
Abstract
Rationale
In party circuits dexamphetamine is frequently used in combination with alcohol. It is hypothesized that co-administration of dexamphetamine to alcohol might reduce the sedative effects of alcohol, but may potentiate risk-taking behaviour.
Objectives
The study was aimed at assessing the effects of alcohol, dexamphetamine and the combination of both on simulated driving and cognitive performance.
Method
Eighteen subjects participated in a randomized, crossover, placebo-controlled study employing four conditions: 10 mg dexamphetamine, 0.8 g/kg alcohol, 10 mg dexamphetamine + 0.8 g/kg alcohol, and placebo. Fundamental driving skills and risk-taking behaviour were assessed in a driving simulator. Subjects also completed vigilance and divided attention tasks, and subjective ratings.
Results
Mean BAC levels during simulated driving were between 0.91‰ and 0.64‰. Subjects using alcohol showed a significantly larger mean standard deviation of lateral position and shorter accepted gap time and distance. Use of alcohol or dexamphetamine + alcohol was associated with a higher frequency of red light running and collisions than the dexamphetamine or placebo conditions. Performance of vigilance and divided attention tasks was significantly impaired in the alcohol condition and, to a lesser degree, in the dexamphetamine + alcohol condition.
Conclusion
Single doses of 0.8 g/kg alcohol increased risk-taking behaviours and impaired tracking, attention and reaction time during a 3-h period after drinking when BACs declined from 0.9 to 0.2 mg/ml. The stimulatory effects of co-administration of dexamphetamine 10 mg were not sufficient to overcome the impairing effects of alcohol on skills related to driving.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
There is substantial evidence that consumption of psychoactive substances such as alcohol, recreative drugs and several prescription and “over-the-counter” drugs may endanger traffic safety (e.g. Movig et al. 2004; Ramaekers 1998). The aim of the European project Driving under the Influence of Drugs, Alcohol and Medicines was to establish guidelines to combat impaired driving under the influence of drugs and/or medication. Because in party circuits, amphetamine appears to be frequently used in combination with high doses of alcohol, the present study concerned the effects of a relatively high dose of alcohol in combination with dexamphetamine on driving performance. The effects of alcohol on driving performance are well documented, and impaired performance has been evidenced for blood alcohol concentrations (BAC) as low as 0.3‰, while higher BAC values are associated with sedation and consequently lowered vigilance, impaired lane keeping and risk-taking behaviour (e.g. Moskowitz and Robinson 1986). The effects of dexamphetamine on driving performance appear to be less clear. Epidemiological data indicated that use of methamphetamine, which is twice as potent as dexamphetamine, was associated with drifting out of lane, erratic driving, weaving, speeding, drifting off the road, increased risk taking and high-speed collisions (Logan 1996; Logan et al. 1998). With regard to the effects on risk-taking behaviour, some studies have reported decreases in impulsive behaviours following acute doses of 10 or 20 mg dexamphetamine (de Wit et al. 2002) and others have shown increases in impulsive behaviours (Hurst et al. 1967; Evenden and Ryan 1996). Concerning cognitive performance, De Wit et al. (2002) found that 10 or 20 mg dexamphetamine improved performance on measures of vigilance and memory, and decreased several forms of impulsive behaviour. These findings suggest that low doses of dexamphetamine may improve driving ability, although results of studies of lower oral doses dexamphetamine (e.g. 10 mg) are equivocal and subject to inter-individual variability (Newhouse et al. 1989; Mills et al. 2001; Holdstock and de Wit 2001).
Data concerning the effects of the combination of dexamphetamine and alcohol on driving ability are scarce and ambiguous. On a theoretical basis, it may be expected that dexamphetamine may reduce sedation and impairment of vigilance caused by alcohol, but may potentiate risk-taking behaviour and impaired judgement.
Moderate to higher doses of alcohol may potentiate some adverse effects of dexamphetamine, particularly increase of heart rate and blood pressure and cardiac arrhythmia risk (Higgins et al. 1988; Mendelson et al. 1995; Ghuran and Nolan 2000). Therefore, it was decided that in the present study, the lowest relevant dose of dexamphetamine (10 mg) was to be used in combination with 0.8 g/kg alcohol. The aim of the study was to assess the effects of 10 mg dexamphetamine, 0.8 g/kg alcohol, and the combination of 10 mg dexamphetamine and 0.8 g/kg alcohol on simulated driving behaviour and cognitive functioning.
