
Abstract
Metabolic bone disease of prematurity is characterised by disordered bone mineralisation and is therefore an increased fracture risk. Preterm infants are especially at risk due to incomplete in utero bone accretion during the last trimester. Currently, diagnosing metabolic bone disease mainly relies on biochemistry and radiographs. Dual-energy x-ray absorptiometry and quantitative ultrasound (US) are used less frequently. However, biochemical measurements correlate poorly with bone mineralisation and although scoring systems exist for metabolic bone disease, radiographs are subjective and do not detect early features of osteopenia. Dual energy x-ray absorptiometry is the reference standard for determining bone density in older children and adults. However, challenges with this method include movement artefact, difficulty scanning small and sick infants and a lack of normative data for young children. Quantitative US has a relatively low cost, is radiation-free and portable, and may hence be suitable for assessing bone status in preterm infants. This review aims to provide an overview of the use of quantitative US in detecting metabolic bone disease in preterm infants.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Metabolic bone disease and osteogenesis imperfecta are the two most common causes of fragile bones in infancy [1]. Metabolic bone disease is characterised by skeletal demineralisation and fractures that can occur during normal handling [2]. The in utero process of bone accretion increases exponentially during the last trimester of pregnancy [3]. Preterm infants are, therefore, deprived of this period of mineral accumulation, have low skeletal mineral stores and are predisposed to developing metabolic bone disease [4].
Other factors that increase their risk of metabolic bone disease include comorbidity, immobility and the use of drugs such as steroids and loop diuretics [3]. Concurrent use of total parenteral nutrition with an inadequate mineral content to match the infant’s higher metabolic demand leads to abnormal bone remodeling and metabolic bone disease [2, 4].
In a recent study, 30.9% of extremely low birth weight infants had radiologic evidence of metabolic bone disease [5]. In the short term, metabolic bone disease may impair the infant’s respiratory status and may be a factor in the development of myopia of prematurity associated with impaired growth of the skull [4]. These infants are also more at risk of fractures beyond the neonatal period, especially during the first 2 years of life [6]. In the same study, about a third of infants with metabolic bone disease developed spontaneous bone fractures [5].
In adolescence, former preterm infants tend to be shorter and lighter for their age and have been reported to have lower bone mass, bone mineral content, bone density and cortical cross-sectional area [4, 7, 8]. Despite the use of mineral-enriched preterm formulas, advances in intensive neonatal care and a reduction in the use of steroids and diuretics, metabolic bone disease remains a significant comorbidity. It has been reported that the incidence of metabolic bone disease in very low birth weight infants and extremely low birth weight infants is 32% and 54%, respectively, and that 10% of very low birth weight infants may be at risk for fractures [9, 10].
Considering these short- and long-term complications of poor neonatal bone health and the increasing survival rates for very low and extremely low birth weight preterm infants, an improved method of assessing bone health is necessary.
Current assessment of bone health
Currently, metabolic bone disease diagnosis relies on biochemical evaluation and radiologic investigation [3]. Biochemical measurements include serum or urinary phosphate, serum calcium and alkaline phosphatase [4]. A raised alkaline phosphatase and low serum phosphate may indicate metabolic bone disease. However, biochemical features correlate poorly with bone mineralisation and may not be consistent indicators of bone strength or mineralisation [6]. Conventional radiographs may be used to look for osteopenia or fractures and to grade metabolic bone disease [10]. However, radiographs are poor at diagnosing mild bone disease and radiologic features of osteopenia only become reproducibly apparent after 30–40% of mineral loss [2, 4].
Dual energy x-ray absorptiometry (DXA) is used to determine bone mineral density, which correlates with bone mineralisation and bone mineral content. DXA is the gold standard in adults and children. However, the lack of portable machines and the small size of (preterm) neonates and infants (who may be very ill) pose challenges for its use [4]. Furthermore, data from DXA scans are difficult to interpret in newborns due to movement artefact and variations in technique [4]. Overall, it is also relatively expensive [7]. Another important limitation of DXA is that it measures bone in just two dimensions, thus only providing an estimate of bone mineral density, which in children is highly variable because of changes in bone geometry with growth. Scientists have not agreed on a mathematical formula to fully account for differences in bone size [11].
The main advantages of DXA are its wide availability, short scanning times and low radiation dose [11].
