
Abstract
In infants without a history of trauma, subdural haemorrhages should raise the concern for an abusive head injury, particularly when they are associated with bridging vein clotting/rupture or with septations. However, non-haemorrhagic, fluid-appearing subdural collections (also called hygromas) may also be the result of abuse. Subdural collections have also been uncommonly observed in patients with benign enlargement of the subarachnoid spaces (BESS) and a few large-scale studies accurately investigate the incidence and the significance. Currently, there is a wide variation of practices in children with BESS and subdural collections. Due to the social risks associated with abuse evaluation and the perceived risk of radiation exposure, there might be a reluctance to fully evaluate these children in some centres. The diagnosis of physical abuse cannot be substantiated nor safely excluded in infants with BESS and subdural collection(s), without investigation for concomitant traumatic findings. The exact prevalence of occult injuries and abuse in these infants is unknown. In macrocephalic infants with subdural collections and imaging features of BESS, thorough investigations for abuse are warranted and paediatricians should consider performing full skeletal surveys even when fundoscopy, social work consult, and detailed clinical evaluation are unremarkable.
Similar content being viewed by others

Explore related subjects
Find the latest articles, discoveries, and news in related topics.Avoid common mistakes on your manuscript.
BESS: Nomenclature, typical clinical, and imaging findings
Benign enlargement of the subarachnoid spaces (BESS) is one of the causes of macrocephaly in infants and a self-limiting condition in most cases. It can be defined as an increased or increasing head circumference, with a widened subarachnoid space on neuroimaging and no other cause accounting for macrocephaly. In infants with a normal, small or gradually reducing head circumference percentile and widened subarachnoid spaces, the diagnosis of BESS should not be considered and other causes of brain underdevelopment or even atrophy secondary to numerous aetiologies might be considered.
BESS most commonly affects boys and the incidence is 0.4 per 1,000 live births (95% confidence interval, 0.34 to 0.46) [1, 2]. Infants with BESS present with macrocephaly (head circumference more than two standard deviations above the mean compared to international standards [3]), often above the 90th–98th percentile, at the age of 3–12 months peaking around 7 months. These children may have a family history of macrocephaly, they are born normocephalic or macrocephalic and a vast majority of them are developmentally normal both at presentation and at follow-up [4,5,6]. The enlarged subarachnoid spaces subside by 1–2 years of age while macrocephaly stabilises and persists along a curve parallel to the 95–98% curve [7]. A small percentage may show transient developmental delay [2] while a non-negligible percentage may end up with motor and verbal delays at pre-school age [8].
Benign enlargement of the subarachnoid spaces (BESS) has also been called benign familial hydrocephalus, benign external hydrocephalus, benign enlargement of the extra-axial spaces, idiopathic external hydrocephalus, benign extra-axial/extracerebral collections of infancy, extra-ventricular hydrocephalus, pseudo-hydrocephalus, benign communicating hydrocephalus, and extra-ventricular obstructive hydrocephalus [9, 10]. Subdural hygroma, benign subdural effusion, benign hygroma of infancy, although they are currently used for collections in a different space, the subdural space, are sometimes inappropriately used to describe BESS, adding to the confusion [11].
Hypotheses regarding the pathogenesis of BESS include a delayed maturation of arachnoid villi leading to defective absorption of cerebrospinal fluid (CSF) and consequent CSF accumulation in the subarachnoid spaces, and/or amplification of the physiologic imbalance between the skull and brain growth in infants between 3 months and 1 year of age [12]. Subarachnomegaly-venous congestion of infancy has recently emerged as a term to indicate the correct location of prominent CSF space and implicates venous outflow impairment as a possible pathogenetic mechanism [7]. Magnetic resonance (MR) venogram may show hypoplasia of transverse sinuses in subarachnomegalic patients [7, 13]. In infants, arachnoid granulations are not completely developed and the intradural vascular plexus is larger; these, together with meningeal lymphatic vessels in the dura matter appear to play a role in CSF absorption, although further studies are required to demonstrate age-related changes of CSF outflow in humans [14].