Method and materials
Subjects
Eighteen subjects participated in the study. All participants were infrequent recreational users of alcohol and amphetamine-like substances, had a driving licence and had at least 2 years of driving experience. Participants were medically screened and familiarized in the driving simulator. Subjects were paid for their participation, and all participants signed an informed consent form. The study was approved by the medical ethics committee of the University Medical Center Utrecht.
Study design
The study was a double-blind, placebo-controlled study for dexamphetamine using a randomized crossover repeated measures design. The experimental study conditions were (1) 10 mg dexamphetamine (DEX), (2) 0.8 g/kg alcohol + matching placebo for dexamphetamine (ALC), (3) 10 mg dexamphetamine + 0.8 g/kg alcohol (DEX+ALC), and (4) matching placebo for dexamphetamine (PLA). The washout period between the study conditions was 7 days.
Procedure
One week before the first trial day, the subjects have been trained to perform the driving task in the simulator and the cognitive tasks. Subjects were instructed to abstain from alcohol and/or psychoactive drugs in the 24 h prior to each trial day and to use no more than two caffeinated drinks from 12 h prior to each test session. After arrival on each of the 4 trial days, subjects were screened for alcohol in breath (Dräger Alcotest 6510), drugs in urine (Triage® 8) and pH of urine. Subjects were questioned about sleep quality and length, health, abstinence from alcohol/drugs and number of caffeinated drinks within 12 h prior to the test session.
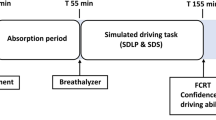
All study sessions were performed between 1400 and 2200 hours, and each subject was assessed at the same time of day, in order to standardize for circadian influences. Participants drove the TNO driving simulator, consisting of a BMW 316 car mock-up with original controls linked to a dedicated graphics computer. Participants had a 180° screen, interactive traffic, sound and a hexapod moving base. The validity to use this driving simulator for studies concerning cognitive aspects of driving behaviour has been established in subjects with various degrees of hypoglycemia (Stork et al. 2007). All scenarios for the driving simulator were developed by the University of Groningen (Veldstra et al. 2010). The simulated drive had a duration of 50 min and included urban, rural and highway driving with various traffic densities. Critical events were included at random locations. At the start of the ride, participants were instructed to drive as they would normally do unless instructed otherwise. To reduce predictability of critical events, four parallel scenarios were used.
The C max of 10 mg dexamphetamine is estimated to be 2.6 ± 2.5 h after ingestion (de Wit et al. 2000). Because it was pursued that the T max would cover the 50-min simulated driving test, the best time for the simulated ride was considered to be approximately 2 h after ingestion of dexamphetamine. Time of ingestion of dexamphetamine was then defined as T = 0. The BAC has been titrated to be 0.8 g/kg at T = 120 min, administered in three gifts according to the method described in De Wit et al. (2000). All study treatments were taken with orange juice. Each trial day tests were performed at the following experimental times:
- T = 120–170:
-
simulated driving test
- T = 180–200:
-
cognitive tasks, subjective ratings
- T = 240–260:
-
cognitive tasks, subjective ratings
- T = 300:
-
end of study sessions
Driving performance measures
During the simulated ride, performance has been assessed by measuring skills at a strategical level (speed), manoeuvring level (gap acceptance, car following, reaction to traffic light and critical situations) and control level (lateral and longitudinal control). A calibration study using the identical scenario has been performed by Veldstra et al. (2010). The driving scenario included the following features.
Road tracking task
In this part, participants drove on a 5.9-km straight road with a speed limit of 80 km/h and on a 4.8-km straight rural motorway where the speed limit was100 km/h. The drive is monotonous, and the participant is asked to drive as she/he would normally do (no specific instruction). Performance is assessed by measuring the standard deviation of the lateral position (SDLP).
Car following
The participant had to respond to the speed changes of a lead car. Performance was measured by assessing distance headway, which was calculated as the distance between the follow car and the lead car (bumper to bumper) and time headway (THW) calculated as the time interval between the two cars. Furthermore, average, SD, and minimum of time to collision (TTC), speed and lateral position were measured.
