
Abstract
Purpose
Accurate diagnosis and staging of prostate cancer are crucial to improving patient care. Prostate-specific membrane antigen (PSMA)-targeted positron emission tomography with computed tomography (PET/CT) imaging has demonstrated superiority for initial staging and restaging in patients with prostate cancer. Referring physicians and PET/CT readers must agree on a consistent communication method and application of information derived from this imaging modality. While several guidelines have been published, a single PSMA PET/CT reporting template has yet to be widely adopted. Based on the consensus from community and academic physicians, we developed a standardized PSMA PET/CT reporting template for radiologists and nuclear medicine physicians to report and relay key imaging findings to referring physicians. The aim was to improve the quality, clarity, and utility of imaging results reporting to facilitate patient management decisions.
Methods
Based on community and expert consensus, we developed a standardized PSMA PET/CT reporting template to deliver key imaging findings to referring clinicians.
Results
Core category components proposed include a summary of any prior treatment history; presence, location, and degree of PSMA radiopharmaceutical uptake in primary and/or metastatic tumor(s), lesions with no uptake, and incidentally found lesions with positive uptake on PET/CT.
Conclusions
This article provides recommendations on best practices for standardized reporting of PSMA PET/CT imaging. The generated reporting template is a proposed supplement designed to educate and improve data communication between imaging experts and referring physicians.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Background
Prostate-specific membrane antigen
Prostate cancer (PCa) is the most diagnosed cancer among males worldwide and the accurate methods for diagnosis, staging, and restaging of this disease are crucial for patient management. Prostate-specific membrane antigen (PSMA) positron emission tomography (PET) scan has recently been adopted as an imaging modality for men with PCa. PSMA is a membrane-bound metallopeptidase glycoprotein encoded by the folate hydrolase 1 gene on chromosome 11 [1]. It is expressed in several tissues with moderate to intense physiological uptake seen in the liver, duodenum, parotid glands, ganglions, and others [2, 3] (Supplemental Table 1). Additionally, PSMA is overexpressed in over 90% of PCa cells. In untreated patients, PSMA overexpression increases with the tumor grade and aggressiveness [4].
PSMA-targeting compounds (e.g., PSMA-11, PSMA I&T, PSMA-617, PSMA-1007, DCFPyL, rhPSMA7.3) can be coupled with positron emitting radioisotopes such as gallium-68, fluorine-18 or copper-64 to form a PET radiopharmaceutical [5]. Following injection, the PSMA-targeted radiopharmaceutical rapidly clears out from the bloodstream, binds to the PSMA site, and gets internalized via clathrin-coated pits and then endocytosed [6]. Because of the typically high density of PSMA on the surface of PCa cells relative to the adjacent prostate (for primary tumor) or other close or distant non-neoplastic background tissues (for primary and metastatic tumors), PSMA PET provides images with a high tumor-to-background uptake ratio [7,8,9]. PSMA PET has been shown to have higher sensitivity and specificity than conventional imaging for PCa in several clinical settings, from initial staging to detection and localization of biochemical recurrence (BCR), restaging and assessment of eligibility for PSMA-targeted radiopharmaceutical therapies [10].
PSMA positron emission tomography and computed tomography (PET/CT) imaging is increasingly adopted in routine clinical practice worldwide [11]. Developing consensus guidelines for interpreting PSMA PET may improve the quality of care by reducing variability in interpretation through accurate quantification of disease burden with increased reproducibility on a patient level, which may lead to more accurate diagnoses and appropriate treatment strategies. Moreover, standardized reporting facilitates clearer communication among the multidisciplinary team members involved in PCa care, including urologists, oncologists, radiation oncologists, and pathologists. This can lead to more effective and coordinated patient management [12]. The currently available guidelines are directed more towards academic imaging experts, and their terminology and technical details may be less familiar or useful to the community imaging experts and clinicians. In this paper, we propose a practical, downloadable, standardized PSMA image reporting tool targeted towards community physicians that includes information for the referring providers to understand a patient’s full clinical picture and to better help determine patient management [13].
