
Abstract
Introduction and hypothesis
Visual tools are a valuable tool for ascertaining patient symptoms, especially in populations with low literacy rates. The objective was to develop and validate a pictorial scale for assessing symptomatic pelvic organ prolapse (POP) and urinary incontinence among women in western Kenya.
Methods
Illustrations of POP, stress urinary incontinence (SUI), and urgency urinary incontinence (UUI) were developed by an artist. Virtual Zoom interviews were conducted with gynecology providers in Kisumu soliciting feedback on the illustrations. Cognitive interviews with patients were then conducted. Validation of the illustrations was performed against the gold standard of clinical history and examination amongst patients presenting for outpatient care at three Kisumu hospitals.
Results
Sixteen provider interviews were conducted. The illustrations were revised to reflect each disorder more clearly, and performed well during cognitive interviews with 8 patients (aged 21 to 76). One hundred patients were included in the validation study. Nine patients had symptomatic POP, whereas 32 had UUI and 25 had SUI. Sensitivity and specificity for the SUI illustration was 80% (95% CI 61–91%) and 97% (95% CI 72–98%) and for UUI they were 81% (95% CI 65–91%) and 99% (95% CI 92–100%) respectively. POP illustrations had lower sensitivity and specificity, with the best performing illustration having sensitivity of 67% (95% CI 35–88%) and specificity of 99% (95% CI 94–100%), which improved when only bulge or pressure symptoms were included.
Conclusions
We present a newly developed pictorial scale to assess for clinical urinary incontinence and POP that may be adapted and evaluated in other settings for clinical and research purposes.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Pelvic floor disorders (PFDs) represent a significant health burden worldwide. Their prevalence and impact on patients’ quality of life are relatively understudied, especially in low- and middle- income countries (LMICs) where the emphasis has historically been placed on obstetric fistulas and access to treatment for PFDs is limited. A systematic review of PFDs in 16 LMICs in Asia, Latin America, and Africa estimated a prevalence of pelvic organ prolapse (POP) of 19.7%, urinary incontinence (UI) of 28.7%, and fecal incontinence of 7% [1]. However, only three countries in sub-Saharan Africa were represented in the review. Prior studies in Ghana, Gambia, Ethiopia, and Tanzania have reported prevalence rates ranging from 1% to 65%. The large differences in the prevalence rates could be due to differences in the classification and definition of both anatomical and symptomatic disease, given that only a few women with prolapse are symptomatic [2,3,4,5,6]. For example, an epidemiological study in Gambia reported the overall prevalence of POP to be 46% in 1,067 women examined; however, only 16% of the 152 women with “moderate/severe prolapse” (defined differently based on anterior, uterine, or posterior prolapse) endorsed symptoms [5]. To this day, little information exists regarding the prevalence of PFDs specifically in the Kenyan population.
The lack of appropriate validated instruments for assessing POP and UI is an important limiting factor in existing epidemiological studies of POP and UI in LMICs. This has resulted in prevalence data drawn from heterogeneous instruments that had either never been validated or that had been developed and validated among a high school to college-educated English-speaking population, and thus unlikely to be valid in a culturally and linguistically distinct setting [7,8,9,10]. Previous attempts to validate translated surveys in LMICs have concluded that the sensitivity and specificity of these instruments are variable, and in some cases, questions have had to be eliminated owing to incompatibility with the target language [3, 11, 12].
The main reason for pursuing treatment for either POP or UI is the presence of bothersome symptoms. Thus, it is critical to ensure that patients’ symptoms are accurately assessed. Using an illustration-based scale developed and validated among women in the target population living with POP or UI may help to bridge the literacy gap and more easily capture patients’ pelvic floor symptoms than would otherwise be captured using written language. The objective of the study was to develop a pictorial scale for assessing symptomatic POP and UI, and to describe knowledge, attitudes, and practices as they relate to pelvic floor disorders among patients and providers in western Kenya. We hypothesized that a pictorial scale that captures patients’ symptoms of POP and UI would have good performance characteristics in a population presenting for outpatient care at three hospitals in Kisumu, Kenya.