Gap acceptance
Gap acceptance measures the driver’s ability to safely traverse a crossing. The parameters included to assess risk taking are size of the accepted gap in seconds and the distance to the car approaching the driver while traversing the crossing.
Violating traffic regulations
The violations that were assessed in the virtual driving environment included violating the posted speed limit, failing to give right of way, overtaking via the emergency lane and running a red light.
Reaction to unexpected events
Three scenarios were used to measure reactions to unexpected events: a car failing to give way, a car suddenly pulling out of a car park and cars suddenly coming to a standstill on the motorway. How the driver handles these situations was assessed by measuring the deceleration and the minimal TTC (Van der Horst 1990).
Driving on the motorway
Speed and headway are considered as general indicators of driving style that have been linked to accident risk when driving on a motorway with traffic. Headway choice is measured as an indication of risky driving. The participants are faced with several scenarios: first, the participants have to filter into traffic to get onto the motorway, and second, they are driving on the motorway with normal density traffic for 15 km when suddenly the traffic comes to a standstill, from this point on the participants are driving in congested traffic for 10 km, the last 5 km is normal driving again until the participants finally leave the motorway.
Normal highway driving
The participant has to drive in normal traffic density on a two-lane motorway with a 120-km/h speed limit. Some other (virtual) traffic participants are programmed to keep to the exact posted speed limit, some drive below or above the posted speed to simulate the natural situation. How the subjects deal with this situation is assessed by measuring the number of times they change lanes and the mean and minimal THW the participant holds to other traffic participants. These above measures have been shown to be sensitive to the effects of sedative drugs (Brookhuis et al. 2004).
Cognitive performance and subjective ratings
In addition to the above-mentioned primary outcome variables, variables addressing vigilance and (divided) attention were assessed in order to evaluate the effects of alcohol and/or amphetamine. In that context, subjects performed five cognitive tasks: (1) the critical tracking task (CTT, Jex et al. 1966) measuring the ability to control a displayed error signal in a first-order compensatory tracking task; (2) divided attention task (DAT, Moskowitz 1973), assessing the ability to divide attention between two tasks; (3) the psychomotor vigilance task (PVT, Loh et al. 2004), assessing the reaction time to a visual stimulus; (4) the VigTrack, a dual-task measuring vigilance performance under the continuous load of a compensatory tracking task (Valk et al. 1997) and (5) the selective attention task from the usual field of view test (UFOV, Ball and Owsley 1992). The sequence of the different tasks was balanced over the subjects to minimize order effects. After the simulator ride, subjects completed the following subjective ratings: the Profile of Mood States (POMS, de Wit et al. 2002), Rating Scale Mental Effort (Zijlstra 1993), Driving Quality Scale (Brookhuis et al. 1985), and the nine-point Karolinska Sleepiness Scale (KSS, Reyner and Horne 1998).
Analysis
All statistical analyses were conducted by means of Statistica Data Analysis Software (StatSoft®). Treatment effects were investigated with repeated measures ANOVA. If the analysis of variance indicated a condition effect, comparisons between conditions means of the parameters were performed using planned comparison or Tukey HSD tests. Equivalence testing of drug effects was based on difference scores from placebo (within group) relative to the alcohol criterion (i.e. equivalence to a BAC of 0.8 mg/ml).
Relationships between different variables and methods were investigated by using correlational computations (Pearson product–moment or Spearman Rank correlation coefficients). In all statistical tests performed, a significance level of 0.05 was used.
Results
Subjects
Eighteen subjects were enrolled in the study. Data sets of 16 volunteers (4 female and 12 male) were available for analysis, because one subject did not wish to continue the study due to sickness on the first trial day and one subject withdrew due to medical reasons not related to the study.
Mean age of the subjects was 25.7 years (range 21–37), and mean weight was 76.1 kg (range 50.1–106.6). On average, subjects held a driving licence for 4.3 years and drove 5,600 km/year on average.
Blood alcohol concentration
Alcohol levels were measured in breath by the Dräger Alcotest 6510 (Lubeck) and transformed to BAC (Table 1). Differences between the DEX+ALC and the ALC condition were not significant.
Dexamphetamine concentration
Prior to the simulated driving test, 10 ml blood was taken by venipuncture to determine dexamphetamine levels. Blood concentrations of dexamphetamine showed no significant difference between the DEX+ALC and DEX condition and were respectively 20.7 ng/ml (range 11.9–39.1) and 20.8 ng/ml (range 11.8–40.7).