Assessing bone health and/or diagnosing metabolic bone disease in the preterm infant remains difficult as there is no screening test that is both specific and sensitive. Biochemical indices are not diagnostic, radiographs have low sensitivity, and DXA is impractical for routine use and of questionable reliability [4].
Quantitative ultrasonography
Quantitative ultrasonography (US) was developed in 1984 as a non-ionising, portable and low-cost alternative to conventional methods of measuring bone health [4]. Quantitative US follows the principle that velocity of transmission and amplitude are influenced when a US wave is propagated through bone [11]. Many quantitative US devices are specific to only one skeletal site, such as the calcaneum or tibia. A US transducer and receiver are placed at opposite ends of the bone. The US wave passes through the area of interest and parameters such as speed of sound (speed of propagation of US wave through bone) and bone transmission time (time taken for ultrasonic wave to pass through bone) are recorded [4]. Speed of sound increases and bone transmission time decreases with an increase in bone density and strength. The parameters reflect bone density, architecture and elasticity, including qualitative bone properties such as bone mineralisation and quantitative properties such as cortical thickness, elasticity and microarchitecture, providing a more complete picture of bone health as compared to current assessment techniques [4, 11]. This is useful in preterm infants because qualitative bone properties may be affected in addition to bone mineral density, further predisposing them to metabolic bone disease [3].
Quantitative US techniques can be applied to peripheral sites, are safe, easy to use and cost effective; the devices are portable and only a few minutes are needed to perform the measurements at the bedside. These characteristics make it favourable for use in assessing bone status in children [11].
In vitro studies have shown that forearm quantitative US variables correlate significantly with bone strength, and these parameters have been found to correspond to bone mineral assessment by DXA in children [7]. Results have demonstrated that quantitative US devices adapted for children can be used as frequently as DXA to estimate bone mineral status and bone fragility, but current data are not sufficient to establish which of them is the best choice [11]. This review will evaluate the potential of quantitative US as an important tool in the diagnosis, management and follow-up of metabolic bone disease in preterm infants. In this review, we evaluate studies that have used a total of four commercially available quantitative US devices: Omnisense 7000P (Sunlight Medical Inc., Tel Aviv, Israel), DBM Sonic (IGEA, Capri, Italy), DBM Bone Profiler (IGEA, Capri, Italy) and Osteoson KIV (Minhorst, Medut, Germany).
Search strategy
For literature analysis we used the Critical Appraisal Skills Programme tool [12]. A systematic search (Fig. 1) was performed of Medline and Embase (Table 1). Reference lists from identified studies were hand-searched to identify further relevant studies. No time limits were applied. Unpublished data such as conference proceedings were not included. Articles not written in English were excluded. Twenty-nine papers were included and are summarised in Table 1. The Critical Appraisal Skills Programme tool [12] was also used to assess the quality of these papers and is shown in Table 2.

Identification and inclusion of articles for analysis
Analysis
Feasibility
Twenty-eight studies reported successful scanning of all study subjects including premature and very low birth weight infants, while one study reported a proportion of failed scans. Quantitative US appeared well-tolerated, had no adverse side effects, and was appropriate for use for both single and serial scans. Fewtrell et al. [25] reported failed scans, due to technical problems. In that study, 17 of 99 patients had at least one failed scan and 4 patients had no successful scans at all. There were no clinical features or patterns related to the failed scans, but it was suggested that oedema from illness or fat deposition from rapidly growing infants could be affecting scan success.
Reproducibility
Reproducibility of the technique (as mentioned in 11 studies) is summarised in Table 3. Intraobserver coefficient variant, interobserver coefficient variant and instrumental precision coefficient variant were all less than 2%. Instrumental precision reported for Omnisense 7000P is 0.25–0.5%.
No significant differences were found in readings taken from different anatomical sites [2]. The ability to take measurements from various sites has significant potential advantages and the absence of large differential measurement errors between sites is important.
Quantitative US values
Table 1 summarises the equipment used and speed of sound values in the 29 reviewed studies. Most studies (23) used Omnisense 7000P at the tibial site, and their values were comparable for the term and preterm populations.
Speed of sound and gestational age
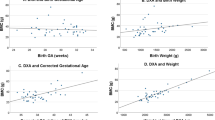
Regardless of quantitative US equipment used, a positive correlation was found between speed of sound values and gestational age, with term infants having higher speed of sound values than preterm infants reflecting the increased maturity of their bones. It is to be noted that significant correlation does not mean diagnostic accuracy in any of the presented results.