Typical imaging appearances in BESS include excess CSF in the subarachnoid space, overlying both frontal lobes and extending into a widened anterior interhemispheric fissure. Occasionally, widened Sylvian fissures and a normal or only slight increase in the volume of the lateral ventricles may be seen [2, 8, 10, 15, 16]. At present, there are no imaging criteria for BESS and no established cut-off values [17]. Age-dependent sinocortical, craniocortical, and interhemispheric widths above the 95th percentile are considered abnormal [18, 19]. Upper limits of normal craniocortical width have reportedly ranged from 4 to 10 mm in infants (<1 year of age) and 3.3 to 5 mm in neonates [17]. Craniocortical width of >5 mm is considered widened and >10 mm significantly widened, regardless of modality used, ultrasound (US), computed tomography (CT), or MR imaging (MRI) [15, 18,19,20,21]. In BESS, in contrast to subdural hygromas, fluid does not cause a mass effect upon the brain, vessels are elongated and cross the entire width of the enlarged subarachnoid space, without being displaced towards the gyri [21, 22]. On US, there should be no cortical flattening, no midline shift, no areas of increased echogenicity within the CSF and no visible arachnoid membrane (Fig. 1). In children with BESS, on CT and MRI images, vessels in the subarachnoid spaces appear thin, non-displaced towards the gyri, without evidence of adjacent clots (Figs. 2 and 3).

Brain ultrasound, coronal scans of a 6-month macrocephalic boy with normal psychomotor development and a family history of macrocania (both parents), diagnosed as benign enlargement of the subarachnoid spaces. a Coronal image with a 15 MHz linear probe through the anterior fontanelle shows increased cranio-cortical width (the widest vertical distance between brain surface and calvarium), increased sino-cortical width (the widest distance between lateral wall of superior sagittal sinus and cortical surface) and moderately wide interhemispheric fissure width (the widest horizontal distance between hemispheres), all ≥ 5 mm. b Colour Doppler, shows multiple vessels (arrows) traversing the subarachnoid space CCW: Cranio-cortical width SCW: Sino-cortical width IFW: interhemispheric fissure width

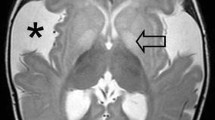
Axial brain computed tomography image of a 7-month-old boy with macrocrania and benign enlargement of the subarachnoid spaces. There is an enlargement of the subarachnoid spaces over the frontal lobes and at the interhemispheric fissure without cortical compression. Importantly, the vessels are located away from the cortical surface of the brain (arrows)

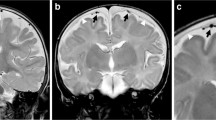
Brain magnetic resonance imaging of a 7-month-old male with a large head and seizures lasting less than 5 min. a Axial and (b) coronal T2-weighted scans show prominence of Cerebrospinal fluid (CSF) spaces over the frontal lobes with vessels traversing the entire width of the subarachnoid space (arrows). c Coronal fluid attenuation inversion recovery image shows extracerebral fluid with isointense signal compared to the CSF
Multimodality differentiation between enlarged subarachnoid spaces and subdural collections
Subdural collections can appear unicompartmental without septations exhibiting a homogeneous or heterogeneous echogenicity, density, or intensity, while multicompartmental subdural collections with septations and heterogeneous components may also occur. Different terms including haematoma, haematohygroma, chronic haematoma, and hygroma have been used in the literature to describe these imaging patterns in a subdural collection. These imaging appearances are attributed to the presence of clotted and unclotted blood, mixture of blood with CSF following bridging vein injury and arachnoid tear, and the presence of neomembranes [21].
On US, it is important to closely inspect the convexity with linear probes, colour Doppler and/or power Doppler or B-flow techniques. In BESS, a widened subarachnoid space containing crossing bridging veins is seen on colour Doppler (Fig. 1). In subdural collections, an excess line parallel to the dura, represents the arachnoid membrane which is normally not visible (Figs. 4 and 5). Moreover, the subarachnoid vessels are displaced towards or against the cortical surface, while differences in fluid echogenicity and space-occupying phenomena on the brain surface may exist (Figs. 4 and 5) [22].