Materials and methods
An iterative process was used for the development of a candidate set of illustrations that was first developed by both a local Kenyan illustrator and symbols downloaded from the Noun Project online database. The illustrations were then reviewed by local gynecological providers via virtual interviews, and revised illustrations were pre-tested via in-person cognitive interviews with patients presenting for outpatient care in Kisumu. Validation of the finalized illustrations was then performed among a larger population of patients presenting for outpatient care.
Patients and providers were recruited from Jaramogi Oginga Odinga Teaching & Referral Hospital (JOOTRH), the main tertiary care center in Kisumu, Kenya, as part of an iterative, patient-centered, pictorial item development process. For the latter validation of the pictorial instruments, patients were additionally recruited from Migosi and Lumumba sub-county hospitals. The latter sites were chosen as the study authors had used them for previous research.
Creation of original candidate illustrations
An iterative item development process was used for the creation of pictorial representations of POP and UI. First, a local illustrator developed pictorial representations of women experiencing POP and UI. The illustrations underwent review by an expert group of gynecologists and urogynecologists from Kisumu, Kenya and Durham, USA and were revised to further clarify the condition being represented. Emotional representations of how POP or UI may impact the woman were then selected and downloaded from The Noun Project, an online, open-access repository of symbols created by graphic designers (Fig. 1). The use of an item bank of “facial pictures” to represent different emotional categories has been previously described in the development of a pictorial scale to assess hospitalization-related anxiety in the pediatric setting [8].

Initial candidate emotional representations of how prolapse and urinary incontinence may make a woman feel. a Emotional representation version 1. b Emotional representation version 2. c Emotional representation version 3
Initial review of illustrations with providers
Providers in the outpatient gynecology clinics were recruited by a local departmental research assistant and given a brief description of the research study. Interested providers who give permission to be contacted by MO provided their e-mail address and confirmed a time that would be convenient for them for an interview. Interviews were conducted on the online virtual Zoom platform in English, and verbal consent was obtained prior to each interview. During each session, which was conducted via smartphone or laptop as per the preference of the participant, screen-sharing was used to share each illustration. A semi-structured interview guide was used to solicit feedback on what each provider thought each illustration represented, how their patients may interpret the illustrations, and what suggestions they had on how the illustrations may be improved to better represent each condition. All participants were given direct monetary compensation (equivalent of USD 10) for participation in the interviews, which was approved by the local ethics committee.
Content validity was assessed following each revised iteration of the pictorial scales by the study investigators, which comprised 2 Kenyan obstetrician-gynecologists, 1 US obstetrician-gynecologist, and 1 urogynecology fellow.
Cognitive interviews
Following final revision of the illustrations based on provider feedback, patients with and without UI or POP were recruited from the outpatient clinics of JOOTRH and asked to complete cognitive interviews. A cognitive interview script was developed which probed participants on the extent to which she understood the content of the pictorial items, as well as the representativeness of the pictorial items of her symptoms. A sample size of 3–5 participants per candidate illustration was planned based on previous studies of questionnaire item development [13, 14].
Validation of pictorial assessment scale
Patients presenting for care at JOOTRH, Lumumba Health Center, and Migosi Health Center were invited to participate in a study validating the existing POP and UI illustration scales. Participants were asked to provide responses to the illustrations based on the presence or absence of UI or POP symptoms. Participants were asked to undergo full clinical history and examination to confirm the presence or absence of POP and UI.
To screen for symptomatic prolapse, participants were asked two questions adopted from a previous epidemiological study of POP in the USA, which was translated and back-translated into both Kiswahili and Dholuo, the primary languages spoken in Kisumu [15]:
-
1.
Do you have a feeling of bulging/pressure or something seems to be coming out of the vagina?
-
2.
Do you have a visible mass protruding via the vagina?
These questions were previously used in the Pelvic Floor Disorders in Tanzania (PEDITA) epidemiological study by Masenga and colleagues to assess symptomatic POP [3]. An affirmative answer to the questions indicated symptomatic prolapse. To assess for symptomatic incontinence, participants were asked the two screening questions from the Incontinence Severity Index to screen for symptomatic urinary incontinence [9]. Patients meeting criteria for "moderate" incontinence severity according to the Incontinence Severity Index were considered to have symptomatic UI. Although this has not specifically been validated in Dholuo or specifically among patients in Kisumu, following initial piloting of the screening surveys during cognitive interviews, good comprehension of the questionnaires was noted.
