
Abstract
Summary
Fragility fractures of the hip have a major impact on the lives of patients and their families. This study highlights significant geographical variation in secondary fracture prevention with even the highest performing regions failing the majority of patients despite robust evidence supporting the benefits of diagnosis and treatment.
Introduction
The purpose of the study is to describe the geographic variation in anti-osteoporosis drug therapy prescriptions before and after a hip fracture during 1999–2013 in the UK.
Methods
We used primary care data (Clinical Practice Research Datalink) to identify patients with a hip fracture and primary care prescriptions of any anti-osteoporosis drugs prior to the index hip fracture and up to 5 years after. Geographic variations in prescribing before and after availability of generic oral bisphosphonates were analysed. Multivariable logistic regression models were adjusted for gender, age and body mass index (BMI).
Results
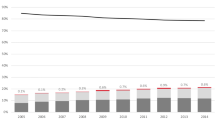
Thirteen thousand sixty-nine patients (76 % female) diagnosed with a hip fracture during 1999–2013 were identified. Eleven per cent had any anti-osteoporosis drug prescription in the 6 months prior to the index hip fracture. In the 0–4 months following a hip fracture, 5 % of patients were prescribed anti-osteoporosis drugs in 1999, increasing to 51 % in 2011 and then decreasing to 39 % in 2013.
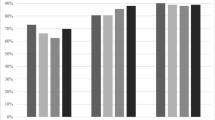
The independent predictors (OR (95 % CI)) of treatment initiation included gender (male 0.42 (0.36–0.49)), BMI (0.98 per kg/m2 increase (0.97–1.00)) and geographic region (1.29 (0.89–1.87) North East vs. 0.56 (0.43–0.73) South Central region). Geographic differences in prescribing persisted over the 5-year follow-up. If all patients were treated at the rate of the highest performing region, then nationally, an additional 3214 hip fracture patients would be initiated on therapy every year.
Conclusions
Significant geographic differences exist in prescribing of anti-osteoporosis drugs after hip fracture despite adjustment for potential confounders. Further work examining differences in health care provision may inform strategies to improve secondary fracture prevention after hip fracture.


Similar content being viewed by others
References
Abrahamsen B, van Staa T, Ariely R, Olson M, Cooper C (2009) Excess mortality following hip fracture: a systematic epidemiological review. Osteoporos Int 20:1633–1650
Cooper C, Mitchell P, Kanis JA (2011) Breaking the fragility fracture cycle. Osteoporos Int 22:2049–2050
Johnell O, Kanis JA, Oden A, Sernbo I, Redlund-Johnell I, Petterson C, De Laet C, Jonsson B (2004) Fracture risk following an osteoporotic fracture. Osteoporos Int 15:175–179
Melton LJ 3rd, Kearns AE, Atkinson EJ, Bolander ME, Achenbach SJ, Huddleston JM, Therneau TM, Leibson CL (2009) Secular trends in hip fracture incidence and recurrence. Osteoporos Int 20:687–694
Freemantle N, Cooper C, Diez-Perez A, Gitlin M, Radcliffe H, Shepherd S, Roux C (2013) Results of indirect and mixed treatment comparison of fracture efficacy for osteoporosis treatments: a meta-analysis. Osteoporos Int 24:209–217
Ross S, Samuels E, Gairy K, Iqbal S, Badamgarav E, Siris E (2011) A meta-analysis of osteoporotic fracture risk with medication nonadherence. Value Health 14:571–581
NICE (2008) Alendronate, etidronate, risedronate, raloxifene, strontium ranelate and teriparatide for the secondary prevention of osteoporotic fragility fractures in postmenopausal women. NICE technology appraisal guidance 161
Solomon DH, Johnston SS, Boytsov NN, McMorrow D, Lane JM, Krohn KD (2014) Osteoporosis Medication Use after Hip Fracture in U.S. Patients between 2002 and 2011. J Bone Miner Res
Hawley S, Leal J, Delmestri A, Prieto-Alhambra D, Arden NK, Cooper C, Javaid MK, Judge A (2016) Refresh study group Anti-Osteoporosis medication prescriptions and incidence of subsequent fracture among primary hip fracture patients in England and Wales: An Interrupted Time-Series Analysis. doi:10.1002/jbmr.2882.