Clinical utility of PSMA
Most primary and metastatic prostate adenocarcinomas demonstrate PSMA overexpression, which correlates with disease aggressiveness in the treatment naïve setting [14]. The use of PSMA PET/CT is increasing in routine clinical practice, such as in the initial staging of high-risk primary PCa, patients with BCR, follow-up during and after local or systemic treatment, and, recently, several centers use it for intraprostatic evaluation of the lesions where magnetic resonance imaging (MRI) is contraindicated and for assessment of extra-prostatic extension for surgical guidance in PCa [15,16,17]. The adoption of PSMA PET/CT has resulted in a profound transformation of PCa management since its FDA approval and addition to various international cancer management guidelines (Supplemental Table 2) in recent years [13, 18,19,20,21,22,23].
Despite the “prostate-specific” term, PSMA is also expressed in non-prostatic tissues and other pathologic conditions and can be visualized through the urinary, salivary, or hepatobiliary system where it is physiologically excreted [24]. In addition, PSMA is expressed on neovascular cells, other neoplasms, and inflammatory or remodeling processes [25, 26]. Different radiopharmaceuticals exhibit unique physiological distribution patterns [27, 28]. Reader training and knowledge of the normal biodistribution of PSMA-targeted radiopharmaceutical and understanding other pathological conditions with increased radiopharmaceutical uptake on PET/CT are important for precise interpretation [2, 15, 24, 29]. One study reported that properly trained physicians accurately interpret [68Ga]Ga-PSMA-11 PET images in up to 90% of cases [30].
Gaps and barriers in current reporting guidelines
Risk stratification is an important factor for deciding the further course of management following diagnosis. Currently, this is based on various clinical and histopathological factors and predictive mathematical models, as seen in the D’Amico, National Comprehensive Cancer Network®, and University of California San Francisco-Cancer of the Prostate Risk Assessment risk stratifications [31, 32]. The commonly used variables are prostate-specific antigen (PSA), Gleason score, and clinical T/N/M stage to divide patients into now practiced three risk categories of low, intermediate, and high risk [32]. Thus, PSMA PET/CT can help direct risk stratification and monitoring by more accurately identifying localized tumors (T), nodal metastases (N), and distal metastases (M) for clinician management [33]. PSMA PET imaging of PCa has potential equivocal findings and interpretive pitfalls, as with any other imaging test [34].
Currently, several reporting guidelines have been suggested (Prostate Cancer Molecular Imaging Standardized Evaluation [PROMISE], Prostate-specific Membrane Antigen Reporting and Data System [PSMA-RADS], European Association of Nuclear Medicine-Prostate-Specific Membrane Antigen [E-PSMA]), which vary in reporting details; however, none are utilized in the community practice setting (Supplemental Table 3) [2, 34, 35]. The reasons for this lack of utilization in the community may include:
-
1.
None of the current reporting guidelines developed have been officially adopted among radiological or clinical societies and, as a result, their use has been largely limited to imaging experts in academic circles or clinical research.
-
2.
With no single source, a number of different PSMA imaging guidelines have been created and are available; moreover, the volume of information within each guideline is extensive and can be difficult to navigate.
-
3.
The available guidelines are directed more towards academic imaging experts, and their terminology and technical details may be less familiar or useful to the community imaging experts and clinicians. Moreover, community radiologists can often face greater time pressures due to higher patient loads and may prioritize the need to maximize throughput over implementing an additional protocol.
Nonetheless, community physicians, including imaging experts and referring providers, would greatly benefit from disseminating a standardized, easily communicated reporting template as the PSMA technology grows and becomes increasingly applicable to the clinical management of patients.
To this end, we developed a practical, multidisciplinary, and downloadable template for PSMA image reporting to overcome these barriers and augment the implementation of a standardized PSMA imaging guideline within the community setting. Moreover, unlike the other templates, this template was developed with the input of an expert panel that includes the input from community radiologists in order to properly hone the most clinically relevant reporting information in a community clinical setting.