Ashmeade et al. [7] found a positive correlation between speed of sound and gestational age in preterm but not in term infants. Similarly, Zuccotti et al. [13] found no correlation between gestational age and speed of sound values in term infants. Conversely, Tansug et al. [14] suggested that speed of sound and gestational age are positively correlated when reviewing values from preterm and term infants as a whole, but the correlation did not seem to apply to the preterm group alone. The small sample size (three infants with gestational age <28 weeks) could be the reason for this finding.
Postnatal trend of speed of sound values
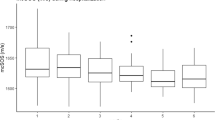
Postnatal speed of sound values decrease in preterm infants. A similar decrease has been seen in term infants [15,16,17]. This is mentioned in 14 studies and summarised in Table 4. As postnatal age increases, speed of sound values decrease despite overall growth, as shown by limb length and biochemical markers [18]. The rate of decline in speed of sound values is related to the prematurity of the infant, with most preterm infants having the steepest decline in speed of sound values [7, 17, 19]. This trend seems counterintuitive as one would expect bone density and strength to increase as infants grow. This may be because the postnatal trend of speed of sound values in preterm infants differs from that of term infants, and quantitative US is able to reflect a decline in either quantitative or qualitative bone properties despite linear growth.
Catch-up growth
Catch-up growth of preterm infants has been documented from longitudinal studies. This is shown by the postnatal equalising of speed of sound values between preterm and term infants. McDevitt et al. [8] reported that catch-up in speed of sound values is independent of postnatal growth and occurs in most infants by 6 months. The fastest rate of catch-up in speed of sound values was seen in infants who had the lowest initial speed of sound. This finding agrees with Tansug et al. [14], who demonstrated no significant difference in speed of sound values between term and preterm infants by month 12. A similar catch-up phenomenon was seen for metacarpal bone transition time in the preterm cohort in Ritschl et al. [17]. In this study, metacarpal bone transmission time values were stable for the term cohort, and the preterm cohort displayed increasing metacarpal bone transmission time values after birth, reaching the values of term infants at around 6 months of life [17].
Anthropometry
There are contradicting reports on whether speed of sound values are positively correlated, negatively correlated or not significantly correlated to birth weight. This is evaluated in 19 studies and summarised in Table 5. In Tansug et al. [14], Day 10 speed of sound values correlated with birth weight when considering both preterm and term infants as a whole, but when looking at preterm infants alone, there was no significant correlation. However, as previously alluded to, a limitation is the small number of preterm births included in this study. Zuccotti et al. [13] only looked at term infants and found no relation between weight and speed of sound values. In Ashmeade et al. [7], there was a significant positive correlation between speed of sound measurements and birth weight among preterm infants. In contrast, the correlation was negative in term infants. This suggests that lower rates of intrauterine growth are associated with high speed of sound values at birth.
Perhaps more interesting is the new insight into appropriate, small and large for gestational age infants and how their speed of sound values differ. Ten studies in this review have made mention of the effects of size for gestational age on speed of sound values (Table 6).
McDevitt et al. [20] found no significant difference in speed of sound values between small for gestational age and appropriate for gestational age infants of more than 32 weeks’ gestation. Younger than 32 weeks’ gestation, small for gestational age infants had higher speed of sound values than appropriate for gestational age infants. Liao et al. [19] and Altuncu et al. [21] also found no difference in speed of sound values between small for gestational age and appropriate for gestational age infants. Chen et al. [22] suggested that the higher speed of sound may be attributable to the older gestational age in small for gestational age infants compared to appropriate for gestational age infants with similar birth weight. This may show that maturity of the fetus has a larger bearing on bone speed of sound than birth weight. However, Rack et al. [23] reported lower speed of sound values in small for gestational age infants than appropriate for gestational age infants. This could be explained by a deficiency in calcium and phosphate leading to reduced placental transfer and diminished bone mineralisation in small for gestational age infants or perhaps a soft-tissue effect causing higher speed of sound values in small for gestational age infants than appropriate for gestational age infants. Mercy et al. [2] found a rapid decline in speed of sound values postnatally in small for gestational age infants as compared to appropriate for gestational age infants, while there was an upward trend for large for gestational age infants. There were no explanations provided, but it was stated that this is the first time such a trend has been reported.