Hollingworth W, Rooshenas L, Busby J et al (2015) Using clinical practice variations as a method for commissioners and clinicians to identify and prioritise opportunities for disinvestment in health care: a cross-sectional study, systematic reviews and qualitative study. Health Services and Delivery Research 3:1–172
Herrett E, Gallagher A, Bhaskaran K, Forbes H, Mathur R, van Staa T, Smeeth L (2015) Data resource profile: clinical practice research datalink (CPRD). Int J Epidemiol 44:827–836
Hawley S, Javaid MK, Prieto-Alhambra D, Lippett J, Sheard S, Arden NK, Cooper C, Judge A (2016) Clinical effectiveness of orthogeriatric and fracture liaison service models of care for hip fracture patients: population-based longitudinal study. Age Ageing 45:236–242
White IR, Royston P, Wood AM (2011) Multiple imputation using chained equations: issues and guidance for practice. Stat Med 30:377–399
Fine JPG, Gray RJ (1999) A proportional hazards model for the subdistribution of a competing risk. J Am Stat Assoc 94:496–509
Glover JA (1938) The incidence of tonsillectomy in school children: (section of epidemiology and state medicine). Proc R Soc Med 31:1219–1236
Sinner MF, Piccini JP, Greiner MA, Walkey AJ, Wallace ER, Heckbert SR, Benjamin EJ, Curtis LH (2015) Geographic variation in the use of catheter ablation for atrial fibrillation among Medicare beneficiaries. Am Heart J 169:775–782 e772
Williams MV, Drinkwater KJ (2009) Geographical variation in radiotherapy services across the UK in 2007 and the effect of deprivation. Clin Oncol (R Coll Radiol) 21:431–440
Lawlor DA, Bedford C, Taylor M, Ebrahim S (2003) Geographical variation in cardiovascular disease, risk factors, and their control in older women: British Women’s Heart and Health Study. J Epidemiol Community Health 57:134–140
Kaur B, Anderson HR, Austin J, Burr M, Harkins LS, Strachan DP, Warner JO (1998) Prevalence of asthma symptoms, diagnosis, and treatment in 12-14 year old children across Great Britain (international study of asthma and allergies in childhood, ISAAC UK). BMJ 316:118–124
Wennberg JE, Barnes BA, Zubkoff M (1982) Professional uncertainty and the problem of supplier-induced demand. Soc Sci Med 16:811–824
Skinner J, Staiger D (2015) Technology diffusion and productivity growth in health care. Rev Econ Stat 97:951–964
Reames BN, Shubeck SP, Birkmeyer JD (2014) Strategies for reducing regional variation in the use of surgery: a systematic review. Ann Surg 259:616–627
Kanis JA, Johnell O, Oden A, Johansson H, McCloskey E (2008) FRAX and the assessment of fracture probability in men and women from the UK. Osteoporosis international: a journal established as result of cooperation between the European Foundation for Osteoporosis and the National Osteoporosis Foundation of the USA 19:385–397
Hippisley-Cox J, Coupland C (2009) Predicting risk of osteoporotic fracture in men and women in England and Wales: prospective derivation and validation of QFractureScores. BMJ 339:b4229
Kanis JA, McCloskey EV, Johansson H, Strom O, Borgstrom F, Oden A (2008) Case finding for the management of osteoporosis with FRAX®—assessment and intervention thresholds for the UK. Osteoporos Int 19:1395–1408
Shepstone L, Fordham R, Lenaghan E et al (2012) A pragmatic randomised controlled trial of the effectiveness and cost-effectiveness of screening older women for the prevention of fractures: rationale, design and methods for the SCOOP study. Osteoporos Int 23:2507–2515
Javaid MK, Rai S, Schoo R, Stanley R, Vasilakis N, Tsang C (2016) Fracture Liaison Service (FLS) Database facilities audit. FLS breakpoint: opportunities for improving patient care following a fragility fracture. Royal College of Physicians, London
Hiligsmann M, Evers SM, Ben Sedrine W, Kanis JA, Ramaekers B, Reginster JY, Silverman S, Wyers CE, Boonen A (2015) A systematic review of cost-effectiveness analyses of drugs for postmenopausal osteoporosis. PharmacoEconomics 33:205–224
Services PaPC (2014) Quality and outcomes framework–prevalence, achievements and exceptions report: England, 2013–14. In Centre HaSCI (ed). Health and Social Care Information Centre
Compston J (2015) Overdiagnosis of osteoporosis: fact or fallacy? Osteoporos Int 26:2051–2054
Black DM, Cummings SR, Karpf DB et al (1996) Randomised trial of effect of alendronate on risk of fracture in women with existing vertebral fractures. Fracture Intervention Trial Research Group. Lancet 348:1535–1541
Reynolds K, Muntner P, Cheetham TC, Harrison TN, Morisky DE, Silverman S, Gold DT, Vansomphone SS, Wei R, O'Malley CD (2013) Primary non-adherence to bisphosphonates in an integrated healthcare setting. Osteoporos Int 24:2509–2517
Li L, Roddam A, Gitlin M, Taylor A, Shepherd S, Shearer A, Jick S (2012) Persistence with osteoporosis medications among postmenopausal women in the UK General Practice Research Database. Menopause 19:33–40
Klop C, Welsing PM, Elders PJ, Overbeek JA, Souverein PC, Burden AM, van Onzenoort HA, Leufkens HG, Bijlsma JW, de Vries F (2015) Long-term persistence with anti-osteoporosis drugs after fracture. Osteoporos Int 26:1831–1840