Methods
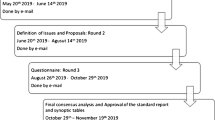
An independent, multidisciplinary panel of global expert physicians involved in PCa patient care (including radiologists, medical oncologists, nuclear medicine physicians, radiation oncologists and urologists from both academic institutions and community practices) convened throughout several meetings to discuss current reporting practices across institutions and countries. Panel participants identified the gaps and implementation of PSMA PET guidelines to aid the understanding of current practices across settings. Common themes, data elements, and their relationship to prognostication and relevance to treatment consideration were identified, from which a concise set of reporting criteria deemed most relevant across a multidisciplinary platform intended to aid patient management decisions was agreed upon in the context of PSMA PET/CT imaging. The main output was the development of an easily implementable, user-friendly, standard PSMA PET/CT reporting template with the minimum necessary information, for radiologists and nuclear medicine physicians to provide to referring physicians. Results from panel participant discussions are presented.
Results
Template components
Clinical history & procedure
Panel participants agreed the imaging report should begin with a standardized description of pertinent clinical history, similar to other existing guidelines. Clinical history should include the diagnosis and reason(s) for the referral (primary staging, BCR/ restaging, or PSMA target expression assessment for PSMA-targeted therapy). Relevant oncological history is an essential aspect when reviewing each patient and to minimize the need for freehand text, checkboxes of common treatment options were incorporated to facilitate rapid review. A comparison or prior PSMA PET/CT scans (if available) is critical for assessing the progression or regression of disease overtime and included in the template. Date of initiation of ongoing or concurrent therapy with type of therapy should be noted. The results of relevant diagnostic tests, especially PSA level, should be summarized. Procedural and technical details should include the type and dosage of radiopharmaceutical, injection time, PET acquisition time and field of imaging (Fig. 1). Imaging acquisition should begin at the proximal thighs and proceed cranially to skull base or vertex.

PSMA PET/CT image reporting template
Interpretation & reporting considerations
Since normal and variable PSMA-targeted radiopharmaceutical uptake can be found in lacrimal/salivary glands, liver, spleen, kidney, digestive tract, ureters, and bladder [2, 24], imaging experts should consider potential false positive findings where increased PSMA uptake is considered normal. In addition, the radiopharmaceutical uptake level relative to the background is important in patients that may be candidates for systemic PSMA-targeted radiopharmaceutical therapy [36]. Thus, background reference uptake for parotid glands, liver, and blood pool was included as part of this image reporting template.
In the general review, attention should be paid to the presence of lesions and, if present, their size, location, and SUVmax; regions that may relate to any symptoms or pathology noted on the referral form should be given specific attention. The panel agreed that emphasis should be placed on the prostate gland/bed, seminal vesicles, pelvic lymph nodes (including external iliac, obturator, internal iliac, common iliac, and perirectal/presacral), and extra-pelvic lymph nodes (including abdominal, thoracic, supraclavicular/neck, and inguinal). Common locations for potential metastases are similarly important to decision patient management and thus, similar data should be recorded for skeletal system and visceral metastases (such as lung, liver, brain, and penis) found. These inclusion categories will similarly help direct risk stratification and monitoring by more accurately identifying localized tumors (T), nodal metastases (N), and distal metastases (M) for clinician management. The panel agreed that the presence of PSMA-negative findings and additional PSMA-positive lesions should be reported if detected on CT scan. Lastly, indeterminate findings or additional notes should be included to encompass other image reporting not represented in this template, including the option to include the miTNM code per the PROMISE (v2.0) 2023 guidelines, PROMISE, PRIMARY, and RECIP guidelines [35]. An infographic with instructions on how to approach this PSMA image reporting template, including detailed information on the purpose of each section, can be seen in Supplemental Fig. 1.