Patients responding affirmatively to either of the POP symptom questions, or reporting "moderate" UI severity, were considered to have screened positive for POP or UI symptoms and were invited to participate. Asymptomatic patients were also invited to participate. Following consent, patients completed a demographic and medical history questionnaire with questions regarding age, marital status, employment, parity, religion, gravidity, parity, route of delivery, previous hysterectomy, and menstrual status. Patients then underwent pelvic examination, in which absence of urogenital fistula, presence of leakage on a simple cough stress test, and level of prolapse based on the Baden–Walker Halfway Scoring System were noted [16].
Patients with grade 2 prolapse (descent to the hymen or beyond) and who were noted to have symptoms based on clinical history were considered to have symptomatic POP. Patients who had clinical symptoms of urgency urinary incontinence and stress urinary incontinence, with or without the presence of leakage on supine cough stress test, and without clinical evidence for a fistula, were considered to have symptomatic UUI or SUI. Informed consent was obtained in the local language of Dholuo or Swahili.
Ethical approval to conduct the study was obtained from the JOOTRH and Duke University Hospital Institutional Review Boards.
Sample size calculations
A convenience sample of 200 participants was planned for the validation study. This sample size also allowed for 80% power to detect a sensitivity of the instrument of 80% using a conservative estimate of the prevalence of prolapse and urinary incontinence of 10%, based on prior studies of low- and middle-income countries, which included countries within sub-Saharan Africa [17, 18]. Patients’ illustration responses and clinical history and examination data were used to calculate sensitivity, specificity, and positive and negative likelihood ratios (+LR and −LR) with 95% confidence intervals. Receiver-operating characteristic analysis was used to determine the diagnostic accuracy of each of the illustrations in this population.
Results
Initial review of illustrations with providers
Eighteen providers were recruited in the department of Obstetrics and Gynecology between October and December 2020, of whom 16 providers provided verbal consent and participated in virtual interviews (Table 1). One provider was unable to connect for an interview until after the illustrations underwent final review, and another provider ultimately did not schedule an interview. Illustrations representing POP, SUI, and UUI were revised to more clearly reflect each disorder and decrease confusion with other conditions such as abdominal pain, urogenital fistula, and menorrhagia (Fig. 2; Supplementary Figs. 1–3) All candidate emotion symbols downloaded from the Noun Project were deemed too abstract to be readily interpreted by patients as discrete emotional states. Therefore, a new set of illustrations was developed to depict life-like representations of positive, negative, and neutral emotions associated with POP and UI (Fig. 3).

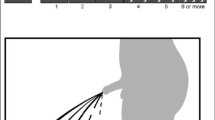
Final illustrations of stress urinary incontinence, urgency urinary incontinence, and pelvic organ prolapse. a Stress urinary incontinence. b Urgency urinary incontinence. c Pelvic organ prolapse (version 1). d Pelvic organ prolapse (version 2)

Final illustrations of negative, neutral, and positive emotions associated with pelvic organ prolapse and urinary incontinence
Cognitive interviews
Eight participants participated in cognitive interviews between March and October of 2021 (age range 21–76; age of 1 participant unknown). Most (n=5, 83%) patients without POP did not initially understand what was being represented by the POP illustration; however, they were able to correctly identify that they did not have the condition. The 2 participants with POP were able to easily identify their conditions in the POP illustrations. Two of the participants who did not have POP thought the POP illustration represented childbirth, although they were unable to provide specific recommendations as to how the artist could improve the illustration.
During the review process of the cognitive interviews, one of the authors (SG) recommended a new illustration be made for POP showing a woman standing and holding a heavy load with one leg resting on a chair, as the first version, of a woman squatting, could be easily confused with childbirth. This new illustration (Fig. 2d) was shown to 1 participant with POP during the final round of cognitive interviews. The woman with POP did note that of the two illustrations, this new illustration was likely more appropriate for POP.
For the SUI illustration, 1 of the 2 women with SUI was able to correctly identify themselves as having SUI in the illustration. Three of the 6 women without SUI were able to identify the illustration as being consistent with SUI. The other 2 participants did not know what the illustration was showing but were confident that they did not have the condition being represented. Other than to make the dress darker as if wet with urine, participants were unable to identify specific suggestions for improvement of the illustration.