Driving performance
Road tracking: SD of lateral position
The SDLP was assessed during monotonous driving on a 5.9-km straight road with a speed limit of 80 km/h and on a 4.8-km straight motorway where the speed limit was100 km/h. Three subjects were excluded from the analysis due to off-road driving. Mean SDLP was 32% (4.9 cm) higher in the alcohol condition (ALC) than in the placebo condition (PLA). The differences between the ALC and PLA condition were significant at 80 km/h (F 1, 12 = 7.12; p < 0.02) as well as at 100 km/h (F 1, 12 = 6.49; p < 0.03). SDLP in the ALC condition was also higher than in the DEX and DEX+ALC conditions, but these differences did not reach statistical significance. Differences between DEX or DEX+ALC and the PLA condition were not significant. Results are presented in Table 2.
Speed
On a road with a posted speed of 50 km/h, a treatment effect was found on average speed (F 3, 36 = 1.92; p < 0.07, trend), SD of speed (F 3, 36 = 3.02; p < 0.04) and maximum speed (F 3, 36 = 3.86; p < 0.02). Subjects using ALC drove with higher average speed (56 km/h) than those using DEX or PLA (p < 0.05), had a higher SD of speed than in the PLA condition (p < 0.05) and drove with a higher maximum speed (63 km/h) than in the DEX and PLA conditions. A treatment effect was found for the SD of speed when driving on a 80-km/h road (F 3, 39 = 4.05; p < 0.01). Subjects with DEX+ALC showed a higher SD of speed than in the other treatments (p < 0.05). When driving on the motorway with a speed limit of 100 km/h, subjects with DEX+ALC treatment showed higher SD of speed than in other treatment conditions (F 3, 39 = 3.47; p < 0.003).
Gap acceptance
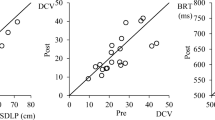
There were two city junction gap acceptance challenges with traffic coming from the left and right side (gap LR) and upcoming traffic at a Y junction (gap Y). There were no traffic lights, while road markings and a traffic sign indicated that the other traffic had the right of way. Results of the LR gap challenge are presented in Figs. 1 and 2. In both gap acceptance challenges, a significant treatment effect was found concerning accepted gap time (F 3, 42 = 5.13, p = 0.004 and F 3, 42 = 3.88, p = 0.02, respectively) and accepted gap distance (F 3, 42 = 3.87, p = 0.02 and F 3, 42 = 4.41, p = 0.009, respectively). Compared with the PLA and DEX conditions, accepted gap time and distance were significantly shorter when subjects had used ALC (p < 0.05) or DEX+ALC (p < 0.05). No significant difference was found between DEX+ALC and ALC concerning gap distance.

Gap acceptance with traffic coming from left to right side (gap LR): mean accepted gap time (in seconds). Whiskers denote standard error

Gap acceptance with traffic coming from left to right side (gap LR): mean accepted gap distance (in metres). Whiskers denote standard error
Traffic lights
Some of the traffic light scenarios were set in order to induce a dilemma for the driver, where drivers suddenly had to stop for the red light. Drivers in the DEX+ALC and the ALC conditions did not stop for the red traffic light in 64% and 59% of the cases, while in the DEX and PLA conditions drivers did not stop in 30% of the cases (chi-square = 10.8496, df = 3, p = 0.02).
Giving right of way
Participants were driving on a road towards a normal junction at a posted speed of 50 km/h. The driver coming from the right has priority over the participant. A treatment effect was found when approaching the junction where the subject had to give way (F 3, 36 = 5.53; p = 0.003). Subjects using ALC had significantly higher maximum speed approaching the junction than in the DEX (p < 0.05), DEX+PLA (p < 0.01) and PLA (p < 0.05) condition. There were two cases in which no right of way was given, and there were no significant differences between treatments concerning the number of participants coming to a standstill.
Other measures of driving behaviour
No relevant or significant differences between conditions were found concerning variables of driving behaviour when approaching a stop sign, filtering into traffic (ramp entry velocity, velocity when merging, THW and merging distance), highway driving (time to line crossing), number of line crossings, during car following scenarios (TTC, headway, THW, speed, lateral position) and the reaction to a car suddenly pulling out of a parking lay (max deceleration, TTC).