A 3-month-old ex-premature boy with progressive macrocrania and normal development. On ultrasound (US), there was an incidentally discovered subdural collection, confirmed by magnetic resonance imaging (MRI). Fundoscopy, skeletal surveys, social and family history, and clinical follow-up were unremarkable. The diagnosis was subdural collection in the setting of benign enlargement of the subarachnoid spaces. a Coronal US with a high-frequency linear transducer shows enlargement of subarachnoid spaces bilaterally and an anechoic subdural collection (*) displacing the arachnoid dura (arrow) on the right. A small linear membrane was also seen on the left. b MRI 2 weeks later. Axial T2-weighted image confirms increased craniocortical width and the presence of a hyperintense subdural collection (*). c MRI, axial FLAIR image, same level as in b. The subdural collection (*) is more conspicuous and restricts the adjacent subarachnoid space. d Axial T2-weighted image at thew convexity shows normal bridging veins. e Repeat ultrasound scan on the same day shows increased echogenicity of the subdural collection (*) while the arachnoid membrane is still visible (arrow). f Coronal colour doppler US of the same area confirms lack of vessels within the collection (*)

A 3.5-month-old abused boy was shaken and thrown against the floor in public by his alcoholic father. He was brought to hospital by the police with irritability, unalert gaze, bulging anterior fontanelle, generalised hypertonia, and a head circumference above the 97th percentile. a Coronal ultrasound, showing visible arachnoid membranes bilaterally (arrows), clearly separating the pericerebral spaces into subdural and subarachnoid (between cursors) compartments. b, c Axial computed tomography scan images demonstrate convexity subdural collections with cerebrospinal fluid density (*), a hyperdense infratentorial subdural haematoma (arrow) and subarachnoid vessels displaced against the brain’s surface (arrowheads). Such imaging findings should always rise concerns for trauma and should not be misinterpreted for benign enlargement of subarachnoid spaces
On CT, subdural haematomas can be clearly identified when hyperdense and less conspicuous when isodense is related to grey matter. It can be difficult to differentiate between BESS and subdural hygromas because there might be no difference in density between CSF in BESS, almost pure CSF in hygromas (Fig. 5) and CSF mixed with few blood products in haematohygromas following rupture of the arachnoid membrane and mixture of CSF with blood [23,24,25]. It can be useful to use a subdural (blood) window which may increase the sensitivity to detect thin subdural haematomas (centre/level 50–100 HU; width 130–300 HU) [26].
On MR, this differentiation is easier because in BESS the brain is surrounded by one fluid compartment, exhibiting CSF signal intensity, containing free-traversing vessels (Fig. 5) [25]. In subdural collections/haematomas, at least two fluid compartments with different signal intensities may be seen and displaced vessels against the cortical surface are easier to identify (Fig. 6) [25, 27]. Radiologists should be aware of exceptional appearances of subdural collections in which bridging veins will remain visible with minimal displacement and subdural collections will show similar signal intensities to CSF. Utilization of T2* or susceptibility-weighted sequences for identification of blood products and routine performance of diffusion sequences for evaluation of brain cytotoxic oedema, maximize the diagnostic capabilities of this method in comparison to US and CT and should be an indispensable part of the MRI protocol in these children.

A 7-month-old ex-premature boy with progressive macrocephaly and normal development presenting with collections on ultrasound, confirmed by magnetic resonance imaging (MRI). Fundoscopy revealed retinal haemorrhages and skeletal survey revealed multiple fractures. The child was reported to authorities as physical abuse. a Coronal ultrasound with high-frequency linear transducer shows extra-axial anechoic collections (*) and vessels displaced against the brain surface (arrowhead) and below the arachnoid membrane (arrow). b-d MRI on the same day. b Axial T2-weighted sequence shows subdural hyperintense collections (*). c Axial fluid-attenuated inversion recovery image shows different intensity subdural collections. d T2* axial image shows a vessel-like structure (arrow) adjacent to a line (arrowhead), thought to represent bridging vein thrombosis and a subdural membrane, respectively
Radiologists should compare CSF density and signal intensity at the convexity to the respective density or signal intensity within the lateral ventricles to ensure they do not misinterpret bilateral symmetric hypodense subdural collections for BESS [26, 28].
Subdural collections and their significance in the setting of BESS
Subdural haemorrhagic collections in children younger than 2 years, without any medical cause or a relevant history of trauma, should always raise concern for abusive head injury and should be extensively evaluated as per international guidelines [29,30,31,32,33,34,35,36,37]. Subdural collections can occur in children with BESS either spontaneously or because of accidental trauma [15, 16, 27, 38,39,40]. The theory of BESS predisposing to isolated subdural haemorrhage implicates over-stretching of the extra-axial blood vessels following brain translocation and has been supported by a mathematical model of the cranial vault [41]. The association between a greater depth of the subarachnoid space and the increased prevalence of such collections is controversial [15, 42]. Although enlarged subarachnoid spaces can be associated with subdural collections in children with macrocrania [39], long-term observations of infants with BESS as well as a finite element study indicated no increased risk for developing subdural haematomas [11, 43].