For the UUI illustration, all 4 participants with UUI were able to correctly identify themselves as having the condition in the illustration. One of the 4 asymptomatic women (the patient had pure SUI) also thought that she had the condition represented in the illustration. One participant provided a suggestion for improvement—that the dress could be shown as not being wet. As 3 patients relied on the dress looking wet to identify the illustration as representing UUI, the illustration was not changed.
Validation of finalized candidate illustrations
Between October and November 2021, a total of 388 participants were screened for symptoms and invited to participate in the study at the outpatient gynecology clinics of JOOTRH, Lumumba, and Migosi Health Centres. Overall, 26% of patients agreed to participate in the study. Although not all reasons for nonparticipation were recorded, the majority of patients whose reasons were recorded had declined owing to a lack of time or not wanting to undergo a pelvic examination. Overall, 9 patients had POP, 25 had SUI, and 32 had UUI. Eighty-eight percent of symptomatic patients according to the screening questions gave consent to study participation, whereas 17% of asymptomatic patients according to the screening questions gave consent to study participation. Seven percent of participants were unable to read and write. Ultimately, on clinical history and examination, 53% of study participants were symptomatic for prolapse, SUI, or UUI, whereas 47% of participants were asymptomatic (Table 2).
Overall, patients symptomatic with UI or POP were older. No participants had clinical evidence of fistula or a history of fistula or other anti-incontinence surgery (Table 1). Of the 9 women with prolapse, 1 woman (17%) had grade 4 apical prolapse, 4 women (67%) had grade 3 prolapse, and 1 woman had grade 2 prolapse. Only 2 women demonstrated leakage on cough stress test. Five women (83%) noted a bulge or pressure symptoms, whereas the 1 woman with grade 2 prolapse had post-defecatory stool seepage, which was suspected to be secondary to a grade 2 rectocele and 1 woman with grade 3 prolapse denied bulge symptoms but endorsed difficulty with bladder emptying.
Performance of UI and POP illustrations
The SUI illustration had 80% sensitivity (95% CI 61–91%) and 97% specificity (95% CI 91–99) for detecting SUI, whereas the UUI illustration had 81% sensitivity (95% CI 65–91) and 99% specificity (95% CI 92–100) for detecting UUI (Table 3). Receiver operating characteristic (ROC) analysis showed an area under the curve (AUC) of 0.89 for the SUI illustration, whereas the UUI had an AUC of 0.90.
The first version of the POP illustration had a low sensitivity of 56% (95% CI 27–81%) for detecting POP. The second version had 67% sensitivity (95% CI 36–88%) and 99% specificity (95% CI 94–100%) for clinical POP (Table 3). ROC analysis showed AUC of 0.76 for the first POP illustration, whereas for the second version the ROC analysis showed AUC of 0.83.
As 2 of the patients who were found to have symptomatic POP had either urinary or defecatory symptoms, we performed a sub-analysis of POP patients with only bulge or pressure symptoms. The second version of the POP illustration had significantly higher sensitivity for the detection of bulge symptoms (86% sensitivity; 95% CI 49–97%; Table 3).
Because our population of patients had likely significant over-representation of patients with POP or UI symptoms, positive and negative predictive values were not calculated, as the true prevalence was not known.
Emotion illustrations
Of 20 patients with SUI who identified themselves as having SUI in the illustrations, 18 patients indicated that their condition made them feel the negative facial expression. Most common reasons for choosing that image included feelings of discomfort and embarrassment. Two patients selected the middle, neutral face, both of whom noted it was because they considered their symptoms to be normal.
Of 26 patients with UUI who identified themselves as having UUI in the illustrations, 24 patients indicated the negative facial expression, with most patients noting that it made her feel bad and uncomfortable. Two patients identified with the neutral expression, 1 of whom noted it that was “normal,” whereas the other noted that she was unsure how she felt.
Of 7 patients with POP who identified themselves as having POP in the illustrations, 4 chose the negative emotion owing to discomfort, whereas 2 patients chose the neutral expression because they considered it normal or had mixed reactions, whereas 1 patient chose the positive expression because she was happy that she was not experiencing pain.