Accidents and dangerous actions
When encountering a traffic jam at the highway, traversing unsignalised crossroads or filtering into the traffic, some participants collided on a vehicle. Compared with placebo, significantly more accidents were observed in the ALC and the DEX+ALC conditions (F 1, 13 = 6.06; p < 0.03). In total there were 18 collisions, with 1 collision for DEX, 6 for DEX+ALC, 8 for ALC and 3 for the PLA condition. There were no significant differences between the DEX and PLA conditions. In two cases, both in the ALC condition, participants overtook a car by driving over the emergency lane, instead of taking over via the left lane.
Cognitive tasks
The first cognitive test session was performed with mean BACs between 0.64‰ and 0.55‰, while mean BACs during the second session were between 0.37‰ and 0.23‰. For each condition the mean of the results of the two test sessions was used to perform the statistical analysis of differences between treatments.
Divided attention task
Performance on the DAT was significantly impaired for subjects using ALC (Table 3). Compared to the other conditions, they showed a larger tracking error (F 3, 39 = 5.15; p = 0.004), higher reaction time (F 3, 39 = 4.04; p = 0.01), higher number of missed targets (F 3, 39 = 5.05; p = 0.005), a lower number of hits (F 3, 39 = 5.05; p = 0.005), higher number of control losses (F 3, 39 = 6.39; p = 0.001) and more false alarms (F 3, 39 = 4.04; p = 0.01). The number of false alarms was higher when subjects used DEX+ALC compared to DEX (p < 0.05). No relevant and/or significant correlations between DAT scores and BACs or dexamphetamine levels in blood could be demonstrated.
Vigilance and tracking test
Subjects using ALC showed significantly impaired vigilance performance compared to the other conditions. This was signified by a larger tracking error (F 3, 45 = 5.01; p = 0.004), longer reaction times (F 3, 45 = 8.38, p = 0.0002) and a higher percentage of omissions (trend: F 3, 45 = 2.55, p = 0.07). Subjects using dexamphetamine alone (DEX) showed the best performance, although this was not statistically significant. There were no relevant and/or significant correlations between VigTrack scores and BACs or dexamphetamine levels in blood.
Other cognitive tasks
The CTT and the PVT showed no significant or relevant differences between the treatments. On the selective attention task from the UFOV, no significant differences between treatments were found.
Subjective rating scales
Subjects completed the subjective rating scales immediately after ending the simulated driving test. The KSS and POMS were also completed in the second session at T = 240.
There were significant treatment effects on KSS scores (F 3, 45 = 6.82; p = 0.0007) Subjects using dexamphetamine alone (DEX) or in combination with alcohol (DEX+ALC) were less sleepy than subjects using PLA or ALC alone (p < 0.01 for both DEX and DEX+PLA).
The POMS scores showed significant treatment effects, indicating that subjects using DEX reported to feel less fatigued, more energetic, more cheerful, less depressed and more clear headed than when they had used ALC or PLA (all differences p < 0.05). Subjects using DEX showed higher subjectively estimated driving quality than those who used ALC (p < 0.05) and showed the lowest level of subjectively estimated mental effort during driving (n.s.)
Adverse effects
There were no severe adverse effects and no significant clinical or statistical differences between the different conditions concerning adverse effects, heart rate, or blood pressure. Continuous ECG monitoring revealed paroxysmal supraventricular tachycardia (SVT) in two cases using the combination of amphetamine and alcohol. Both cases of SVT were asymptomatic and recovered spontaneously.
Discussion
The aim of the present study was to assess the effects of 10 mg dexamphetamine, 0.8 g/kg alcohol, and the combination of 10 mg dexamphetamine and 0.8 g/kg alcohol on driving behaviour and cognitive functioning, using a set of measures within a scenario developed to investigate the effects of stimulants, like dexamphetamine and/or alcohol on simulated driving performance. We found that mean BAC levels between 0.9‰ and 0.6‰ alcohol significantly impaired road tracking performance, which is in agreement with literature and replicates earlier demonstration of alcohol-induced impairment of road tracking performance in actual, on-the-road driving test scenarios (Kuypers et al. 2006; Louwerens et al. 1987; Ramaekers et al. 2000). The mean differences in SDLP between the alcohol and placebo conditions found in the present study are considered to be relevant in the context of traffic safety (4.9 cm). Co-administration of dexamphetamine did not significantly change the impairing effect of alcohol as evidenced by the lack of statistical interaction between dexamphetamine and alcohol. Equivalence testing demonstrated that the 95%CI of the change in road tracking performance (i.e. SDLP) after combined use of dexamphetamine and alcohol included both the 0.8 g/kg alcohol criterion as well as the placebo reference (zero). It is therefore considered that the clinical relevance of the combined effects of 10 mg dexamphetamine and 0.8 g/kg alcohol is ambiguous, which means that some individuals may show impairment whereas others may not.