Drew S, Judge A, Cooper C, Javaid MK, Farmer A, Gooberman-Hill R (2016) Secondary prevention of fractures after hip fracture: a qualitative study of effective service delivery. Osteoporos Int
Tafaro L, Nati G, Leoni E, Baldini R, Cattaruzza MS, Mei M, Falaschi P (2013) Adherence to anti-osteoporotic therapies: role and determinants of "spot therapy". Osteoporos Int 24:2319–2323
Curtis JR, Cai Q, Wade SW, Stolshek BS, Adams JL, Balasubramanian A, Viswanathan HN, Kallich JD (2013) Osteoporosis medication adherence: physician perceptions vs. patients’ utilization. Bone 55:1–6
Bianchi ML, Duca P, Vai S et al (2015) Improving adherence to and persistence with oral therapy of osteoporosis. Osteoporos Int 26:1629–1638
Solomon DH, Iversen MD, Avorn J et al (2012) Osteoporosis telephonic intervention to improve medication regimen adherence: a large, pragmatic, randomized controlled trial. Arch Intern Med 172:477–483
Tuzun S, Akyuz G, Eskiyurt N et al (2013) Impact of the training on the compliance and persistence of weekly bisphosphonate treatment in postmenopausal osteoporosis: a randomized controlled study. International journal of medical sciences 10:1880–1887
Silverman SL, Siris E, Kendler DL et al (2015) Persistence at 12 months with denosumab in postmenopausal women with osteoporosis: interim results from a prospective observational study. Osteoporos Int 26:361–372
Hadji P, Papaioannou N, Gielen E et al (2015) Persistence, adherence, and medication-taking behavior in women with postmenopausal osteoporosis receiving denosumab in routine practice in Germany, Austria, Greece, and Belgium: 12-month results from a European non-interventional study. Osteoporos Int 26:2479–2489
Marsh D, Akesson K, Beaton DE, Bogoch ER, Boonen S, Brandi ML, McLellan AR, Mitchell PJ, Sale JE, Wahl DA (2011) Coordinator-based systems for secondary prevention in fragility fracture patients. Osteoporos Int 22:2051–2065
Eisman JA, Bogoch ER, Dell R, Harrington JT, McKinney RE, Jr., McLellan A, Mitchell PJ, Silverman S, Singleton R, Siris E (2012) Making the first fracture the last fracture: ASBMR task force report on secondary fracture prevention. J Bone Miner Res
Association BO (2007) The care of patients with fragility fractures
Akesson K, Marsh D, Mitchell PJ, McLellan AR, Stenmark J, Pierroz DD, Kyer C, Cooper C, Group IOFFW (2013) Capture the fracture: a best practice framework and global campaign to break the fragility fracture cycle. Osteoporos Int 24:2135–2152
Acknowledgments
The ReFRESH study group consists of Dr. Andrew David Judge, Dr. Muhammad Kassim Javaid, Professor Nigel Arden, Professor Cyrus Cooper, Professor Andrew Farmer, Dr. Daniel Prieto-Alhambra, Dr. Jose Leal, Professor Michael Goldacre, Professor Alastair Gray, Dr. Janet Lippett, Dr. Rachael Gooberman-Hill and Laura Graham.
Author information
Authors and Affiliations
Consortia
Corresponding author
Ethics declarations
Conflicts of interest
AS, SH and AD have no competing financial interests relevant to the submitted work. DPA, JL, CC, MKJ and AJ received grants from NIHR HS&DR during the conduct of the study. Outside the submitted work, MKJ reports personal fees from Lilly UK, Amgen, Sevier, Merck, Medtronic, Internis, Consilient Health, Stirling Anglia, Mereo Biopharma and Optasia. He serves on the Scientific Committee of the National Osteoporosis Society and International Osteoporosis Foundation; DPA received grants from Bioiberica S.A. and Amgen Spain S.A.; CC received personal fees from Servier, Amgen, Eli Lilly, Merck, Medtronic and Novartis. AJ has received consultancy, lecture fees and honoraria from Servier, UK Renal Registry, Oxford Craniofacial Unit, IDIAP Jordi Gol, Freshfields Bruckhaus Deringer, has held advisory board positions (which involved receipt of fees) from Anthera Pharmaceuticals, INC., and received research sponsorship from ROCHE.
Role of the funding source
This work was supported by the National Institutes of Health and Research (NIHR) Health Services and Delivery Research programme HS&DR) (project number 11/1023/01); and from the Oxford NIHR Musculoskeletal Biomedical Research Unit, Nuffield Orthopaedic Centre, University of Oxford. The views and opinions expressed therein are those of the authors and do not necessarily reflect those of the HS&DR programme, NIHR, NHS or the Department of Health. This study is based in part on data from the Clinical Practice Research Datalink obtained under licence from the UK Medicines and Healthcare products Regulatory Agency. The funding source had no role in the design and conduct of the study, in the collection, analysis and interpretation of the data, or in the preparation, review or approval of the manuscript.
Additional information
A Judge and MK Javaid are joint last authors.
Electronic supplementary material
Table S1
(DOCX 19 kb)
Rights and permissions
About this article

Cite this article
Shah, A., Prieto-Alhambra, D., Hawley, S. et al. Geographic variation in secondary fracture prevention after a hip fracture during 1999–2013: a UK study. Osteoporos Int 28, 169–178 (2017). https://doi.org/10.1007/s00198-016-3811-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-016-3811-4