Limitations
Despite the significant advantages and clinical utility of the standardized PSMA PET/CT reporting template developed in this study, several potential limitations and sources of error should be acknowledged:
-
The challenge of variability in interpreting PSMA PET/CT scans persists, primarily due to differences in reader experience and expertise. Even with standardized reporting guidelines, the potential for discrepancies in the subjective assessment of PSMA-targeted radiopharmaceutical uptake and lesion characterization remains, which could significantly influence clinical decision-making.
-
The inherent biological variability in PSMA expression among different patients and within different tumor sites can lead to variability in imaging results, which may affect the reproducibility and accuracy of the scans.
-
There is always a potential for false-positive or false-negative findings due to the physiological uptake of PSMA-targeted radiopharmaceutical in non-prostatic tissues and benign conditions, which can be mistaken for pathological uptake.
-
The study’s reliance on expert consensus may introduce biases related to the experts’ specific clinical practices and interpretations, which might only partially represent the broader clinical community.
-
The suggested template has not yet been tested in a real-world clinical setting, which may reveal unforeseen issues and further areas for improvement.
-
Implementing this standardized template in routine clinical practice may require more support, such as additional training and potential resistance to change from established reporting practices.
It is important to address these limitations through continuous education, validation studies, and iterative refinement of the guidelines to ensure the effectiveness and broad adoption of the standardized PSMA PET/CT reporting template.
Conclusion
PSMA PET/CT is an imaging modality for PCa that can be indicated for primary staging, restaging, targeted biopsies, evaluation for PSMA-targeted therapies and monitoring treatment response in PCa. Several reporting guidelines have been developed and vary in reporting details; however, none have been officially adopted among radiological or clinical societies and are wholly underutilized by community imaging experts and referring physicians. Here, we have provided a high-level overview of PSMA PET/CT imaging and guidelines, along with the development of a standardized reporting tool by a panel of experts composing both academic and community physicians. This reporting tool is intended to complement the existing international guidelines, help understand the patient’s full clinical picture, and facilitate overall patient management. This article extends the existing body of standardized reporting guidelines for PSMA PET/CT imaging aiming at improving the clarity and quality of reporting, decreasing the ambiguity in communication of findings, and increasing precision, repeatability, and utility of the clinical decision report.
Data availability
The original contributions presented in the study are included in the article. Further enquiries can be directed to the corresponding author.
References
O’Keefe DS, Bacich DJ, Huang SS, Heston WDW. A perspective on the Evolving Story of PSMA Biology, PSMA-Based imaging, and endoradiotherapeutic strategies. J Nucl Med. 2018;59:1007–13. https://doi.org/10.2967/jnumed.117.203877.
Ceci F, Oprea-Lager DE, Emmett L, Adam JA, Bomanji J, Czernin J, et al. E-PSMA: the EANM standardized reporting guidelines v1.0 for PSMA-PET. Eur J Nucl Med Mol Imaging. 2021;48:1626–38. https://doi.org/10.1007/s00259-021-05245-y.
de Galiza Barbosa F, Queiroz MA, Nunes RF, Costa LB, Zaniboni EC, Marin JFG, et al. Nonprostatic diseases on PSMA PET imaging: a spectrum of benign and malignant findings. Cancer Imaging. 2020;20:23. https://doi.org/10.1186/s40644-020-00300-7.
Heesch A, Ortmanns L, Maurer J, Stickeler E, Sahnoun SEM, Mottaghy FM, et al. The potential of PSMA as a vascular target in TNBC. Cells. 2023;12. https://doi.org/10.3390/cells12040551.
El Fakiri M, Geis NM, Ayada N, Eder M, Eder AC. PSMA-Targeting radiopharmaceuticals for prostate Cancer therapy: recent developments and future perspectives. Cancers (Basel). 2021;13. https://doi.org/10.3390/cancers13163967.
van der Gaag S, Bartelink IH, Vis AN, Burchell GL, Oprea-Lager DE, Hendrikse H. Pharmacological optimization of PSMA-Based Radioligand Therapy. Biomedicines. 2022;10. https://doi.org/10.3390/biomedicines10123020.