A review of 14 relevant studies describing imaging findings in children with BESS showed that subdural collection(s) occurred in 128 out of 1,705 children with BESS (7.5%) with a varying prevalence ranging from 0 to 42.1% (Table 1) [8, 12, 15, 16, 27, 39, 42, 44,45,46,47,48,49,50]. A review of 16 relevant studies mentioning co-existence of subdural collections with BESS, showed that only 83 out of 191 children with BESS and subdural collections were further evaluated with skeletal surveys and/or fundoscopy and 28/83 (33.7%) also had concomitant injuries, including extensive retinal haemorrhages and/or fractures (Table 1) [8, 12, 15, 16, 27, 38, 39, 42, 44,45,46,47,48,49,50,51,52]. In Table 1, the different prevalence of subdural collections among infants with BESS and of concomitant suspicious injuries among different studies can be attributed to the diversity of imaging modalities with different sensitivities in the detection of subdural collections and the diversity of practices among institutions in the investigation of such children. It is important to understand that in some of these historically important publications in Table 1, images produced with CT and MRI scanners of previous generations, it might have been difficult to determine whether the enlarged extra-axial spaces were actually subarachnoid or potentially subdural. This might also factor into the prevalence range variation stated. It should also be emphasized that a visible subdural space in the context of BESS, mentioned in the recent literature as a common finding of approximately 1 mm width [50] is not a synonym for a subdural haematoma discussed herein.
In infants with macrocephaly and subdural collections, the possibility of abusive injury may be supported by the presence of concomitant suspicious injuries in various organs and sites: co-existing parenchymal injuries or cytotoxic oedema, bridging vein thrombosis/rupture, subdural collections in different locations (around right frontal lobe, around left frontal lobe, convexity, interhemispheric fissure, posterior fossa), spinal injuries (including ligamentous injuries and subdural spinal haematomas), unexplained fractures, especially classic metaphyseal lesions (CMLs), rib and skull fractures [23, 29,30,31,32, 53,54,55,56,57,58,59,60,61,62]. Skin, oral and genital stigmata are extremely important to identify, strongly supporting the hypothesis of abuse in the absence of any additional finding in a child with BESS and subdural collection(s) [63,64,65]. A relevant social history disclosing factors and conditions that might place a child at risk for maltreatment and a previous history of unexplained or frequent trauma to the same patient or household members, a delay in seeking help and a changing history are also red flags for physical abuse [10, 64]. Apnoea, loss of consciousness, and death, to our knowledge, have not been described in infants with BESS, as opposed to infants with abusive head trauma [10, 35, 53]. Indeed, the hypothesis of subdural collection in the setting of BESS does not provide explanations for the presence of the concomitant injuries described above [51].
On the other hand, the presence of a homogeneous subdural collection, without clots over the vertex in particular, with continuous bridging veins in a macrocephalic asymptomatic infant with large subarachnoid spaces, with the expected head growth curve and lack of the aforementioned concomitant suspicious injuries on craniocerebral structures, bones (including vertebrae), skin/soft tissues, fundus, etc., favours the hypothesis of BESS associated with incidental subdural collections [15, 38].
Topics requiring further studies
Non-specific signs including occasional seizures of less than 5 min duration, twitching, fussiness, crying, bulging fontanelle, and drowsiness cannot, when they are isolated, be used as discriminators between abusive head trauma and BESS with spontaneous subdural collections because they have been reported in both [9, 35, 51, 66]. It is not clearly known at present whether these signs are incidentally seen in BESS i.e., during a benign infectious intercurrent process or other neurological disease or if they can occur per se in BESS. Importantly, not only symptomatic but even asymptomatic or minimally symptomatic children with subdural collections and BESS may have concomitant injuries suspicious of abuse in up to 35% of cases when systematically screened according to the recommended protocols for suspected abuse [51]. Further studies are required to specify the severity of clinical signs and symptoms in children with subdural haemorrhages and BESS in an attempt to identify clinical discriminators and their potential association with fractures on skeletal surveys.
Macrocephaly with a fast-growing head, crossing percentiles, with a gradual or “abrupt” onset has been described in BESS [7, 17]. An abrupt onset of macrocephaly may also occur following acute abusive head trauma. The criteria for “abrupt onset” have not been yet specified in the literature. Traumatic large and bilateral subdurals may cause macrocrania and secondary enlargement of the subarachnoid spaces due to disruption of the arachnoid-dura interface, resulting in reduced CSF absorption by blocked arachnoid granulations [10, 24]. Further studies measuring head circumference with accuracy and comparing percentiles to international charts [3], may determine discriminating features of head circumference growth between the two entities, also keeping in mind that abusive head trauma may be repetitive [58].
Retinal haemorrhages have been described in approximately 85% of children with abusive head trauma and exceptionally in children with BESS [35, 67, 68]. Further studies are required to identify and clarify differences in occurrence and in imaging /fundoscopic patterns of retinal haemorrhages between the two populations.
Additional studies are required to define differences in characteristics of subdural collections in abused children with BESS compared to the subdural collections occurring in the setting of BESS following minor trauma, with regard to subdural collection depth, density on CT, or intensity on various MRI sequences and consequently stratify the risk of concomitant injuries. It is likely that the presence or absence of clots at the vertex related to the rupture of bridging veins is an important marker of severe trauma [35].
