
Abstract
Purpose
To determine reliable CT features to distinguish cancerous from inflammatory colorectal perforations.
Materials and methods
A total of 43 patients with surgically and pathologically confirmed colorectal perforation caused by either colorectal cancer (n =27) or an inflammatory conditions (n = 16) were identified. Two radiologists independently assessed the contrast-enhanced CT features for locations of perforation, mural configurations, soft-tissue alterations, lymphadenopathy, and metastases. Intergroup comparisons for univariate analysis were performed using Fisher’s exact test or chi-square test for categorical data and Mann–Whitney test for numeric data. Stepwise logistic regression analysis was conducted with features that were found significant under the univariate analysis. Interobserver agreement was assessed using intraclass correlation coefficient (ICC) and kappa test.
Results
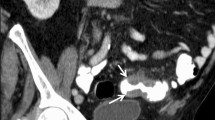
Maximal mural thickness >1.39 cm (sensitivity, 100%; specificity, 68.75%), luminal mass or shoulder formation (sensitivity, 88.89%; specificity, 68.75%), absence of diverticula (sensitivity, 96.30%; specificity, 50.00%), irregular mural thickening (sensitivity, 92.59%; specificity, 81.25%), lymphadenopathy (sensitivity, 40.74%; specificity, 93.75%), and metastases (sensitivity, 25.93%; specificity, 100%) were significantly frequent in cancerous perforations. The maximal mural thickness (P = 0.0493, odds ratio = 439.83) and irregular mural thickening (P = 0.0343, odds ratio = 4.69) were identified as the highly distinguished identifiers.
Conclusions
The CT manifestations of cancerous and inflammatory colorectal perforations overlap. Definitive diagnosis is not always possible with imaging alone. The maximal mural thickness >1.39 cm and irregular configuration of the thickened bowel wall were the two highly statistically significant CT features that may help order the difference between the two entities.