Hoffman A, Amiel GE. The impact of PSMA PET/CT on modern prostate Cancer Management and decision making-the Urological Perspective. Cancers (Basel). 2023;15. https://doi.org/10.3390/cancers15133402.
Awenat S, Piccardo A, Carvoeiras P, Signore G, Giovanella L, Prior JO, et al. Diagnostic role of (18)F-PSMA-1007 PET/CT in prostate Cancer staging: a systematic review. Diagnostics (Basel). 2021;11. https://doi.org/10.3390/diagnostics11030552.
Houshmand S, Lawhn-Heath C, Behr S. PSMA PET imaging in the diagnosis and management of prostate cancer. Abdom Radiol (NY). 2023;48:3610–23. https://doi.org/10.1007/s00261-023-04002-z.
Giesel FL, Knorr K, Spohn F, Will L, Maurer T, Flechsig P, et al. Detection efficacy of (18)F-PSMA-1007 PET/CT in 251 patients with biochemical recurrence of prostate Cancer after Radical Prostatectomy. J Nucl Med. 2019;60:362–8. https://doi.org/10.2967/jnumed.118.212233.
Shaygan B, Zukotynski K, Bénard F, Ménard C, Kuk J, Sistani G, et al. Canadian Urological Association best practice report: prostate-specific membrane antigen positron emission tomography/computed tomography (PSMA PET/CT) and PET/magnetic resonance (MR) in prostate cancer. Can Urol Assoc J. 2021;15:162–72. https://doi.org/10.5489/cuaj.7268.
Rowe SP, Pienta KJ, Pomper MG, Gorin MA. Proposal for a structured reporting system for prostate-specific membrane Antigen-targeted PET imaging: PSMA-RADS Version 1.0. J Nucl Med. 2018;59:479–85. https://doi.org/10.2967/jnumed.117.195255.
Fendler WP, Eiber M, Beheshti M, Bomanji J, Calais J, Ceci F, et al. PSMA PET/CT: joint EANM procedure guideline/SNMMI procedure standard for prostate cancer imaging 2.0. Eur J Nucl Med Mol Imaging. 2023. https://doi.org/10.1007/s00259-022-06089-w.
Oruç Z, Güzel Y, Ebinç S, Kömek H, Küçüköner M, Kaplan MA, et al. Efficacy of 68Ga-PSMA PET/CT-derived whole-body volumetric parameters in predicting response to second-generation androgen receptor axis-targeted therapy, and the prognosis in metastatic hormone-refractory prostate cancer patients. Nucl Med Commun. 2021;42:1336–46. https://doi.org/10.1097/mnm.0000000000001464.
Palot Manzil FF, Kaur H, Szabados L. Gallium-68 prostate-specific membrane Antigen Positron Emission Tomography: a practical guide for radiologists and clinicians. Cureus. 2022;14:e22917. https://doi.org/10.7759/cureus.22917.
Emmett L, Papa N, Buteau J, Ho B, Liu V, Roberts M, et al. The PRIMARY score: using Intraprostatic (68)Ga-PSMA PET/CT patterns to optimize prostate Cancer diagnosis. J Nucl Med. 2022;63:1644–50. https://doi.org/10.2967/jnumed.121.263448.
Bahler CD, Green MA, Tann MA, Swensson JK, Collins K, Alexoff D, et al. Assessing extra-prostatic extension for surgical guidance in prostate cancer: comparing two PSMA-PET tracers with the standard-of-care. Urol Oncol. 2023;41:48e1. https://doi.org/10.1016/j.urolonc.2022.10.003.
Mottet N, van den Bergh RCN, Briers E, Van den Broeck T, Cumberbatch MG, De Santis M, et al. EAU-EANM-ESTRO-ESUR-SIOG guidelines on prostate Cancer-2020 update. Part 1: screening, diagnosis, and local treatment with curative intent. Eur Urol. 2021;79:243–62. https://doi.org/10.1016/j.eururo.2020.09.042.