Children with BESS and subdural collections: Who should we evaluate for abuse and how?
Evidence-based guidelines regarding children with subdural collections and BESS are currently lacking. Due to perceived social risks associated with abuse evaluation and perceived risks of radiation exposure from skeletal surveys, some physicians may choose not to conduct an abuse evaluation in children with BESS, thin subdural collections, and no or minimal neurological symptoms, assuming that these infants exhibit evidence of subdural collections in the setting of BESS and cannot also be victims of abusive head trauma [16, 51]. However, it is well-known that a significant proportion of children who suffered from severe abusive head trauma have been seen previously with findings which should have required further child abuse evaluation [69, 70]. Therefore, the “better safe than sorry” approach would dictate careful multi-disciplinary team assessment, including a thorough evaluation for skin (top-to-toe examination), oral, and genital abnormalities, investigation for previous history of unexplained trauma or frequent trauma to the same patient or household members, investigation of the family environment for factors and conditions that might place the child at risk for maltreatment (social work-up), laboratory tests for bleeding diathesis, fundoscopy and further imaging with a skeletal survey in all patients [10, 30, 51]. Importantly, fundoscopy and skeletal surveys should be performed as early as possible, since relative fundoscopic findings and CMLs may heal quickly, the latter within 2 weeks, the former within a few days, and as early as 3 days, depending on type and severity [40, 61, 68]. Some paediatricians may decide not to perform skeletal surveys if the remaining investigations are unremarkable. However, a skeletal survey may reveal key finding (s) even when fundoscopy is normal [53, 58] and is particularly indicated in symptomatic children, in the previous history of unexplained or frequent trauma in the same child or other members in the child’s household and in large, compressing, clearly haemorrhagic subdural collections [10, 16, 51]. The prevalence of skeletal injuries in children with prominent subarachnoid spaces and subdural collection(s) not examined with skeletal surveys and repeat skeletal surveys, is currently unknown.
In practice, the diagnosis of physical abuse cannot be medically ruled out without the exclusion of concomitant important findings in children with BESS and subdural collections [40]. Conversely, the diagnosis of physical abuse in an infant with BESS and an isolated subdural collection, especially when asymptomatic, is presumptive [69]. Not performing the full work-up may result in an unknown possibility of missing important occult findings. Consequently, based on our current understanding, we recommend to fully evaluate all these children as per national and international guidelines including initial and follow-up skeletal surveys (Fig. 7) [37]. Whole spine MRI, if included in the protocol of suspected physical abuse (Fig. 7), may reveal thoracolumbar injuries even when spinal radiographs are unremarkable [70].

Clinical and imaging considerations in infants with macrocephaly and possible subdural collections. Children with benign enlargement of subarachnoid spaces (BESS) are more likely to be asymptomatic. Symptoms should alert physicians to the possibility of a subdural collection or another imaging finding not visible on ultrasound. CCW cranio-cortical width, SCW sino-cortical width, IFW interhemispheric fissure width, US ultrasound, CT computed tomography, MRI magnetic resonance imaging
Parents of children with BESS should be made aware of the possibility of subdural collection development and advised to take extra precautions to avoid minor trauma. This knowledge of the association of BESS and subdural collections may also alleviate unnecessary emotional trauma to parents/caregivers during interrogations to rule out abuse.
Conclusions
Subdural collections in the setting of BESS are uncommon and large-scale studies are few.
-
1.
Infants with subdural collection(s) and BESS: The diagnosis of abuse cannot be substantiated nor safely excluded without investigation for concomitant traumatic findings. The exact prevalence of occult injuries and abuse in these infants is unknown.
-
2.
Infants with subdural haemorrhages (with or without BESS): Infants should be thoroughly evaluated, including initial and follow-up skeletal surveys even when fundoscopy, social work consult, and detailed clinical evaluation are unremarkable.
Subdural haematomas in children with macrocephaly and concomitant injuries cannot be attributed to the hypothesis of BESS, particularly if there is rupture of bridging veins at the vertex. The absence of concomitant and previous injuries and a generally benign clinical course supports the hypothesis of BESS-related collections rather than abuse. As a precaution, the children with BESS and subdural collections should be clinically followed for a few months by available specialists, ideally by the child abuse paediatrician and the child protection services, even if the diagnosis of abuse is not retained.
Availability of data and material
All relevant information is already provided within the manuscript.
Code availability
Not applicable.