Accepted gap time and distance were significantly shorter when subjects had used alcohol or the combination of dexamphetamine with alcohol. Shorter accepted gap time and distance may be interpreted as indications of increased risk taking caused by alcohol. Such interpretation is supported by data evidencing that alcohol increases impulsive behaviour (de Wit et al. 2000). There was no difference between the effects of alcohol alone or alcohol + amphetamine.
Although the addition of 10 mg dexamphetamine appeared to reduce some impairing effects of alcohol, these effects were not significant. These findings indicate that addition of 10 mg amphetamine may not mitigate the effects of a relatively high dose of alcohol. We found only a few indications for increased risk taking associated with the combination of dexamphetamine and alcohol. The lack of evidence of increased risk taking associated with dexamphetamine may be explained by the fact that due to medical considerations, in the present study, a relatively low dose (10 mg) of dexamphetamine was used instead of higher doses which are known to cause risk-taking behaviour and impaired judgement (Simons and Valk 2000). Doses of 5–10 mg dexamphetamine are used in the US Air Force to improve performance of fatigued pilots (Emonson and Vanderbeek 1995) and are known to reduce the effects of fatigue and sleep deprivation without adverse effects such as stimulating risk-taking behaviour (Caldwell and Caldwell 1997). Therefore it is hypothesized that a dose of 10 mg dexamphetamine might have been too low to cause significant anti-sedative effects, impaired judgement and stimulation of risk-taking behaviour.
It was found that participants using 10 mg dexamphetamine alone caused the least number of collisions and less passing of red traffic lights, and showed the best performance on the divided attention and vigilance tasks. Participants using dexamphetamine alone felt less fatigued, more energetic, more cheerful, less depressed and more clear headed than in any other condition.
The stimulatory effects of dexamphetamine on human performance have been widely acknowledged, and beneficial effects on road tracking have been described (Ramaekers et al. 2006; Kuypers and Ramaekers 2005). However, previous research has also demonstrated that stimulant drugs such as amphetamine can improve tracking performance, impulse control and reaction time, while impairing working memory and movement perception (Kuypers and Ramaekers 2005; Lamers et al. 2003; Silber et al. 2005, 2006). Therefore, it should be considered that although dexamphetamine may improve some aspects of driving performance, it might have detrimental effects in other performance domains that are relevant to traffic safety.
It is known that in the ‘party circuit’ (e.g. dance parties), the amphetamine doses that are used in combination with alcohol may be much higher than the dose used in the present study. Moreover, the effects of the combination of alcohol and amphetamine used during dance parties may be potentiated by sleep deprivation. Our findings have shown that co-administration of 10 mg dexamphetamine did not significantly change the impairing effect of alcohol. Moreover, red light running and collisions, both highly dangerous driving acts, were observed significantly more frequent in the alcohol condition as well as in the alcohol + dexamphetamine condition compared to the other conditions.
Conclusion
Risk scenarios and measures employed in the present study were very sensitive to the effects of alcohol alone and to the combination of alcohol and dexamphetamine. These measures demonstrated that during simulated driving, single doses of alcohol (0.8 g/kg body weight) impaired road tracking and increased risk-taking behaviours, indicated by shorter gap acceptance time and distance and an increase of red light crossings and number of collisions, and impaired tracking, attention and reaction time during a 3-h period after drinking when BACs declined from 0.9 to 0.2 mg/ml. These alcoholic impairments were not affected by the co-administration of 10 mg dexamphetamine, indicating that the stimulatory effects of dexamphetamine were not sufficient to overcome the impairing effects of alcohol on skills related to driving. The lack of mitigating effects of dexamphetamine on alcohol-induced performance impairment may be of particular importance in terms of road safety issues. The findings of the present study justify the conclusion that individuals using alcohol, or the combination of dexamphetamine with alcohol, should not be allowed to participate in traffic.