Trabulsi EJ, Rumble RB, Jadvar H, Hope T, Pomper M, Turkbey B, et al. Optimum imaging strategies for advanced prostate Cancer: ASCO Guideline. J Clin Oncol. 2020;38:1963–96. https://doi.org/10.1200/jco.19.02757.
Garje R, Rumble RB, Parikh RA. Systemic therapy update on (177)Lutetium-PSMA-617 for metastatic castration-resistant prostate Cancer: ASCO Rapid Recommendation. J Clin Oncol. 2022;40:3664–6. https://doi.org/10.1200/jco.22.01865.
Schaeffer EM, Srinivas S, Adra N, An Y, Barocas D, Bitting R, et al. NCCN Guidelines® insights: prostate Cancer, Version 1.2023. J Natl Compr Canc Netw. 2022;20:1288–98. https://doi.org/10.6004/jnccn.2022.0063.
Crawford ED, Koo PJ, Shore N, Slovin SF, Concepcion RS, Freedland SJ, et al. A clinician’s guide to Next Generation Imaging in patients with advanced prostate Cancer (RADAR III). J Urol. 2019;201:682–92. https://doi.org/10.1016/j.juro.2018.05.164.
Eastham JA, Auffenberg GB, Barocas DA, Chou R, Crispino T, Davis JW, et al. Clinically localized prostate Cancer: AUA/ASTRO Guideline. Part III: principles of Radiation and future directions. J Urol. 2022;208:26–33. https://doi.org/10.1097/ju.0000000000002759.
Shetty D, Patel D, Le K, Bui C, Mansberg R. Pitfalls in Gallium-68 PSMA PET/CT Interpretation-A Pictorial Review. Tomography. 2018;4:182–93. https://doi.org/10.18383/j.tom.2018.00021.
Gordon IO, Tretiakova MS, Noffsinger AE, Hart J, Reuter VE, Al-Ahmadie HA. Prostate-specific membrane antigen expression in regeneration and repair. Mod Pathol. 2008;21:1421–7. https://doi.org/10.1038/modpathol.2008.143.
Adnan A, Basu SPSMA, Receptor-Based PET-CT. The basics and current Status in Clinical and Research Applications. Diagnostics (Basel). 2023;13. https://doi.org/10.3390/diagnostics13010158.
Hagens MJ, Oprea-Lager DE, Vis AN, Wondergem M, Donswijk ML, Meijer D, et al. Reproducibility of PSMA PET/CT imaging for primary staging of Treatment-Naïve prostate Cancer patients depends on the Applied Radiotracer: a retrospective study. J Nucl Med. 2022;63:1531–6. https://doi.org/10.2967/jnumed.121.263139.
Phelps TE, Harmon SA, Mena E, Lindenberg L, Shih JH, Citrin DE, et al. Predicting outcomes of Indeterminate Bone lesions on (18)F-DCFPyL PSMA PET/CT scans in the setting of high-risk primary or recurrent prostate Cancer. J Nucl Med. 2023;64:395–401. https://doi.org/10.2967/jnumed.122.264334.
Hofman MS, Hicks RJ, Maurer T, Eiber M. Prostate-specific membrane Antigen PET: clinical utility in prostate Cancer, normal patterns, pearls, and Pitfalls. Radiographics. 2018;38:200–17. https://doi.org/10.1148/rg.2018170108.
Fendler WP, Calais J, Eiber M, Flavell RR, Mishoe A, Feng FY, et al. Assessment of 68Ga-PSMA-11 PET accuracy in localizing recurrent prostate Cancer: a prospective single-arm clinical trial. JAMA Oncol. 2019;5:856–63. https://doi.org/10.1001/jamaoncol.2019.0096.
Barbosa FG, Queiroz MA, Ferraro DA, Nunes RF, Dreyer PR, Zaniboni EC, et al. Prostate-specific membrane Antigen PET: Therapy Response Assessment in metastatic prostate Cancer. Radiographics. 2020;40:1412–30. https://doi.org/10.1148/rg.2020200058.