Discussion
We present a novel instrument to aid in the screening of patients for symptomatic POP and UI, as well as to assess level of symptom impact using facial illustrations. Overall, the SUI and UUI illustrations had moderate performance characteristics whereas the second version of the POP illustration had high point estimates for sensitivity and specificity, particularly for bulge symptoms. However, given wide confidence intervals due to a low overall number of POP patients, further evaluation of the POP illustrations in a larger sample of patients with symptomatic POP is needed. The present illustrations may prove useful for clinical and research purposes, not only in Kenya but also in other culturally and linguistically distinct areas where the primary language may not be written, there may be an overall low literacy rate, or there may be poor pelvic health literacy amongst the population.
Although there have been several screening tools for both POP and UI, these were developed in a Western population and none has been validated for use in western Kenya in Dholuo or Kiswahili. Furthermore, even in areas where the language is written and the literacy rates are high, because of the stigma associated with gynecological health, low pelvic health literacy and discomfort with verbally communicating stigmatized symptoms may impede the accurate assessment of symptomatic pelvic floor disorders. This is demonstrated by a previous study in which the Pelvic Organ Prolapse Distress Inventory-6 and Pelvic Floor Impact Questionnaire-7 (PFIQ-7) were translated into Swahili in Tanzania; however, one question from each questionnaire ultimately had to be eliminated because there was no appropriate, easily comprehensible Swahili translation [3].
Previous studies validating written screening tools for POP and UI in sub-Saharan Africa have demonstrated variable results. A prior study in Ethiopia of the four-item Pelvic Organ Prolapse Simple Screening Inventory (POPSSI), adapted from the Pelvic Floor Distress Inventory-20 (PFDI-20), in Amharic, reported 90% sensitivity and 60% specificity [12]. Similar to our findings, the sensitivity and specificity of the one item assessing the presence of feeling or seeing a bulge in the vagina was much higher (sensitivity 93% and specificity 84% for anterior compartment prolapse), whereas items eliciting SUI symptoms, urinary urgency, and pain during defecation had very low sensitivity and specificity for detecting prolapse. This is a finding consistent with studies that have found the presence of a bulge to be the most reliable predictor of anatomical prolapse [19, 20]. As the symptom most reliably improved by any treatment method for prolapse is a vaginal bulge, it is arguably reasonable to prioritize this symptom in a screening questionnaire. To address some of the issues inherent in a written questionnaire, Goba and colleagues adapted the PFDI-20 and PFIQ-7 into the Tigrinya language in northern Ethiopia, and evaluated the validity and reliability of the oral administration of these questionnaires, as 60% of their study population were not literate [21]. To our knowledge, this is the only other study that addresses an alternative to the standard written survey for ascertainment of patient symptoms. Although oral administration of the PFDI-20 and PFIQ-7 eliminates some of the barriers related to the written survey, it introduces additional time and surveyor burden, which may ultimately limit the feasibility of implementation in a busy clinical setting. The lack of a written questionnaire does limit the ability to assess more granular aspects of the impact of PFDs on quality of life, but our emotion illustrations did correlate well with verbal representations of patients’ level of distress secondary to the prolapse.
The strengths of the study lie in its incorporation of patient and provider feedback during multiple phases of illustration development and the use of targeted feedback with patients during the cognitive interview process. The main limitation was the sample size, which was largely impacted by asymptomatic patients who declined a pelvic examination, as well as lower clinical numbers of patients presenting for outpatient care in the context of the COVID-19 pandemic. Symptomatic patients may have been more motivated to undergo a pelvic examination owing to personal interest in the topic under study. This ultimately biased our sample toward women with symptomatic PFDs and thus our cohort does not describe overall POP or UI prevalence in this region. Therefore, although anecdotally the POP illustrations worked well amongst patients with POP, further validation of this instrument is needed. Older patients, who may have been more likely to be impacted by prolapse, may have been less likely to present for care at hospital or sub-county hospital clinics. We are planning to address this limitation in a future community-based validation study of these illustrations with the goal of evaluating these illustrations in a larger population of patients, potentially representing a larger pelvic floor symptom burden. Focus group discussions with patients were also initially planned with the original candidate illustrations; however, because of the COVID-19 pandemic and limits on in-person gatherings, this was replaced by virtual interviews with Kenyan gynecology providers. We were eventually able to incorporate patient feedback during the later cognitive interviews.