References
Wiig US, Zahl SM, Egge A et al (2017) Epidemiology of benign external hydrocephalus in Norway-a population-based study. Pediatr Neurol 73:36–41
Khosroshahi N, Nikkhah A (2018) Benign enlargement of subarachnoid space in infancy: a review with emphasis on diagnostic work-up. Iran J Child Neurol 12:7–15
Head circumference velocity https://www.who.int/tools/child-growth-standards/standards/head-circumference-velocity. Accessed 21 Nov 2022
Alvarez LA, Maytal J, Shinnar S (1986) Idiopathic external hydrocephalus: natural history and relationship to benign familial macrocephaly. Pediatrics 77:901–907
Castro-Gago M, Pérez-Gómez C, Novo-Rodríguez MI et al (2005) Hidrocefalia externa idiopática benigna (efusión subdural benigna) en 39 niños: evolución natural y relación con la macrocefalia familiar [Benign idiopathic external hydrocephalus (benign subdural collection) in 39 children: its natural history and relation to familial macrocephaly]. Rev Neurol 40:513–517
Wilms G, Vanderschueren G, Demaerel PH et al (1993) CT and MR in infants with pericerebral collections and macrocephaly: benign enlargement of the subarachnoid spaces versus subdural collections. AJNR Am J Neuroradiol 14:855–860
Sainz LV, Schuhmann MU (2022) Subarachnomegaly-venous congestion of infancy. Childs Nerv Syst 37:3455–3463
Yew AY, Maher CO, Muraszko KM, Garton HJL (2011) Long-term health status in benign external hydrocephalus. Pediatr Neurosurg 47:1–6
Hellbusch LC (2007) Benign extracerebral fluid collections in infancy: clinical presentation and long-term follow-up. J Neurosurg 107:119–125
Caré MM (2021) Macrocephaly and subdural collections. Pediatr Radiol 51:891–897
Wittschieber D, Karger B, Niederstadt T et al (2015) Subdural hygromas in abusive head trauma: pathogenesis, diagnosis, and forensic implications AJNR 36:432–439.
Marino MA, Morabito R, Vinci S et al (2014) Benign external hydrocephalus in infants. A single centre experience and literature review. Neuroradiol J 27:245–250
Cinalli G, di Martino G, Russo C et al (2021) Dural venous sinus anatomy in children with external hydrocephalus: analysis of a series of 97 patients. Childs Nerv Syst 37:3021–3032
Proulx ST (2021) Cerebrospinal fluid outflow: a review of the historical and contemporary evidence for arachnoid villi, perineural routes, and dural lymphatics. Cell Mol Life Sci 78:2429–2457
Tucker J, Choudhary AK, Piatt J (2016) Macrocephaly in infancy: benign enlargement of the subarachnoid spaces and subdural collections. J Neurosurg Pediatr 18:16–20
McKeag H, Christian CW, Rubin D et al (2013) Subdural hemorrhage in pediatric patients with enlargement of the subarachnoid spaces. J Neurosurg Pediatr 11:438–444
Zahl SM, Egge A, Helseth E, Wester K (2011) Benign external hydrocephalus: a review, with emphasis on management. Neurosurg Rev 34:417–432
Libicher M, Tröger J (1992) US measurement of the subarachnoid space in infants: normal values. Radiology 184:749–751
Lam WW, Ai VH, Wong V, Leong LL (2001) Ultrasonographic measurement of subarachnoid space in normal infants and children. Pediatr Neurol 25:380–384
Prassopoulos P, Cavouras D, Golfinopoulos S, Nezi M (1995) The size of the intra- and extraventricular cerebrospinal fluid compartments in children with idiopathic benign widening of the frontal subarachnoid space. Neuroradiology 37:418–421
Wittschieber D, Karger B, Pfeiffer H, Hahnemann ML (2019) Understanding subdural collections in pediatric abusive head trauma. Am J Neuroradiol. https://doi.org/10.3174/ajnr.a5855
Veyrac C, Couture A, Baud C (1990) Pericerebral fluid collections and ultrasound. Pediatr Radiol 20:236–240
Orrù E, Calloni SF, Tekes A et al (2018) The child with macrocephaly: differential diagnosis and neuroimaging findings. AJR 210:848–859
Zouros A, Bhargava R, Hoskinson M, Aronyk KE (2004) Further characterization of traumatic subdural collections of infancy. Report of five cases. J Neurosurg 100:512–518
Wittschieber D, Karger B, Niederstadt T et al (2015) Subdural hygromas in abusive head trauma: pathogenesis, diagnosis, and forensic implications. AJNR 36:432–439
Knipe H, Toumpanakis D, Hacking C et al CT head (subdural window). Reference article, Radiopaedia.org (Accessed on 21 Nov 2022) https://doi.org/10.53347/rID-48361