Hanna B, Ranasinghe W, Lawrentschuk N. Risk stratification and avoiding overtreatment in localized prostate cancer. Curr Opin Urol. 2019;29:612–9. https://doi.org/10.1097/mou.0000000000000672.
Combes AD, Palma CA, Calopedos R, Wen L, Woo H, Fulham M, et al. PSMA PET-CT in the diagnosis and staging of prostate Cancer. Diagnostics (Basel). 2022;12. https://doi.org/10.3390/diagnostics12112594.
Rowe SP, Pienta KJ, Pomper MG, Gorin MA, PSMA-RADS, Version. 1.0: a step towards standardizing the interpretation and reporting of PSMA-targeted PET imaging studies. Eur Urol. 2018;73:485–7. https://doi.org/10.1016/j.eururo.2017.10.027.
Seifert R, Emmett L, Rowe SP, Herrmann K, Hadaschik B, Calais J, et al. Second Version of the prostate Cancer molecular imaging standardized evaluation Framework including response evaluation for clinical trials (PROMISE V2). Eur Urol. 2023. https://doi.org/10.1016/j.eururo.2023.02.002.
Zhao J, Hamm B, Brenner W, Makowski MR. Lesion-to-background ratio threshold value of SUVmax of simultaneous [(68)Ga]Ga-PSMA-11 PET/MRI imaging in patients with prostate cancer. Insights Imaging. 2020;11:137. https://doi.org/10.1186/s13244-020-00926-y.
Acknowledgements
The authors acknowledge the medical writing and editorial support provided by Darren Lynn at OMNI Tech Medical.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
Shadi A. Esfahani – study design, data collection, data analysis, manuscript editing. Michael Morris, Oliver Sartor, Mark Frydenberg, Stefano Fanti, Jeremie Calais, Neha Vapiwala – study design, data analysis, manuscript editing. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent to publish
Not applicable.
Competing Interests
SE – No relevant competing interests. S.A.E. is supported by NCI K08CA259626 and has received research support from Sofie Biosciences, Telix and Novartis. MM – (none). OS - Received research or grant support from Advanced Accelerator Applications, Amgen, AstraZeneca, Bayer, Constellation, Endocyte, Invitae, Janssen, Lantheus, Merck, Progenics, Tenebio; is a consultant for Advanced Accelerator Applications (AAA), Amgen, ArtBio, Astellas, AstraZeneca, Bayer, Blue Earth Diagnostics, Inc., Clarity Pharmaceuticals, Clovis, Constellation, Convergent, Dendreon, EMD Serono, Foundation Medicine, Fusion, Genzyme, Hengrui, Isotopen Technologien Meunchen, Merck, Janssen, Morphimmune, Myovant, Myriad, Noria Therapeutics, Inc., NorthStar, Novartis, Noxopharm, Progenics, POINT Biopharma, Pfizer, Sanofi, Tenebio, Telix, Tessa, Theragnostics. MF – (none). SF – Grants/honoraria/travel support from AAA, Amgen, Astellas, AstraZeneca, Bayer, Debio, GE, Immedica, Janssen, Merck, Novartis, Sofie, Telix, Associate Editor of JNM, Editor of EJNMMI. JC - Reports prior consulting activities outside the submitted work for Advanced Accelerator Applications, Blue Earth Diagnostics, CuriumPharma, GE Healthcare, Janssen, POINT Biopharma, Progenics, Radiomedix, and Telix Pharmaceuticals. He is the recipient of grants from the Prostate Cancer Foundation (2020 Young Investigator Award 20YOUN05), the Society of Nuclear Medicine and Molecular Imaging (2019 Molecular Imaging Research Grant for Junior Academic Faculty), the Philippe Foundation Inc. (New York, USA), and the ARC Foundation (France) (International Mobility Award SAE20160604150).
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Esfahani, S.A., Morris, M.J., Sartor, O. et al. Standardized template for clinical reporting of PSMA PET/CT scans. Eur J Nucl Med Mol Imaging (2024). https://doi.org/10.1007/s00259-024-06857-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s00259-024-06857-w