Similar content being viewed by others


References
Lee IK, Sung NY, Lee YS, et al. (2007) The survival rate and prognostic factors in 26 perforated colorectal cancer patients. Int J Colorectal Dis 22(5):467–473
Ogawa M, Watanabe M, Eto K, et al. (2009) Clinicopathological features of perforated colorectal cancer. Anticancer Res 29(5):1681–1684
Mandava N, Kumar S, Pizzi WF, Aprile IJ (1996) Perforated colorectal carcinomas. Am J Surg 172(3):236–238
Chen HS, Sheen-Chen SM (2000) Obstruction and perforation in colorectal adenocarcinoma: an analysis of prognosis and current trends. Surgery 127(4):370–376
Steinberg SM, Barkin JS, Kaplan RS, Stablein DM (1986) Prognostic indicators of colon tumors. The Gastrointestinal Tumor Study Group experience. Cancer 57(9):1866–1870
Kaiser AM, Jiang JK, Lake JP, et al. (2005) The management of complicated diverticulitis and the role of computed tomography. Am J Gastroenterol 100(4):910–917
Berg DF, Bahadursingh AM, Kaminski DL, Longo WE (2002) Acute surgical emergencies in inflammatory bowel disease. Am J Surg 184(1):45–51
Wu CH, Huang CC, Wang LJ, et al. (2012) Value of CT in the discrimination of fatal from non-fatal stercoral colitis. Korean J Radiol 13(3):283–289
Oguro S, Funabiki T, Hosoda K, et al. (2010) 64-Slice multidetector computed tomography evaluation of gastrointestinal tract perforation site: detectability of direct findings in upper and lower GI tract. Eur Radiol 20(6):1396–1403
Thornton E, Mendiratta-Lala M, Siewert B, Eisenberg RL (2011) Patterns of fat stranding. AJR Am J Roentgenol 197(1):W1–14
Padidar AM, Jeffrey RB Jr, Mindelzun RE, Dolph JF (1994) Differentiating sigmoid diverticulitis from carcinoma on CT scans: mesenteric inflammation suggests diverticulitis. AJR Am J Roentgenol 163(1):81–83
Chintapalli KN, Chopra S, Ghiatas AA, et al. (1999) Diverticulitis versus colon cancer: differentiation with helical CT findings. Radiology 210(2):429–435
Anderson EM, Betts M, Slater A (2011) The value of true axial imaging for CT staging of colonic cancer. Eur Radiol 21(6):1286–1292
Lips LM, Cremers PT, Pickhardt PJ, et al. (2015) Sigmoid cancer versus chronic diverticular disease: differentiating features at CT colonography. Radiology 275(1):127–135
Kircher MF, Rhea JT, Kihiczak D, Novelline RA (2002) Frequency, sensitivity, and specificity of individual signs of diverticulitis on thin-section helical CT with colonic contrast material: experience with 312 cases. AJR Am J Roentgenol 178(6):1313–1318
Naqvi J, Hosmane S, Lapsia S (2015) Revisiting the potential signs of colorectal cancer on contrast-enhanced computed tomography without bowel preparation. Abdom Imaging 40(8):2993–3001
Macari M, Balthazar EJ (2001) CT of bowel wall thickening: significance and pitfalls of interpretation. AJR Am J Roentgenol 176(5):1105–1116
Wittenberg J, Harisinghani MG, Jhaveri K, Varghese J, Mueller PR (2002) Algorithmic approach to CT diagnosis of the abnormal bowel wall. Radiographics 22(5):1093–1107
Balthazar EJ (1991) CT of the gastrointestinal tract: principles and interpretation. AJR Am J Roentgenol 156(1):23–32
Horton KM, Abrams RA, Fishman EK (2000) Spiral CT of colon cancer: imaging features and role in management. Radiographics 20(2):419–430
Hainaux B, Agneessens E, Bertinotti R, et al. (2006) Accuracy of MDCT in predicting site of gastrointestinal tract perforation. AJR Am J Roentgenol 187(5):1179–1183
Ghekiere O, Lesnik A, Millet I, et al. (2007) Direct visualization of perforation sites in patients with a non-traumatic free pneumoperitoneum: added diagnostic value of thin transverse slices and coronal and sagittal reformations for multi-detector CT. Eur Radiol 17(9):2302–2309
Kim SW, Shin HC, Kim IY, Kim YT, Kim CJ (2010) CT findings of colonic complications associated with colon cancer. Korean J Radiol 11(2):211–221
Kim SW, Kim HC, Yang DM (2012) Perforated tumours in the gastrointestinal tract: CT findings and clinical implications. Br J Radiol 85(1017):1307–1313
Welch JP, Donaldson GA (1974) Perforative carcinoma of colon and rectum. Ann Surg 180(5):734–740
Kelley WE Jr, Brown PW, Lawrence W Jr, Terz JJ (1981) Penetrating, obstructing, and perforating carcinomas of the colon and rectum. Arch Surg 116(4):381–384
Ripolles T, Martinez-Perez MJ, Gomez Valencia DP, Vizuete J, Martin G (2015) Sigmoid stenosis caused by diverticulitis vs. carcinoma: usefulness of sonographic features for their differentiation in the emergency setting. Abdom Imaging 40(7):2219–2231
Shen SH, Chen JD, Tiu CM, et al. (2005) Differentiating colonic diverticulitis from colon cancer: the value of computed tomography in the emergency setting. J Chin Med Assoc 68(9):411–418
Jang HJ, Lim HK, Lee SJ, et al. (2000) Acute diverticulitis of the cecum and ascending colon: the value of thin-section helical CT findings in excluding colonic carcinoma. AJR Am J Roentgenol 174(5):1397–1402
Sheiman L, Levine MS, Levin AA, et al. (2008) Chronic diverticulitis: clinical, radiographic, and pathologic findings. AJR Am J Roentgenol 191(2):522–528
Greenbaum EI, Freedman S (1973) Neoplasia of the colon over a long segment. Clin Radiol 24(4):416–426
Sheth AA, Longo W, Floch MH (2008) Diverticular disease and diverticulitis. Am J Gastroenterol 103(6):1550–1556
Law WL, Lo CY, Chu KW (2001) Emergency surgery for colonic diverticulitis: differences between right-sided and left-sided lesions. Int J Colorectal Dis 16(5):280–284
Khalil HA, Yoo J (2014) Colorectal emergencies: perforated diverticulitis (operative and nonoperative management). J Gastrointest Surg 18(4):865–868
Markham NI, Li AK (1992) Diverticulitis of the right colon–experience from Hong Kong. Gut 33(4):547–549
Acknowledgments
This study was partly funded by the Chinese National Natural Science Foundation (Grant 81401373). The authors thank Dr. Wei He, department of pathology, Renji Hospital, School of Medicine, Shanghai Jiao Tong University, for her help with pathological consultation.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
This study was partly funded by the Chinese National Natural Science Foundation (Grant 81401373).
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. The study was approved by our institutional review board. For this type of study formal consent is not required.
Informed consent
Informed consents were waived by the ethical commission of our institution.
Rights and permissions
About this article

Cite this article
Gong, X.H., Zhuang, Z.G., Zhu, J. et al. Differentiation of cancerous and inflammatory colorectal perforations using multi-detector computed tomography. Abdom Radiol 42, 2233–2242 (2017). https://doi.org/10.1007/s00261-017-1134-3
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00261-017-1134-3