Wilms G, Vanderschueren G, Demaerel PH et al (1993) CT and MR in infants with pericerebral collections and macrocephaly: benign enlargement of the subarachnoid spaces versus subdural collections. AJNR 14:855–860
Meybodi KT, Habibi Z, Nejat F (2020) Temporary exacerbation of benign external hydrocephalus following minor head trauma. Childs Nerv Syst 36:2603–2604
Paine CW, Scribano PV, Localio R, Wood JN (2016) Development of guidelines for skeletal survey in young children with intracranial hemorrhage. Pediatrics 137:e20153024
Kemp AM, Jaspan T, Griffiths J et al (2011) Neuroimaging: what neuroradiological features distinguish abusive from non-abusive head trauma? A systematic review. Arch Dis Child 96:1103–1112
Kemp AM (2002) Investigating subdural haemorrhage in infants. Arch Dis Child 86:98–102
Maguire SA, Kemp AM, Lumb RC et al (2011) Estimating the probability of abusive head trauma: a pooled analysis. Pediatrics 128:e550–e564
Greeley CS (2015) Abusive head trauma: a review of the evidence base. AJR 204:967–973
Wootton-Gorges SL, Soares BP, Alazrakin AL et al (2017) ACR appropriateness criteria ® suspected physical abuse—child. J Am Coll Radiol 14:S338–S349
Choudhary AK, Servaes S, Slovis TL et al (2018) Consensus statement on abusive head trauma in infants and young children. Ped Rad 48:1048–1065
Kelly P, John S, Vincent AL et al (2015) Abusive head trauma and accidental head injury: a 20-year comparative study of referrals to a hospital child protection team. Arch Dis Child 100:1123–1130
The Royal College of Radiologists, The Royal College of Paediatrics and Child Health, The Society and College of Radiographers (2018) The radiological investigation of suspected physical abuse in children. London. https://www.rcr.ac.uk/system/files/publication/field_publication_files/bfcr174_suspected_physical_abuse.pdf. Accessed 8 Feb 2023
McNeely PD, Atkinson JD, Saigal G et al (2006) Subdural hematomas in infants with benign enlargement of the subarachnoid spaces are not pathognomonic for child abuse. AJNR 27:1725–1728
Greiner MV, Richards TJ, Care MM, Leach JL (2013) Prevalence of subdural collections in children with macrocrania. AJNR 34:2373–2378
Vinchon M, Delestret I, Defoort-Dhellemmes S et al (2010) Subdural hematoma in infants: can it occur spontaneously? Data from a prospective series and critical review of the literature. Childs Nerv Syst 26:1195–1205
Papasian NC, Frim DM (2000) A theoretical model of benign external hydrocephalus that predicts a predisposition towards extra-axial hemorrhage after minor head trauma. Pediatr Neurosurg 33:188–193
Holste KG, Wieland CM, Ibrahim M et al (2022) Subdural hematoma prevalence and long-term developmental outcomes in patients with benign expansion of the subarachnoid spaces. J Neurosurg Pediatr 11:1–7
Raul JS, Roth S, Ludes B, Willinger R (2008) Influence of the benign enlargement of the subarachnoid space on the bridging veins strain during a shaking event: a finite element study. Int J Legal Med 122:337–340
Mori K, Sakamoto T, Nishimura K, Fujiwara K (1993) Subarachnoid fluid collection in infants complicated by subdural hematoma. Child Nerv System 9:282–284
Alper G, Ekinci G, Yilmaz Y et al (1999) Magnetic resonance imaging characteristics of benign macrocephaly in children. J Child Neurol 14:678–682
Laubscher B, Deonna T, Uske A, van Melle G (1990) Primitive megalencephaly in children: natural history, medium term prognosis with special reference to external hydrocephalus. Eur J Pediatr 149:502–507
Ghosh PS, Ghosh D (2011) Subdural hematoma in infants without accidental or nonaccidental injury: benign external hydrocephalus, a risk factor. Clin Pediatr (Phila) 50:897–903
Haws ME, Linscott L, Thomas C et al (2017) A retrospective analysis of the utility of head computed tomography and/or magnetic resonance imaging in the management of benign macrocrania. J Pediatr 182:283-289.e1
Lee HC, Chong S, Lee JY et al (2018) Benign extracerebral fluid collection complicated by subdural hematoma and fluid collection: clinical characteristics and management. Childs Nerv Syst 34:235–245