References
Ball K, Owsley C (1992) The useful field of view test: a new technique for evaluating age-related declines in visual function. J Am Optom Assoc 63:71–79
Brookhuis KA, De Vries G, Prins van Wijngaarden P, Veenstra G, Hommes M, Louwerens JW, O'Hanlon JF (1985) The effects of increasing doses of meptazinol (100, 200, 400 mg) and glafenine (200 mg) on driving performance (Report VK 85–16). Traffic Research Centre, University of Groningen, Haren
Brookhuis KA, de Waard D, Samyn N (2004) Effects of MDMA (ecstasy), and multiple drugs use on (simulated) driving performance and traffic safety. Psychopharmacology (Berl) 173:440–445
Caldwell JA, Caldwell JL (1997) An in-flight investigation of the efficacy of dextroamphetamine for sustaining helicopter pilot performance. Aviat Space Environ Med 68:1073–1080
de Wit H, Crean J, Richards JB (2000) Effects of d-amphetamine and ethanol on a measure of behavioral inhibition in humans. Behav Neurosci 114(4):830–837
de Wit H, Enggasser JL, Richards JB (2002) Acute administration of d-amphetamine decreases impulsivity in healthy volunteers. Neuropsychopharmacology 27(5):813–825
Emonson DL, Vanderbeek RD (1995) The use of amphetamines in U.S. Air Force tactical operations during Desert Shield and Storm. Aviat Space Environ Med 66(3):260–263
Evenden JI, Ryan CN (1996) The pharmacology of impulsive behaviours in rats: the effects of drugs on response choice with varying delays of reinforcement. Psychopharmacology (Berl) 128:161–170
Ghuran A, Nolan J (2000) Recreational drug misuse: issues for the cardiologist. Heart 83:627–633
Higgins S, Capeless M, Hughes J, Bickel W, Belinson M (1988) Behavioral and cardiovascular effects of alcohol and d-amphetamine combinations in normal volunteers. In: Harris LS (ed) Problems of drug dependence, 1988. NIDA research monograph 90. US Department of Health and Human Services, Rockville, pp 35–36
Holdstock L, de Wit H (2001) Individual differences in responses to ethanol and d-amphetamine: a within subject study. Alcohol Clin Exp Res 25(4):540–548
Hurst PM, Weidner MF, Radlow R (1967) The effects of amphetamines upon judgement and decisions. Psychopharmacologia 1(5):397–404
Jex et al (1966) A critical tracking task for man-machine research related to the operator’s effective delay time. I. Theory and experiments with a first-order divergent controlled element. NASA CR-616. NASA Contract Rep NASA CR, 1–105
Kuypers KP, Ramaekers JG (2005) Transient memory impairment after acute dose of 75 mg 3.4-methylene-dioxymethamphetamine. J Psychopharmacol 19:633–639
Kuypers KP, Samyn N, Ramaekers JG (2006) MDMA and alcohol effects, combined and alone, on objective and subjective measures of actual driving performance and psychomotor function. Psychopharmacology (Berl) 187:467–475
Lamers CT, Ramaekers JG, Muntjewerff ND, Sikkema KL, Samyn N, Read NL et al (2003) Dissociable effects of a single dose of ecstasy (MDMA) on psychomotor skills and attentional performance. J Psychopharmacol 17:379–387
Logan BK (1996) Methamphetamine and driving impairment. J Forensic Sci 41(3):457–464
Logan BK, Fligner CL, Haddix T (1998) Cause and manner of death in fatalities involving methamphetamine. J Forensic Sci 43(1):28–34
Loh S et al (2004) The validity of psychomotor vigilance tasks of less than 10-minute duration. Behaviour research methods, instruments, and computers. J Psychon Soc Inc 36:339–346
Louwerens JW, Gloerich ABM, De Vries G, Brookhuis KA, O'Hanlon JF (1987) The relationship between drivers' blood alcohol concentration (BAC) and actual driving performance during high speed travel. In: Noordzij PC, Roszbach R (eds) Alcohol, drugs and traffic safety-T86. Excerpta Medica, Amsterdam, pp 183–186
Mendelson J, Jones RT, Upton R, Peyton J (1995) Methamphetamine and ethanol interactions in humans. Clin Pharmacol Ther 57(5):559–568