In Littner et al. [24], large for gestational age infants were found to have lower speed of sound values than appropriate for gestational age infants. This finding is not reproduced in Liao et al. [19], where it was concluded that no differences in speed of sound values were found between appropriate for gestational age, small for gestational age and large for gestational age infants. Littner et al. [24] speculate that the relative lack of motion of macrosomic infants as compared to appropriate for gestational age infants may lead to lower speed of sound, as physical activity is known to enhance mineral accretion.
Biochemical bone markers
Fewtrell et al. [25], Chen et al. [26] and Tansug et al. [14] did not find any relationship between speed of sound values and the bone turnover markers serum alkaline phosphatase and serum phosphate. In Chen et al. [26], there was only a slight upward trend in alkaline phosphatase, which did not correlate with any speed of sound trends. Serum alkaline phosphatase is the sum of three isoforms from the liver, intestines and bone, as such an increase in serum alkaline phosphatase might be due to a liver dysfunction. Tansug et al. [14] explained that their findings might be because there were no infants with very low serum phosphate or high serum alkaline phosphatase in their study. As a high serum alkaline phosphatase is known to develop relatively late in the pathological process of metabolic bone disease, Fewtrell et al. [25] aimed to assess the ability of early speed of sound measurements to predict a high serum alkaline phosphatase level later on. They found that speed of sound measurements did not predict a high alkaline phosphatase. Conversely, a high serum alkaline phosphatase was also not associated with a lower final speed of sound measurement. However, this study did not consider some confounding factors, such as factors related to the severity of illness or infant characteristics such as gestational age or birth weight. Conversely, Altuncu et al. [21] found that there was an inverse correlation between alkaline phosphatase levels and tibia z score at term corrected age in preterm infants. In their study, patients with alkaline phosphatase>900 international units per litre were found to have significantly lower tibia z score for speed of sound, indicating ongoing osteoblastic activity [21].
Other studies have found significant correlations between biochemical markers and speed of sound values. McDevitt et al. [8] found that serum phosphate and speed of sound were significantly positively correlated. This correlation is replicated in Betto et al. [16], with another quantitative US parameter. The study found that metacarpal bone transmission time was correlated to serum phosphate, phosphaturia and calciuria in the third week of life and suggested that these three biochemical tests could be used in the workup of metabolic bone disease. This observation was also made in Ashmeade et al. [7] and Rack et al. [23]. Additionally, in Ashmeade et al. [7], a significant negative correlation was found at various time points between serum alkaline phosphatase and speed of sound values. This shows that serum markers in combination with longitudinal speed of sound measurements may be useful for identifying infants at risk of developing metabolic bone disease. Rack et al. [23] also found a negative correlation between serum alkaline phosphatase and quantitative US parameters. The study also measured urine calcium and phosphate concentrations and serum calcium concentration and found that none of these variables correlated with quantitative US, contrary to Betto et al. [16].
Litmanovitz et al. [18] used bone specific alkaline phosphatase and carboxy terminal cross-links telopeptide of Type-I collagen as markers of bone formation and bone resorption, respectively. They found that although there was a significant increase in bone specific alkaline phosphatase and significant decrease in carboxy terminal cross-links telopeptide of Type-1 collagen, both parameters remained within the normal range and there were no significant correlations between bone turnover markers and speed of sound.
Summary of findings
In neonates, quantitative US can be measured with Omnisense 7000P, DBM sonic and Osteon KIV devices. The measurements are well tolerated by all infants, even those in intensive care. This review did not compare the reliability of different US devices; however, the trend of speed of sound values was similar for each device. Intraobserver, interobserver and intersite precision were high in all devices. The studies reviewed showed a difference between preterm and term infants at birth, and a decreasing trend in speed of sound values in preterm infants when longitudinal measurements were taken. This may reflect either that the postnatal trend of speed of sound values in preterm infants differs from term infants, or that quantitative US is able to assess both quantitative and qualitative bone properties, and gives a more holistic picture of bone health. Catch-up growth of preterm infants has been demonstrated in longitudinal studies.