Alshareef M, Tyler M, Litts C et al (2022) Prevalence of visible subdural spaces in benign enlargement of subarachnoid spaces in infancy: a retrospective analysis utilizing magnetic resonance imaging. World Neurosurg 164:e973–e979
Hansen JB, Frazier T, Moffatt M et al (2018) Evaluations for abuse in young children with subdural hemorrhages: findings based on symptom severity and benign enlargement of the subarachnoid spaces. J Neurosurg Pediatr 21:31–37
Ravid S, Maytal J (2003) External hydrocephalus: a probable cause for subdural hematoma in infancy. Pediatr Neurol 28:139-41
Piteau SJ, Ward MG, Barrowman NJ, Plint AC (2012) Clinical and radiographic characteristics associated with abusive and nonabusive head trauma: a systematic review. Pediatrics 130:315–323
Caré MM (2022) Parenchymal insults in abuse-a potential key to diagnosis. Diagnostics (Basel) 12:955
Hahnemann ML, Kinner S, Schweiger B et al (2015) Imaging of bridging vein thrombosis in infants with abusive head trauma: the “Tadpole Sign.” Eur Radiol 5:299–305
Adamsbaum C, Rambaud C (2012) Abusive head trauma: don’t overlook bridging vein thrombosis. Pediatr Radiol 42:1298–1300
Zuccoli G, Khan AS, Panigrahy A et al (2017) In vivo demonstration of traumatic rupture of the bridging veins in abusive head trauma. Pediatr Neurol 72:31–35
Adamsbaum C, Grabar S, Mejean N, Rey-Salmon C (2010) Abusive head trauma: judicial admissions highlight violent and repetitive shaking. Pediatrics 126:546–555
Choudhary AK, Ishak R, Zacharia TT, Dias MS (2014) Imaging of spinal injury in abusive head trauma: a retrospective study. Pediatr Radiol 44:1130–1140
Orman G, Kralik SF, Desai NK et al (2022) An in-depth analysis of brain and spine neuroimaging in children with abusive head trauma: beyond the classic imaging findings. AJNR 43:764–768
Marine MB, Forbes-Amrhein MM (2021) Fractures of child abuse. Pediatr Radiol 51:1003–1013
Offiah A, van Rijn RR, Perez-Rossello JM, Kleinman PK (2009) Skeletal imaging of child abuse (non-accidental injury). Pediatr Radiol 39:461–470
Hobbs CJ, Bilo RAC (2009) Nonaccidental trauma: clinical aspects and epidemiology of child abuse. Pediatr Radiol 39:457–460
Stray-Pedersen A, Vollmer-Sandholm MJ, Aukland SM et al (2022) Re-evaluation of abusive head trauma in Norway appears flawed. Acta Paediatr 111:793–797
Ludwig S, Warman M (1984) Shaken baby syndrome: a review of 20 cases. Ann Emerg Med 13:104–107
Togioka BM, Arnold MA, Bathurst MA et al (2009) Retinal hemorrhages and shaken baby syndrome: an evidence-based review. J Emerg Med 37:98–106
Piatt JH (1999) A pitfall in the diagnosis of child abuse: external hydrocephalus, subdural hematoma, and retinal hemorrhages. Neurosurg Focus 7:E5
Pierre-Kahn V, Roche O, Dureau P et al (2003) Ophthalmologic findings in suspected child abuse victims with subdural hematomas. Ophthalmology 110:1718–1723
Pittman T (2003) Significance of a subdural hematoma in a child with external hydrocephalus. Pediatr Neurosurg 39:57–59
Karmazyn B, Reher TA, Supakul N et al (2022) Whole spine MRI in children with suspected abusive head trauma. AJR 218:1074–1087
Funding
Open access funding provided by HEAL-Link Greece.
Author information
Authors and Affiliations
Contributions
All authors listed in this manuscript fulfill the ICMJE recommendations for authorship.
Study concepts and design-ACO and MR
Guarantor of integrity of the study -ACO
Literature research -MR, RvR
Clinical studies -n/a
Experimental studies /data analysis -n/a
Statistical analysis -n/a
Primary write-up of the manuscript: MR
Reviewing and editing the manuscript: All authors (MR, CA, MIA, AKC, AJ, KM, IM, RvR, ACO)
Approval of final manuscript: All authors (MR, CA, MIA, AKC, AJ, KM, IM, RvR, ACO)
Corresponding author
Ethics declarations
Conflicts of interest
None
Ethics approval
Ethical approval was not required for this collective opinion piece regarding the management of children with BESS and subdural collections.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Raissaki, M., Adamsbaum, C., Argyropoulou, M.I. et al. Benign enlargement of the subarachnoid spaces and subdural collections—when to evaluate for abuse. Pediatr Radiol 53, 752–767 (2023). https://doi.org/10.1007/s00247-023-05611-y
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00247-023-05611-y