Mills KC, Spruill SE, Kanne RW, Parkman KM, Zhang Y (2001) The influence of stimulants, sedatives, and fatigue on tunnel vision: risk factors for driving and piloting. Hum Factors 43(2):310–327
Moskowitz H (1973) Laboratory studies of the effects of alcohol on some variables related to driving. J Saf Res 5:185–199
Moskowitz H, Robinson C (1986) Driving-related skills impairment at low alcohol levels. In: P.C. Noordzij, R. Roszbach (eds) Alcohol, drugs and traffic safety-T86. Excerpta Medica International Congress Series 721. Excerpta Medica, Amsterdam
Movig KLL, Mathijssen MPM, Nagel PHA, Van Egmond T, De Gier JJ, Leufkens HGM, Egberts ACG (2004) Psychoactive substance use and the risk of motor vehicle accidents. Accid Anal Prev 36(4):631–636
Newhouse PA, Belenky G, Thomas M, Thorne D, Sing HC, Fertig J (1989) The effects of d-amphetamine on arousal, cognition, and mood after prolonged total sleep deprivation. Neuropsychopharmacology 2(2):153–164
Ramaekers JG (1998) Behavioural toxicity of medicinal drugs. Practical consequences, incidence, management and avoidance. Drug Saf 18(3):189–208
Ramaekers JG, Robbe HW, O'Hanlon JF (2000) Marijuana, alcohol and actual driving performance. Hum Psychopharmacol 15:551–558
Ramaekers JG, Kuypers KP, Samyn N (2006) Stimulant effects of 3,4-methylenedioxymethamphetamine (MDMA) 75 mg and methylphenidate 20 mg on actual driving during intoxication and withdrawal. Addiction 101:1614–1621
Reyner LA, Horne JA (1998) Falling asleep whilst driving: are drivers aware of prior sleepiness. Int J Legal Med 111:120–123
Silber BY, Papafotiou K, Croft RJ, Ogden E, Swann P, Stough C (2005) The effects of dexamphetamine on simulated driving performance. Psychopharmacology (Berl) 179(3):536–543
Silber BY, Croft RJ, Papafotiou K, Stough C (2006) The acute effects of d-amphetamine and methamphetamine on attention and psychomotor performance. Psychopharmacology (Berl) 187:154–169
Simons M, Valk PJL (2000) Sleep and alertness management during military operations: questions to be answered. RTO-MP-31; NATO-AGARD, Neuilly-sur-Seine, France, p. 8/1-8/7
Stork ADM, van Haeften TW, Veneman TF (2007) The decision not to drive during hypoglycemia in patients with type 1 and type 2 diabetes according to hypoglycemia awareness. Diabetes Care 30(11):2822–2826
Valk PJL, Simons M, Struyvenberg PAA, Kruit J, Van Berge Henegouwen M (1997) Effects of a single dose of loratadine on flying ability under conditions of simulated cabin pressure. Am J Rhinol 11(1):27–33
Van der Horst ARA (1990) A time-based analysis of road user behaviour in normal and critical encounters. Proefschrift. Technische Universiteit, Delft
Veldstra JL, Brookhuis KA, de Waard D (2010) Dose related effects of alcohol on simulated driving performance: a calibration study. Report Department of Traffic and Environmental Psychology of the University of Groningen
Zijlstra FRH (1993) Efficiency in work behavior. A design approach for modern tools. PhD thesis, Delft University of Technology, Delft
Acknowledgements
We are greatly indebted to Janet Veldstra and Karel Brookhuis, University of Groningen, who made their driving scenario and their alcohol calibration study available for us. This work was conducted as part of the Driving under the influence of Drugs, Alcohol and Medicines (DRUID) research consortium funded by European Union grant TREN-05-FP6TR-S07.61320-518404-DRUID.
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License (https://creativecommons.org/licenses/by-nc/2.0), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
About this article
Cite this article
Simons, R., Martens, M., Ramaekers, J. et al. Effects of dexamphetamine with and without alcohol on simulated driving. Psychopharmacology 222, 391–399 (2012). https://doi.org/10.1007/s00213-011-2549-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00213-011-2549-0