Although quantitative US is now widely used in adults in the context of osteoporosis, its use in infants and children is limited to studies of small sample size [23]. Lack of reference data, use of different quantitative US devices and assessment of different sites makes it challenging to compare the outcome between studies [27]. The correlation of quantitative US parameters with various factors mentioned in this review, for example biochemical markers and anthropometry, has not provided consistent results. The correlation between quantitative US parameters and the current gold standard assessment DXA is also lacking consistent data [22]. US reference values are available for term and preterm infants, but they are specific to the manufacturer of the device used and standardised values have not been achieved [28]. Most importantly, values for predicting or monitoring metabolic bone disease have not been established [14].
Conclusion
The noninvasive, financially viable and convenient monitoring of bone health with US might hold potential as an initial screening tool to predict metabolic bone disease but also for follow-up to review treatment efficacy and assess subsequent trends in bone health. However, the results presented in the papers we evaluated were not always concordant. More studies focusing on the association of biochemical bone markers, DXA, radiographs and quantitative US parameters will be essential in assessing the accuracy and reproducibility of quantitative US variables before widespread clinical use on neonatal units.
References
Bishop N, Sprigg A, Dalton A (2007) Unexplained fractures in infancy: looking for fragile bones. Arch Dis Child 92:251–256
Mercy J, Dilon B, Morris J et al (2007) Relationship of tibial speed of sound and lower limb length to nutrient intake in preterm infants. Arch Dis Child Fetal Neonatal Ed 92:381–385
Nemet D, Dolfin T, Wolach B et al (2001) Quantitative ultrasound measurements of bone speed of sound in premature infants. Eur J Pediatr 160:736–740
McDevitt H, Ahmed SF (2007) Quantitative ultrasound assessment of bone health in the neonate. Neonatology 91:2–11
Visawanathan S, Khasawneh W, McNelis K et al (2014) Metabolic bone disease: a continued challenge in extremely low birth weight infants. J Parenter Enter Nutr 38:982–990
Dahlenburg SL, Bishop NJ, Lucas A (1989) Are preterm infants at risk for subsequent fractures? Arch Dis Child 64:1384–1393
Ashmeade T, Pereda L, Chen M et al (2007) Longitudinal measurements of bone status in preterm infants. J Pediatr Endocrinol Metab 20:415–424
McDevitt H, Tomlinson C, White MP et al (2007) Changes in quantitative ultrasound in infants born at less than 32 weeks gestation over the first 2 years of life: influence of clinical and biochemical changes. Calcif Tissue Int 81:263–269
Vachharajani AJ, Mathur AM, Rao R (2009) Metabolic bone disease of prematurity. NeoReviews 10:402–411
Koo WKK, Gupta JM, Nayanar VV et al (1982) Skeletal changes in preterm infants. Arch Dis Child 57:447–452
Baroncelli GI (2008) Quantitative ultrasound methods to assess bone mineral status in children: technical characteristics, performance and clinical application. Pediatr Res 63:220–228
CASP UK (1993) CASP Checklists. CASP International. https://casp-uk.net/casp-tools-checklists/. Accessed 27 March 2018
Zuccotti G, Vigano A, Cafarelli L et al (2011) Longitudinal changes of bone ultrasound measurements in healthy infants during the first year of life: influence of gender and type of feeding. Calcif Tissue Int 89:312–317
Tansug N, Yildirim SA, Canda E et al (2011) Changes in quantitative ultrasound in preterm and term infants during the first year of life. Eur J Radiol 79:428–431
Gonnelli S, Montagnani A, Gennari L et al (2004) Feasibility of quantitative ultrasound measurements on the humerus of newborn infants for the assessment of the skeletal status. Osteoporos Int 15:541–546
Betto M, Gaio P, Ferrini I et al (2014) Assessment of bone health in preterm infants through quantitative ultrasound and biochemical markers. J Matern Fetal Neonatal Med 27:1343–1347
Ritschl E, Wehmeijer K, Terlizzi FD et al (2005) Assessment of skeletal development in preterm and term infants by quantitative ultrasound. Pediatr Res 58:341–346