Many patients declined study participation because they did not want to undergo a pelvic examination. At least 2 patients at one of the sub-county hospitals specifically declined an examination by a white provider owing to previous negative experiences with undergoing a study examination by a different foreign provider, in which a picture had been unexpectedly taken during the examination. We are unaware of the specifics of this other study, but this mistrust may have accounted for other patients’ lack of willingness to participate. Although we ultimately did not achieve our originally calculated sample size, the confidence intervals for the sensitivity and specificity of the SUI and UUI illustrations suggest good performance of these illustrations, and the facial illustrations chosen by patients to represent their emotional states were concordant with those verbalized.
In conclusion, we present a novel pictorial scale for assessing for clinical UI and POP that was developed using a hybrid virtual and in-person format. Overall, the SUI and UUI illustrations had acceptable performance characteristics in our population. Validation of the POP illustrations was limited by the low overall number of participants with symptomatic POP and requires further evaluation in a larger population of patients with clinically significant POP. The present illustrations may be adapted and evaluated in other culturally and linguistically distinct settings for clinical and research purposes.
References
Walker GJA, Gunasekera P. Pelvic organ prolapse and incontinence in developing countries: review of prevalence and risk factors. Int Urogynecol J. 2011;22(2):127–35. https://doi.org/10.1007/s00192-010-1215-0.
Ballard K, Ayenachew F, Wright J, Atnafu H. Prevalence of obstetric fistula and symptomatic pelvic organ prolapse in rural Ethiopia. Int Urogynecol J. 2016;27(7):1063–7. https://doi.org/10.1007/s00192-015-2933-0.
Masenga GG, Shayo BC, Rasch V. Prevalence and risk factors for pelvic organ prolapse in Kilimanjaro, Tanzania: a population based study in Tanzanian rural community. PLoS One. 2018;13(4):e0195910. https://doi.org/10.1371/journal.pone.0195910.
Megabiaw B, Adefris M, Rortveit G, et al. Pelvic floor disorders among women in Dabat district, northwest Ethiopia: a pilot study. Int Urogynecol J. 2013;24(7):1135–43. https://doi.org/10.1007/s00192-012-1981-y.
Scherf C, Morison L, Fiander A, Ekpo G, Walraven G. Epidemiology of pelvic organ prolapse in rural Gambia, West Africa. BJOG. 2002;109(4):431–6. https://doi.org/10.1111/j.1471-0528.2002.01109.x.
Wusu-Ansah OK, Opare-Addo HS. Pelvic organ prolapse in rural Ghana. Int J Gynaecol Obstet. 2008;103(2):121–4. https://doi.org/10.1016/j.ijgo.2008.06.014.
Bradley CS, Rovner ES, Morgan MA, et al. A new questionnaire for urinary incontinence diagnosis in women: development and testing. Am J Obstet Gynecol. 2005;192(1):66–73. https://doi.org/10.1016/j.ajog.2004.07.037.
Barber MD, Walters MD, Bump RC. Short forms of two condition-specific quality-of-life questionnaires for women with pelvic floor disorders (PFDI-20 and PFIQ-7). Am J Obstet Gynecol. 2005;193(1):103–13. https://doi.org/10.1016/j.ajog.2004.12.025.
Shumaker SA, Wyman JF, Uebersax JS, McClish D, Fantl JA. Health-related quality of life measures for women with urinary incontinence: the Incontinence Impact Questionnaire and the Urogenital Distress Inventory. Continence Program in Women (CPW) Research Group. Qual Life Res. 1994;3(5):291–306. https://doi.org/10.1007/BF00451721.
Sandvik H, Hunskaar S, Seim A, Hermstad R, Vanvik A, Bratt H. Validation of a severity index in female urinary incontinence and its implementation in an epidemiological survey. J Epidemiol Community Health. 1993;47(6):497–9. https://doi.org/10.1136/jech.47.6.497.
