R, Trosko JA, Li D, Shaik MN, Tolcher AW, Hamid O (2013) Phase I study of the CD40 agonist antibody CP-870,893 combined with carboplatin and paclitaxel in patients with advanced solid tumors. Oncoimmunology 2:e23033. doi:10.4161/onci.23033
Caskey M, Lefebvre F, Filali-Mouhim A, Cameron MJ, Goulet JP, Haddad EK, Breton G, Trumpfheller C, Pollak S, Shimeliovich I, Duque-Alarcon A, Pan L, Nelkenbaum A, Salazar AM, Schlesinger SJ, Steinman RM, Sekaly RP (2011) Synthetic double-stranded RNA induces innate immune responses similar to a live viral vaccine in humans. J Exp Med 208:2357–2366. doi:10.1084/jem.20111171
Rosenfeld MR, Chamberlain MC, Grossman SA, Peereboom DM, Lesser GJ, Batchelor TT, Desideri S, Salazar AM, Ye X (2010) A multi-institution phase II study of poly-ICLC and radiotherapy with concurrent and adjuvant temozolomide in adults with newly diagnosed glioblastoma. Neuro Oncol 12:1071–1077. doi:10.1093/neuonc/noq071
Hamid O, Robert C, Daud A, Hodi FS, Hwu WJ, Kefford R, Wolchok JD, Hersey P, Joseph RW, Weber JS, Dronca R, Gangadhar TC, Patnaik A, Zarour H, Joshua AM, Gergich K, Elassaiss-Schaap J, Algazi A, Mateus C, Boasberg P, Tumeh PC, Chmielowski B, Ebbinghaus SW, Li XN, Kang SP, Ribas A (2013) Safety and tumor responses with lambrolizumab (anti-PD-1) in melanoma. N Engl J Med 369:134–144. doi:10.1056/NEJMoa1305133
Brahmer JR, Drake CG, Wollner I, Powderly JD, Picus J, Sharfman WH, Stankevich E, Pons A, Salay TM, McMiller TL, Gilson MM, Wang C, Selby M, Taube JM, Anders R, Chen L, Korman AJ, Pardoll DM, Lowy I, Topalian SL (2010) Phase I study of single-agent anti-programmed death-1 (MDX-1106) in refractory solid tumors: safety, clinical activity, pharmacodynamics, and immunologic correlates. J Clin Oncol 28:3167–3175. doi:10.1200/jco.2009.26.7609
Small EJ, Tchekmedyian NS, Rini BI, Fong L, Lowy I, Allison JP (2007) A pilot trial of CTLA-4 blockade with human anti-CTLA-4 in patients with hormone-refractory prostate cancer. Clin Cancer Res 13:1810–1815. doi:10.1158/1078-0432.ccr-06-2318
Acknowledgments
This work was supported by grants from the National Cancer Institute of the National Institutes of Health, R01CA136828 and R01CA157303, and by start-up funds from Augusta University Cancer Center and the Georgia Research Alliance (GRA). Esteban Celis holds the Cecil F. Whitaker Jr. MD/GRA Eminent Scholar Chair in Tumor Immunology.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Esteban Celis has filed patent applications based on the use of synthetic peptides and poly-IC combinatorial vaccines. The rights of the patent applications have been transferred to the Moffitt Cancer Center (Tampa, FL). Andres Salazar is President and CEO of Oncovir, Inc., who is developing poly-ICLC (Hiltonol™) for the clinic. Hussein Sultan, Valentyna Fesenkova, Diane Addis, Aaron Fan, Takumi Kumai, and Juan Wu declare no conflict of interest.
Additional information
This paper is a Focussed Research Review based on a presentation given at the Fifteenth International Conference on Progress in Vaccination against Cancer (PIVAC 15), held in Tübingen, Germany, 6th–8th October, 2015. It is part of a Cancer Immunology, Immunotherapy series of Focussed Research Reviews and meeting report.
Rights and permissions
About this article

Cite this article
Sultan, H., Fesenkova, V.I., Addis, D. et al. Designing therapeutic cancer vaccines by mimicking viral infections. Cancer Immunol Immunother 66, 203–213 (2017). https://doi.org/10.1007/s00262-016-1834-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00262-016-1834-5