Litmanovitz I, Dolfin T, Arnon S et al (2007) Assisted exercise and bone strength in preterm infants. Calcif Tissue Int 80:39–43
Liao XP, Zhang WL, He J et al (2005) Bone measurements of infants in the first 3 months of life by quantitative ultrasound: the influence of gestational age, season, and postnatal age. Pediatr Radiol 35:847–853
McDevitt H, Tomlinson C, White MP et al (2005) Quantitative ultrasound assessment of bone in preterm and term neonates. Arch Dis Child Fetal Neonatal Ed 90:341–342
Altuncu E, Akman I, Yurdakul Z et al (2007) Quantitative ultrasound and biochemical parameters for the assessment of osteopenia in preterm infants. J Matern Fetal Neonatal Med 20:401–405
Chen HL, Tseng HI, Yang SN et al (2012) Bone status and associated factors measured by quantitative ultrasound in preterm and full-term newborn infants. Early Hum Dev 88:617–622
Rack B, Lochmuller EM, Janni W et al (2012) Ultrasound for the assessment of bone quality in preterm and term infants. J Perinatol 32:218–226
Littner Y, Mandel D, Mimouni FB et al (2004) Decreased bone ultrasound velocity in large for gestational age infants. J Perinatol 24:21–23
Fewtrell MS, Loh KL, Chomtho S et al (2008) Quantitative ultrasound (QUS): a useful tool for monitoring bone health in preterm infants? Acta Paediatr 97(12):1625–1630
Chen HL, Lee CL, Tseng HI et al (2010) Assisted exercise improves bone strength in very low birth weight infants by bone quantitative ultrasound. J Paediatr Child Health 46:653–659
Visser F, Sprij AJ, Brus F (2012) The validity of biochemical markers in metabolic bone disease in preterm infants: a systematic review. Acta Paediatr 101:562–568
Yamazaki K (2012) Is QUS available for clinical use? Clin Calcium 22:120–123
Litmanovitz I, Dolfin T, Friedland O et al (2003) Early physical activity intervention prevents decrease of bone strength in very low birth weight infants. Pediatrics 112:15–19
Pereda L, Ashmeade T, Zaritt J et al (2003) The use of quantitative ultrasound in assessing bone status in newborn preterm infants. J Perinatol 23:655–659
Littner Y, Mandel D, Mimouni FB et al (2003) Bone ultrasound velocity curves of newly born term and preterm infants. J Pediatr Endocrinol Metab 16:43–47
Rubinacci A, Moro GE, Boehm G et al (2003) Quantitative ultrasound for the assessment of osteopenia in preterm infants. Eur J Endocrinol 149:307–315
Littner Y, Mandel D, Cohen S et al (2004) Bone ultrasound velocity of appropriately grown for gestational age concordant twins. Am J Perinatol 21:269–273
Littner Y, Mandel D, Mimouni FB et al (2005) Bone ultrasound velocity of infants born small for gestational age. J Pediatr Endocrinol Metab 18:793–797
Teitelbaum JE, Rodriguez RJ, Ashmeade TL et al (2006) Quantitative ultrasound in the evaluation of bone status in premature and full-term infants. J Clin Denistrom 9:358–362
Chen M, Ashmeade R, Carver JD (2007) Bone ultrasound velocity in small versus appropriate for gestational age preterm infants. J Perinatol 27:485–489
Ahmad I, Nemet D, Eliakim A et al (2010) Body composition and its components in preterm and term newborns: a cross-sectional, multimodal investigation. Am J Hum Biol 22:69–75
Liao XP, Zhang WL, Yan CH et al (2010) Reduced tibial speed of sound in Chinese infants at birth compared with Caucasian peers: the effects of race, gender, and vitamin D on fetal bone development. Osteoporos Int 21:2003–2011
Savino F, Viola S, Benetti S et al (2013) Quantitative ultrasound applied to metacarpal bone in infants. PeerJ 1:e141
Erdem E, Tosun O, Bayat M et al (2015) Daily physical activity in low-risk extremely low birth weight preterm infants: positive impact on bone mineral density and anthropometric measurements. J Bone Miner Metab 33:329–334
Acknowledgements
We thank Mrs. Sarah Massey for her help with the literature search.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
None
Electronic supplementary material
ESM 1
(DOC 42 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Tong, L., Gopal-Kothandapani, J.S. & Offiah, A.C. Feasibility of quantitative ultrasonography for the detection of metabolic bone disease in preterm infants — systematic review. Pediatr Radiol 48, 1537–1549 (2018). https://doi.org/10.1007/s00247-018-4161-5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00247-018-4161-5