Tehrani FR, Hashemi S, Simbar M, Shiva N. Screening of the pelvic organ prolapse without a physical examination; (a community based study). BMC Womens Health. 2011;11(1):48. https://doi.org/10.1186/1472-6874-11-48.
Kassa DW, Ferede YG, Advolodkina P. Validation of the Pelvic Organ Prolapse Simple Screening Inventory (POPSSI) in a population of Ethiopian women. BMC Womens Health. 2019;19(1):52. https://doi.org/10.1186/s12905-019-0746-x.
DeWalt DA, Rothrock N, Yount S, Stone AA. PROMIS Cooperative Group. Evaluation of item candidates: the PROMIS qualitative item review. Med Care. 2007;45(5 Suppl 1):S12–21. https://doi.org/10.1097/01.mlr.0000254567.79743.e2.
Morgan SJ, Amtmann D, Abrahamson DC, Kajlich AJ, Hafner BJ. Use of cognitive interviews in the development of the PLUS-M item bank. Qual Life Res. 2014;23(6):1767–75. https://doi.org/10.1007/s11136-013-0618-z.
Rortveit G, Brown JS, Thom DH, Van Den Eeden SK, Creasman JM, Subak LL. Symptomatic pelvic organ prolapse: prevalence and risk factors in a population-based, racially diverse cohort. Obstet Gynecol. 2007;109(6):1396–403. https://doi.org/10.1097/01.AOG.0000263469.68106.90.
ACOG. Committee on Practice Bulletins—Gynecology. ACOG Practice Bulletin No. 85: pelvic organ prolapse. Obstet Gynecol. 2007;110(3):717–29. https://doi.org/10.1097/01.AOG.0000263925.97887.72.
Islam RM, Oldroyd J, Rana J, Romero L, Karim MN. Prevalence of symptomatic pelvic floor disorders in community-dwelling women in low and middle-income countries: a systematic review and meta-analysis. Int Urogynecol J. 2019;30(12):2001–11. https://doi.org/10.1007/s00192-019-03992-z.
Bujang MA. Requirements for minimum sample size for sensitivity and specificity analysis. J Clin Diagn Res. 2016;10(10):YE01–6. https://doi.org/10.7860/JCDR/2016/18129.8744.
Ellerkmann RM, Cundiff GW, Melick CF, Nihira MA, Leffler K, Bent AE. Correlation of symptoms with location and severity of pelvic organ prolapse. Am J Obstet Gynecol. 2001;185(6):1332–7; discussion 1337–1338. https://doi.org/10.1067/mob.2001.119078.
Tan JS, Lukacz ES, Menefee SA, Powell CR, Nager CW. San Diego Pelvic Floor Consortium. Predictive value of prolapse symptoms: a large database study. Int Urogynecol J Pelvic Floor Dysfunct. 2005;16(3):203–9; discussion 209. https://doi.org/10.1007/s00192-004-1243-8.
Goba GK, Legesse AY, Zelelow YB, et al. Reliability and validity of the Tigrigna version of the Pelvic Floor Distress Inventory-Short Form 20 (PFDI-20) and Pelvic Floor Impact Questionnaire-7 (PFIQ-7). Int Urogynecol J. 2019;30(1):65–70. https://doi.org/10.1007/s00192-018-3583-9.
Acknowledgements
The authors would like to thank Benjamin Nyang’oma for his assistance with illustration development and the Duke Division of Urogynecology for assistance with initial illustration review.
Funding
This study was funded by the Josiah Charles Trent Memorial Foundation Endowment Fund and the Charles Hammond Fund.
Author information
Authors and Affiliations
Contributions
M. O’Shea: protocol/project development, data collection or management, data analysis, manuscript writing/editing; J. Omoto: protocol/project development, data collection or management, manuscript writing/editing; M. Huchko: protocol/project development, manuscript writing/editing; S. Gwer: protocol/project development, data collection or management, manuscript writing/editing.
Corresponding author
Ethics declarations
Conflicts of interest
None.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
O’Shea, M., Omoto, J., Huchko, M. et al. Development and initial validation of a pictorial survey to assess for symptomatic pelvic organ prolapse and urinary incontinence in western Kenya. Int Urogynecol J 33, 2515–2523 (2022). https://doi.org/10.1007/s00192-022-05214-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00192-022-05214-5