
Abstract
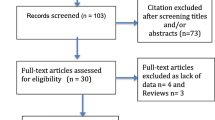
Because the prognostic value of 1-h pad testing has received scant attention, we tested the hypothesis that mild incontinence of any etiology is more readily cured than moderate incontinence. A consecutive series of 150 patients with mild (2–9.9 g) to moderate (10–49.9 g) incontinence (as judged by weight gain on 1-h pad testing) [1] attending a urogynecology unit were recruited, of whom 145 completed all baseline objective measures: 110 completed 12 weeks of conservative therapy, with follow-up data at 2 years available for 51 subjects. At 12 weeks 81% of 'mild' patients became 'dry' on the 1-h pad test versus 36.8% in the moderate group (χ2 <0.0001). Interestingly the post-treatment changes seen in all other outcomes demonstrated equally positive responses for the mild and moderate groups. At 2-year follow-up 29/71 (40.8%) of patients with mild incontinence and 22/74 (29.7%) of patients with moderate incontinence were satisfied and had no requirement for further therapy, the remainder having sought other treatments (χ2=1.963 P=0.161). Of the responders, (11/29) (37.9%) of mildly incontinent patients and (8/22 (36.4%)) of moderately affected subjects remained continent (on 20-point incontinence score ≤2 m, χ2=0.013, P=0.9087). Improvements in quality of life persisted to an equal degree in both groups.

Similar content being viewed by others


Abbreviations
- GSI:
-
Genuine stress incontinence
- DI:
-
Detrusor instability
- SU:
-
Sensory urgency
- FVC:
-
Frequency/volume chart
- NCA:
-
Nurse continence adviser
References
Klarskov P, Hald T (1984)Reproducibility and reliability of urinary incontinence assessment with a 60 min test. Scand J Urol Nephrol. 18: 293–298
Cammu H, Van Nylen A (2000) 10-year follow-up after Kegel pelvic floor muscle exercises for genuine stress incontinence. Br J Urol 85:655–658
Burns P,PranikoffK, Nochajski M et al(1990) Treatment of stress incontinence with pelvic floor exercises and biofeedback. J Am Geriartr Soc 38:341–344
Fonda D, Resnick N.M, Kirschner-Hermanns R (1998) Prevention of urinary incontinence in older people. Br J Urol 82 [Suppl 1]:5–10
Moore KH, O'Sullivan RJ, Simons A, Prashar S, Anderson P, Louey M (2003) Randomised controlled trial of nurse continence advisor therapy compared with standard urogynaecology regimen for conservative incontinence treatment: efficacy, costs and two year follow up. Br J Obstet Gynaecol 110:649–657
Blackwell A, Yoong W, Moore KH (2003) Criterion validity, test retest reliability and sensitivity to change of the St. George Urinary Incontinence Score. BJU Int (In press)
Lose G, Rosenkilde P, Gammelgaard J, Schroeder T (1988) Pad weighing tests performed with standardized bladder volumes. Urology 32:78–80
Ware JE, Sherbourne CD (1992) The MOS 36-item short form health survey (SF-36). Med Care 473–481
Shumaker SA, Wyman JF, Uebersax JS, McClish D, Fantl JA (1994) Health-related quality of life measures for women with urinary incontinence: the Incontinence Impact Questionnaire and the Urogenital Distress Inventory. Continence Program in Women (CPW) Research Group. Qual Life Res 3:291–306
Laycock J (1992) Clinical evaluation of the pelvic floor. PhD thesis, University of Bradford
Plevnick S (1985) A new method for testing and strengthening of pelvic floor muscles. Proc 15th Annual Meeting, International Continence Society, p 247
Simons AM, Yoong WC, Buckland S, Moore KH (2001) Inadequate repeatability of the one hour pad test: the need for a new incontinence outcome measure. Br J Obstet Gynaecol 108:315–319
Simons AM, Foote A, Moore K (2001) Quality of life assessment as an outcome measure in urinary incontinence research. A comparison of various quality of life and incontinence measures (abstract). Int Urogynecol J 12 [Suppl 3]:169
Maher C, Carey P (2001) Pubovaginal or vicryl mesh rectus fascia sling in intrinsic sphincter deficiency. Int Urogynecol J 12:111–116
Millard RJ, Oldenberg B (1983) The symptomatic, urodynamic and psychodynamic results of bladder re-education programs. J Urol 130:715–719
Millard R, Moore K (eds) (1996) Urinary incontinence: the Cinderella subject. Med J Aust 165:124
Berghmans LCM, Hendricks HJM, De Bie RA et al (2000) Conservative treatment of urge urinary incontinence in women: a systematic review of randomized clinical trials. Br J Urol 85:254–263
Morkvend S, Bo K (2000) Effect of postpartum pelvic floor muscle training in prevention and treatment of urinary incontinence: a one-year follow up. Br J Obstet Gynaecol 107:1022–1028
Author information
Authors and Affiliations
Corresponding author
Additional information
Editorial Comment: The authors compare treatment outcomes and costs of mild versus moderate urinary incontinence. They use a population of patients in whom the different types of incontinence (i.e., urge, stress, etc.) are not separated. A 1-h pad test is used as the severity measure to separate out the two groups. According to the authors' own acknowledgement, the 1-h pad test is rather artificial. Therefore, it is not an appropriate test to use for severity assessment. The authors could have chosen one of numerous other outcome measures in order to design this study.
Their secondary goal was to determine potential outcomes of secondary prevention of urinary incontinence. The paper confirms the fact that a 1-h pad test does not correlate with multiple other tools for severity assessment.
Rights and permissions
About this article
Cite this article
O'Sullivan, R., Simons, A., Prashar, S. et al. Is objective cure of mild undifferentiated incontinence more readily achieved than that of moderate incontinence? Costs and 2-year outcome. Int Urogynecol J 14, 193–198 (2003). https://doi.org/10.1007/s00192-003-1062-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00192-003-1062-3